
Abstract
Objective:
To compare the efficacy and tolerability of lithium versus quetiapine for the treatment of manic or mixed episodes in youths with early course bipolar I disorder.
Methods:
Six-week, randomized, double-blind clinical trial of lithium versus quetiapine for the treatment of adolescents with acute manic/mixed episode. Target dose of quetiapine dose was adjusted to a target dose of 400–600 mg and target serum level for lithium was 1.0–1.2 mEq/L. Primary outcome measure was baseline-to-endpoint change in the Young Mania Rating Scale (YMRS). Secondary outcomes were treatment response (50% or more decrease from baseline in YMRS score) and remission (YMRS score ≤12, Children's Depression Rating Scale-Revised [CDRS-R] total score ≤28 and Clinical Global Impression Bipolar Severity Scale [CGI-BP-S] overall score of ≤3, respectively).
Results:
A total of 109 patients were randomized (quetiapine = 58 and lithium = 51). Participants in the quetiapine treatment group showed a significantly greater reduction in YMRS score than those in the lithium group (−11.0 vs. −13.2; p < 0.001; effect size 0.39). Response rate was 72% in the quetiapine group and 49% in the lithium group (p = 0.012); no differences in remission rates between groups were observed. Most frequent side effects for lithium were headaches (60.8%), nausea (39.2%), somnolence (27.5%), and tremor (27.5%); for quetiapine somnolence (63.8%), headaches (55.2%), tremor (36.2%), and dizziness (36.2%) were evidenced. Participants receiving quetiapine experienced more somnolence (p < 0.001), dizziness (p < 0.05), and weight gain (p < 0.05).
Conclusions:
Treatment with both lithium and quetiapine led to clinical improvement. Most study participants in this study experienced a clinical response; however, less than half of the participants in this study achieved symptomatic remission. The head-to-head comparison of both treatment groups showed quetiapine was associated with a statistically significant greater rate of response and overall symptom reduction compared with lithium. Trial registration:
Introduction
Onset of bipolar disorder most commonly occurs during adolescence and typically, patients with bipolar disorder experience repeated affective episodes that progressively increase in frequency and severity with illness duration, particularly early in the illness course (Perlis et al. 2004). Moreover, youth with bipolar disorder experience significantly more disability (Scott et al. 2014), increased risk of suicide (Hauser et al. 2013), reduced quality of life (Freeman et al. 2009), and significant functional impairment compared with nonaffected peers (Goldstein et al. 2009). Mania is the defining clinical feature of bipolar I disorder and is characterized by periods of abnormally elevated mood and/or abnormally irritable mood paired with an abnormal and persistent increase in activity or energy.
Several pharmacological agents are effective for the treatment of mania in youth (Liu et al. 2011; Biederman et al. 2012; Peruzzolo et al. 2013); however, treatment response is highly heterogeneous and selecting among pharmacological agents for a specific patient remains mostly empirical. At present, there is no reliable method to determine which subgroups of patients are more likely to respond to a specific medication. Moreover, pharmacologic agents with similar antimanic properties may have different molecular targets and exert distinct neurophysiologic effects. Among the agents effective in treating mania in youth, quetiapine and lithium seem to have different molecular targets and neurophysiological effects. Both lithium (Findling et al. 2015) and quetiapine (Pathak et al. 2013) have demonstrated efficacy in treating mania in children and adolescents in randomized placebo-controlled clinical trials. Lithium has been linked to a variety of molecular targets that may be critical for treatment response including direct inhibition of glycogen synthase kinase 3β (Klein and Melton 1996; Lin et al. 2013; de Sousa et al. 2015) and inositol monophosphatase 1 (Davanzo et al. 2001; Sarkar et al. 2005; Patel et al. 2006; Damri et al. 2015), indirectly inhibiting protein kinase C (Chen et al. 2000; Szabo et al. 2009) and regulating the adenylyl cyclase and cyclic adenosine monophosphate system (Alda et al. 2013; Heinrich et al. 2013). Quetiapine has been theorized to exert its therapeutic effect through interaction with dopaminergic and serotonergic receptors. Identifying predictors of treatment response among antimanic agents with different mechanisms of action might identify subgroups of youths with mania who are more likely to respond to a particular agent, thus permitting strategies for targeted treatment assignment.
To date there have been few comparative efficacy studies between medications used in the treatment of mania in youths with bipolar disorder. Lithium has been compared with risperidone in a randomized controlled trial of early age mania, where risperidone yielded higher response rates compared with lithium (Geller et al. 2012). In addition, quetiapine has been compared with divalproex for mania in adolescents and was found to be superior to divalproex in terms of response and remission (DelBello et al. 2006). Quetiapine and lithium have been compared in adult populations (Bowden et al. 2005; Li et al. 2008); however, there are no clinical trials directly comparing lithium and quetiapine for mania in this age group.
This study represents the clinical results from a larger project of neurophysiologic predictors of treatment response (
Methods
Participants
This study enrolled participants 10–17 years of age (Tanner scale stage II–V) (Duke et al. 1980) with a diagnostic and statistical manual (DSM)-IV (American Psychiatric Association, 2000) diagnosis of bipolar I disorder, during their first hospitalization for a manic or mixed episode, or who had been recently diagnosed in an outpatient setting. The diagnosis of bipolar I disorder with current mixed or manic episode was confirmed using the Washington University in St. Louis Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-KSADS) (Geller et al. 2001) performed by a trained clinician with demonstrated diagnostic interrater reliability (kappa >0.9). All participants were required to have an intelligence quotient (IQ) of at least 70 as assessed by the Wechsler Abbreviated Scale of Intelligence (WASI). Participants were also required to have a Young Mania Rating Scale (YMRS) (Young et al. 1978) baseline score of ≥20 to be eligible for study entry. In addition, all participants were required to have no previous hospitalization for a manic/mixed episode; have <2 years from onset of bipolar disorder, defined by age at onset of first DSM-IV-TR affective episode (mania, hypomania, depression, or mixed); have no >3 months of lifetime psychotropic medication exposure (with the exception of psychostimulants); and have no active psychotropic medication at least 1 week before enrollment (72 hours for psychostimulants and benzodiazepines). No study participants were taken off medications for the purpose of study participation. Female patients were required to agree to one of the following methods of birth control: complete abstinence from sexual intercourse, barrier (diaphragm or condom), or oral/injectable contraceptive.
Subjects were excluded from the study if they had a lifetime diagnosis of any psychotic disorder, posttraumatic stress disorder, any non-nicotine substance use disorder, or had a diagnosis of intellectual disability. Subjects were also excluded if they had a history of major medical or neurological illness; any lifetime significant episode (>10 minutes) of loss of consciousness; or had a positive pregnancy test at baseline.
The study and all procedures were approved by the institutional review board at the Cincinnati Children's Hospital Medical Center and the University of Cincinnati and conducted in accordance with the International Conference on Harmonization Good Clinical Practice guidelines and with the ethical principles of the Declaration of Helsinki. All subjects and their legal guardians provided written assent and written informed consent, respectively, before any study procedure.
Study design
A total of 123 children and adolescents were screened for study participation; of these, 109 subjects met study criteria and were enrolled in this 6-week, double-blind, randomized, clinical trial of quetiapine versus lithium for the treatment acute mania in youths with bipolar disorder (Fig. 1). Enrolled subjects completed all sociodemographic and clinical assessments at baseline. Sociodemographic measures collected at baseline included the following: previous medical and psychiatric treatments; family history of psychopathology (Family Interview for Genetics Studies: FIGS); and socioeconomic status (Hollingshead Four-Factor Index of Social Status) (Hollingshead 1975). Subjects were evaluated weekly for symptomatic progression and tolerability for duration of the study.
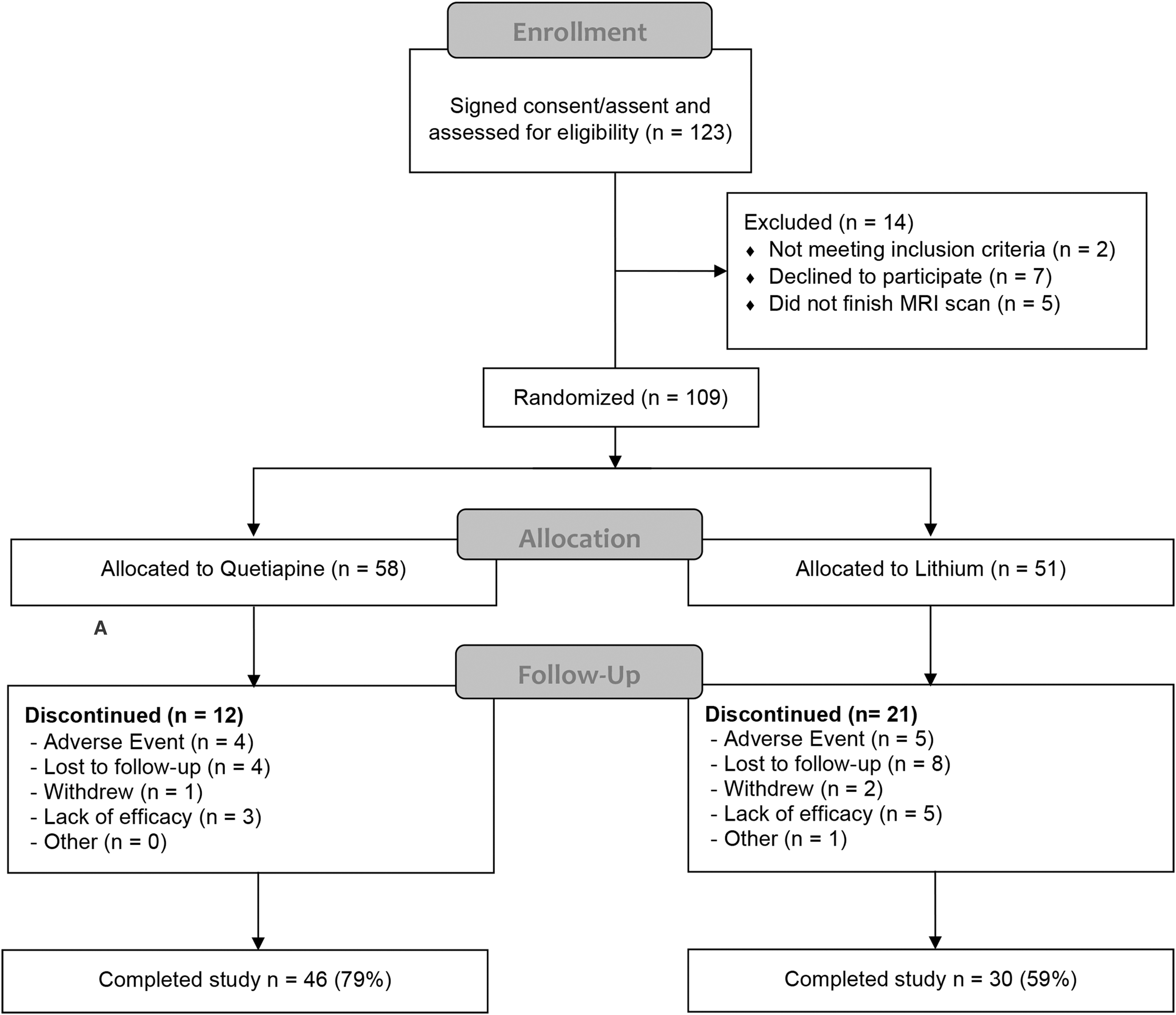
Patient disposition. Safety includes subjects who had at least one dose of the medications and had one post-follow-up visit. The intent-to-treat populations include all subjects randomized to receive medications.
Treatment allocation and study drug administration
Randomization to quetiapine versus lithium was stratified by the presence or absence of attention-deficit/hyperactivity disorder (ADHD) and/or psychosis, and whether the index episode was a mixed or manic episode. Treatment was administered in a double-dummy double-blind manner with medication pills being over-encapsulated to maintain the blind. Participants were initiated on 100 mg/d of quetiapine (or placebo) and 30 mg/kg (maximum starting dose of 600 mg twice daily) of lithium carbonate (or placebo), depending on randomization assignment. Participants received placebo for the medication to which they were not assigned. Based on tolerability, quetiapine dose was adjusted to a target dose of 400–600 mg and lithium was adjusted to a target serum level of 1.0–1.2 mEq/L. The target dose was intended to be reached during the first week of treatment; however, subsequent dose adjustments were allowed during the duration of the study. Because the target dose of lithium was based upon achieving a specific blood level we used an unblinded physician (C.M.A.), who monitored lithium levels in all study participants and implemented a yoking procedure to ensure the blind was maintained, and that participants randomized to lithium, achieved a therapeutic blood level. The unblinded physician did not participate in any direct patient evaluations. The use of lorazepam (up to 4 mg/d) as a rescue medication was permitted for the first 21 days. The use of benztropine for extrapyramidal side effects and diphenhydramine for insomnia was also permitted, with participants asked not to take these medications within 8 hours of their study visit. No other concomitant medications were allowed during the study.
Efficacy measures
Participants were evaluated weekly for symptomatic mood changes using the YMRS and the Children's Depression Rating Scale-Revised (CDRS-R) (Poznanski et al. 1984). Participants were also rated using the Clinical Global Impression Bipolar Severity Scale (CGI-BP-S) and the Clinical Global Impression Bipolar Improvement Scale (CGI-BP-I) at each study visit (Guy 1976). The a priori primary measure of efficacy changed from baseline to endpoint in YMRS. Secondary efficacy measures included treatment response and remission, defined by a ≥ 50% reduction from baseline to endpoint on YMRS score and an endpoint YMRS score ≤12, CDRS-R total score ≤28, and CGI-BP-S overall score of ≤3, respectively.
Tolerability
Tolerability was assessed and monitored weekly throughout the 6-week clinical trial and at a 4-week poststudy safety follow-up visit. To evaluate for the emergence of movement disorders the Simpson-Angus Rating Scale (SARS), Abnormal Involuntary Movement Scale (AIMS), and Barnes Akathisia Rating Scale (BARS) were performed by trained clinicians. Physical examination and anthropometric measurements; vital signs; laboratory tests (renal profile, complete blood count, liver function tests, thyroid-stimulating hormone [TSH], fasting lipid profile and glucose serum levels); and a 12-lead electrocardiogram (EKG) were conducted at baseline and at week 6 or study termination. Suicidal ideation and behavior were assessed using the Columbia Suicide Severity Rating Scale (C-SSRS) at every visit. In addition, a trough serum lithium level and serum quetiapine level was measured at weeks 1, 3, and 6. To maximize safety, participants who had two consecutive visits with a ≥ 33% increase in YMRS or CDRS-R scores from baseline were discontinued from study participation.
Statistical analysis
Descriptive statistics are presented for sociodemographic, clinical, laboratory, and tolerability variables (Table 1). Analysis for efficacy assessment used the intent-to-treat population, which consisted of all subjects randomized. For the primary efficacy measure, change from baseline YMRS was analyzed using a mixed model for repeated-measures analysis that included fixed effects for treatment group, week (as a categorical variable), sex, age, YMRS total score at baseline, and treatment-by-week interaction. The structure of the covariance model was fitted by minimizing the Akaike information criteria. Between-group effect size was calculated as the absolute value of estimated marginal mean (EMM) difference divided by the model estimate of the pooled standard deviation (SD), obtained from the square root of the diagonal element from the covariance matrix. For secondary measures, groups were compared at endpoint (week 6 or last observation carried forward [LOCF]) with standard chi-square; predictors of treatment response were presented as odds ratios (ORs) with corresponding 95% confidence intervals (95% CIs).
Baseline Patient Demographic and Clinical Characteristics
ADHD, attention-deficit/hyperactivity disorder; CDRS-R, Children's Depression Rating Scale-Revised; SD, standard deviation; SES, socioeconomic status; SGAs, second generation antipsychotics; WASI, Wechsler Abbreviated Scale of Intelligence; YMRS, Young Mania Rating Scale.
Similarly, to evaluate changes from baseline to endpoint in body weight and in standardized body mass index (BMI) (de Onis et al. 2007), a mixed model for repeated measurements was constructed. Changes from baseline to endpoint in SARS, BARS, and AIMS scores were analyzed using analyses of covariance with terms for medication group adding age and baseline YMRS scores as covariates. To evaluate role of demographic and clinical predictors with the a priori definition of treatment response, we performed binary logistic regressions adjusted for baseline severity using treatment response as dependent variable and the clinical and demographic variables as independent variables.
Results
Patients and disposition
A total of 109 subjects were randomly assigned to 6-week, double-blind treatment with quetiapine (n = 58) or lithium (n = 51); 105 participants (quetiapine, n = 57; lithium, n = 48) had at least one postbaseline assessment (Fig. 1). Study completion rates were significantly different between treatment arms with fewer subjects completing the 6-week follow-up and shorter mean days of follow-up in the lithium group compared with the quetiapine group (59% vs. 79%, p = 0.02; 32.7 vs. 41.4 days, p = 0.002). A majority of subjects who did not complete the study in the lithium arm discontinued during the first 3 weeks (75%), whereas those in the quetiapine group (63.6%) more commonly discontinued after the first 3 weeks (p = 0.035).
Baseline and clinical characteristics were similar between the two treatment groups (Table 1), although subjects randomized to lithium were slightly older (15.0 vs. 14.2 years of age, p = 0.046).
Study medications
In the intent-to-treat population, the mean daily dose for participants randomized to lithium was 1023 mg/d (±362 mg/d), whereas the average individual median lithium serum level was 0.57 mEq/L and the mean individual highest serum level was 0.88 mEq/L (SD ±0.4). Among subjects who completed the study, mean individual highest serum lithium level was 1.0 (SD ±0.3). Meanwhile the mean daily dose for those who were randomized to quetiapine was 428.3 mg/d (SD ±100 mg/d). Three participants (two in lithium group and one in quetiapine group) each received a single dose of lorazepam 1 mg single dose (one for anxiety and two for agitation). Six participants received a single dose of anti-histaminergic medication for insomnia (four in the quetiapine group and one in the lithium group). Three participants in the quetiapine group received benztropine for extrapyramidal symptoms—two subjects had mild rigidity and one mild akathisia.
Efficacy
The mixed-linear model for change in YMRS score revealed a significant fixed effect of treatment group (F = 16.04, df = 172.23, p < 0.001), week (F = 96.38, df = 458.05, p < 0.001), with a treatment group-by-week interactive effect (F = 2.26, df = 461.13, p = 0.039). On average, subjects in the quetiapine treatment group showed a significantly greater reduction in YMRS score (−11.0 vs. −13.2; p < 0.001; effect size = 0.39) than those in the lithium group. Separation between quetiapine and lithium in terms of change in YMRS score was seen as early as week 1; however, this difference lost statistical significance after week 4 (Fig. 2). No statistically significant differences between groups were noted at endpoint in clinician-assessed global severity (mean overall CGI-BP-S: 3.4 vs. 3.0, p = 0.12, respectively) and improvement (mean overall CGI-BP-I: 2.4 vs. 2.2, p = 0.27).

Clinical efficacy measures over time.
More than half of the 109 subjects randomized (61.5%) met a priori criteria for treatment response at endpoint (week 6 or LOCF). Comparing both treatment arms at endpoint, a statistically significant (p = 0.012) larger proportion of subjects in quetiapine group (72.4%) met criteria for treatment response compared with subjects in lithium group (49%). Overall remission rate at endpoint was 45.9% for both treatment groups. Remission rates did not differ between treatment groups (quetiapine = 51.7% vs. lithium = 39.2%; p = 0.19).
Adverse events
The percentage of study participants reporting at least one treatment-emergent adverse event did not differ between groups. The most frequently reported adverse events in the lithium group were headaches (60.8%), nausea (39.2%), somnolence (27.5%), tremor (27.5%), and emesis (25.5%), whereas the most commonly reported adverse events in the quetiapine group were somnolence (63.8%), headaches (55.2%), tremor (36.2%), dizziness (36.2%) and nausea (31%). Participants treated with quetiapine reported significantly more somnolence (p < 0.001) and dizziness (p < 0.05). No other reported side effects were significantly different between groups. The number of patients who discontinued the study owing to an adverse event was small in both treatment arms (lithium n = 5 and quetiapine n = 4). No pregnancies and no deaths were recorded in the study.
Weight and BMI
Patients in the quetiapine group had a greater increase in body weight compared with those in the lithium group (EMM +3.7 kg vs. +1.3 kg, p = 0.02). In addition, change in standardized BMI z-score was greater in the quetiapine group (fixed effect of treatment group F = 10.16, df = 153.36, p = 0.002). The EMM for BMI z-score change also revealed a treatment group-by-week interactive effect (p = 0.05) and a treatment group-by-baseline BMI z-score that fell short of statistical significance (p = 0.064). Moreover, post hoc testing on EMM revealed there was a significant within-group effect for change in BMI z-score in the quetiapine group (F = 7.15, df = 477.76 p < 0.001) but not in the lithium group (F = 1.45, df = 4866.44, p = 0.183). In addition, according our linear mixed effects model, a subject with a baseline BMI on the age- and sex-adjusted 50th percentile randomized to quetiapine would on average finish the 6-week follow-up on the 62.26th percentile for BMI (95% CI: 58.7 to 65.9th percentile), whereas a subject with a baseline BMI on the 50th percentile randomized to lithium would on average finish the 6-week follow-up with a BMI in the 53.15th percentile (95% CI: 48.32 to 57.93th percentile). This between-group difference was statistically significant (F = 9.15, df = 432.74, p = 0.003).
Laboratory and electrocardiogram
There were no statistically significant differences between groups in baseline laboratory values. Changes from baseline to endpoint in laboratory values are given in Table 2. Several within-group significant changes from baseline for an uncorrected p-value of <0.05 were identified. For participants treated with lithium there was a significant increase from baseline to endpoint in TSH, platelets, and white blood cell (WBC) and a significant decrease in blood urea nitrogen, red blood cell (RBC), and hemoglobin. Meanwhile, participants treated with quetiapine displayed a significant increase from baseline to endpoint in triglycerides and low-density lipoprotein/high-density lipoprotein (LDL/HDL) ratio and a decrease in calcium, HDL, RBC, hemoglobin, and WBC. None of these changes were clinically significant. Statistically significant between-group differences in baseline to endpoint changes were detected for calcium, LDL/HDL ratio, TSH, and WBC (uncorrected p < 0.01).
Mean Change from Baseline to Week 6 (Last Observation Carried Forward) in Laboratory Tests
Wilcoxon rank sum test.
Significant within group change from baseline at uncorrected p < 0.05.
95% CI, 95% confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein; RBC, red blood cell; WBC, white blood cell.
The mean change from baseline in QT interval using the Fridericia correction (QTcF) was greater for the lithium group than for the quetiapine group (13.6 milliseconds, 95% CI: 7.7 to 19.5 milliseconds vs. −3.8 milliseconds, 95% CI: −8.0 to 0.4; Wilcoxon rank sum p < 0.01). No participant in either treatment group had a postbaseline QTcF ≥460 milliseconds or a change in QTcF ≥60 milliseconds.
Predictors of treatment response
Participants with a family history of bipolar disorder (OR = 2.9; 95% CI: 1.3 to 6.8), with no prior psychopharmacological treatment (OR = 3.4; 95% CI: 1.2 to 9.8) and more specifically with no history of stimulant use (OR = 2.7; 95% CI: 1.2 to 6.1) were more likely to achieve response. No significant associations with treatment response were identified for comorbid psychiatric diagnosis, psychosis, age, and age of onset. The association of family history, prior psychopharmacological treatment, and prior treatment with stimulant medications was only seen in the lithium group. Patients treated with lithium who had a family history of bipolar disorder were four times more likely to meet criteria of treatment response than subjects treated with lithium who did not have a family history of bipolar disorder (OR = 4.1; 95% CI: 1.2 to 13.6). In addition, patients treated with lithium who had no history of prior treatment with stimulant medication were five times more likely to meet criteria for treatment response compared with patients treated with lithium who had a history of treatment with stimulant medication (OR = 4.9; 95% CI: 1.5 to 15.9). Meanwhile, for patients receiving quetiapine, no statistically significant differences in treatment response were seen for family history of bipolar disorder and history of treatment with stimulant medication.
Discussion
In this randomized, double-blind, head-to-head, 6-week clinical study of children and adolescents with a current manic or mixed episode, treatment with either lithium or quetiapine led to clinical improvement as determined by the primary efficacy measures. A majority of participants in this study experienced a clinical response; however, less than half of the subjects in this study achieved the a priori definition of remission. The head-to head comparison of both treatment groups showed quetiapine was associated with a statistically significant greater rate of response and overall symptom reduction compared with lithium. Differences in symptom reduction were observed as early as week 1. To our knowledge, this is the first study to compare lithium with quetiapine in a randomized and double-blind head-to-head trial.
Our study adds to the existing literature regarding efficacy of pharmacological treatments for children and adolescent bipolar disorder during a manic or mixed episode. Decrease in symptom scores and rates of response and remission observed in our study are similar to those reported in other clinical trials of lithium and quetiapine. In a randomized, double blind, placebo-controlled trail of children and adolescents with bipolar mania with comparable primary outcomes, treatment with lithium lead to a mean decrease in YMRS score of −11.8 and a response rate of 32% (Findling et al. 2015). Similarly, treatment with quetiapine in a 3-week randomized double-blind placebo-controlled trial led to mean YMRS reductions of −14.3 and −15.6 and response rates of 55% and 56% at doses of 400 and 600 mg daily, respectively (Pathak et al. 2013).
Overall, evidence seems to suggest second-generation antipsychotics (SGAs) may be superior to conventional mood stabilizers and lithium in treating bipolar disorder. A well-designed meta-analysis found a larger effect in symptom score reductions for SGAs compared with mood stabilizers (Liu et al. 2011). In addition, in another head-to-head clinical trial the SGA risperidone was superior to lithium in response rates (68.5% vs. 35.6%, p < 0.001) (Geller et al. 2012). Direct head-to-head comparison of lithium versus quetiapine in the treatment of adult patients with an acute manic/mixed episode have yielded mixed results with one study finding no difference between medications (Bowden et al. 2005) and another study finding quetiapine to be slightly superior to lithium (Li et al. 2008). In our study, a larger proportion of subjects treated with quetiapine achieved treatment response compared with subjects receiving lithium. Separation between groups in symptom score was evident as early as 1 week; however, after week 4 differences were no longer statistically significant. Although quetiapine was superior to lithium in reduction of symptoms as measured by the YMRS, the mean difference was just below two points, which amounts to a small effect size favoring quetiapine. In addition, treatment groups did not differ in terms of rates of remission. Moreover, lithium and quetiapine did not differ in the secondary measures of efficacy, including those based on clinical global impressions of clinician's blinded to treatment group. Furthermore, comparing only those subjects who completed the 6-week treatment period (total n = 77; lithium n = 30 and quetiapine n = 47), no statistically significant differences in change in YMRS score, response and remission rates were observed. Taking this information as a whole suggests quetiapine superiority to lithium is at best marginal and probably found mainly in the earlier weeks of treatment.
In addition, we found that family history of bipolar disorder and no previous psychostimulant use was associated with treatment response. More specifically, among patients receiving lithium, those with a family history of bipolar disorder were more likely to achieve respond in this 6-week clinical trial. This finding is consistent with prior studies that have indicated family history of bipolar disorder is a clinical predictor of response to lithium in patients with bipolar disorder (Hui et al. 2019). Furthermore, in our study lithium appeared to be less effective in individuals with a prior psychostimulant use. This result is also consistent with previous findings; a subsequent analysis of a clinical trial comparing lithium and risperidone (Geller et al. 2012), lithium was less effective in the presence of ADHD comorbidity and stimulant use (Vitiello et al. 2012).
In our study, lithium and quetiapine were generally well tolerated. However, there were some differences in terms of side effects, laboratory values, and EKG variables. We found that lithium and quetiapine had similar rates of treatment emergent side effects. In our study, only sedation and dizziness were side effects that differed between treatment groups, with higher rates reported in those treated with quetiapine. In addition, in this study we found that patients treated with quetiapine experienced on average greater increase in body weight and BMI compared with those receiving lithium. The weight gain observed in our study is similar to previous clinical studies of similar duration, diagnosis, and age population for both quetiapine (DelBello et al. 2006) and lithium (Findling et al. 2015). Moreover, regarding change in BMI we found an interaction that fell below standard statistical significance suggesting patients with higher baseline BMI may be at greater risk of greater increases in BMI when treated with quetiapine compared with lithium. Changes in laboratory values also differed between the two treatment groups. Subjects treated with lithium showed larger increases in TSH and WBC, whereas subjects treated with quetiapine showed an increasing LDL/HDL ratio. Moreover, subjects treated with lithium had on average larger increases in the QTcF interval compared with quetiapine; yet, this did not amount to any clinically significant increase QT prolongation.
The completion rate in our study showed a significant difference, with subjects treated with lithium more likely to drop out or be lost to follow-up. Completion rates for quetiapine were similar to other clinical trials of children and adolescents with acute mania (Kowatch et al. 2000; DelBello et al. 2002). Of note, other studies using lithium in children and adolescents with bipolar mania dropout rates have been high (Kafantaris et al. 2003, 2004; Pavuluri et al. 2004; Findling et al. 2015). One possible explanation in dropout rates between groups may be a slower response to lithium. A slower response in lithium is consistent with previous findings. In a previous randomized double-blind placebo controlled clinical trial for children and adolescents with acute mania, separation from placebo was observed after 5 weeks of treatment (Findling et al. 2015), whereas in a similar study, quetiapine separated from placebo within the first week of treatment (Pathak et al. 2013). In our study, differences between groups in change from baseline YMRS scores were longer evident after 4 weeks of treatment.
Limitations
Several study limitations should be noted. There was a higher drop off rate in the group randomized to receive lithium; analysis was conducted with an intent-to-treat design with the LOCF. Although quetiapine was statistically superior to lithium, not only was this difference small with regard to effect size but the difference between groups diminished with time. It is possible that the loss of a statistical significant difference between groups over time is related to the differences in dropout rates. Higher dropout rates in the lithium group may have been influenced by a slower response to treatment. In addition, although no significant difference between groups was detected regarding dropout because of adverse events, it is possible that the differences may also be related to the tolerability of lithium.
Conclusion
This head-to-head treatment study of children and adolescent with early course bipolar disorder in an acute manic or mixed episode showed that both lithium and quetiapine may be effective in reducing symptoms of mania and at least in a portion of patients who achieve remission. Quetiapine appeared to be superior to lithium in terms of effect size and achieving response; however, these differences were marginal and because of differences in dropout rates, they may represent a better tolerability of quetiapine.
Footnotes
Clinical Significance
In this study, we aimed to compare the efficacy and tolerability of lithium versus quetiapine for early course bipolar disorder in a manic or mixed episode using a head-to-head randomized, double-blind, clinical trial design. We found that both lithium and quetiapine may be effective in reducing symptoms of mania and in at least in a portion of patients, achieve remission. Quetiapine appeared to be statistically superior to lithium; however, the differences were marginal and perhaps mostly related to the initial period of treatment. Differences in drop-out rates and side effects suggest quetiapine may be better tolerated than lithium.
Disclosures
L.R.P. has received research support from Eli Lilly, Pfizer, Otsuka, Novartis, Lundbeck, Sunovion, AbbVie, Martek and Shire. J.R.S. has received research support from Allergan, Neuronetics, Otsuka Pharmaceutical Co., Ltd., National Institute of Mental Health, National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, and the Yung Family Foundation; receives royalties from Springer Publishing Co., UpToDate and has received honoraria from CMEology and Neuroscience Education Institute; has received material support from and provided consultation to Myriad Genetics. C.M.A. has received research support from National Institute of Mental Health, Johnson and Johnson, Merck, Forest, Otsuka, Purdue, Takeda, Pfizer, Shire, Sunovion, and SyneuRx; has received consulting/honoraria from Sunovion. J.A.W. has received research support from National Institute of Mental Health. M.P.D. has received research support from National Institute of Mental Health, National Institute of Child Health and Human Development, Amylin, Eli Lilly, Pfizer, Otsuka, GlaxoSmithKline, Merck, Martek, Novartis, Lundbeck, Pfizer, Sunovion, and Shire; has received consulting/advisory board/honoraria/travel support from Pfizer, Lundbeck, Sunovian, Supernus, and Otsuka. All other authors have no disclosures. The authors declare no competing interests.