
Abstract
Objectives:
Maternal 15q11-13 duplication syndrome (dup15q) is one of the most frequently observed and penetrant genetic abnormalities associated with autism spectrum disorder (ASD), and commonly presents with psychiatric symptoms and seizures. Although carbamazepine has been reported as effective in managing comorbid seizures in dup15q, it has not been reported to be used as a mood stabilizer in this population.
Methods:
We retrospectively reviewed the charts of five consecutive patients presenting with previously diagnosed dup15q and ASD seeking treatment for psychiatric symptoms and, in four of the patients, seizures. These were the only patients with dup15q treated with carbamazepine in the Neurodevelopmental Psychopharmacology Clinic at the University of Illinois at Chicago during the review period.
Results:
During treatment, carbamazepine was found to be more effective than other mood stabilizers in all five patients, and in one case a better antiepileptic. Symptoms consistent with bipolar mood disorder such as hyperactivity, impulsivity, irritability, mood lability, intrusiveness, and pressured speech were improved with carbamazepine in combination with other psychotropic medications. This improvement was greater than with other mood stabilizers, including oxcarbazepine, valproate, and lamotrigine. In one case, valproate paradoxically worsened symptoms. In three cases, anxiety was improved with carbamazepine when used in conjunction with other medications targeting anxiety.
Conclusions:
In treating five patients with dup15q, carbamazepine more effectively stabilized mood-related symptoms than alternative treatments. Prospective randomized controlled trials are necessary to confirm this observation.
Introduction
Maternal 15
Isodicentric chromosomes are found in ∼80% of patients and interstitial duplications are found in the remaining ∼20% of patients (Finucane et al. 2016). Dup15q syndrome has been associated with epilepsy, intellectual disability, hypotonia with motor delays, language impairment, social impairments, and ASD. Symptoms in patients with the isodicentric abnormality are generally more severe and there is a higher chance the patient will develop epilepsy (Distefano et al. 2016). Psychiatric symptoms, including aggression and hyperactivity, have been described as significant comorbidities in dup15q (Battaglia et al. 2010; Al Ageeli et al. 2014).
Mood disorders are common psychiatric comorbidities reported in individuals with ASD (Lord et al. 2018). Mood changes can go unnoticed in some individuals with ASD because of an insufficiency in language skills needed to express their emotions, to describe changes in mood, or to verbalize biological symptoms of depression. Although typical manic symptoms, such as overspending, gambling, and other pleasurable goal-oriented behaviors, may not be present, behavior problems may be present in the form of aggression, intrusiveness, restlessness, or general agitation (Lord et al. 2018).
Mood symptoms may overlap with anxiety, which is highly prevalent in patients with bipolar disorder. About half of patients with bipolar disorder are at risk of developing an anxiety disorder in their lifetimes, and a third of them will manifest these disorders at any point of time (Spoorthy et al. 2019). Finally, these mood and anxiety symptoms may be difficult to differentiate in patients with impaired communication skills.
Carbamazepine is prescribed in disorders, including epilepsy, bipolar mood disorder, and neuropathic pain. Carbamazepine has several sites of action, with voltage-dependent sodium channels as the main target. Owing to its multifaceted effects on the brain and nervous system, the precise mechanism of action for carbamazepine in each condition has yet to be established (Ambrósio et al. 2002). Carbamazepine has been reported as effective in managing comorbid seizures in dup15q (Conant et al. 2014). In this article, we describe the role of carbamazepine for use in mood stabilization in a series of patients with dup15q, ASD, and comorbid bipolar disorder referred for assessment for psychopharmacological treatment.
Methods
We retrospectively reviewed the charts of five consecutive patients presenting with previously diagnosed maternal dup15q, ASD, and comorbid bipolar disorder, and in four of the patients, seizures. These were the only patients with dup15q in the clinic from July 2005 to November 2018 treated with carbamazepine, the timeframe in which their medical records were reviewed. Patients were diagnosed by Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria and followed by Dr. Fedra Najjar and Dr. Edwin Cook in the Neurodevelopmental Disorder Psychopharmacology Clinic at the University of Illinois at Chicago.
In several cases, this included review of treatment at a previous university clinic by the same providers. The patients were numbered chronologically based on their presentation to the clinic. The number of clinic visits and phone calls were tallied for each patient while taking and not taking carbamazepine. The study protocol was reviewed and approved for IRB exemption by the University of Illinois Chicago Office of Protection of Research Subjects. Verbal informed consent was obtained from the patients' legal guardians for publication of this case series.
Results
Patient #1
Patient #1 is a 45-year-old female who has been followed as an outpatient for 27 years. Haloperidol was trialed by a previous provider for self-injurious behavior (SIB) with no improvement. The patient had comorbid seizures well controlled with 100 mg TID of carbamazepine. Patient had the following comorbid behavioral symptoms: mood lability, SIB, hyperactivity, and aggression. She exhibited decreased severity of symptoms with carbamazepine for hyperactivity and aggression and paroxetine for SIB. She has had no major side effects with her current medications, including no neutropenia.
Patient #2
Patient #2 is a 23-year-old male who has been followed for 17 years and who does not have comorbid seizures. Before puberty, he had attention-deficit/hyperactivity disorder (ADHD), combined presentation but during adolescence, he developed mood lability with episodes of increased irritability and impulsivity. He has the following comorbid behavioral symptoms: hyperactivity, impulsivity, irritability, and anxiety. He has had improved severity of psychiatric symptoms with 800 mg bis in die (BID) of carbamazepine for hyperactivity, impulsivity, irritability, and anxiety. He has no hyponatremia or neutropenia on his current medications. Before carbamazepine, valproate had been trialed but led to paradoxical worsening of mood-related symptoms.
Oxcarbazepine and aripiprazole were then started with mild improvement. Oxcarbazepine was cross-titrated with lamotrigine leading to further improvement of symptoms but dose-related tics. Lamotrigine was then discontinued and replaced with carbamazepine with improved symptoms and a decrease in tics. While taking carbamazepine, citalopram and fluoxetine were trialed for continuing anxiety and mood problems leading to no improvement and an increase in activity, respectively. Mixed amphetamine/dextroamphetamine salts XR and dexmethylphenidate XR were trialed before initiation of carbamazepine therapy without improvement in hyperactivity. Guanfacine ER, atomoxetine, and mirtazapine were also unsuccessfully trialed for hyperactivity while on carbamazepine. He has recently been restarted on low dose aripiprazole.
Patient #3
Patient #3 is a 34-year-old female who has been followed in the clinic for 13 years. She has comorbid seizures currently controlled with carbamazepine. She has had the following comorbid behavioral symptoms: hyperactivity, mood lability, intrusiveness, and pressured speech. She has had a decreased severity of symptoms with 800 mg BID of carbamazepine along with risperidone. She has had drooling due to risperidone, which is currently controlled with benztropine. She has had neutropenia (lowest absolute neutrophil count [ANC] 1200 cells/μL) that prompted attempts to switch to another anticonvulsant/mood stabilizer by another provider, which led to status epilepticus and worsened behavior.
Her seizures were stabilized with oxcarbazepine along with risperidone, but she continued to have worsened psychiatric symptoms. Oxcarbazepine was cross-titrated to carbamazepine with improved symptoms and continued seizure control along with neutropenia. Because of the neutropenia, valproate and oxcarbazepine trials were repeated but less effective than carbamazepine. Both lamotrigine and lithium were prescribed but discontinued due to adverse effects (rash and severe polyuria/polydipsia, respectively). Carbamazepine was then restarted with improvement in mood stability, including irritability.
Patient #4
Patient #4 is a 20-year-old female who has been followed in the clinic for 12 years. Patient has myoclonic epilepsy, which has been controlled with clobazam. She has had the following comorbid behavioral symptoms: anxiety, hyperactivity, mood lability, and impulsivity. She has had decreased severity of psychiatric symptoms with 600 mg BID of carbamazepine for hyperactivity, mood lability, and impulsivity, citalopram for anxiety, aripiprazole for control of irritability and impulsivity, and methylphenidate for hyperactivity. Citalopram was continued from her previous treatment regimen without carbamazepine, and aripiprazole was started shortly after beginning carbamazepine therapy.
Her dose of carbamazepine was not increased due to mild neutropenia (lowest ANC 1200 cells/μL). She has had no other major side effects on her current medications. Oxcarbazepine was initially trialed but did not improve symptoms. Carbamazepine was started with an improvement of symptoms. Her seizures worsened so carbamazepine was stopped for clobazam by neurology. She had an acute anxiety attack with dangerous and impulsive behavior shortly thereafter, which led to admission to the hospital. Carbamazepine was restarted with another admission for anxiety before it reached therapeutic levels. She has had no admissions since that time.
Patient #5
Patient #5 is a 21-year-old male who has been followed for 12 years. He has a history of comorbid grand mal epilepsy that evolved into juvenile myoclonic epilepsy with seizures controlled with valproate and lamotrigine prescribed by neurology. He has had the following symptoms: mood lability, hyperactivity, aggression, and short duration of sleep. He is currently on guanfacine ER and amphetamine/dextroamphetamine mixed salts XR for hyperactivity and carbamazepine, which has reduced aggression and short duration of sleep at 800 mg/day divided in three doses. He has had no major side effects with his current medications, including no neutropenia.
Discussion
This report shows that in five patients with a maternal isodicentric chromosome associated with dup15q, carbamazepine was found to more effectively treat bipolar disorder when compared with alternative mood stabilizers, including oxcarbazepine, valproate, and lamotrigine (Figure 1). In addition, in one patient carbamazepine provided improved control of epileptic seizures relative to other antiepileptic drugs.
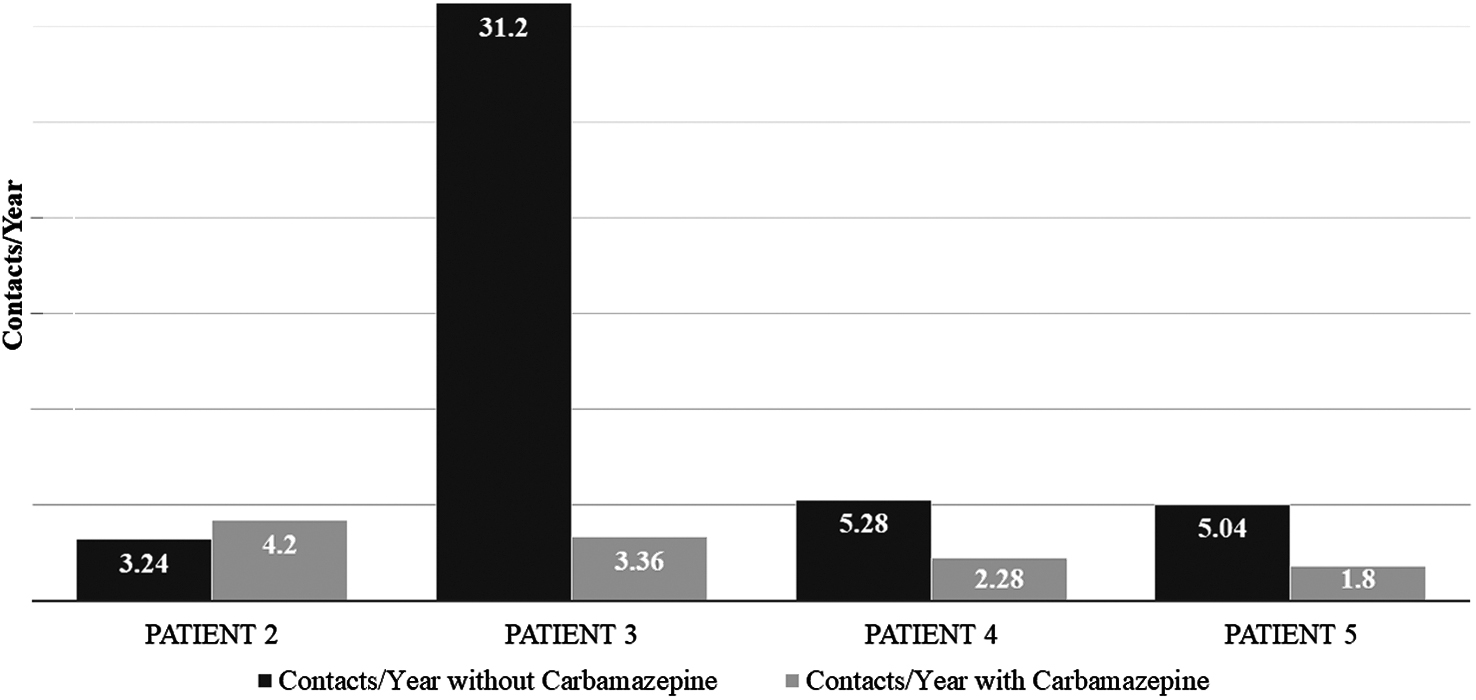
Contacts with and without carbamazepine. *Patient 1 was omitted because treatment was initiated in 1991 and contact information is not available.
Bipolar disorder tends to present in adolescence and early adulthood (Rowland and Marwaha 2018). Although the criteria for bipolar disorder are universal in all individuals and across age groups, the expression of the signs and symptoms could vary depending on the developmental level and verbal abilities of the individual. Some of the symptoms observed in this study, such as hyperactivity and irritability, are common for both ADHD and bipolar disorder. Anxiety disorders are highly prevalent with bipolar disorders (Spoorthy et al. 2019), and in these patients it is likely that there was an overlap of anxiety symptoms that were worsened with co-occurring mood episodes.
The signs and symptoms of bipolar disorder can be attributed to ADHD and share clinical manifestations of anxiety in children and adolescents. These symptoms often become more consistent with bipolar disorder after puberty, as for two of the cases (#2 and #4) that were followed before and after puberty (Goldstein and Birmaher 2012).
In this report, the patients' psychiatric symptoms were variable, which is consistent with previous studies. ASD and hyperactivity were noted in all patients, both of which have previously been observed at high rates in dup15q (Al Ageeli et al. 2014; Battaglia 2021). Each of the patients reported in this case series had mood instability, and this includes all of the patients with dup15q and mood instability presenting to the clinic from 2005 to 2018. Thus, all patients who presented to the clinic with dup15q ad mood instability in this time frame were treated with carbamazepine. Carbamazepine was a better mood stabilizer with improvement in symptoms consistent with bipolar disorder; however, all patients required additional medications for effective management.
Notably, anxiety, a symptom frequently associated with mood disorders, was improved in cases #2, 3, and 4 but required treatment with other medications (Table 1). Also, sustained mood stability may have a positive effect of comorbid anxiety symptoms. The refractory nature of symptoms in these patients is consistent with previous findings, and may have been exacerbated in this study by the more severe presentation of patients with isodicentric chromosomes when compared with those with interstitial duplications (Al Ageeli et al. 2014; Distefano et al. 2020). This underscores the difficulty in treating the psychiatric symptoms related to isodicentric dup15q.
Unsuccessful Psychopharmacotherapies and Current Medications
Of note, the average age of the participants and length of follow-up in this study were 28.6 and 16.2 years, respectively. This is significantly higher than previous studies on dup15q (Battaglia et al. 2010; DiStefano et al. 2020). To our knowledge there are no studies investigating the presentation of dup15q in adults older than 45, the oldest patient in our study.
Dup15q has also been associated with seizures and four of the five patients in this study had epilepsy. The efficacy of carbamazepine as an antiepileptic in dup15q has been explored by Conant et al. (2014). They surveyed family members of individuals with dup15q and found carbamazepine to be useful in the treatment of seizures in this population. In addition, their findings suggested epilepsy in dup15q is more likely to be refractory to medication when compared with the general population. This emphasizes the importance of communication between psychiatrists and neurologists to ensure optimal treatment management, especially when considering the overlap between mood stabilizers and antiepileptics.
Carbamazepine is associated with neutropenia, which was also observed in two patients while taking the medication (Sobotka et al. 1990). Although the participants of this study were asymptomatic, it is important to monitor for neutropenia while on carbamazepine.
Lithium treatment was limited by difficulty managing polyuria and has the potential to worsen seizures in dup15q. Worsening of symptoms experienced by patient #2 from valproate may be related to epigenetic effects, as studies have demonstrated alteration of neuronal gene expression with valproate (Mello 2021). It is uncertain why oxcarbazepine or lamotrigine was not as effective as carbamazepine.
This study was a case series and was thus limited based on sample size. Rating scales were not collected over the several years of treatment. In addition, this study was not blinded and did not have a control group with which to compare carbamazepine treatment. Over many years, these patients had different school placements, therapies, and medications making it less certain whether the benefits were due to carbamazepine alone, other interventions, or interactions between therapeutic modalities. These limitations could be addressed in future research involving a randomized control trial focused on the efficacy of carbamazepine.
However, it can often be difficult conducting randomized controlled trials for a psychiatric indication in a specific rare disorder. With some exceptions, trials in genetically defined disorders such as Fragile X syndrome and Phelan McDermid syndrome target symptoms common to everyone with the disorder, thus increasing sample size (Kolevzon et al. 2014; Zwanenburg et al. 2016; Luu et al. 2020; Rajaratnam et al. 2020).
Conclusions
In treating five patients with maternal isodicentric 15q11-13 duplication syndrome, carbamazepine more effectively stabilized mood than alternative treatments. The properties of carbamazepine as an antiepileptic and mood stabilizer make it an option for treatment of bipolar disorder in dup15q syndrome.
Clinical Significance
Dup15q is associated with ASD as well as significant risk for epilepsy and comorbid psychiatric symptoms, but more research needs to be done to elucidate optimal treatment strategies. This report proposes treatment with carbamazepine as a potential step toward improved management of mood instability in dup15q.
Footnotes
Acknowledgments
We thank all the participants and their families who participated in this study.
Disclosures
No competing financial interests exist.