
Abstract
Objectives:
This systematic review provides an overview of full economic evaluations of attention-deficit/hyperactivity disorder (ADHD) treatments, evaluates their outcomes, and highlights gaps in the literature.
Data Sources:
Electronic databases were searched for full economic evaluations of ADHD treatments for children, adolescents, or adults published in English or Dutch.
Results:
Twenty-nine studies met the inclusion criteria. Almost all studies that compared medication or psychosocial treatment to no treatment, placebo, or care as usual indicated that medication and psychosocial treatment were cost-effective compared to the control group. Stimulant treatment appeared to be cost-effective for the treatment of ADHD in children and adolescents. Only few studies focus on treatments in adults and psychosocial treatments and the number of studies with long time horizons and without industry funding is limited.
Conclusions:
Despite the rising interest in cost-effectiveness, this systematic review shows that more cost-effectiveness research of higher quality is warranted to aid in the optimal use of available treatments and resources for individuals with ADHD. Specifically, more studies should focus on treatments in adults and psychosocial treatments, and more studies with long time horizons and without industry funding are warranted. Nevertheless, we can conclude that treating ADHD is generally cost-effective compared to no treatment.
PROSPERO: CRD42017060074. Available from:
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is associated with high personal, societal, and governmental costs across all ages (Doshi et al. 2012; Le et al. 2014; Sciberras et al. 2020). The worldwide prevalence of ADHD is estimated to be around 5.3% (Polanczyk et al. 2007). This high prevalence results in a burden of disease of approximately half a million disability-adjusted life years* (DALYs) worldwide (Erskine et al. 2014), as well as high societal costs: in Europe, annual ADHD-related costs are estimated between €1041 and €1529 million (Le et al. 2014). According to Doshi et al. (2012), costs in the United States range from $143 to $266 billion. Effective treatments (such as behavioral and medical treatment) can reduce symptom severity and alleviate impairment associated with ADHD (Groenman et al. 2021). However, since health care budgets are limited (The Commonwealth Fund 2020), it is imperative that health care funds are allocated efficiently: covering treatments in such a way that the highest number of individuals receives the best possible health benefits. Economic evaluations of ADHD treatments may help policy makers in reaching an efficient allocation of funds and contribute to improvement of ADHD-related impairments within the limits of available resources. Consequently, in this systematic review, we aim to provide an overview of the cost-effectiveness of treatments for individuals with ADHD.
Treatment of ADHD can result in better outcomes of the core symptoms of ADHD and accompanying problems such as criminality, problems with occupation, substance use, obesity, and suicidal behavior (for review see Franke et al. 2018). This in turn might lead to lower costs associated with ADHD.
Treatment options for individuals with ADHD include pharmacological, behavioral (i.e., psychosocial), or combined interventions (American Academy of Pediatrics 2011; NICE 2018c). While some guidelines recommend behavioral interventions as first-line treatments (American Academy of Pediatrics 2011), pharmacotherapy is most often used (Pelham et al. 2007). Common psychosocial interventions are behavioral treatments such as parent/teacher training, skills training, and behavioral peer interventions (DuPaul et al. 2020). Commonly used medications for ADHD can be subdivided into stimulants (e.g., methylphenidate immediate release [IR] or extended release [ER] and [dex]amphetamine) and nonstimulants (e.g., atomoxetine and guanfacine).
Although previous reviews on the cost-effectiveness of treatment in ADHD have been performed (Wu et al. 2012; Catalá-López et al. 2013; Klora et al. 2016), they had some important shortcomings. While Wu et al. (2012) focused on full economic evaluations (i.e., those comparing both cost and effectiveness of two or more comparators). they only included pharmacological treatments and not psychosocial interventions. The systematic review by Catalá-López et al. (2013) also only focused on pharmacological treatments (i.e., methylphenidate and atomoxetine) for ADHD in children, which were available in Spain at that time. Both reviews (Wu et al. 2012; Catalá-López et al. 2013) did not include studies on adult ADHD, as these were not available at that time.
While there are now studies on adult treatments, a recent systematic review (Sampaio et al. 2021) did not include these, and, importantly, included literature from a very limited time period (2010–2020). Although data on adult treatments were included in the systematic review of Klora et al. (2016), this review again only focused on pharmacological treatments. Furthermore, the quality of identified studies was not assessed, which may hamper interpretation of the outcomes.
Consequently, to identify which treatments for ADHD are cost-effective, in this review, we included studies on cost-effectiveness of all interventions (i.e., both pharmacological and nonpharmacological) for individuals with ADHD in all age groups and assessed the quality of all included studies. Furthermore, we notify important gaps in the literature and provide directions for further research.
Methods
This systematic review has been registered in the PROSPERO database with registration number CRD42017060074 (available from
Economic evaluations
Full economic evaluations contrast two comparators (either active interventions or no treatment/placebo) by investigating their differences in costs and effects. Which costs and effects are included in the evaluation depends on the perspective of the evaluation. For example, an economic evaluation from a health care perspective will include health care costs, but not productivity losses due to missed work. Effects can be measured using an ADHD-specific outcome, such as ADHD symptom severity, as is done in cost-effectiveness research, or a generic measure of health gain, such as the EQ-5D (EuroQol five dimensions), which generates an outcome in quality-adjusted life years (QALYs), as is done in cost-utility research (please see Drummond et al. 2015 for an in-depth explanation). Depending on the measure used, economic evaluations are referred to as cost-effectiveness (disorder- or disease-specific outcome), or cost-utility (generic outcome † ) analyses.
Since empirical data often lack the longevity needed to study long-term costs and effects of an intervention, empirical results from trial data can be extrapolated using quantitative modeling techniques. Common modeling techniques are decision trees and Markov models, both of which generally use probabilities of having a certain health outcome or health state for treated and control group individuals and extend these over time to model long-term costs and effects of treatment and control.
Once the difference in costs and effects between two interventions has been assessed, both measures can be combined in a single incremental cost-effectiveness ratio (ICER): for example, costs per QALY or costs per 1-unit increase on an ADHD severity scale. Whether a certain ICER is desirable depends on the willingness to pay (WTP) for, for example, one additional QALY or a 1-unit increase on an ADHD questionnaire. If the ICER is lower than the WTP, the intervention is generally deemed to be cost-effective compared to its comparator. For a more detailed overview of the nature of cost-effectiveness research, see the Supplementary Appendix S1.
Inclusion and exclusion criteria
We included studies published in peer-reviewed journals on full economic evaluations that compared at least two treatments on the basis of costs and effects, where one of the treatments could also entail care as usual or no treatment (Drummond et al. 2015). The study population (all ages) was required to have a clinical score on an ADHD assessment tool and/or a clinical diagnosis of ADHD. The investigated treatments had to be aimed at reducing ADHD and/or behavioral symptoms and could include both pharmacological and nonpharmacological treatments.
Study protocols, methodological research, implementation research, reviews of economic evaluations, and cost of illness studies were excluded.
Literature search and study selection
Two authors (a combination of L.M.W., H.H.D., and A.P.G.) performed screening and study selection. Disagreement was resolved by consensus between the two authors performing the screening and selection. We used a two-step approach to identify relevant studies. We first searched the databases Medline, EMBASE, The Cochrane Library, PsycINFO, CINAHL, and CRD, using the following terms, their synonyms, and their hierarchical form (i.e., MESH terms): attention-deficit hyperactivity disorder, disruptive behavior disorders, randomized controlled trials, epidemiological studies, prognostic and prediction rule studies, qualitative studies, (pharma)economics, economic evaluations, costs, and QALYs. Second, we hand-searched literature lists of all selected studies, relevant systematic reviews, and meta-analyses to identify missing articles. A complete copy of the search terms per database is available on request. All searches were run up to January 2021 and limited to retrieve material published in English or Dutch.
Data extraction
Two authors (L.M.W. and H.H.D.) independently extracted the following data, using a predefined data extraction form: type of economic evaluation (i.e., trial based or model based), type of analysis (i.e., cost-effectiveness analysis or cost-utility analysis), study population, perspective (i.e., health care, societal or third-party payer), time horizon, comparators, effectiveness/utility measure, valuation of costs and results (i.e., how both costs and outcomes were measured and which data sources were used), sampling uncertainty (only in trial-based economic evaluations), parameter uncertainty, funding, and relations with pharmaceutical industry. For a summary of the extracted data, see Table 1.
Study Characteristics and Main Outcomes of Economic Evaluations of Attention-Deficit/Hyperactivity Disorder Treatments
Converted into 2019 Euros using purchasing power parities and corrected for inflation.
Mean quality score = 68.2%.
Data on sex distribution were not available.
MPH-OROS is a variant of MPH-ER.
Atypical antipsychotics in this study: aripiprazole, olanzapine, paliperidone, quetiapine, risperidone, ziprasidone.
Year of valuation: 2019.
AAPs, atypical antipsychotics; ADHD, attention-deficit/hyperactivity disorder; AMP, amphetamine; AQoL, assessment of quality of life; ATX, atomoxetine; CBT, cognitive behavioral therapy, CD, conduct disorder; CEA, cost-effectiveness analysis; CHQ, Child Health Questionnaire; CHU9D, child health utility 9D; CIS, Columbia Impairment Scale; CLAS, Child Life and Attention Skills; CSI, Child Symptom Inventory; CUA, cost-utility analysis; DALY, disability-adjusted life year; DAS, dextroamphetamine sulfate; DEX, dexamphetamine; DISC, Diagnostic Interview Schedule for Children; DOA, Directly Observed Attention; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, fourth edition; ECBI, Eyberg Child Behaviour Inventory; EQ-5D, EuroQol five-dimensions; ER, extended release; GXR, guanfacine extended release; HKD, hyperkinetic disorder; HUI, health utilities index; ICER, incremental cost-effectiveness ratio; IHR-QOL, index of health related quality of life; ICD, International Classification of Diseases; IR, immediate release; IY, incredible years; LDX, lisdexam-fetamine dimesylate; MBEE, model-based economic evaluation; MedMgt, medical management; MoH, ministry of health; MPH, methylphenidate; NFPP, New Forest Parenting Programme; NHS, national health perspective; NR, not reported; ODD, oppositional defiant disorder; OROS, osmotic-controlled release oral delivery system; PedsQL, Pediatric Quality of Life Inventory; PEM, pemoline; PFT, parent-focused treatment; PSS, personal social services; QALY, quality-adjusted life year; SA, sensitivity analysis; SD, standard deviation; SDQ, strengths and difficulties questionnaire SNAP, Swanson, Nolan and Pelham Rating Scale; SF-6D, short-form six dimension health inventory; TAU, treatment as usual; TBEE, trial based economic evaluation; TTO, time trade off; WTP, willingness to pay; WWP, Weiss-Peters Activity Rating Scale.
Quality assessment
We assessed the quality of each study with the Consensus Health Economic list (CHEC) (Evers et al. 2005), a questionnaire with 19 questions that is frequently used in systematic reviews of economic evaluations (Jensen et al. 2005; van Steenbergen-Weijenburg et al. 2010; Fitzpatrick and Floyd 2012). To improve the quality assessment of model-based evaluations, we added one question to the CHEC: “Are the structural assumptions and the validation methods of the model properly reported?.” Each item on the CHEC list was independently scored with 0 (no), 0.5 (suboptimal), or 1 (yes) by two authors (L.M.W. and H.H.D.). Disagreement was resolved by consensus. To account for differences in the maximum attainable score between trial- and model-based studies, scores were transformed into percentages of the maximum attainable score. That is, a higher percentage implies better conformity to the quality criteria of the CHEC list.
Outcomes
Primary outcomes were the reported cost-effectiveness and cost-utility estimates. All costs were converted in 2019 Euros, using purchasing power parities (Organisation for Economic Co-operation Development 2018). If the year of valuation of the included costs was unknown, the publication year was used to value the costs.
To assess whether interventions were cost-effective, we compared them to a WTP threshold. Such a WTP threshold generally describes how much an individual, or society, is willing to pay for one additional QALY. Following the median WTP estimate found in the literature by Ryen and Svensson (2015), we applied a WTP threshold of €29,000. ‡ Interventions with an ICER below this threshold are deemed cost-effective, while interventions with an ICER above this threshold are considered to not be cost-effective. This threshold also lies within the NICE (2012) recommendations of £20,000–£30,000 (€21,906.01 to €32,769.00) and is close to the recommendations of the Dutch Care Standards (Zwaap et al. 2015) of €20,000 (€21,943.89 in €2019). However, we also reported the ICERs (in €2019) of all included studies in Table 1, since WTP thresholds depend on many factors, such as the country in which the threshold is applied, gross domestic product, estimation method, and whether the increase in QALYs is mainly the result of an improvement in quality of life or an increase in lifespan (Ryen and Svensson 2015).
Results
Literature search and study selection
In total, 29 studies were included in the qualitative synthesis. The study selection process is presented in the PRISMA flow diagram (Fig. 1).
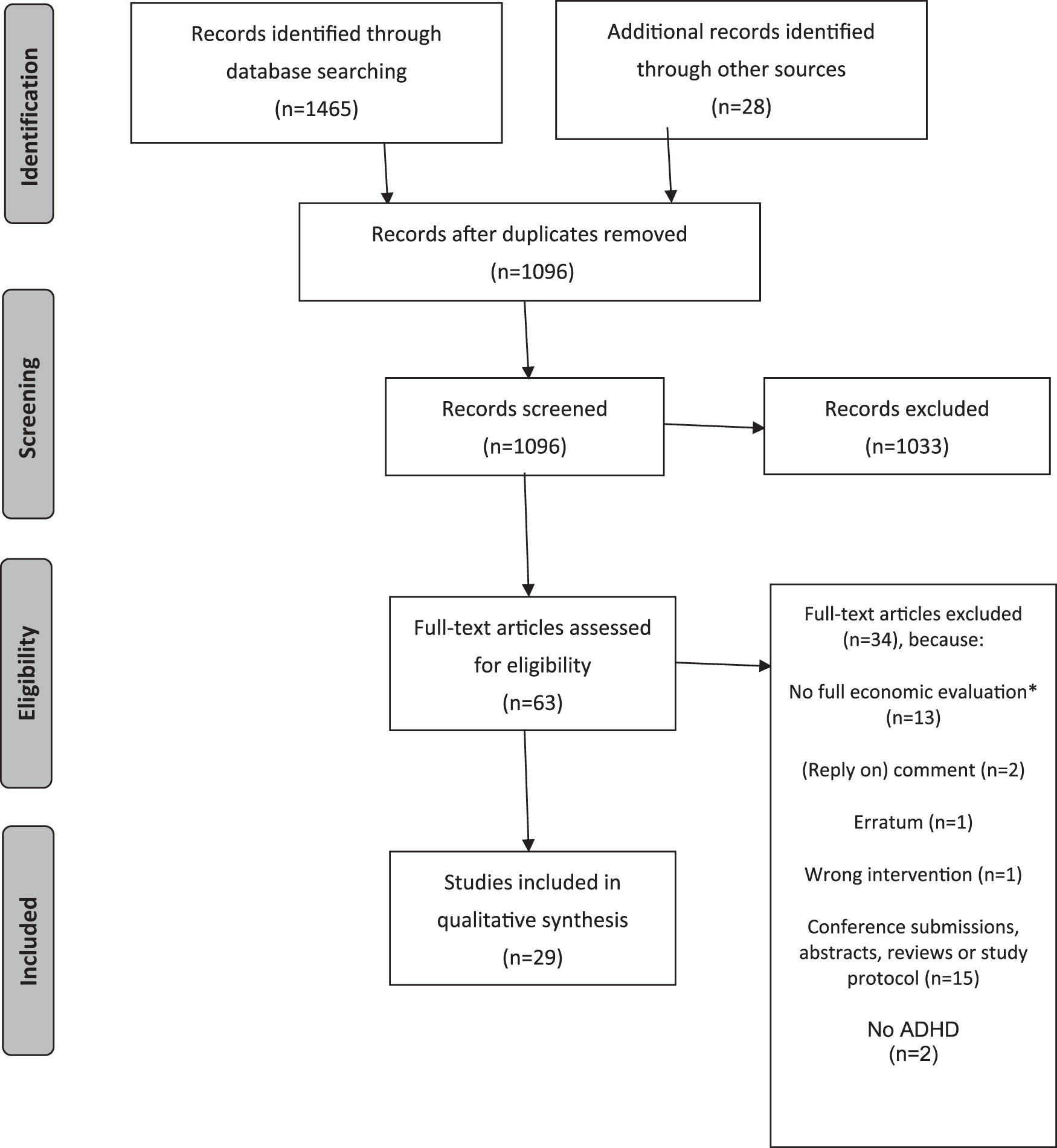
PRISMA flow diagram describing the systematic review process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data extraction
Characteristics of identified studies
An overview of the characteristics of the 29 included studies can be found in Figure 2. Please see Table 1 for a detailed summary of each study. Since one study contained three separate economic evaluations (NICE 2018b), these three evaluations are referred to separately in all figures and tables, aside from the PRISMA diagram. Most studies (90%) were performed on children, and most studies (55%) were performed on pharmacological interventions.
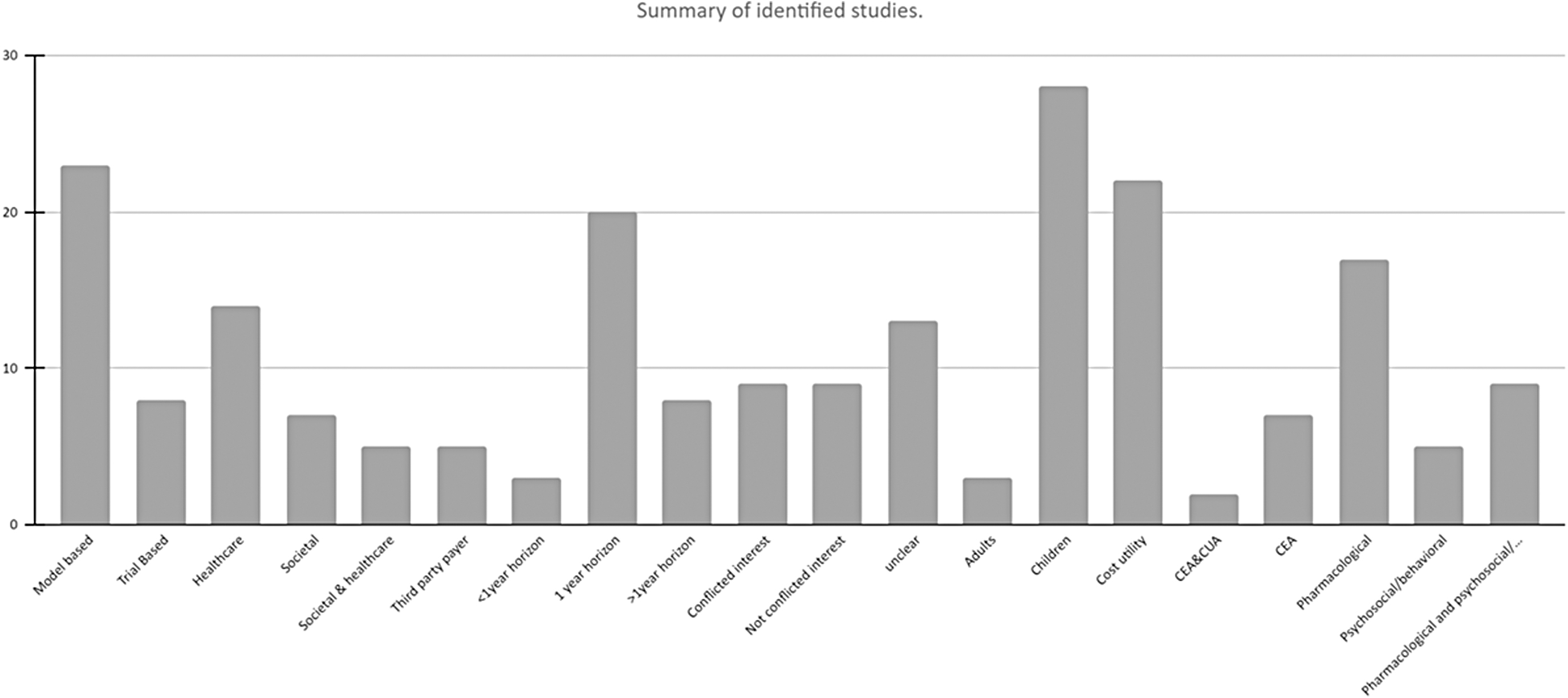
Number of evaluations that met the inclusion criteria with specific characteristics out of 29 included studies and 31 evaluations.
All studies performed a probabilistic sensitivity analysis and/or a deterministic sensitivity analysis to detect uncertainty. Table 1 provides detailed information about measurement and valuation of effects and costs.
Quality assessment
Quality
Overall CHEC results per study are provided in Supplementary Table S2, a summary per item per evaluation can be found in the supplements. The average percentage score of evaluations on the CHEC was 69% (95% CI: 52–87).
In general, evaluations scored high on the items related to the research question and objective (28 evaluations scored 1 and 3 evaluations scored 0.5), economic design (31 evaluations scored 1), time horizon (27 evaluations scored 1; 3 evaluations scored 0.5; and 1 evaluation scored 0), identification of relevant outcomes (30 evaluations scored 1 and 1 evaluation scored 0), and reporting of an ICER (29 evaluations scored 1; 1 evaluation scored 0; and for 1 evaluation, this question was not applicable).
Items with generally low scores on the CHEC related to the description of the model and assumptions (9 evaluations scored 1; 8 evaluations scored 0.5; 6 evaluations scored 0; and for 8 evaluations this question was not applicable), discussion on the generalizability of the results (7 evaluations scored 1; 6 evaluations scored 0.5; and 18 evaluations scored 0), conflicts of interest (6 evaluations scored 1; 2 evaluations scored 0.5; and 23 evaluations scored 0), and discussion on ethical and distributional issues (3 evaluations scored 1; 1 evaluation scored 0.5; and 27 evaluations scored 0).
Overview of specific treatment comparisons
Medication treatment
Cost-utility analyses in stimulant treatment
Two model-based studies compared methylphenidate IR to no treatment or placebo in children from a health care perspective in United Kingdom (Gilmore and Milne 2001) and Brazil (Maia et al. 2016). While these studies differed in time horizons (i.e., 6 years vs. 1 year, respectively) and were conducted in different countries and QALYs were valued in different ways, both found that methylphenidate was cost-effective compared to no treatment or placebo.
Three Dutch model-based studies (Faber et al. 2008; Schawo et al. 2015; van der Schans et al. 2015) compared methylphenidate IR to methylphenidate ER for children from a societal perspective for a period of 10–12 years. All studies found that methylphenidate ER was cost-effective for our WTP threshold, where two studies (Schawo et al. 2015; van der Schans et al. 2015) even found that methylphenidate ER dominated methylphenidate IR, in that methylphenidate ER yielded lower incremental costs and higher benefits. Using a third-party payer perspective for the United States and a time horizon of 1 year, Shah et al. (2017) also found that methylphenidate ER dominated amphetamine/dexamphetamine in adults. Thus, methylphenidate ER was more effective and less costly than the alternative. Consequently, these modeling studies indicate that methylphenidate ER might be a cost-effective treatment option compared to methylphenidate IR in children and amphetamine/dexamphetamine in adults.
Two model-based studies compared dexamphetamine with no treatment or care as usual for children with a 1-year time horizon (Donnelly et al. 2004; Narayan and Hay 2004). Narayan and Hay (2004) used a societal perspective in the United States and showed that (dex)amphetamine was cost-effective compared to no treatment. Moreover, methylphenidate IR was dominated by (dex)amphetamine, suggesting that (dex)amphetamine is also cost-effective compared to methylphenidate IR. Similarly, Donnelly et al. (2004) used a health care perspective in Australia and found an ICER of €3622/DALY for dexamphetamine and €13,250/DALY for methylphenidate IR. Hence, they also found that dexamphetamine appears to be more cost-effective than methylphenidate IR.
Zimovetz et al. (2016, 2018) compared the cost utility of lisdexamfetamine dimesylate and atomoxetine from a health care perspective in United Kingdom. While the two model-based studies differed in study population (children vs. adults) and time horizon (1 year vs. 5 years), both found that lisdexamfetamine dimesylate was cost-effective compared to atomoxetine, where Zimovets et al. (2018) even found that lisdexamfetamine dimesylate dominated both atomoxetine and methylphenidate ER, in that it was more effective and had lower costs than the alternative. Thus, this research showed that lisdexamfetamine dimesylate might be a cost-effective alternative to atomoxetine in children and adults. Moreover, in adults, there is also evidence that lisdexamfetamine dominates methylphenidate ER.
Similar to Zimovets et al. (2016), Hong et al. (2009) studied the cost-effectiveness of atomoxetine compared to methylphenidate IR and ER in stimulant-naive children in Spain using a Markov model and found that, while atomoxetine was cost-effective compared to methylphenidate ER, it was not cost-effective compared to methylphenidate IR.
Two model-based studies compared treatment algorithms for children and adolescents that included stimulants. King et al. (2006) compared methylphenidate IR, methylphenidate ER, dexamphetamine, atomoxetine, and behavioral therapy from a UK health care and personal social services perspective using a time horizon of 12 years. Although differences in QALY gains between the treatment strategies were small, the treatment strategy first-line dexamphetamine, followed by second-line methylphenidate IR, followed by third-line atomoxetine treatment, dominated all other treatment options. Cottrell et al. (2008) compared treatment algorithms containing atomoxetine, methylphenidate ER and IR, dexamphetamine, and no medication from a UK health care perspective with a 1-year time horizon for different populations of children with ADHD: stimulant-naive children, stimulant-nonresponding children, and children with contraindications for stimulant medication. First-line atomoxetine was cost-effective compared to other treatment algorithms for all populations.
Overall, most studies comparing stimulant to nonstimulant treatment in children found that stimulant treatment was cost-effective (Gilmore and Milne 2001; King et al. 2006; Narayan and Hay 2004; Maia et al. 2016; Zimovetz et al. 2016), and in adults (Zimovetz et al. 2018). The exception was atomoxetine, where evidence is mixed. While three studies found evidence in favor of cost-effectiveness of stimulants compared with atomoxetine (King et al. 2006; Zimovetz et al. 2016, 2018), Hong et al. (2009) found that methylphenidate IR is cost-effective compared to atomoxetine, but methylphenidate ER is not. In addition, Cottrell et al. (2008) found that treatment algorithms with first-line atomoxetine were cost-effective. Generally, in children and adolescents, research on cost-effectiveness of stimulant treatment compared to other stimulant treatment is mixed and limited, although methylphenidate ER appears to be cost-effective when compared to methylphenidate IR (Faber et al. 2008; Schawo et al. 2015; van der Schans et al. 2015). Evidence on the cost-effectiveness of stimulants on adults is extremely limited, as only two studies focused on adults (Shah et al. 2017; Zimovetz et al. 2018).
Cost-effectiveness analyses in stimulants
Several studies used a different measure of effectiveness, such as ADHD symptomatology (Zupancic et al. 1998; Jensen et al. 2005), impairment (Foster et al. 2007), or delinquency (Freriks et al. 2019) instead of QALYs. Three of these cost-effectiveness studies were performed based on the multimodal treatment of ADHD (MTA) data (Jensen et al. 2005; Foster et al. 2007; Freriks et al. 2019). The MTA study followed U.S. children and compared medication management (i.e., methylphenidate, and if necessary, dextroamphetamine, pemoline, imipramine, or other medications), intensive behavioral treatment, combined medication management and behavioral treatment, and community care (including medication) in a 14-month trial, with follow-ups in later years.
Jensen et al. (2005) assumed the U.S. societal perspective and a time horizon of 14 months and found that medication management had the lowest ICER compared to community care, followed by combined medical and behavioral treatment, behavioral treatment when looking at improvement in ADHD symptoms.
Foster et al. (2007) investigated cost-effectiveness using impairment, as measured by the Columbia Impairment Scale (CIS) (Bird et al. 1993), as an effectiveness measure from the U.S. third-party payer perspective using a time horizon of 14 months, and showed medication management to be most cost-efficient.
Finally, in a model-based study, Freriks et al. (2019) took delinquent behavior as an outcome, and showed that not medication treatment, but routine community care, which could also include medication treatment, was most cost-effective in a 10-year time horizon of the four treatments studied in the MTA. However, we should note here that after the initial trial phase of the MTA study, treatment choice was left free, and it could be that more individuals used medication, than indicated by the original randomization that was extrapolated over the 10-year period.
Zupancic et al. (1998) compared pemoline to dexamphetamine, methylphenidate IR, psychosocial/behavioral treatment, combination treatment (i.e., medication combined with psychosocial/behavioral treatment), and no treatment from a Canadian third-party payer perspective on ADHD symptoms as measured with the Conners Rating Scale (Conners et al. 1998) using a model with a time horizon of 1 year. In all cases, methylphenidate IR was cost-effective, and methylphenidate IR dominated dexamphetamine, psychosocial/behavioral treatment, combination treatment, and no treatment.
The abovementioned cost-effectiveness analyses showed that in most cases, stimulant treatment had lower cost and higher efficiency compared to behavioral treatment.
Cost-utility analyses in nonstimulant treatment
Atomoxetine is often used when there are contraindications for stimulants, such as stimulant adversity, intolerable side effects, or a history of substance misuse (Özgen et al. 2020).
In a model-based study, Tockhorn et al. (2014) assessed the cost utility of atomoxetine compared to no treatment from a health care perspective in Spain for a time horizon of 1 year for three populations of adults with ADHD: ADHD only, ADHD and comorbid alcohol abuse, and ADHD and comorbid anxiety. Atomoxetine was cost-effective compared to no treatment in all three groups.
The abovementioned model-based studies by Cottrell et al. (2008) and Hong et al. (2009) both evaluated 1-year cost-effectiveness of atomoxetine versus methylphenidate IR and ER and no treatment from a UK and Spanish health care perspective, respectively, for three different groups of children: stimulant-naive children, stimulant-nonresponding children, and children with contraindications for stimulant medication. Cottrell et al. (2008) further distinguished between stimulant-averse children, § contraindicated stimulant-naive children, and contraindicated exposed children, where contraindicated children received treatment algorithms without methylphenidate and IR-DEX.
While Cottrell et al. (2008) found that first-line atomoxetine was cost-effective compared to other treatment algorithms for all groups, Hong et al. (2009) found that atomoxetine was cost-effective compared to methylphenidate ER for stimulant-naive children and compared to no treatment for children with contraindications or previous stimulant failure, but not cost-effective compared to methylphenidate IR for stimulant-naive children.
Conversely, the abovementioned model-based study by King et al. (2006) found that the treatment strategy first-line dexamphetamine, followed by second-line methylphenidate IR, followed by third-line atomoxetine treatment, dominated all other treatment options. This study employed a longer time horizon (12 years) and did not distinguish between different populations of children.
Two abovementioned model-based studies (Zimovetz et al. 2016, 2018) compared atomoxetine with lisdexamfetamine dimesylate from a UK health care perspective in children whose response to methylphenidate was clinically insufficient (1-year time horizon) and in adults (5-year time horizon), respectively, and showed that atomoxetine was not cost-effective compared to lisdexamfetamine dimesylate.
In a model-based study, Sohn et al. (2016) compared the cost utility of atypical antipsychotics (i.e., aripiprazole, olanzapine, paliperidone, quetiapine, risperidone, and ziprasidone) to atomoxetine and clonidine/guanfacine in children with ADHD from a U.S. third-party payer perspective, using a 1-year time horizon. Atomoxetine was cost-effective compared to atypical antipsychotics. Atypical antipsychotics were dominated by clonidine/guanfacine.
Erder et al. (2012) conducted a model-based cost-utility analysis comparing guanfacine ER to atomoxetine and placebo in children and adolescents with ADHD. The study was conducted from a U.S. third-party payer perspective and had a 1-year time horizon. Guanfacine ER was cost-effective compared to atomoxetine. Two studies assessed the cost utility of guanfacine ER as an adjunctive therapy to long-acting stimulants in children using a time horizon of 1 year from a Canadian Ministry of Health and a societal perspective (Lachaine et al. 2016) and a U.S. third-party payer perspective (Sikirica et al. 2012). Guanfacine ER as adjunctive therapy to long-acting stimulants compared to only long-acting stimulants was cost-effective from the Ministry of Health perspective and the societal perspective, as well as from a U.S. third-party payer perspective.
Finally, a model-based study from United Kingdon on children with ADHD from NICE (2018b) compared atomoxetine to group-based behavioral therapy and a combination treatment of atomoxetine with behavioral therapy from a national health perspective (NHS) and personal social services perspective with a 1-year time horizon. Both atomoxetine and the combination therapy were not cost-effective compared to the group-based behavioral therapy. However, utilities for responders and nonresponders in this study were based on empirical estimates from responders and nonresponders to medication, even for behavioral therapy. In addition, in a sensitivity analysis with individual-based (as opposed to group based) behavioral therapy, the behavioral therapy was dominated by atomoxetine due to the high cost of individual-based behavioral therapy.
These studies showed that atomoxetine was cost-effective compared to methylphenidate (Cottrell et al. 2008), or no treatment (Hong et al. 2009) when children had contraindications for stimulants, such as stimulant adversity, intolerable side effects, or a history of substance misuse. However, when comparing atomoxetine to lisdexamfetamine dimesylate in children whose response to methylphenidate was insufficient, atomoxetine was not cost-effective (Zimovetz et al. 2016). In addition, in children, guanfacine appeared to be a cost-effective add-on treatment to stimulants (Sikirica et al. 2012; Lachaine et al. 2016). Finally, atomoxetine might not be cost-effective when compared to group-based behavioral therapy, but might be cost-effective compared to individual-based behavioral therapy (NICE 2018b).
Psychosocial treatment
Cost-utility analyses on psychosocial treatment
Four studies performed cost-utility analyses for psychosocial treatments in children with ADHD, consisting of a total of seven separate economic evaluations (Sayal et al. 2016; NICE 2018a,b; Janssen et al. 2019). NICE (2018a,b) performed four model-based cost-utility analyses in United Kingdom on different psychosocial treatments with a 1-year time horizon and likely from an NHS and personal social services perspective.
One of these evaluations (NICE 2018b), as previously mentioned, compared atomoxetine to group-based behavioral therapy and the combination of atomoxetine and group-based behavioral therapy for children with ADHD. Group-based behavioral therapy was cost-effective compared to atomoxetine and combination therapy, where atomoxetine compared to behavioral therapy had a lower ICER than combination therapy compared to behavioral therapy. However, a sensitivity analysis indicated that individual-based therapy was dominated by atomoxetine due to the high cost of individual- versus group-based therapy and that atomoxetine was cost-effective compared to combination therapy when it contained individual-based behavioral therapy.
Another cost-utility analysis by NICE (2018b) evaluated cognitive behavioral therapy (CBT) as an adjunctive treatment for adolescents who were on a stable dose of medication for the last 2 months, but who still had clinically significant symptoms. While medication was defined as any FDA-approved medication for ADHD, model inputs regarding the probability of response and nonresponse to CBT were based on results from a population of adolescents on a stable dose of methylphenidate. The results indicated that CBT is not cost-effective as an adjunctive therapy to medication, compared to medication only.
Two of the NICE (2018a,b) evaluations considered parent-based programs. The first (NICE 2018b) assessed the cost-effectiveness of telephone-assisted self-help for parents in a population of children with ADHD, who were on a stable dose of methylphenidate, but still had functional impairment in at least one of the domains of the Weiss Functional Impairment Rating Scale (American Psychiatric Association 2005). The results indicated that telephone-assisted self-help was not cost-effective as an adjunctive therapy for methylphenidate compared to methylphenidate only. The second compared parent training to no treatment for children with ADHD (NICE 2018a). While their results indicated that parent training might be cost-effective, ICERs—and thus conclusions on cost-effectiveness—depended heavily on the reference study used for data input. Notably, all four NICE (National Institute for Health and Care Excellence) evaluations used utilities for responders and nonresponders based on empirical estimates from responders and nonresponders to medication, even for the behavioral therapies.
Sayal et al. (2016) conducted a cost-effectiveness and cost-utility analysis in children. In the cost-utility analysis, a parent-only treatment (i.e., three 2-hour sessions of a school-based parent training, based on the 1-2-3-Magic parenting program (Phelan 2010), and a combined treatment (i.e., the school-based parent training with a 1.5-hour additional session for teachers) were compared to no treatment from a UK health care and societal perspective over a period of 6 months. From both perspectives, the parent-only treatment was cost-effective compared to no treatment, whereas the combined treatment resulted in lower incremental benefits and higher cost compared to no treatment.
Finally, Janssen et al. (2019) performed cost-utility analyses in adults comparing mindfulness-based cognitive therapy to care as usual from a Dutch societal and health care perspective over a 9-month period. They found that mindfulness-based cognitive therapy was cost-effective when taking a societal perspective, but not when taking a health care perspective. These studies showed that, compared to no treatment, parent training for children (Sayal et al. 2016; NICE 2018a) and mindfulness-based cognitive therapy for adults might be cost-effective treatments for ADHD (Janssen et al. 2019). However, the NICE (2018b) evaluations indicate that behavioral therapies might not be cost-effective as an adjunctive therapy to medication in children and adolescents, although group-based behavioral therapy as a stand-alone intervention might be cost-effective compared to atomoxetine.
Cost-effectiveness analyses on psychosocial treatment
Four studies investigated the cost-effectiveness of psychosocial treatment by comparing parent training to treatment as usual (TAU) (Lord and Paisley 2000; Sayal et al. 2016; Sonuga-Barke et al. 2017; Tran et al. 2018) on ADHD outcomes. Lord and Paisley (2000) used MTA data and compared intensive behavioral treatment (i.e., behavioral parent training, child-focused behavioral treatment, and a school-based behavioral program) to combined treatment (medication management and intensive behavioral treatment) in children with ADHD from a UK health care perspective over a period of 14 months. Combined treatment appeared cost-effective compared to intensive behavioral treatment.
Another cost-effectiveness study on the MTA data (Foster et al. 2007, discussed above), used a third-party payer perspective in the United States for the same time horizon and compared children with ADHD with comorbid anxiety, children with ADHD with other comorbid disorders, and children with ADHD only. It was shown that at higher levels of WTP per point of improvement on impairment, intensive behavioral treatment was the most beneficial alternative in children with ADHD with comorbid anxiety, but not in children with ADHD with other comorbid disorders or ADHD only.
The previously mentioned study by Sayal et al. (2016) compared parent training only and parent training with a school-based component to no treatment. ICERs of €33/one-point improvement on the Conners' Rating Scale (Conners et al. 1998) for the parent-only treatment and €153/one-point improvement for the combined treatment were found in this study.
Tran et al. (2018) conducted an economic evaluation from a U.S. societal perspective, in which Child Life and Attention Skills (CLAS, a program that integrates parent, teacher, and child training) and parent-focused treatment (PFT, only includes the parent training component of CLAS) (Pfiffner et al. 2014) were compared to TAU for children with ADHD Inattentive type (i.e., ADHD-I, characterized by predominantly inattentive symptoms). All treatments occurred over a 10- to 13-week period and cost-effectiveness was assessed using a 13-week time horizon. The ICER for PFT compared to TAU was €2674/resolved ADHD-I case (i.e., not meeting full criteria for ADHD-I after treatment) and the ICER of CLAS compared to TAU was €3312/resolved ADHD-I case. Hence, PFT appeared to be a more cost-effective ADHD treatment for children than CLAS compared to TAU.
In a study by Sonuga-Barke et al. (2017), the cost-effectiveness of the New Forest Parenting Program (NFPP, an 8- to 12-week ADHD-specific parent training) (Sonuga-Barke 2001) and incredible years (IY, a 12-week general parent training for behavioral problems) (Jones et al. 2008) and TAU were compared from a combined UK health care and societal perspective for a 6-month time horizon. The authors did not calculate ICERs because the efficacy of NFPP and IY did not differ significantly; however, the total mean cost of NFPP was lower, indicating that there could perhaps be a difference in cost-effectiveness.
Summarizing, it can cautiously be concluded that behavioral parent training for ADHD is a cost-effective treatment option compared to TAU, and that parent training appears more cost-effective when it is combined with a school-based intervention, such as teacher training.
Discussion
With this systematic review, we aimed to provide an overview of studies on the cost-effectiveness of ADHD treatments and to evaluate their outcomes. Our study indicates that there are several cost-effective treatment options for the treatment of ADHD in children and potentially also adults. Specifically, almost all studies that compared medication or psychosocial treatment to no treatment, placebo, or care as usual, concluded that medication or psychosocial treatment was cost-effective compared to a control condition (Gilmore and Milne 2001; Hong et al. 2009; Maia et al. 2016; Narayan and Hay 2004; Sayal et al. 2016; Tockhorn et al. 2014; NICE 2018a). The exceptions were Janssen et al. (2019), who found that mindfulness-based therapy for adults was cost-effective when taking a societal perspective, but not when taking a health care perspective, and Sayal et al. (2016), who found that, while a parent training was cost-effective compared to no treatment, combined parent and teacher training was not. However, several areas remain underexplored. For instance, up until recently, few studies focused on behavioral interventions and few studies have been performed in adults. Nevertheless, we can conclude that stimulant and nonstimulant treatment and parent training are cost-effective treatment options for children from certain perspectives. This is in line with Sampaio et al. (2021), who concluded that there is evidence for the cost-effectiveness of behavioral interventions in children, non-IR stimulant medication for children with a suboptimal response to IR stimulant treatment, and nonstimulant medication as adjunctive therapy for children with suboptimal response to stimulants.
Drawing unambiguous conclusions about cost-effectiveness of ADHD treatments is difficult, given the numerous different comparators, perspectives, and populations in the literature. Overall, evidence suggests that stimulant treatment is cost-effective for treating ADHD in children and adolescents (Gilmore and Milne 2001; King et al. 2006; Narayan and Hay 2004; Maia et al. 2016; Zimovetz et al. 2016). Within stimulant treatments, several studies showed that methylphenidate ER was cost-effective compared to methylphenidate IR in children (Faber et al. 2008; Schawo et al. 2015; van der Schans et al. 2015).
However, results of studies concerning nonstimulants were more mixed. Atomoxetine appeared cost-effective compared to no treatment in children with contraindications for stimulants, such as stimulant adversity (Cottrell et al. 2008; Hong et al. 2009), or substance abuse (Tockhorn et al. 2014), but results in stimulant-naive children were mixed (Cottrell et al. 2008; Hong et al. 2009), and atomoxetine appeared not to be cost-effective compared to group-based behavioral therapy (NICE 2018b). When comparing atomoxetine to lisdexamfetamine dimesylate, atomoxetine was not cost-effective in children and adults (Zimovetz et al. 2016, 2018). Guanfacine appears to be a cost-effective adjunctive treatment to stimulants (Sikirica et al. 2012; Lachaine et al. 2016).
While psychosocial treatment is a well-established treatment for ADHD, especially in children, only recently, more studies have focused on psychosocial treatments (Lord and Paisley 2000; Sayal et al. 2016; Sonuga-Barke et al. 2017; Tran et al. 2018; NICE 2018a,b; Janssen et al. 2019). The included cost-utility analyses suggest that, compared to no treatment, parent training for children (Sayal et al. 2016; NICE 2018a) and mindfulness-based cognitive therapy for adults might be cost-effective treatments for ADHD (Janssen et al. 2019), but that behavioral therapies might not be cost-effective as an adjunctive therapy to medication (NICE 2018b), although group-based behavioral therapy as a stand-alone intervention might be cost-effective compared to atomoxetine (NICE 2018b). However, these results should be interpreted with caution; since depending on the study, sample sizes were small (Janssen et al. 2019), cost-effectiveness depended on the perspective taken (Sayal et al. 2016), or utilities for response and nonresponse to behavioral interventions were based on empirical results from medication (NICE 2018a,b). Moreover, as there is large variation in the nature of the psychosocial treatments, they are difficult to compare.
Moreover, due to differences in outcome measures and intensity of treatment programs that were used in the psychosocial studies (e.g., the intensive behavioral treatment in the MTA is much costlier than the parent training that was evaluated in Sayal et al., 2016), it is difficult to draw strong conclusions. Nevertheless, in cost-effectiveness studies comparing psychosocial treatments to medication treatment, psychosocial treatments were dominated by medication management. Other studies did show parent training to be more effective and less costly compared to no treatment/TAU (Sayal et al. 2016; Tran et al. 2018). To enhance knowledge about the (dis)advantages and costs of psychosocial ADHD treatments and to facilitate decision making, more cost-utility analyses are warranted.
We found an average quality score of 69% (95% CI: 52–87) on the CHEC, suggesting that, on average, the quality of current cost-effectiveness research could be improved. In general, the included studies scored well on items related to the research question and objective, economic design, time horizon, identification of alternative outcomes, and reporting of an ICER. However, scores were considerably lower for items related to description of the model and assumptions, discussion on the generalizability of the results, conflict of interest, and discussion on ethical and distributional issues. This is worrisome, as clearly described and appropriately argued model descriptions and assumptions lend credibility to the results of cost-effectiveness analyses. If these are absent, it is difficult to assess how realistic the model outcomes are, or how certain we can be that the true cost-effectiveness of a treatment will fall within a certain range of cost per QALY.
As ADHD is a disorder that often persists into adulthood and awareness of ADHD in adults is growing (Willcutt 2012; American Psychiatric Association 2013), it is surprising that at this point, conclusions about cost-effective adult ADHD treatments have to be drawn with caution. We only included four studies that addressed different treatments with various comparators for adults with ADHD (Shah et al. 2017; Tockhorn et al. 2014; Zimovetz et al. 2018; Janssen et al. 2019). Although these studies suggest that there are cost-effective treatments for adults, more studies on most common options (e.g., medication) are warranted to draw unambiguous conclusions.
There is limited evidence on cost-effectiveness of ADHD treatments in the long term, mainly due to lack of long-term empirical data on costs and effectiveness of ADHD treatments (Nagy et al. 2017); economic evaluations do not take this limitation sufficiently into account when expanding their time horizon. This is, for instance, shown by a study by Faber et al. (2008), in which the cost-effectiveness of methylphenidate ER was predicted over a 10-year treatment span. However, their long-term cost-effectiveness prediction was entirely based on short-term empirical data, ignoring the fact that only a small minority of patients use methylphenidate for 10 years consistently and, above all, that short-term efficacy data cannot readily be extrapolated over such a long time frame. Similarly, Freriks et al. (2019) used MTA data up to 8 years after the end of the trial period, but even then cost-effectiveness was only modeled up to late adolescence as the relevant empirical data were not available for adulthood. In addition, the study extrapolated the treatment allocation from the initial 14-month trial period over 10 years and did not account for the fact that children might have switched treatments. Several studies did acknowledge that limited long-term evidence is a problem in economic evaluations (Gilmore and Milne 2001; Tran et al. 2018; Zimovetz et al. 2018), but currently no cost-effectiveness studies have been conducted using long-term empirical data.
Another point of caution is that a large proportion of the included pharmacological treatment studies was funded by pharmaceutical industry (Cottrell et al. 2008; Faber et al. 2008; Hong et al. 2009; Erder et al. 2012; Sikirica et al. 2012; Schawo et al. 2015; Lachaine et al. 2016; Zimovetz et al. 2016, 2018). When funded by industry, published evidence on benefits of medication is likely to be overestimated and more often shows results favorable to the pharmacological treatment being studied (World Health Organization 2017). Although in some industry-funded studies, costs per QALY for the treatments were relatively high (Sikirica et al. 2012) or differences in QALY gains were very small (Hong et al. 2009), all included industry-funded economic evaluations presented results in favor of the studied treatment. In contrast, results of studies that were not sponsored by (pharmaceutical) industry were more diverse (Zupancic et al. 1998; Donnelly et al. 2004; King et al. 2006; van der Schans et al. 2015; Sayal et al. 2016; Sonuga-Barke et al. 2017; Tran et al. 2018; Freriks et al. 2019). This implies that there is an urgent need for unbiased economic evaluations.
Strengths and limitations
One of the strengths of this systematic review is that we conducted a thorough search following stringent inclusion criteria and included all full economic evaluations in the ADHD field, regardless of publication year, age of study population, or treatment modality. Moreover, the systematic review was performed and reported following the standard PRISMA methods (Moher et al. 2009). Finally, we assessed the quality of all identified studies. Despite these strengths, there are also some limitations to note.
First, we compared studies that assessed the cost-effectiveness of the same comparators. However, it is important to bear in mind that differences in factors related to the country of the study, such as health care system, costs (e.g., prices of medication may differ substantially between countries), and societal context (e.g., better educated staff in schools, which might increase or decrease effects of certain ADHD interventions), may have had a substantial influence on the outcomes (i.e., ICERs) (Anderson 2010). Consequently, it is important to consider the country of study when interpreting the results. In addition, differences in the design of the studies, such as the perspective, time horizon, and study population, as well as the time at which the study took place, can also substantially influence cost-effectiveness outcomes. Therefore, these differences should be considered when interpreting results.
Second, while we did an extensive systematic search of all relevant databases, we did not assess possible publication bias. Finally, the generalizability of our results outside high-income countries may be limited, as few studies on middle- and low-income countries were included in this systematic review.
Conclusion
This systematic review provides an overview of the available economic evaluations of treatments for individuals with ADHD. Our results indicate that, generally, medication or psychosocial treatment is cost-effective when compared to no treatment, care as usual, or placebo. In addition, stimulant treatment appears to be a cost-effective treatment for children and adolescents with ADHD. Despite the rising interest in cost-effectiveness, this study shows that more and higher quality cost-effectiveness research is warranted to aid in the optimal use of available treatments and resources for individuals with ADHD. Nevertheless, we can conclude that treatments for ADHD are generally cost-effective compared to no treatment.
Clinical Significance
ADHD is highly prevalent and associated with high personal, societal, and governmental costs across all ages. Effective treatments can reduce symptom severity and alleviate impairment associated with ADHD. However, since health care budgets are limited, it is imperative that health care funds are allocated efficiently: covering treatments in such a way that the highest number of individuals receives the best possible health benefits. Economic evaluations of ADHD treatments may help in reaching an efficient allocation of funds and contribute to improvement of ADHD-related impairments within the limits of the available resources. Consequently, in this systematic review, we provide an overview of the cost-effectiveness of treatments for individuals with ADHD.
Footnotes
Authors' Contributions
L.M.W., H.D., and A.P.G. were responsible for performing systematic searches and data extraction/collection. L.M.W, A.P.G., B.v.d.H., M.C., and P.J.H. were responsible for conception of the article. L.M.W., A.P.G., B.J.v.d.H., and P.J.H. were responsible for designing the study. L.M.W. wrote the first draft of the article. H.D. and A.P.G. wrote subsequent versions of the article. All authors reviewed the article for intellectual content.
Acknowledgments
We wish to thank Reina de Kinderen for her assistance in the conceptualization and start of this article. The findings and views reported in this article are those of the authors and should not be attributed to individuals mentioned in this study.
Disclosures
L.M.W., A.P.G., H.H.D., and M.C. have no conflict of interests to declare. P.J.H. has received research funding from Shire and payments for an advisory board meeting. B.J.v.d.H., financial: receives royalties as one of the editors of “Sociaal Onhandig” (published by Van Gorcum), a Dutch book for parents of children with ADHD or PDD-NOS that is being used in parent training; nonfinancial: has developed and has evaluated/evaluates several Dutch parent training programs, without financial interests; is and has been a member of Dutch ADHD guideline groups; and is an advisor of the Dutch Knowledge Centre for Child and Adolescent Psychiatry.
Data sharing not applicable—no new data generated: data sharing is not applicable to this article as no new data were created or analyzed in this study.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Appendix S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.