
Abstract
Editors' Note:
The Editors would like to address issues related to the acceptance of this manuscript. The original manuscript referenced the study tool as the Bipolar Prodrome Symptom Interview Scale-Prospective (BPSS-P). After the manuscript's initial acceptance, the authors requested a revision of the tool name to Bipolar Prodrome Symptom Interview Scale-Full Perspective (BPSS-FP). When this request was made, the original acceptance was rescinded, and the authors were asked to formally revise and resubmit the manuscript with an explanation for the change. This revision and subsequent review led to the final acceptance of the manuscript. The authors have assured us that the tool used in the manuscript was the BPSS-FP (version 5) as opposed to abbreviated forms of this tool that are also used in research (e.g., Bipolar Prodrome Symptom Scale-Abbreviated Screen for Patients (BPSS-AS-P).
Background:
No scale exists to assess patients at-risk for bipolar disorder (BD) in Turkey. We aimed to assess the psychometric properties of the Turkish version of the Bipolar Prodrome Symptom Interview and Scale-Full Prospective (BPSS-FP).
Method:
Psychiatric service users aged 11–18 years old were interviewed using the BPSS-FP translated into Turkish and the Kiddie Schedule for Affective Disorders and Schizophrenia. Youth with major depressive disorder (MDD, n = 63), bipolar-spectrum disorder (n = 47), and healthy controls (n = 122) were included. Cronbach's alpha was calculated to assess internal consistency. The Young Mania Rating Scale (YMRS) and Children's Depression Rating Scale-Revised (CDRS-R) were administered to test convergent/discriminant validity. Discriminant validity was further tested using one-way ANOVA and “receiver operating characteristic” (ROC) curves. Inter-rater reliability was tested using correlation coefficients.
Findings:
Across 232 youth, Cronbach's alpha values were 0.932 for the BPSS-FP total score, 0.878 for the Mania Symptom Index, 0.887 for the Depression Symptom Index, and 0.797 for the General Symptom Index. Correlation coefficients for inter-rater reliability were high for the Mania Symptom Index (r = 0.989), Depression Symptom Index (r = 0.973), and General Symptom Index (r = 0.981). There were high correlations between the BPSS-FP Mania Symptom Index subscore and YMRS (r = 0.732), and the BPSS-FP Depression Symptom Index subscore and CDRS-R (r = 0.754), whereas cross-polarity correlations were non-significant. ROC analysis cut-off value was ≥21 for the BPSS-FP Mania Symptom Index between patients with BD and MDD (specificity = 85.7%, sensitivity = 78.7%).
Conclusion:
The Turkish version of the BPSS-FP has good psychometric properties and can be used in research. Longitudinal studies are needed to confirm the predictive value of the BPSS-FP.
Introduction
Bipolar disorder (BD) is a debilitating chronic psychiatric disorder, characterized by recurrent mood episodes (Ferrari et al. 2016). The cumulative lifetime prevalence of bipolar-spectrum disorders is 2.4% in the entire population (Merikangas et al. 2011). A meta-analysis conducted by Dagani et al. (2017) demonstrated that the mean duration from the appearance of the first symptoms of the disease to accurate diagnosis was 5.8 years (Dagani et al. 2017). Another study also reported an average duration between illness-onset and diagnosis of 10 years (Hirschfeld et al. 2003).
Early intervention in BD is associated with favorable outcomes, such as better treatment response, lower relapse rate, higher likelihood of symptom remission, and improved psychosocial functioning (Joyce et al. 2016; Saraf et al. 2021). Besides, treatment delay is associated with an increase in the frequency of mood episodes and failure to achieve complete remission (Drancourt et al. 2013; Medeiros et al. 2016). Considering the morbidity, increased mortality risk, chronic course, and increased financial and social burdens of the illness, early diagnosis and treatment are crucial to alleviate illness-related unfavorable outcomes (Hirschfeld et al. 2003; Pini et al. 2005; Laursen et al. 2013; Kessing et al. 2015; Cloutier et al. 2018).
With increasing evidence concerning the utility of identifying a clinical high-risk state for psychosis (Catalan et al. 2021; Fusar-Poli et al. 2020), early identification and intervention during the BD prodrome have come into focus (Correll et al. 2007a, 2007b; Hauser and Correll 2013; Noto et al. 2013; Malhi et al. 2017). Bipolar prodrome is defined as the symptomatic period that occurs before a first manic/hypomanic episode (Skjelstad et al. 2010; Faedda et al. 2019). A meta-analysis by Van Meter et al. (2016) evaluated the duration of depressive and manic prodrome in patients with BD by reviewing studies in all age groups (Van Meter et al. 2016). This meta-analysis showed that the unweighted duration of the prodrome was ∼27 months for the first mood episode (Van Meter et al. 2016).
Since standardized structured interviews are not used in most of the available studies (Van Meter et al. 2016), it is difficult to define and generalize the characteristics of prodromal symptoms, such as duration, severity, frequency, and effects on functioning (Correll et al. 2014a). A study conducted by Correll et al. (2014a) using the Bipolar Syndrome Interview and Scale-Retrospective, included the child and adolescent age group and reported that the prodromal symptoms found in >50% of the cases were irritability, racing thoughts, increased energy/goal-directed activity, mood lability, depressed mood, and distractibility, together with decreased school performance (Correll et al. 2014a).
Previous results indicated that the time from the first newly emerging specific mania symptoms and first mania episode lasted about 18 months, allowing for early detection of the disease before the manic episode arises (Correll et al. 2014a). However, the prodrome duration was shorter when two or three prodromal mania symptoms were required concurrently, especially those being more (hypo)mania-like, shortening the window for intervention (Correll et al. 2014a).
The authors also suggested that unstructured interviews were able to detect only an average of 4 prodromal symptoms in contrast to structured interviews, which yielded an average of 13 prodromal symptoms, including mania, depression, psychosis, and general psychopathology items (Correll et al. 2014a). Accordingly, a structured approach is better for identifying high-risk symptoms by evaluating all possible newly emerging symptoms, while unstructured approaches may miss some of these symptoms and therefore fail to identify a high-risk state.
The Bipolar Prodrome Symptom Interview and Scale-Full Prospective (BPSS-FP) is the first to specifically and comprehensively evaluate the bipolar prodrome (Correll et al. 2014b). The BPSS-FP is a semistructured interview based on the Diagnostic and Statistical Manual of Mental Disorders (DSM), which evaluates three main clusters of symptoms that can be part of the BD prodrome, covered by the Mania Symptom Index, Depression Symptom Index, and General Symptom Index.
The BPSS-FP uses semistructured and open-ended questions aimed at young people and/or their caregivers, allowing to determine subthreshold symptoms that occur before a full manic, depressive, or mixed mood episode (Correll et al. 2014b). However, the good psychometric properties, reliability, and validity of the BPSS-FP have only been established once so far, and only in a sample from the United States of 205 youth aged 12–23 years, including 129 patients with mood-spectrum disorders, 34 with nonmood-spectrum disorders, and 42 healthy controls (Correll et al. 2014b).
Therefore, this study aimed to replicate the reliability, validity, and psychometric soundness of the BPSS-FP in an independent Turkish sample of youth with mood disorders and healthy controls, at the same time validating the Turkish translation of the BPSS-FP.
Methods
Translation and adaptation of the scale
The interview was translated independently into Turkish by an adult psychiatrist and a child and adolescent psychiatrist. The Turkish text was evaluated by the entire research team that comprised five child psychiatrists and two adult psychiatrists in terms of language use and word choice. Later, the interview was back-translated into English by a child psychiatrist outside of the research team. This translation was compared with the original interview and scale by Christoph U. Correll, MD, developer of the BPSS-FP, and Daniel Guinart, MD, PhD, certified BPSS-FP trainer, to find out whether there was any changes in the meaning of phrases in the final version of the Turkish version, which were corrected. The study was approved by the Local Ethics Committee of Manisa Celal Bayar University, Faculty of Medicine (Protocol No.: 16.10.2019/20.478.486).
Participants and study sample
The clinical validation sample consisted of patients diagnosed with major depressive disorder (MDD) or BD and related disorders (i.e., bipolar-I disorder, bipolar-II disorder, and unspecified bipolar and related disorder) who were regularly followed in the outpatient and inpatient clinics of two psychiatry-teaching university hospitals (Dokuz Eylul University, Izmir and Celal Bayar University, Manisa) and a research and training hospital (Behçet Uz Children's Hospital, Izmir).
All research diagnoses were confirmed by a semistructured interview, using the Turkish version of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL) (Unal et al. 2019). The inclusion criteria were as follows: (1) being diagnosed with MDD or BD and related disorders as per the Diagnostic and Statistical Manual of Mental Disorders-5th Edition (DSM-5) (American Psychiatric Association, 2013), (2) being between the ages of 11 and 18 years, (3) being able to understand and speak Turkish, and (4) giving informed consent to participate in the study. All patients and the parents of minors provided written informed consent for the study. Exclusion criteria involved the following: (1) intellectual disability hampering the patient's ability to follow instructions and to answer queries of the BPSS-FP interview, and (2) refusing to participate in the study.
The healthy control sample consisted of volunteers who applied to the general pediatric clinics of the hospitals in which the psychiatric patients were recruited and who accepted to participate in the study. Exclusion criteria for healthy controls included being diagnosed with a mental disorder or an intellectual disability that hampers the patient's ability to follow the research instructions in the clinical assessment and having any chronic medical illness.
Clinical assessment
Bipolar Prodrome Symptom Interview and Scale-Full Prospective (BPSS-FP)
BPSS-FP is a semistructured interview covering DSM-defined diagnostic criteria for mood disorders (i.e., depressive episode and manic episode) (Correll et al. 2014b). BPSS-FP evaluates the severity, frequency, and duration of manic, depressive, and general symptoms from absent via subthreshold expression to syndromal severity of symptoms. The General Symptom Index involves symptoms previously reported in the course of the BD prodrome or syndrome (mood lability, oppositionality, anger, anxiety, self-injurious behavior, obsessions/compulsions, positive psychotic symptoms, negative psychotic symptoms, disorganized psychotic symptoms) (Correll et al. 2014b).
Whenever screening questions listed in an item/symptom of the interview are answered positively, the highest/worst severity, frequency, and duration of a symptom during lifetime (or since the last visit if it is a follow-up interview) and during the last month are determined by using open-ended questions listed in the instructions. Each symptom index (i.e., Mania, Depression, and General Symptom Index) is summarized at the end of the related section.
Severity ratings are made using specific anchors on the following Likert-type scale: 0 = absent, 1 = questionably present (i.e., “may be at the upper limit of normal” and/or “can be explained by external factors”), 2 = mild (i.e., “not fully explained by external factors”), 3 = moderate (i.e., “beginning to be noticed by others”), 4 = moderately severe (i.e., “can be noticed by others” and/or “beginning to interfere with functioning”), 5 = severe (i.e., “can be clearly noticed by others” and “affects functioning”), and 6 = severe (i.e., “impairs functioning”).
Frequency ratings are made using the following anchors: 0 = absent, 1 = less than once in a month, 2 = once in a month, 3 = 2–3 times a month, 4 = 4–7 times a month, 5 = 8–27 times a month, and 6 = ≥28 times a month ( = ultradian cycling). The duration of Mania Symptom Index symptoms is rated as follows per month: 0 = absent or <1 hour, 1 = 1 hour, 2 = 2–3 hours, 3 = 4–23 hours, 4 = 1–3 days, 5 = 4–6 days (definition of hypomania), and 6 = 7 or more days (definition of mania not complicated by the need for psychiatric admission or psychosis). For the Depression Symptom Index and the General Symptom Index, a rating of 6 equals 14 days or more (consistent with the 14-day threshold for depression); all other ratings are similar to the Mania Symptom Index.
Severity, frequency, and duration ratings were determined for both last month and since the last visit or lifetime. Finally, the predominant symptom pattern (frequency) at which symptoms generally occurred (i.e., continuous, episodic-frequent, episodic-infrequent, or rare) and date of symptom onset were also questioned. The interview approximately takes 1 hour for healthy controls and can last 90–150 minutes in psychiatric patients (or their caregivers serving as informants), depending on the current psychopathology and the number of complaints in the last year (Correll et al. 2014b).
Young Mania Rating Scale
The Young Mania Rating Scale (YMRS) was developed to measure the severity and change of the manic state. The YMRS involves 11 mania-related items and the sum of the scores obtained from each item constitutes the total score of the scale. A Turkish validity and reliability study was conducted by Karadag et al. (2002). In this study, the Turkish version of the YMRS was used for convergent validity analysis.
Children's Depression Rating Scale-Revised Form
The Children's Depression Rating Scale-Revised (CDRS-R) is a scale developed for clinicians to evaluate depressive symptoms and the severity of depressive episodes in children. CDRS-R also provides information about the treatment response during the follow-up. Alşen Guney et al. (2018) adapted the scale to the Turkish language and evaluated its psychometric properties (Guney et al. 2018). In this study, the CDRS-R was used for the convergent validity analysis.
Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children
The K-SADS-PL was originally developed by Kaufman et al. (1997) to evaluate psychiatric disorders of children and adolescents (Kaufman et al. 1997). The K-SADS-PL has been updated to be compatible with DSM-5 diagnoses, and the recent version of K-SADS-PL was also translated into and validated in the Turkish language (Unal et al. 2019).
Procedures
First, a person from the research team (C.E.) was trained, supervised, and certified in the interview procedures and ratings by Christoph Correll, MD, the originator of the BPSS-FP, at the Psychiatry Research Department of the Zucker Hillside Hospital, NY, USA. Furthermore, C.E. became a certified trainer for the BPSS-FP interview. Later, all other researchers completed the theoretical and practical supervision training of the scale in Turkey, trained and supervised by C.E.
Data analysis
The severity score of each item for the last month was included in the data analysis. To compare the diagnostic groups in terms of demographics, illness, and treatment characteristics, the ANOVA test was implemented to compare continuous variables, and the chi-square test was used for categorical variables. For all comparisons, p < 0.05 was accepted as the statistical level for significance. In the reliability analysis, the Cronbach alpha value was used for internal consistency and correlation coefficients between the individual BPSS-FP items, and both the BPSS-FP total score and each of the respective three BPSS-FP index scores were investigated. Inter-rater reliability was also tested using correlation coefficients.
To demonstrate convergent validity of mood-related symptoms, the correlation between the BPSS-FP Depressive and Mania Symptom Index subscale scores and the YMRS and the CDRS-R scores was investigated. Correlation coefficients were considered <0.30 = low, 0.30–0.49 = moderate, 0.50–0.80 = high, and ≥0.80 = very high level of correlation. The discriminant validity of the BPSS-FP Mania Symptom Index was calculated using the receiver operating characteristic (ROC) curve. The ROC analysis was implemented between patients with BD and MDD. Statistical Package for Social Sciences Version 24 was used for data analysis (IBM Corporation, Armonk, NY). The ROC curve was drawn using the STATA/IC version 16 (StataCorp. 2019, College Station, TX).
Results
Patient sample
The study sample (n = 232) consisted of 110 youth (mean age = 15.7 ± 1.6 years, 22.7% males) and 122 healthy volunteers (mean age = 14.9 ± 1.8 years, 27.0% males). The patient group was significantly older than controls by nearly 1 year (p = 0.001). The patient group included 47 cases with bipolar-spectrum disorders (mean age = 15.8 ± 1.7 years, 36.2% male) and 63 patients with MDD (mean age = 15.6 ± 1.4 years, 12.7% male). Sex significantly differed between the two patient groups (Table 1). There was no significant difference between the patient groups in terms of comorbid psychiatric diagnoses (p > 0.05). Details of the demographics, illness, and treatment characteristics of patients are depicted in Table 1.
Demographic, Clinical, and Treatment Characteristics of Study Participants
Different superscripts indicate statistical significance between study groups at p < 0.05 level.
ADHD, attention-deficit/hyperactivity disorder, BD-I, bipolar-I disorder; BD-II, bipolar-II disorder; CD, conduct disorder; MDD, major depressive disorder; ODD, oppositional-defiant disorder; SUD, substance use disorder; SD, standard deviation.
Internal consistency
The Cronbach alpha coefficient of all items was 0.932. The Cronbach alpha values of subscales were 0.878 for the Mania Symptom Index, 0.887 for the Depression Symptom Index, and 0.797 for the General Symptom Index. Item total score correlation coefficients between individual BPSS-FP items and the BPSS-FP total score ranged between 0.230 and 0.759, that is, all being >0.20 (Table 2).
Item-Total Score Correlation Coefficients and Cronbach's Alpha if Item Deleted Values of the Bipolar Prodrome Symptom Interview and Scale-Full Prospective
Cronbach's alpha = 0.932.
BPSS-FP, Bipolar Prodrome Symptom Interview and Scale-Full Prospective.
Inter-rater reliability
Correlation coefficients for inter-rater reliability were high for each, the Mania Symptom Index (r = 0.989), Depression Symptom Index (r = 0.973), and General Symptom Index (r = 0.981).
Convergent validity
In the clinical sample, there was a high level of correlation between the BPSS-FP Mania Symptom Index and the YMRS score (r = 0.732), and between the BPSS-FP Depression Symptom Index and the CDRS-R total score (r = 0.754). The BPSS-FP General Symptom Index was moderately correlated with the YMRS (r = 0.342) and the CDRS-R total score (r = 0.403) (Table 3).
Pearson Correlation Coefficients of the Bipolar Prodrome Symptom Interview and Scale-Full Prospective Subscales and Mania as well as Depression Scales Within the Clinical Sample
Statistically significant at p < 0.001.
BPSS-FP, Bipolar Prodrome Symptom Interview and Scale-Full Prospective; CDRS-R, Children's Depression Rating Scale-Revised; YMRS, Young Mania Rating Scale.
Discriminant validity
The correlations between the total BPSS-FP Mania Symptom Index and the CDRS-R score, and between the total BPSS-FP Depression Symptom Index and the YMRS score were not statistically significant, demonstrating good divergent validity (Table 3).
To evaluate the discriminant validity of the BPSS-FP further, the total scores of the BPSS-FP Mania Symptom Index, Depression Symptom Index, and General Symptom Index were compared among study groups using the one-way ANOVA test, yielding significant differences between study group results (Table 4). The BPSS-FP Mania Symptom Index score was highest in the bipolar-spectrum disorder group and the lowest in the healthy control group (BD group = 27.4 ± 9.9, MDD group = 13.1 ± 7.4, healthy control group = 4.4 ± 4.1, F = 207.9, p < 0.001).
Comparisons of Study Groups on the Bipolar Prodrome Symptom Interview and Scale-Full Prospective Subscales and Mania as well as Depression Scales Using One-Way ANOVA
Bold values are significant at 0.05 level.
According to post hoc Tukey's b test.
BPSS-FP, Bipolar Prodrome Symptom Interview and Scale-Full Prospective; CDRS-R, Children's Depression Rating Scale-Revised; SD, standard deviation; YMRS, Young Mania Rating Scale.
The BPSS-FP Depression Symptom Index score was the highest in the MDD group and lowest in the healthy control group (MDD group = 34.3 ± 9.6, BD group = 22.3 ± 12.3, healthy control group = 4.9 ± 4.8. F = 277.1, p < 0.001). The BPSS-FP General Symptom Subscale total score was significantly higher in both patient groups compared with the healthy control group (BD group = 15.2 ± 9.6, MDD group = 14.5 ± 6.4, healthy control group = 2.8 ± 3.1. F = 120.3 p < 0.001), without significant differences between the bipolar-spectrum disorder and MDD patients (post hoc Tukey's b test, p > 0.05).
Figure 1 demonstrates ROC curve between subjects with BD (n = 47) and MDD (n = 63). In the ROC analysis of the capacity of the BPSS-FP to distinguish the bipolar-spectrum disorder group from the MDD group, the area under the curve was 0.867. Mania Symptom Index score of ≥21 was the optimal cutoff between patients with BD and MDD (specificity = 85.7%, sensitivity = 78.7%).
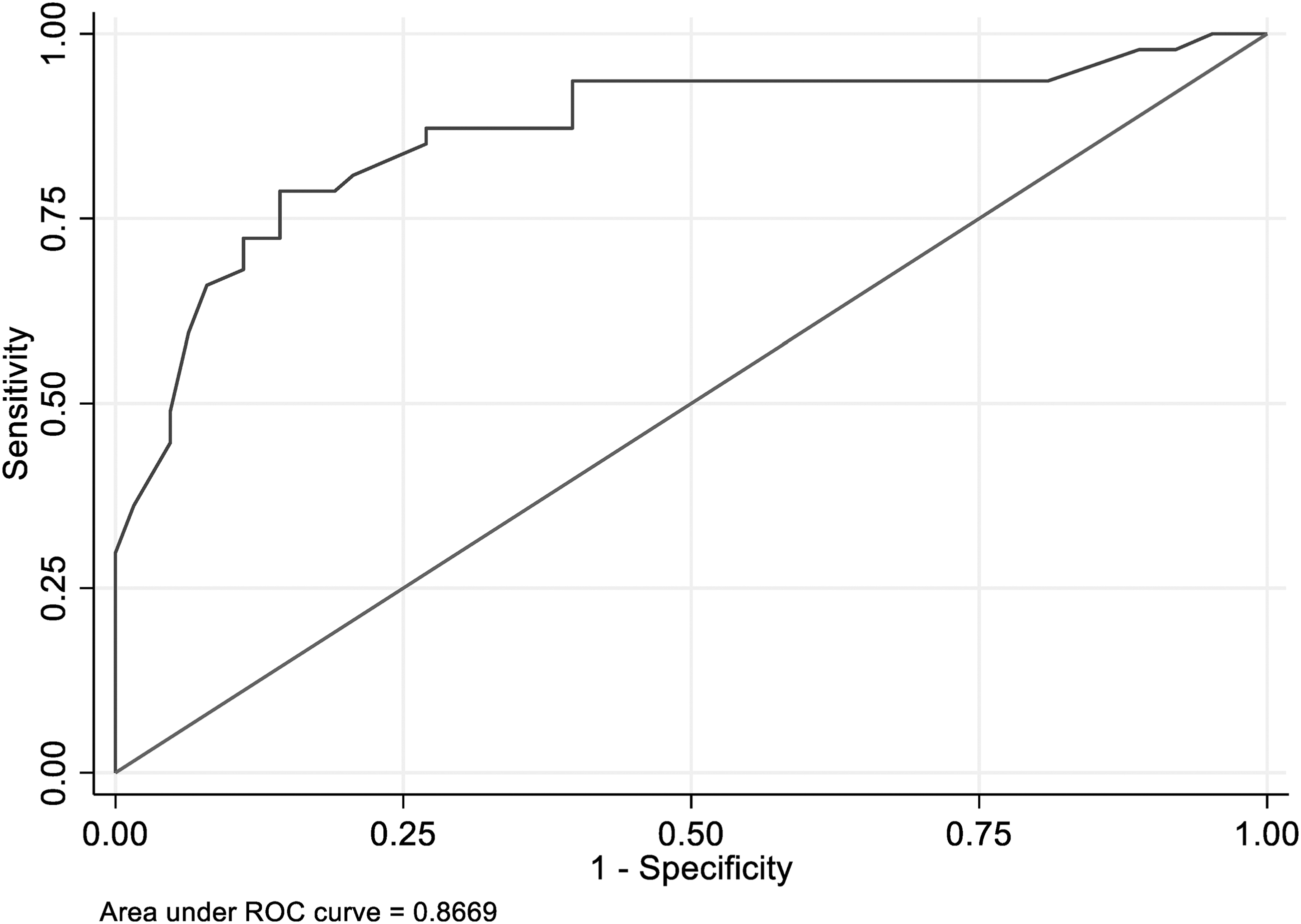
The ROC curve for the Mania Symptom Index between patients with bipolar-spectrum disorders and major depressive disorder. ROC, receiver operating characteristic.
Discussion
To the best of our knowledge, following the initial test of the psychometric properties of the BPSS-FP (Correll et al. 2014b), this is the first independent non-English language validation of the BPSS-FP, a dedicated interview and rating scale for the earliest stages in the development of BD. The results of this study suggest that the Turkish version of BPSS-FP has adequate internal consistency and inter-rater reliability, and sufficient convergent and discriminant validity to be used in research settings. Overall, these results strengthened good psychometric properties of the BPSS-FP in an independent sample with mood disorders.
Individuals who are diagnosed with bipolar-spectrum disorders may experience long delays from the onset of symptoms until they are diagnosed, which prolongs the time to reach the appropriate treatment (Hirschfeld et al. 2003; Dagani et al. 2017). Given the lack of reliable prediction of illness trajectory, early recognition of BD and the development of suitable interventions are still important research endeavors (Faedda et al. 2019; Post et al. 2020).
As a structured interview, the BPSS-FP was developed to help overcome these difficulties by providing detailed assessments and ratings of high-risk symptoms. The BPSS-FP has been reported to have valid and reliable psychometric properties (Correll et al. 2014b). In this study, the adaptation, reliability, and convergent and discriminant validity of the Turkish version of the BPSS-FP were confirmed. Detection of individuals with high-risk symptoms who will develop BD remains a future goal.
In line with the original validation study (Correll et al. 2014b), the inter-rater reliability of the Turkish version of the BPSS-FP was also very high. Similarly, Cronbach's alpha values of the whole scale, BPSS-FP Mania Symptom Index, and Depression Symptom Index revealed high reliability (>0.81), and moderate reliability for the General Symptom Index (>0.71). In the original study, these values were 0.94 for the whole BPSS-FP, 0.87 for the BPSS-FP Mania Symptom Index, 0.89 for the Depression Symptom Index, and 0.74 for the General Symptoms Index (Correll et al. 2014b).
The CDRS-R and the YMRS were administered to study convergent and discriminant validity of BPSS-FP-rated mood symptoms. The correlation coefficients among the mood-concordant subscales of the BPSS-FP and the YMRS or the CDRS-R, respectively, were >0.73, while the polarity-discordant correlations were low (<0.10) and nonsignificant.
While current findings support good psychometric properties of the BPSS-FP within individuals with mood disorders, the sensitivity and specificity of the interview to identify individuals at risk for BD before a full BD episode should be explored in familial and clinical high-risk samples. Thus, future studies also should examine the predictive value of the BPSS-FP that demonstrates individuals with a high-risk status who would develop full BD.
In the original study conducted by Correll et al. (2014b), the YMRS and the Montgomery-Åsberg Depression Rating Scale (MADRS) were used for the convergent validity analysis. In this study, the correlation coefficient values between the BPSS-FP Mania Symptom Index and the total YMRS scores and between the BPSS-FP Depression Symptom Index and the total MADRS scores were higher than 0.50. The correlation coefficients between the BPSS-FP Depression Symptom Index and the YMRS (r = 0.27), and between the BPSS-FP Mania Symptom Index and the MADRS (r = 0.14) were also low (Correll et al. 2014b). Our results were consistent in that cross-polarity analyses revealed very low correlations in the clinical sample. Considering all these findings together, we consider that the scale met the psychometric validity criteria.
There were significant differences among the study groups comparing the total scores of the Mania Symptom Index and the Depression Symptom Index, supporting the discriminant validity of the scale. Recording each severity, frequency, and duration of symptoms also helps provide a comprehensive assessment and characterization of subthreshold symptoms.
The BPSS-FP General Symptom Index score was also higher in the clinical patient groups than in healthy controls. Symptoms, including mood lability, oppositionality, anger, self-harm, anxiety, and subthreshold/syndromal psychotic symptoms, evaluated within the context of general symptoms had been previously reported in the prodromal period of BD (Correll et al. 2014a; Van Meter et al. 2016; Faedda et al. 2019). Patients with bipolar-spectrum disorders and the MDD group had similar General Symptom Index scores. Considering psychiatric comorbidities determined with the KID-SADS-PL overlap with the wide range of internalizing and externalizing symptom-related items of the General Symptom Index, these results were not surprising.
In line with the original study evaluating the psychometric properties of the BPSS-FP, the BPSS-FP Mania Symptom Index score was significantly higher in the bipolar-spectrum disorder group, and the total score of BPSS-FP Depression Symptom Index score was higher in the MDD group (Correll et al. 2014b). Likewise, the General Symptom Index scores were similar in the bipolar-spectrum disorder and MDD groups, both of which significantly differed from healthy controls (Correll et al. 2014b). Finally, in the ROC analysis performed to further determine the discriminant validity of the BPSS-FP, the Mania Symptom Index could distinguish patients with bipolar-spectrum disorders from those with MDD. Accordingly, the Turkish version of the BPSS-FP has similar discriminant properties as the original scale in youth with mood disorders.
Strengths and limitations
The results of this study should be considered together with its strengths and limitations. First, test/retest reliability was not evaluated in this study. Second, the study groups differed in terms of age and sex. However, the age difference between the patient groups and healthy controls was only 1 year. Also, the sex difference between patient groups was related to a higher prevalence of MDD in female adolescents. Third, patients diagnosed with MDD could develop BD in the medium or long term.
Fourth, another key limitation was the cross-sectional design of the study and no predictive validity could be tested. Accordingly, studies with a longitudinal design would be helpful to examine whether the BPSS-FP can identify people who would develop a mood disorder in the follow-up. Symptom clusters of individuals with familial risk, nonmood disorders, and attenuated manic-like symptoms should be explored prospectively.
Despite the aforementioned limitations, this study demonstrated adequate psychometric quality, including internal consistency, inter-rater reliability, and convergent as well as discriminant validity of the Turkish version of the BPSS-FP. Finally, multicenter and consecutive recruitment of the cases could increase the representative power of the sample.
The results of this study will contribute to the methodology of future longitudinal studies, while data of individuals converting from at-risk status to full BD will be needed to further establish at-risk criteria and/or cutoff scores based on this interview.
Conclusions
In addition to validating the Turkish translation of the BPSS-FP, this study also confirms the good psychometric properties of the BPSS-FP, providing a quantitative assessment of attenuated manic and depressive as well as general symptomatology. Follow-up studies, including individuals who are at-risk for BD, are needed to confirm the predictive value of the BPSS-FP.
Clinical Significance
To our knowledge, this is the first non-English language validation of the BPSS-FP after the initial test of the psychometric properties of the BPSS-FP, a dedicated interview and rating scale for the earliest stages in the development of BD. Our article not only validates the Turkish translation but also independently confirms the good psychometric properties of the BPSS-FP.
Epidemiologic data suggested that the prevalence of bipolar-spectrum disorders in the United States was similar to those in other countries (Van Meter et al. 2019). However, a recent epidemiologic multicenter study did not identify BD within children aged 8–10 (Karacetin et al. 2018). Accordingly, more comprehensive assessment tools are needed for a proper assessment of BD in the Turkish language, especially for those with subthreshold symptoms. Thus, there is an increasing interest in the field in the BPSS-FP that can be used to quantify the symptomatic constellations of individuals who may be at risk for the future development of BD.
Footnotes
Acknowledgments
The authors gratefully acknowledge TÜBİTAK—BİDEB for this support. The authors also acknowledge Dr. Serkan Turan, Dr. Ayşegül Tonyalı, Dr. Remzi Oğulcan Çıray, and Dr. Ezgi Karagöz for their collaboration.
Disclosures
Dr. Correll has been a consultant and/or an advisor to or has received honoraria from: Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, IntraCellular Therapies, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedAvante-ProPhase, MedInCell, Medscape, Merck, Mitsubishi Tanabe Pharma, Mylan, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Servier, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva. He provided expert testimony for Janssen and Otsuka. He served on a Data Safety Monitoring Board for Lundbeck, Rovi, Supernus, and Teva. He has received grant support from Janssen and Takeda. He is also a stock option holder of LB Pharma.