
Abstract
Objectives:
The aim of this study was to characterize the clinical profiles, tolerability, and efficacy of two groups of antidepressants, selective serotonin reuptake inhibitors (SSRIs), and the atypical antidepressant, mirtazapine, in children and adolescents treated in a large pediatric Hematology–Oncology center.
Methods:
A review of computerized medical charts of 32 pediatric patients with cancer, from December 2011 to April 2020, was conducted. Efficacy and tolerability of antidepressant medications were retrospectively analyzed. The Clinical Global Impressions-Severity (CGI-S) and Clinical Global Impressions-Improvement (CGI-I) Scales were used to evaluate psychiatric symptoms severity before and following treatment, while the data on adverse events and drug–drug interactions were retrieved from the computerized medical records.
Results:
Thirty-two children and adolescents with cancer, 2–21 years of age (mean 14.1 ± 4.6 years), were treated with antidepressants. Fourteen patients (44%) received mirtazapine, whereas 18 patients (56%) received SSRIs: sertraline (25%), escitalopram (25%), or fluoxetine (6%). Treatment choice was dictated either by physician preference or informed by potential drug–drug interactions. The most common psychiatric diagnoses were major depressive disorders (47%), anxiety disorders (19%), and medication-induced psychiatric disorders (19%). The most common psychiatric-medical symptoms were depressed mood (94%) and anxiety (62%). CGI-S improved significantly (p < 0.05) between pretreatment and on-treatment assessments, with no statistically significant difference between SSRI and mirtazapine-treated patients. CGI-I scores at reassessment indicated improvement in most patients (84%). Adverse events of treatment were mild in all patients.
Conclusions:
The antidepressants used in this study, SSRIs and mirtazapine, were effective and well tolerated in children and adolescents with cancer and psychiatric comorbidities. Given the high rates of depression and anxiety in children with cancer, large-scale, multisite, prospective clinical trials of antidepressants are warranted.
Introduction
Pediatric cancer is undoubtedly one of the most difficult life events for a child and his family (Bruce 2006; Long and Marsland 2011). Despite improving survival rates, the diagnosis and treatment of childhood cancer still impose a considerable physical and mental burden on patients. Commonly identified stressors include physical side effects, such as fatigue, nausea, and pain, as well as more social stressors such as appearance changes, missing home due to hospital confinement, and limited social support (Sharp et al. 2017). Many young cancer patients experience psychiatric comorbidity; depression, anxiety, and adjustment symptoms most commonly precipitate psychiatric referrals in this patient population (Sohn et al. 2017; Shim et al. 2018; Samsel et al. 2019). In children suffering from cancer, the reported rates of depression and anxiety disorders vary between of 7% and 32%, probably depending on the methodology of individual studies.
The diagnosis of major depressive disorder in children is complicated by many factors, including variable age-dependent presentations of depression; varying perceptions of the child's symptoms between caregivers (parents and clinicians); and the individual trajectory of any patient's treatment course (diagnosis, induction therapy, relapse, and end-of-life care are examples). Of pediatric cancer patients referred for psychiatric evaluation, some meet criteria for major depression or anxiety disorders, while others exhibit dysthymia, depressed mood, or an adjustment disorder (Kersun and Elia 2007). Premorbid psychiatric illness and parental distress contribute to the psychiatric morbidity seen in pediatric oncological patients (Okado et al. 2014).
Differentiating between the clinically significant symptoms of a mood disorder, foreseeable adjustment difficulties, and disease/treatment-related effects can be challenging due to frequent overlap of cancer symptomatology and diagnostic criteria for depression (Portteus et al. 2006; Phipps et al. 2012). Anhedonia, weight or appetite changes, insomnia or hypersomnia, psychomotor agitation or retardation, fatigue or loss of energy, and diminished ability to concentrate are frequent in children with cancer; determining an oncologic versus a psychiatric etiology can be difficult. These challenges require a team approach that includes effective communication between oncologists, nurses, mental health and child professionals, and social support teams.
Attention to the mental health needs of these children has evolved into a specialty, psycho-oncology, which is increasingly being recognized as an essential component in the already complex care of children with cancer and their families (Datta et al. 2019).
The detrimental impact of depression and anxiety on various outcomes in cancer patients has been well established (Shim et al. 2018). Depression amplifies medical disease-related disability, impairs quality of life, and has been repeatedly shown to be associated with poor medical outcomes and early death in children who suffer from life-threatening medical conditions (Shemesh et al. 2002). Untreated depression may also interfere with immune system functioning (Apter et al. 2003), potentially influencing the incidence of infectious complications in these already immunocompromised patients.
Furthermore, depression and anxiety are associated with treatment nonadherence (Kennard et al. 2004; Portteus et al. 2006; Kurtz and Abrams 2010; Arrieta et al. 2013; Caruso et al. 2017; Shim et al. 2018), which can have devastating ramifications on treatment efficacy and the risk of disease relapse (Lauer 2015). Nonadherence to treatment regimens in critically ill patients is addressed in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (American Psychiatric Association 2013).
Psychopharmacological management serves as an important element of a comprehensive multidisciplinary approach to the care of pediatric cancer patients (Pao et al. 2006; Samsel et al. 2019). Selective serotonin reuptake inhibitors (SSRIs) are the most prescribed antidepressants in children, despite diverse side effects, including the 2004 black box warning issued by the FDA. Prescription of SSRIs is common practice among pediatric oncologists, often in the absence of (or before) consultation with mental health professionals (Kersun and Kazak 2006; Portteus et al. 2006; Pao et al. 2009; Phipps et al. 2012; Mavrides and Pao 2014).
Despite widespread use, there are limited published studies exploring the use of psychopharmacological treatments for depression and anxiety in children with cancer. Most studies focus on the use of SSRIs, with little data on other antidepressants, such as mirtazapine, which holds a unique pharmacological profile (Gothelf et al. 2005; DeJong and Fombonne 2007; Kersun and Elia 2007).
Despite the absence of definitive clinical data regarding the efficacy and tolerability of antidepressants in children (Steele et al. 2015), this class of drugs seems to be beneficial for the treatment of symptoms of depression and anxiety, such as depressed mood, loss of appetite, fatigue, anxiety, and cognitive impairment, as well as for other associated symptoms such as pain, gastrointestinal tract distress, wasting, hot flashes, vasomotor symptoms, sleep problems, and pruritus in children and in adults (Pao et al. 2006; Zaini et al. 2018; Belinskaia et al. 2019).
In the absence of large, controlled studies, guidelines for the use of psychopharmacological treatment of children with cancer and comorbid psychiatric diseases have yet to be established. The goal of this retrospective study is to describe our experience with the administration of antidepressants in a large pediatric Hematology–Oncology center. We evaluated our experience with the use of antidepressants, including efficacy and tolerability, and assessed potential drug interactions between the psychopharmacological treatments and medications prescribed for the treatment of malignant disease and as supportive care.
Methods
Study design
A review of computerized medical records from December 2011 to April 2020 was conducted at the Hematology–Oncology Department of the Schneider Children's Medical Center in Israel. The department includes an inpatient unit, a stem cell transplantation unit, and a day hospital.
Study population and data collection
The medical records of children and adolescents treated in the Hematology–Oncology Department who had been evaluated by members of the Liaison Psychiatry Unit (five different child psychiatrists) at the request of the patient-care team, and who had been treated with antidepressant medication, were reviewed. Patients who were already being treated with antidepressant medications at the time of initial psychiatric assessment were excluded, as were patients whose charts lacked full documentation of study parameters; these included full demographic information and pre- and posttreatment psychiatric assessments. The same child psychiatrist conducted the initial and follow-up assessments of each participant. The second assessment was scheduled as needed for each patient. Extraction of deidentified data was undertaken by two trained clinical pharmacists (O.P. and I.V.).
The study was approved by the Institutional Review Board of the Rabin Medical Center, Petah Tikva, Israel.
Measures
Demographic and clinical characteristics
Demographic data were collected. Concurrent medications were recorded and evaluated by a clinical pharmacist for potential drug–drug interactions with SSRIs or mirtazapine for each patient. Severity and response of symptoms were measured by the Clinical Global Impressions-Severity (CGI-S) and the Clinical Global Impressions-Improvement (CGI-I) scales.
Psychiatric-medical symptoms
Major psychiatric-medical symptoms, as noted by the medical team and by the liaison psychiatrist, were retrieved, including irritability/agitation, depressed mood, insomnia, anorexia, anxiety, nonadherence, suicidality, psychosis, hypomania/mania, involuntary movements, pruritus, and somatization. Somatization was defined as symptoms such as pain or neurological problems that may be related to a physical cause but cause excessive levels of distress (American Psychiatric Association 2013).
Psychiatric diagnoses
Diagnoses were made by liaison child psychiatrists in accordance with DSM-5 criteria. Psychiatric diagnoses that were considered to be secondary to the patient's medical condition or to adverse effects of concurrent medications were noted.
Clinical Global Impressions-Severity scale
The symptomatic severity at the time of referral, as part of clinical care, was assessed by the liaison psychiatrist using the CGI-S Scale, which uses seven degrees, ranging from 1 (“not ill at all”) to 7 (“very ill compared with other patients”) (Guy 2000).
The Clinical Global Impressions-Improvement scale
The effects of treatment with SSRIs and mirtazapine were assessed by the CGI-I scale. Similar to the CGI-S, this is a 7-point scale, which rates change from baseline as 1 (“very much improved”), 2 (“much improved”), 3 (“minimally improved”), 4 (“no change”), 5 (“minimally worse”), 6 (“much worse”), or 7 (“very much worse”), with zero representing “not assessed” (e.g., patient stopped medication before second assessment) (Guy, 2000).
Antidepressant-induced adverse events
Antidepressant-related adverse effects were collected from patients' computerized medical records, and rated retrospectively using the Common Terminology Criteria for Adverse Events (CTCAE, 2017).
Drug–drug interactions
Potential drug–drug interactions between the medication roster and SSRIs or mirtazapine were assessed by drug interaction reports derived from three different pharmacological databases (Clinical Pharmacology 2021; Lexicomp 2021; Micromedex 2021). A potential drug–drug interaction profile was produced according to the clinical significance and likelihood of each interaction.
Statistical analyses
Analyses were conducted using the Statistical Package for the Social Sciences Version 20 (Released 2011; IBM Corp., Armonk, NY, USA). Descriptive data are presented as mean ± standard deviation (SD), or rates (%). Two-tailed Student's t-test was used to compare continuous variables (e.g., age) between those treated with SSRIs versus mirtazapine. Chi-squared or Fisher's exact tests were used to compare categorical parameters (e.g., gender, oncological diagnoses, psychiatric diagnoses rates, and psychiatric-medical symptoms) between those treated with SSRIs versus mirtazapine. Multivariate General Linear Model was used to compare changes in CGI-S scores over time between the two groups. Similarly, Univariate analysis of variance (ANOVA) was used to compare CGI-I values between the two groups, where interval of days between assessments was used as a covariate. Results are expressed as rates or mean ± SD.
Results
Demographic and clinical characteristics
The initial sample consisted of 37 computerized medical records of children and adolescents who had been evaluated by a child psychiatrist and been treated with an antidepressant medication. None of the patients included in the study had a prior history of antidepressant treatment. Five patients were excluded from the analysis (one who was treated with duloxetine at the time of referral, two patients who had been treated with antidepressants in the past, and two patients with incomplete documentation in their medical records). The final study group consisted of 32 patients between the ages of 2–21 years (mean age of the total cohort was 14.1 ± 4.6 years). The median time interval between primary oncologic diagnosis and referral to the liaison psychiatry service was 18.6 months.
At the time of psychiatric evaluation, 41% of the patients were already receiving one or more psychotropic medications (16% were taking ≥2 drugs). Twenty-five percent were already receiving benzodiazepines (clonazepam 16%, brotizolam 13%, lorazepam 3%, midazolam 3%), 19% were treated with antipsychotics (olanzapine 9%, risperidone 6%), mood stabilizers 3%, cannabinoids 3%, and promethazine 3%.
At the time of psychiatric evaluation, 69% of the patients were receiving nonpsychiatric medications likely to induce neuropsychiatric adverse events, including supraphysiological (38%) or tapering (19%) doses of corticosteroids [hydrocortisone (22%), dexamethasone (13%), prednisone (13%), methylprednisolone (6%), and fludrocortisone (3%)], which are often associated with behavioral and mood changes, such as manic, depressive, and psychotic symptoms (Caplan et al. 2017).
Levetiracetam (19%) is often associated with neuropsychiatric symptoms, such as aggression, agitation, anxiety, depression, apathy, and depersonalization (Josephson et al. 2019; Keppra 2019). Sixteen percent of patients were treated with voriconazole, which is occasionally associated with nervousness, agitation, and confusion (Zonios et al. 2008). Voriconazole may also be associated with visual hallucinations, which have been reported in 2.4% of patients during clinical trials (VFEND 2019).
The antidepressants prescribed were either SSRIs (sertraline, escitalopram, fluoxetine) or mirtazapine. Eighteen (56%) patients were treated with SSRIs—eight (25%) received sertraline, dose range 25–50 mg (mean dose 47 ± 8.8 mg), seven (22%) received escitalopram, dose range 5–10 mg (mean dose 9.2 ± 1.9 mg), and three (17%) received fluoxetine, dose range 10–20 mg (mean dose 17 ± 5.8 mg). Fourteen (44%) patients were treated with mirtazapine, dose range 3.75–30 mg, mean dose 18 ± 10 mg [3.75 ± 0 mg in preschoolers (<6), 15 ± 13 mg in school-aged children (6–12 years), 20.25 ± 8.7 mg in adolescents and young adults (>12 years)]. Treatment was determined by a consensus meeting of the medical team and the clinical pharmacists.
Demographic characteristics of the two groups, including distribution of oncological diagnoses and disease phases, were similar and are presented in Table 1. Mirtazapine was administered more frequently in recipients of stem cell transplants (p < 0.01). Malignancies were grouped into one of four major categories (Chmielecki et al. 2017); there were no statistically significant differences between the four malignancy groups in the length of time to psychiatric consultation. Thirty-one percent of patients were receiving treatment for relapsed or refractory malignancy at the time of consultation with the liaison psychiatrist.
Demographic and Clinical Characteristics of the Study Population (N = 32)
BMT, bone marrow transplantation; SSRI, selective serotonin reuptake inhibitor.
Psychiatric-medical complaints documented by the Oncology Team
The most prevalent complaints reported by the medical team and precipitating psychiatric consultation were depressed mood (69%), anxiety (28%), and nonadherence with medical therapy (22%). Less frequent complaints included insomnia (19%), pruritus (12%), irritability/agitation (9%), loss of appetite (3%), and somatization (3%). Sixteen patients (50%) had two or more psychiatric symptoms as the cause of referral for psychiatric consultation.
Psychiatric-medical symptoms documented by the Liaison Psychiatrist
The psychiatric-medical symptoms reported by the liaison psychiatrists are presented in Table 2. Nearly all patients had more than one psychiatric symptom (31 patients out of 32). Nineteen percent had 2 symptoms, 22% had 3 symptoms, 25% had 4 symptoms, and nearly one-third of patients had ≥5 symptoms. The most prevalent symptoms reported were depressed mood (94%), followed by anxiety (62%) insomnia (59%), and irritability (56%). There were no statistically significant differences between the two medication groups regarding psychiatric-medical symptoms, except for pruritus, which was more prevalent in the mirtazapine treatment group (p < 0.05).
Rates of Psychiatric-Medical Target Symptoms for Treatment with Antidepressants (Selective Serotonin Reuptake Inhibitors and Mirtazapine) in Pediatric Oncology and Bone Marrow Patients (N = 32)
SSRI, selective serotonin reuptake inhibitor.
Psychiatric diagnoses
The psychiatric diagnoses of the 32 patients reviewed in this study are presented in Table 3. Twenty-two percent of the patients had more than one diagnosis. The distribution of psychiatric diagnoses was similar among mirtazapine and SSRI-treated patients. All medication-induced psychiatric disorders were related to corticosteroid usage (n = 6). Three out of six patients were not receiving steroids at the time of the second assessment. Psychiatric disorders due to another medical condition were present in 12.5% of patients and included brain tumors, metastatic brain tumors, and hepatic encephalopathy.
Psychiatric Diagnoses of the Study Population (N = 32)
SSRI, selective serotonin reuptake inhibitor.
Clinical Global Impressions scores
The mean CGI-S score at first assessment of the entire cohort was 5 ± 1.07 (4.7 ± 0.9 and 5.4 ± 1.1 in the SSRIs and mirtazapine recipients, respectively, with no between-group statistically significant difference). Following the initiation of treatment, patients were reassessed at a median of 31 days, (quartile percentiles: 25%: 13 days, 50%: 25 days, 75%: 41 days). The mean CGI-S at reassessment (3.4 ± 1.3), was significantly improved as compared with the first pretreatment time point (F 2,28 = 156, p < 0.001; see Fig. 1) with no statistically significant difference between SSRIs and mirtazapine-treated patients (3.1 ± 1.2 vs. 3.9 ± 1.4, p > 0.15; see Fig. 2). Univariate ANOVA did not reveal any significant effect of reassessment intervals on the model ( F 2,28 = 0.46, p > 0.63).
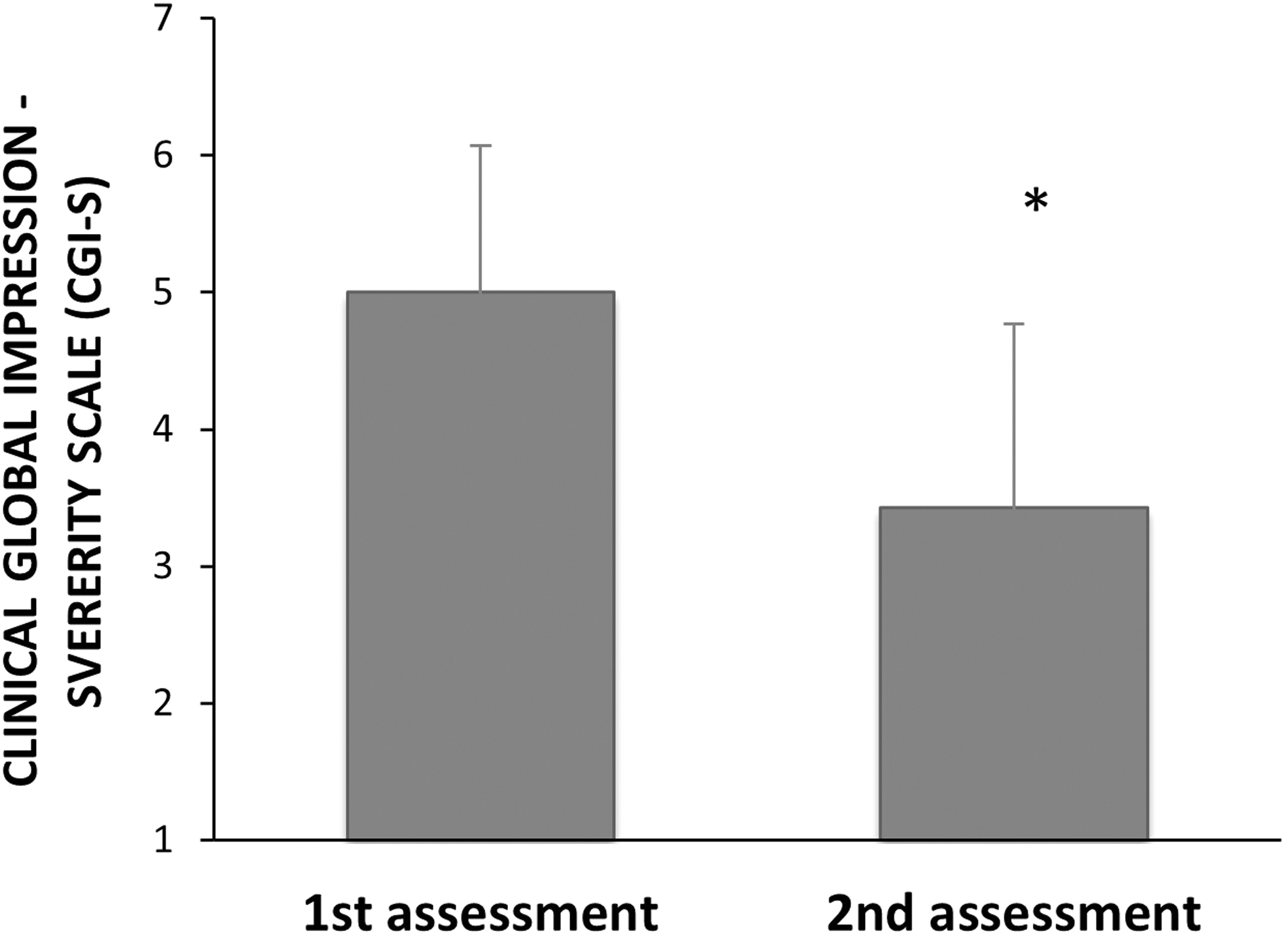
CGI-S Scores of pediatric oncologic patients (n = 32) at first and second assessments, that is, before and after the antidepressant treatment, respectively. Antidepressant treatment significantly (F 2,28 = 156, p < 0.001) reduced CGI-S scores. There were no statistically significant differences in CGI-S scores between the SSRI's and mirtazapine groups (3.1 ± 1.2 vs. 3.9 ± 1.4, p > 0.15). The effect of number of days between assessments between groups was not significant (F 2,28 = = 0.46, p > 0.63). CGI-S, Clinical Global Impressions-Severity.

CGI-S scores of pediatric oncologic patients (n = 32) treated with SSRI's versus mirtazapine. No statistically significant difference was found between CGI-I scores of SSRI's and mirtazapine groups (2.6 ± 1.2 vs. 2.2 + 1.2, p > 0.40). The effect of number of days between assessments was not significant (F 2,28 = 0.46, p > 0.63). CGI-I, Clinical Global Impressions-Improvement.
Twenty-five of 32 patients (78%) showed improvement in the CGI-I score—6 were “very much improved,” 13 “much improved,” 6 “minimally improved,” and 6 showed neither improvement nor aggravation. One patient, who discontinued medication due to side effects, was not included in the analysis. There was no statistically significant difference in CGI-I score between the two groups of antidepressants (2.6 ± 1.2 vs. 2.2 ± 1.2, p > 0.40).
Antidepressant-induced adverse events
Four patients (13%; treated with escitalopram, fluoxetine, sertraline, and mirtazapine) experienced four low-grade (1–2 according to CTCAE grading) treatment-related adverse events (see Table 4; CTCAE, 2017). Each reported a single side effect. The abnormal movements and agitation observed with SSRI's treatment were both transient, disappeared spontaneously, and had no major safety impact or patient distress. The differential diagnosis of abnormal movements includes akathisia, transient tics, agitation, or irritability. In general, agitation with the use of SSRI's presents a clinical diagnostic dilemma in child psychiatry. In our center, we regard the agitation as being part of the activation often seen with the use of SSRI's. Despite the mild nature of the side effects, two out of the four discontinued the medication, with one patient choosing to trial a replacement agent.
Antidepressants' Adverse Events in the Pediatric Oncologic Patients (N = 32)
CTCAE, Common Terminology Criteria for Adverse Events v5.0.
SSRI, selective serotonin reuptake inhibitor.
Drug–drug interactions
The drug of choice, as well as dose adjustments, were tailored according to drug–drug interaction assessment and the medical condition of each patient. A potential drug–drug interaction profile between patients' preexisting medications and either SSRIs or mirtazapine were assessed considering both pharmacodynamic and pharmacokinetic interactions and are listed in Table 5.
Review of the Interaction Profile of the Antidepressants (Selective Serotonin Reuptake Inhibitors and Mirtazapine) with the Specific Medications Administered to the 32 Patients
Source: Clinical Pharmacology (2020); Lexicomp (2020); Micromedex (2020).
CNS, central nervous system; NSAID, nonsteroidal anti-inflammatory drug; SSRI, serotonin selective reuptake inhibitor; 5HT3, 5-hydroxytryptamine type 3.
Pharmacodynamic interactions are classified according to cumulative potential effects, while pharmacokinetic interactions are classified according to the mechanism of the interaction. Table 5 includes potential clinically significant drug–drug interactions.
Fluoxetine is a potent inhibitor of CYP2D6 and a moderate inhibitor of CYP2C19 and alters blood levels of other medications that are cleared or deactivated by these enzymes. Therefore, it was the drug of choice for only two patients (6%) in our cohort.
Discussion
The diagnosis and treatment of childhood cancer impose considerable physical and psychological burdens on patients; psychopharmacological interventions, together with other nonpharmacological treatments, are an important element of the interdisciplinary treatment approach of these children (Samsel et al. 2019). The use of antidepressants in the treatment of anxiety and depression in children with cancer has increased (Pao et al. 2006; Kurtz and Abrams 2010), but there are only few small studies on the treatment of these challenging patients (Gothelf et al. 2005; DeJong and Fombonne 2007; Kersun and Elia 2007; Steele et al. 2015).
Our retrospective study reviews the use of two groups of antidepressants prescribed by liaison psychiatrists at the Hematology–Oncology Department of the Schneider Children's Medical Center in Israel. Our main finding shows that the use of SSRIs and mirtazapine in this population is well tolerated, in a wide age range, with benefits that outweigh adverse reactions. We demonstrated a combined clinical and pharmacological approach through use of a multidisciplinary team consisting of a child psychiatrist, clinical pharmacist, and pediatric oncologist.
The diagnosis of psychiatric disorders in cancer patients can be confusing and sometimes even misleading. There is considerable and challenging overlap between the presentation of psychiatric illness in general and mood disorders in particular and the symptomatology that follows the diagnosis of cancer, as well as the adverse effects of its treatment (Portteus et al. 2006; Phipps et al. 2012).
Such symptoms as anhedonia, weight or appetite loss, insomnia, psychomotor agitation or retardation, fatigue or loss of energy, and diminished ability to concentrate are frequent in children with cancer. Concomitant somatic symptoms present a special challenge to the mental health practitioner, as they may be signs of either the primary disease or of an underlying mental illness. Thus, standard depression criteria and questionnaires may be of more limited utility in medically ill patients (Cohen-Cole and Stoudemire 1987; Canning and Kelleher 1994; Knapp and Harris 1998), while a symptom-oriented approach may be more appropriate (Fleishman 2004; Pao et al. 2006; Peled et al. 2020). Clearly, a “one-size-fits-all” approach is inadequate both in the diagnostic and treatment contexts.
Nearly all our patients (94%) reported “depressed mood” as a symptom that led to the use of antidepressants, even though half of our patients did not fulfill the DSM-5 criteria of a major depressive disorder. It has been reported that depression in cancer patients often does not reach cutoff thresholds for “clinically significant depression,” but nonetheless, depressive symptoms negatively affect patients' quality of life (Mavrides and Pao 2014).
The most frequent psychiatric diagnosis in this study was major depressive disorder (47%), followed by anxiety and medication-induced psychiatric disorders (19% each), findings similar to those reported in adults with cancer (Cullivan et al. 1998). At the time of psychiatric evaluation, 69% of the patients were receiving different nonpsychiatric medications likely to induce neuropsychiatric adverse events, although all the medication-induced psychiatric disorders in our cohort were attributable to corticosteroid usage. The use of systemic corticosteroids can induce various psychiatric changes, ranging from behavioral and mood changes to psychotic symptoms (Caplan et al. 2017). It is noteworthy that corticosteroid-associated psychopathology can occur during therapy, during steroid taper, or following discontinuation of the drug (Drozdowicz and Bostwick 2014).
The beneficial therapeutic effect of antidepressants in our patients was similar in SSRIs and mirtazapine-treated patients. Adverse effects of treatment were infrequent and mild, but of sufficient magnitude to lead two patients to stop treatment. Among our mirtazapine-treated patients, elevated liver enzymes and jaundice were noted in one patient, and causality was not demonstrated.
The investigated antidepressants in this study differ in their pharmacological profiles. SSRIs tend to have similar side-effect profiles, however, certain SSRIs may be more likely to cause specific side effects (Nierenberg et al. 2008). Common SSRI side effects include sexual dysfunction, drowsiness, weight gain, insomnia, agitation, anxiety, dizziness, orthostatic hypotension, headache, and dry mouth. The mild side effects reported by the three patients treated within the relatively narrow range of SSRI dosages prescribed are compatible with the side-effect profile of SSRIs.
Among antidepressant medications, mirtazapine possesses a unique pharmacological profile, potentially rendering it effective in treating multiple symptoms such as depression, anxiety, sleep disorders, cachexia, and neuropathic pain (Davis et al. 2002; Lovell and Ward 2011; Zaini et al. 2018). Mirtazapine, a noradrenergic and specific serotonergic receptor antagonist, has proved effective in the treatment of depression among patients with cancer (Lovell and Ward 2011; Economos et al. 2020).
Although data regarding the use of mirtazapine in children with cancer are sparse, the drug was shown to be safe and well tolerated in children (Gray et al. 2018). Mirtazapine presents a variety of side effects, with drowsiness and dizziness being the most common (Economos et al. 2020). Moreover, some of the commonly described “adverse” effects of mirtazapine, such as sedation, appetite stimulation, and weight increase, are exclusive to mirtazapine and have potential palliative benefits.
Additionally, recent studies describe mirtazapine's utility in relieving refractory pruritus (Demierre and Taverna 2006; Sheen et al. 2008; Lee et al. 2016; Bromberg et al. 2020; Fawaz et al. 2021), making it the go-to medication for patients with graft versus host disease, who require treatment for concurrent depression (Davis et al. 2002; Lovell and Ward 2011; Zaini et al. 2018). For these and other reasons, mirtazapine was prescribed to a particularly young patient of ours (2 years old); the medication was well tolerated and proved to be beneficial.
The precipitation of bleeding due to serotonin depletion by SSRIs has been described and referred before in postchemotherapy and poststem cell transplantation thrombocytopenic patients (Tseng et al. 2010, 2013); None of the patients in our cohort experienced SSRI-induced thrombocytopathy and bleeding. Nevertheless, we have encountered two cases of laboratory-confirmed SSRI-induced inhibited platelet aggregation and critical bleeding in the past, which have raised our awareness to this adverse event. Therefore, we preferred mirtazapine in patients who were at risk for bleeding (Clinical Pharmacology 2021).
Children with cancer often receive many different medications, both for treatment of the primary oncological disease and for treatment or prevention of infectious and noninfectious complications of therapy. Drug–drug interactions between concomitant medications and antidepressants are a cause of concern. Antidepressants must be chosen not only based on potential efficacy and side-effect profile, but with careful attention to the proposed agent's toxicity and interactions with the medications that the patient already receives. Table 5 illustrates a profile of drug–drug interactions that should assist cautious choice of antidepressants in children with cancer.
All SSRIs may inhibit one or more cytochrome P450 drug-metabolizing enzymes, causing pharmacokinetic interactions with many drugs. Most SSRIs are weak inhibitors of CYP450 enzymes and unlikely to cause clinically relevant pharmacokinetic interactions. In contrast, fluoxetine is a potent inhibitor of CYP2D6 and a moderate inhibitor of CYP2C19, suggesting that its use may be inappropriate in children with cancer and explaining its infrequent use in our cohort. Fluvoxamine was not prescribed in our cohort, as it is a potent inhibitor of CYP1A2, with moderate effects on CYP2C9, CYP2C19, and CYP3A4. Among SSRIs, escitalopram and sertraline are the drugs of choice for situations in which drug–drug interactions are a concern (Preskorn 1997; Labbate et al. 2010).
The narrow therapeutic window and wide inter- and intrapatients' variability of many of these drugs require initial and ongoing consultation with a clinical pharmacologist during the treatment, taking into consideration the list of concomitant medications involved in the course of the oncological therapy.
We also note that antidepressants are often prescribed by pediatric oncologists without consultation with a liaison psychiatrist or a clinical pharmacologist (Kersun and Kazak 2006; Portteus et al. 2006; Pao et al. 2009; Phipps et al. 2012; Mavrides and Pao 2014). Forty-one percent of the patients was already receiving one or more psychotropic medications at the time of psychiatric evaluation, highlighting the need for access to a specialized psychiatric consultation. Rigorous follow-up by mental-health professionals is important to monitor the efficacy of treatment and to permit timely change of treatment as dictated by the dynamic nature of the treatment trajectory of children with cancer.
The major limitations of this study are its open, retrospective nature and its small sample size. The treatment outcome was assessed based on the clinical global impressions of the psychiatrist at the time of examination, in an unblinded process (the evaluator knew both that medication had been given and which agent had been used, potentially affecting his or her assessment of the magnitude of improvement). Standardized scales for psychiatric evaluation were not used. Finally, the current study presents the practice patterns in one treatment center; its results require confirmation in other sites. We hope that this report will encourage large-scale, multisite, prospective studies of the use of antidepressants in Pediatric Oncology practice.
Conclusions
The antidepressants (fluoxetine, escitalopram, sertraline, and mirtazapine) used in this study population were found to be well tolerated and beneficial, suggesting a role in ameliorating acute psychiatric symptoms in children and adolescents with cancer. Clinicians may elect to utilize some secondary effects of mirtazapine for palliation of symptoms associated with cancer and its treatment in young patients.
Clinical Significance
Our findings have important implications for pediatric oncologists; pediatricians providing supportive care for children with cancer in both outpatient and inpatient settings; and child psychiatrists. Furthermore, our study has the benefit of including a wide age range (2–21), a unique strength among published works in the field. Our study emphasizes the importance of psychiatric and pharmacological evaluations of children with cancer before starting antidepressant therapy, to provide safe and efficacious management and monitoring. The antidepressants used in this study population were found to be beneficial and well tolerated. Prospective clinical trials are needed to explore the relative benefits of different specific antidepressants and to validate our findings. Such studies will facilitate the elaboration of specific guidelines regarding the use of antidepressants for children with malignant diseases.
Footnotes
Acknowledgments
The authors thank Lior Adler, MD, Dan Farbstein, MD, Ella Kimmel-Tamir, MD, Ella Yaniv, MD, and Asaf Yaakoby, MD (Department of Psychological Medicine, Schneider Children's Medical Center of Israel, Petah Tikva, Israel), for their help in psychiatric assessments: Georgina Martin, MD (Royal Preston Hospital, United Kingdom), for her invaluable help as a research assistant; and Rachelle Aviv for her assistance in editing and proofreading.
Disclosures
No competing financial interests exist.