
Abstract
Objective:
Ongoing studies are focused on adapting transcranial magnetic stimulation (TMS) for the treatment of major depressive disorder in adolescent humans. Most protocols in adolescent humans to date have delivered daily 10 Hz prefrontal stimulation with mixed results. Novel TMS dosing strategies such as accelerated TMS have recently been considered. There are knowledge gaps related to the potential clinical and pragmatic advantages of accelerated TMS. This pilot study compared the behavioral effects of a standard daily and accelerated low-intensity TMS (LI-TMS) protocol in an adolescent murine model of depression.
Methods:
Male adolescent Sprague Dawley rats were placed in transparent plexiglass tubes for 2.5 hours daily for 13 days as part of a study to validate the chronic restraint stress (CRS) protocol. Rats subsequently received 10 minutes of active or sham 10 Hz LI-TMS daily for 2 weeks (standard) or three times daily for 1 week (accelerated). Behavior was assessed using the elevated plus maze and forced swim test (FST). Hippocampal neurogenesis was assessed by injection of the thymidine analogue 5-ethynyl-2′-deoxyuridine at the end of LI-TMS treatment (2 weeks standard, 1 week accelerated), followed by postmortem histological analysis.
Results:
There were no significant differences in behavioral outcomes among animals receiving once-daily sham or active LI-TMS treatment. However, animals treated with accelerated LI-TMS demonstrated significant improvements in behavioral outcomes compared with sham treatment. Specifically, animals receiving active accelerated treatment showed greater latency to the first immobility behavior (p < 0.05; active: 130 ± 46 seconds; sham: 54 ± 39 seconds) and increased climbing behaviors (p < 0.05; active: 16 ± 5; sham: 9 ± 5) during FST. There were no changes in hippocampal neurogenesis nor any evidence of cell death in histological sections.
Conclusions:
An accelerated LI-TMS protocol outperformed the standard (once-daily) protocol in adolescent male animals with depression-like behaviors induced by CRS and was not accompanied by any toxicity or tolerability concerns. These preliminary findings support the speculation that novel TMS dosing strategies should be studied in adolescent humans and will inform future clinical protocols.
Introduction
Repetitive transcranial magnetic stimulation (TMS) is a noninvasive brain stimulation technique that is Food and Drug Administration approved and widely delivered as a therapy for treatment-resistant major depressive disorder (MDD) in adult humans (Horvath et al. 2010).
Currently approved TMS protocols for the treatment of depression involve daily (weekday) stimulation, using 10 Hz frequency or intermittent theta burst stimulation, for 4–6 weeks. Recently, accelerated treatment protocols (multiple daily stimulation sessions for 1–2 weeks) have been explored in humans as an alternative dosing method for TMS (Loo et al. 2007; Holtzheimer et al. 2010; George et al. 2014; McGirr et al. 2015; Fitzgerald et al. 2018; Modirrousta et al. 2018). However, the design of accelerated protocols varies widely between studies (Sonmez et al. 2019), reducing statistical power. As a result, to date, there is no clear evidence of a clinical or biological benefit of accelerated over standard protocols (Fitzgerald et al. 2018; Modirrousta et al. 2018).
There are ongoing efforts to adapt TMS treatment for MDD in adolescent humans. Most of these studies have examined standard once-daily, 10 Hz TMS delivered to the left prefrontal cortex. Recently, a randomized controlled trial failed to demonstrate a significant difference between active and sham TMS in adolescents with MDD (Croarkin et al. 2021). There are a number of conceptual and methodological challenges in the study of TMS in adolescents (Lisanby 2017; Oberman et al. 2021). As with historical pharmacology trials, it is likely that effective TMS strategies in adolescents with MDD will require novel dosing strategies. Accelerated TMS dosing has potential neurophysiological and pragmatic advantages that warrant study in adolescents with MDD (Croarkin and Rotenberg 2016).
Murine models have utility in high-throughput dosing studies and refining clinical protocols for research in adolescent MDD. For example, recent work examined the effectiveness of different TMS intensities in murine models, showing that low intensities (10–50 mT; 1%–5% of rodent motor threshold) had significant behavioral and neurological effects (Makowiecki et al. 2014; Tang et al. 2016, 2018; Poh et al. 2018). In a mouse model of treatment-resistant depression, 10 Hz TMS delivered at an intensity of 50 mT reduced psychomotor agitation and increased cortical and hippocampal brain-derived neurotrophic factor and hippocampal neurogenesis levels (Heath et al. 2018).
In addition, magnetic resonance imaging studies in healthy rats demonstrate that 10 Hz TMS at 13 mT has long-lasting effects on resting-state networks and neurochemistry (Seewoo et al. 2019). Low-intensity stimulation also has benefits in human studies (Huang and Rothwell 2004; Huang et al. 2005; Boggio et al. 2010) and offers advantages over high intensity by reducing side effects (Wassermann 1998; Rossi et al. 2009) and equipment cost.
This pilot study compared the behavioral effects of the standard 10 Hz protocol (one stimulation session per weekday) and an accelerated 10 Hz low-intensity TMS (LI-TMS) protocol (three stimulation sessions per weekday) using LI-TMS (13 mT) in a validated chronic restraint stress (CRS) adolescent rat model of depression (Lee et al. 2009; Henckens et al. 2015; Wang et al. 2017; Seewoo et al. 2020) with the aims of examining tolerability and efficacy, while informing the development of a human protocol.
Materials and Methods
Animals
The experimental protocol was approved by the University of Western Australia Animal Ethics Committee (RA/3/100/1640) and conducted in accordance with the National Health and Medical Research Council Australian code for the care and use of animals for scientific purposes.
Adolescent male Sprague Dawley rats (n = 20; 242.79 ± 14.18 g; 6–7 weeks old) were sourced from the Animal Resources Centre (Canning Vale, Western Australia) and housed in pairs under temperature-controlled conditions on a 12-hour light–dark cycle. Food and water were provided ad libitum, except during the CRS procedure and fasting before the sucrose preference test. All rats acclimatized to their new environment for 1 week following their arrival. Depression-like behaviors were induced in the rats using the CRS model (Bravo et al. 2009; Ulloa et al. 2010; Stepanichev et al. 2014), as validated in the study by Seewoo et al. (2020). This involved placing the rats in individual transparent acrylic tubes for 2.5 hours each day, for 13 consecutive days.
Repetitive TMS
LI-TMS was delivered at 10 Hz using a custom-built round coil (described in detail in Grehl et al. 2015; Seewoo et al. 2018). Sham stimulation was delivered with the pulse generator switched off to act as a handling control. Animals were placed on the investigator's lap, with the coil held against the top-left side of the animal's head for the duration of the treatment session. The coil was placed between the left eye and ear to target the left prefrontal cortex to reflect clinical protocols used for human patients. Each treatment session was conducted during the afternoon, commencing between 12:00 and 13:30.
Animals were randomly assigned to one of four groups (n = 5 per group): standard active treatment, standard sham treatment, accelerated active treatment, and accelerated sham treatment. Following CRS, animals in the standard treatment groups received LI-TMS for 10 minutes once daily, 5 days/week for 2 weeks. Animals in the accelerated treatment groups received 10 minutes of LI-TMS three times daily (1 hour apart) for 5 days/week for 1 week. The duration of treatment in this pilot study was half of the conventional duration for each type of treatment (2 weeks for standard and 1 week for accelerated) and was chosen to provide a rapid insight into the relative efficacy of standard and accelerated protocols.
Behavioral testing
All behavioral testing occurred between 08:30 and 11:00. The full behavioral videos can be obtained from the corresponding author upon request. Animals first underwent the elevated plus maze (EPM) test (see Walf and Frye 2007 for full protocol) to assess the presence of anxiety-related behaviors. Animals were placed in the center of a plus-shaped maze, facing an open arm, and allowed to explore the maze for 5 minutes. The sucrose preference test (data not shown) was conducted following the EPM but yielded unreliable results as previously reported (Seewoo et al. 2020). The forced swim test (FST) was conducted last and followed the protocol by Slattery and Cryan (2012), to evaluate learned-helplessness (see Seewoo et al. 2020 for full protocol). Before the first test, animals were exposed to the test conditions in a pretest (Slattery and Cryan 2012), where they were placed in water for 10 minutes.
For EPM and FST, behavior was recorded using a GoPro Hero7 (GoPro, Inc.) camera and the footage was analyzed offline (full 5 minutes for EPM, the first 5 minutes for FST) by a trained experimenter blind to condition and time point. For EPM, exploration was determined through the number of exits and time spent in the open and closed arms. Number of occurrences and time spent exhibiting rearing and grooming behaviors were also measured to quantify stress responses. For FST, the video was split into 5 second segments. Each segment was analyzed to determine the predominant behavior. Behaviors were classified as climbing, swimming, or immobility behaviors. Latency to the first segment with predominant immobility was also determined.
Histological study of neurogenesis
On the last day of LI-TMS delivery, rats received intraperitoneal injections of the thymidine analogue 5-ethynyl-2′-deoxyuridine (EdU, two doses of 50 mg/kg, 8 hours apart). Animals receiving daily LI-TMS were euthanized 2 weeks after the last LI-TMS session, whereas animals receiving the accelerated LI-TMS were euthanized 1 week after the last LI-TMS session. Rats were administered an overdose of sodium pentobarbitone (>160 mg/kg i.p.) and transcardially perfused with 200 mL of 4% paraformaldehyde in 0.2 M phosphate buffer.
Brains were extracted, postfixed in 4% paraformaldehyde, and transferred to 30% sucrose in PBS 48 hours before cryosectioning into 40 μm coronal sections. Six sections were chosen per brain for immunohistochemical staining at Bregma: −2.80, −3.60, −4.30, −5.20, −5.60, and −6.04 mm (Paxinos et al. 2015). The brain sections were triple stained for EdU, neuronal nuclei (NeuN), and Hoechst to label dividing cells (EdU), neurons (NeuN), and all cell nuclei, thus allowing us to specifically identify the newly born cells during LI-TMS that had differentiated into neurons (Supplementary Data).
Statistical analyses
Statistical analyses were conducted using RStudio (v. 4.0.2), (RStudio Team, Boston, MA) and DABEST (via
Results
This pilot study compared the short-term efficacy of a standard once-daily protocol of TMS treatment delivery versus an accelerated three times daily timeline. In the standard LI-TMS treatment group, there were no significant differences (n = 5 per group, p > 0.05) between the active and sham groups for any of the behaviors in the FST and EPM test. In the accelerated LI-TMS group, animals receiving active stimulation had a significantly longer latency until the first immobility count (active: 130.00 ± 45.96 seconds, n = 5; sham: 54.00 ± 38.79 seconds, n = 5; p = 0.011), and a significantly higher total climbing count (active: 15.80 ± 4.92, n = 5; sham: 9.20 ± 5.45, n = 5; p = 0.035) compared with sham during the FST.
Additionally, the active group showed a trend toward less immobility (n = 5 per group, p = 0.076; Fig. 1). In the EPM, there were no significant differences between the active and sham groups; however, there was a trend for more grooming in the active group (n = 5 per group, p = 0.059; Supplementary Fig. S1). There were no difficulties with tolerability or safety among the standard and accelerated LI-TMS dosing protocols. Rats tolerated the stimulation (no behavioral responses during stimulation), and postmortem histological analysis showed no changes in neurogenesis, nor any evidence of DNA damage, neuronal loss or injury in the hippocampus and overlying cortex (Fig. 2).
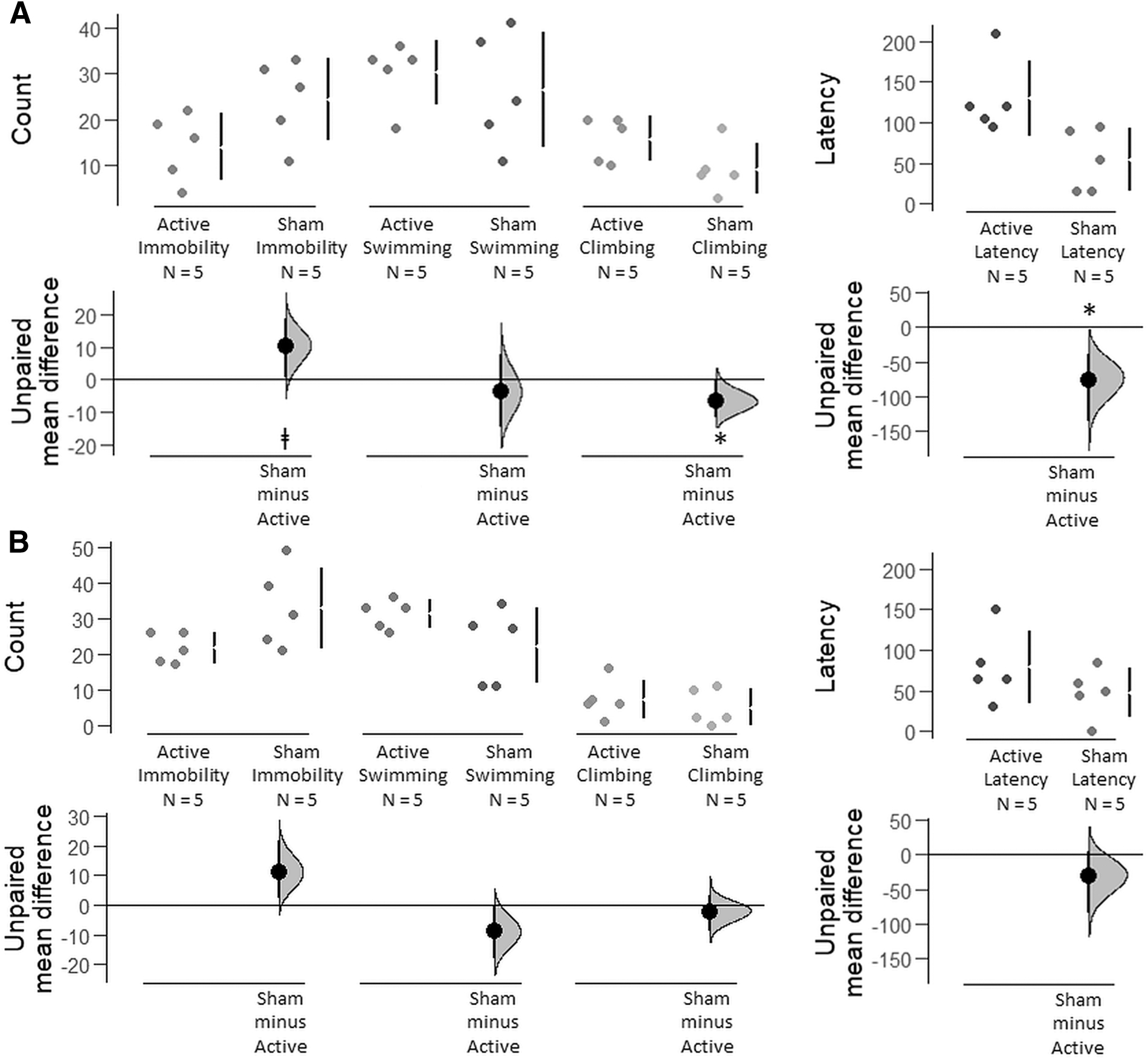
Comparisons of depression-related behaviors during forced swim test between the active and sham groups of the accelerated

EdU+/NeuN+ double-labeled cells in the dentate gyrus of the hippocampus.
Discussion
The findings from this pilot study demonstrated that accelerated LI-TMS was superior to daily LI-TMS and sham comparison groups in an adolescent rat CRS model of depression. Accelerated LI-TMS was tolerable and rescued anxiety and depression-like behaviors in adolescent rats. Interestingly, despite the positive behavioral effects, there was no effect on hippocampal neurogenesis. This result is consistent with previous work in adult mice suggesting that higher intensities (50 mT) are needed to drive neurogenesis. Our findings imply that LI-TMS may exert its antidepressant action via mechanisms that are distinct from those of serotonin reuptake inhibitors, which involve increased neurogenesis (Santarelli et al. 2003).
This study contributes to a growing body of literature that supports the utility of preclinical LI-TMS studies (Makowiecki et al. 2014; Grehl et al. 2015; Seewoo et al. 2019). Clinical studies suggest that accelerated TMS protocols have promise for treatment refractory mood disorders, but there are many unanswered questions with respect to dosing TMS (Lisanby 2017; Cole et al. 2020). Preclinical research is critical in advancing this area given the profound subject and financial burden of large clinical studies. These opportunities and challenges are accentuated in research focused on the application of TMS for adolescent MDD (Croarkin and Rotenberg 2016).
The application of TMS to address an aberrantly developing prefrontal cortex with imbalances in gamma-aminobutyric acid and glutamatergic neurotransmission has face validity and is appealing. However, prior clinical research that focused on the application of TMS for adolescent MDD has a number of limitations. These protocols most often adapt the standard, once-daily, left prefrontal, 10 Hz TMS that has been widely studied and applied to adults with treatment-resistant depression.
This approach forgoes numerous practical and neurophysiological considerations in the context of neurodevelopment (Oberman et al. 2021). For example, interventions with theta burst stimulation and accelerated protocols may confer more beneficial neuroplastic effects in the adolescent brain compared with standard protocols (Elmaghraby et al. 2021; Oberman et al. 2021). However, safety, neurophysiological, and clinical studies are lacking. Most adolescents would likely prefer briefer treatment protocols.
Strengths of this present work include a standardized approach to TMS delivery and a murine model of depression with prior validation (Seewoo et al. 2020). In addition, the lack of cell death in our histological analysis is a small but important step in addressing safety concerns. There are a number of methodological and engineering challenges related to animal models of TMS. Stimulation with LI-TMS has been previously validated and has utility for informing clinical research and practice (Grehl et al. 2016).
The limitations of this study are its small sample size and the use of only adolescent male rats, precluding the ability to study differential sex effects. The protocol also evaluated 10 Hz dosing as opposed to theta burst stimulation, which has increasingly been applied in human protocols of accelerated TMS (Cole et al. 2020; Baeken et al. 2021). The current protocol also had a briefer duration compared with standard clinical protocols. Despite these limitations, the present study demonstrated the utility of this adolescent murine model of TMS. Future efforts will inform the development of human adolescent TMS protocols.
Conclusions
Our findings demonstrate that accelerated LI-TMS may be more effective than the standard protocol in reducing depression-like behaviors in male adolescent animals and therefore provides preliminary evidence supporting the use of accelerated TMS protocols to treat depression in adolescent human patients.
Clinical Significance
Accelerated TMS protocols have the potential to provide similar or improved treatment outcomes compared with standard once-daily dosing. Accelerated TMS protocols also may have neuroplastic advantages in adolescents with MDD. Accelerated TMS protocols may provide pragmatic advantages for some patients. The present pilot study is the first to directly compare the two protocols in an adolescent animal model of depression.
Footnotes
Authors' Contributions
B.J.S. and J.R. designed the research. B.J.S., L.A.H., L.A.J., and L.A.M. conducted the experiments and acquired data. B.J.S. and L.A.H. analyzed the data. B.J.S., L.A.H., P.E.C., and J.R. wrote the article, and all authors contributed to the revisions and approved the final article for publication.
Acknowledgments
The authors thank Ms. Marissa Penrose-Menz, Ms. Kerry Leggett, Ms. Kaylene Schutz, Ms. Yashvi Bhatt, Mr. Parth Patel, Ms. Sandra Goodin, and Mr. Stefan Davis at M-Block Animal Care Services for their assistance with the behavioral experiments.
Disclosures
This research was funded by the University of Western Australia. B.J.S. is supported by a Forrest Research Foundation Scholarship, an International Postgraduate Research Scholarship, and a University Postgraduate Award. L.A.H. is supported by a University Postgraduate Award at the University of Western Australia, and the Commonwealth Government's Australian Government Research Training Program Fees Offset. P.E.C. has received research grant support from Mayo Foundation for Education and Research, Neuronetics, Inc.; NeoSync, Inc.; National Science Foundation, National Institute of Mental Health, and Pfizer, Inc. He has received grant-in-kind (equipment support for research studies) from Assurex; MagVenture, Inc.; and Neuronetics, Inc. He has served as a consultant for Engrail Therapeutics, Myriad Neuroscience, Procter and Gamble, and Sunovion. J.R. was supported by a Fellowship from Multiple Sclerosis Western Australia and the Perron Institute for Neurological and Translational Science and a grant from the Perpetual Foundation—The Helen Leech Endowment. All other authors have nothing to disclose.
Supplementary Material
Supplementary Data
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.