
Abstract
Objective:
Although it is known that attention-deficit/hyperactivity disorder (ADHD) increases the risk of bullying perpetration and victimization, the data on the effect of methylphenidate (MPH) treatment, which is frequently used in the treatment of ADHD, on bullying perpetration and victimization, are very limited. The aim of this study was to investigate the effect of MPH treatment on bullying perpetration and victimization in children and adolescents with ADHD.
Methods:
Children and adolescents with ADHD, aged 8–16 years, who had not been treated for ADHD for at least 1 year and prescribed only MPH treatment were invited to participate in this open-label naturalistic study. After 3 months of MPH treatment, peer bullying involvement status was analyzed in comparison with the pretreatment data.
Results:
There was a significant decrease in all subscales of the Conners' Parent Rating Scale (CPRS) and Conners' Teacher Rating Scale after MPH treatment. Being a bully decreased from 50% to 18% and being a victim decreased from 80% to 46%. It was determined that for every 1 point decrease in the CPRS Conduct Problems subscale, the risk of being a bully was reduced ∼2-fold, and every 1 point decrease in the CPRS Anxiety subscale reduced the risk of being a victim 2.44-fold.
Conclusions:
This is the first longitudinal study examining the effect of MPH treatment on bullying perpetration and victimization in children and adolescents with ADHD. It appears that MPH treatment may be effective in improving the situations of bullying perpetration and victimization in ADHD patients. In addition, the fact that the decrease in behavioral problems reduces the risk of being a bully and the decrease in anxiety symptoms reduces the risk of being a victim, suggests that prevention and intervention programs for bullying perpetration and victimization should target these problem areas.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders characterized by symptoms of inattention, hyperactivity, and impulsivity (American Psychiatric Association 2013), affecting 5.7% of children worldwide (Polanczyk et al. 2007) and 12.4% of children in Turkey (Ercan et al. 2019).
ADHD is associated with social problems such as poor school performance and academic success, and a deterioration in family and peer relationships (American Psychiatric Association 2013). Peer relationship difficulties such as the inability to establish mutual friendships, peer rejection, and bullying represent a crucial area of deterioration in ADHD (Gardner and Gerdes 2015). Bullying is a repetitive form of aggressive behavior that develops based on an imbalance of power with the intention of deliberately harming the other person, and several different forms of bullying have been identified, including physical, verbal, relational, and cyberbullying (Olweus 2013).
Recent studies have reported that ADHD increases the risk of bullying perpetration and victimization (Bacchini et al. 2008; Fite et al. 2014; Holmberg and Hjern 2008; Sciberras et al. 2012; Taylor et al. 2010; Unnever and Cornell 2003; Wiener and Mak 2009). In a cross-sectional population-based study in Sweden, it was reported that students with ADHD bullied others three times more (odds ratio [OR] = 3.8, 95% confidence interval [CI 2.0–7.2]) and were bullied 10 times more than students without ADHD (OR = 10.8, 95% CI [4.0–29.0]) (Holmberg and Hjern 2008). That study also found that students who were bullying perpetrators had higher parental reports of behavioral problems than students with ADHD who were not involved in bullying perpetration.
Behavioral problems have not been included in many studies examining the relationship between ADHD and peer bullying (Bacchini et al. 2008; Taylor et al. 2010; Unnever and Cornell 2003). Few studies examining the relationship between peer bullying and both ADHD and oppositional defiant disorder (ODD) symptoms have suggested that ODD symptoms more than ADHD symptoms predict participation in bullying (Fite et al. 2014; Sciberras et al. 2012; Wiener and Mak 2009).
Methylphenidate (MPH) (short or long-acting) is one of the first-line pharmacological therapies recommended for the treatment of ADHD and can be used from the age of 5 years (National Guideline 2018). Studies of young people with ADHD have shown that MPH has a large effect on aggression-related behaviors similar to the effect of MPH on the core symptoms of ADHD (Connor et al. 2002; Pringsheim et al. 2015). However, studies on the effect of MPH on bullying perpetration and victimization are very limited. To the best of our knowledge, there is no longitudinal study examining the effect of MPH treatment on peer bullying in children and adolescents with ADHD. In two cross-sectional studies in the literature, ADHD cases in two groups with and without MPH treatment were compared in terms of bullying perpetration and victimization (Hesapcıoglu and Kandemir 2020; Orengul and Sabuncuoglu 2018).
Hesapcıoglu and Kandemir (2020) found both bullying perpetration and victimization to be higher in terms of damage to property in cases who did not receive treatment. However, Orengul and Sabuncuoglu (2018) did not find a statistically significant difference between cases who received or did not receive treatment. Owing to the limited literature on this subject, the aim of this research was to investigate the effect of MPH treatment on bullying perpetration and victimization in ADHD cases with a follow-up study. The study hypothesis was that MPH treatment would reduce bullying perpetration and victimization in children and adolescents with ADHD, and that improvements in ADHD and disruptive behavior symptoms would be associated with an improvement in bullying perpetration and victimization.
Methods
Participants
The study sample consisted of children and adolescents with ADHD, aged 8–16 years, who presented at the Child and Adolescent Psychiatry Outpatient Clinic of Ondokuz Mayıs University Medical Faculty Hospital. Children and adolescents who were newly diagnosed with ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV-TR diagnostic criteria by their primary physician, or who had previously been diagnosed with ADHD but had not used medical treatment for ADHD for at least 1 year, and were prescribed only MPH at the first stage were invited to participate in the study.
Since this study was in a naturalistic design, the initial and maintenance dose of MPH and the type of preparation were determined by the primary physicians of the cases. MPH treatment is taken as either immediate-release tablets (taken two to three times a day) or modified-release tablets (taken once a day and the dose released throughout 8 or 12 hours).
In the second stage, the study sample was formed of 72 children and adolescents with no neurological disease, intellectual disability, psychotic disorder, bipolar disorder, or autism spectrum disorder, who had been involved in bullying perpetration or victimization at least twice a month according to the Olweus Peer Bullying Questionnaire. The Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL) was applied to the participants to support the diagnosis of ADHD and to detect comorbid psychiatric disorders.
In addition, before the MPH treatment, the parents of the cases were asked to complete the sociodemographic data form, the peer bullying parent reporting form, and the Conners' Parent Rating Scale (CPRS); and the teachers had to fill the Conners' Teacher Rating Scale (CTRS) and the peer bullying teacher reporting form. The cases were followed-up by their primary physicians during the 3-month treatment period.
They were referred to the researcher again after the polyclinic follow-up examination at the end of the third month. In the third stage of the study, participants were asked to complete the Olweus Peer Bullying in Students Questionnaire (OBVQ), the parents had to complete the peer bullying parent reporting form with CPRS, and the teachers to complete the peer bullying teacher reporting forms with CTRS. The study was completed with 50 participants who completed the forms and scales and continued the treatment during the 3-month follow-up period (Fig. 1).
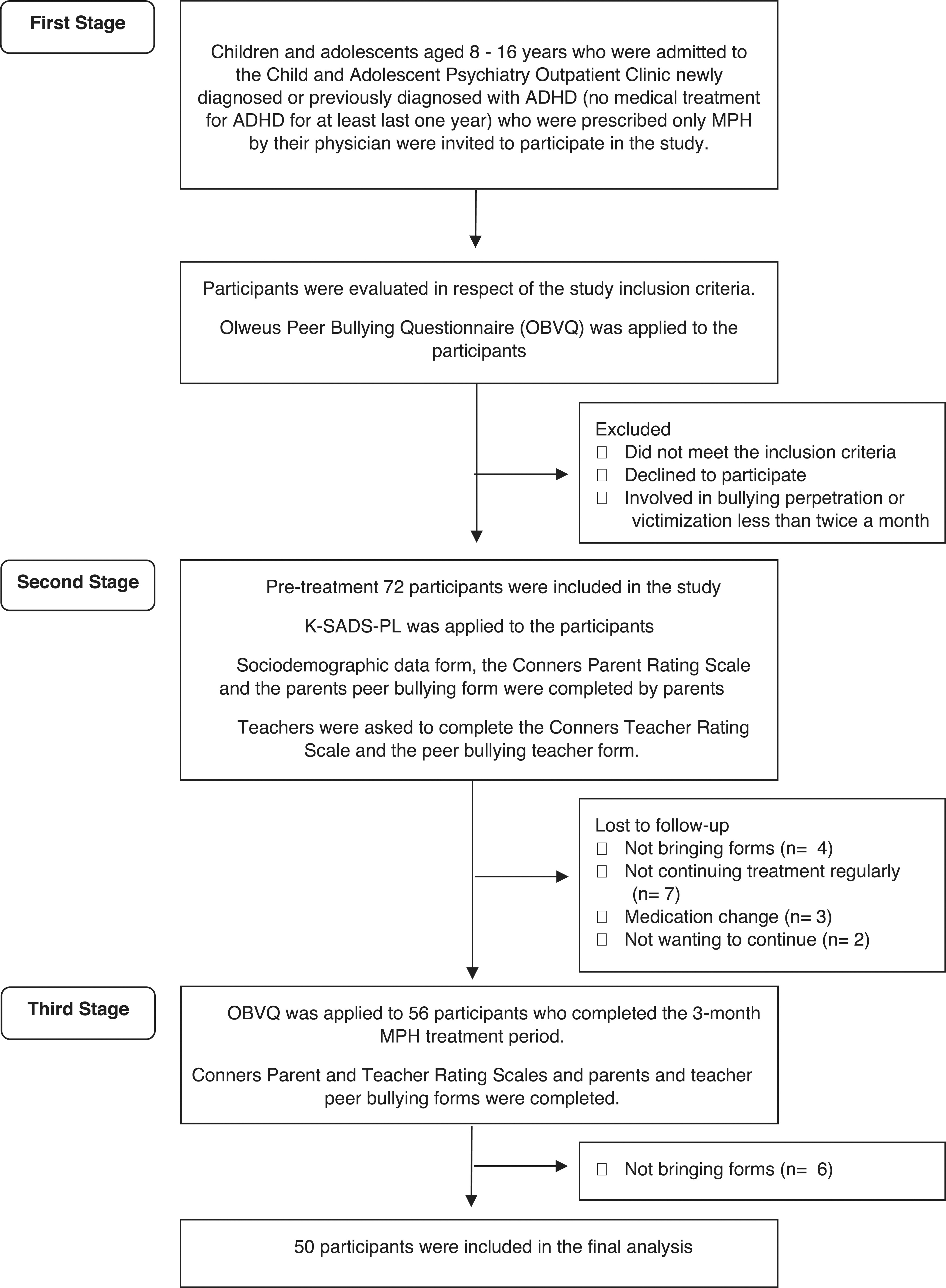
Flow chart of the study. ADHD, attention-deficit/hyperactivity disorder; MPH, methylphenidate; K-SADS-PL, Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version.
Participants who did not bring parent and teacher forms before and after the treatment, did not continue the treatment regularly, had a medication change, or did not want to continue were excluded from the study. The nonuse of drugs for more than four or more school days a month was accepted as no drug compliance. Of the participants who did not complete the study, 54.5% were newly diagnosed, and 45.5% had been previously diagnosed with ADHD.
Measures
Conners' Parent Rating Scale
The first 93-item version of the CPRS developed by Conners was shortened by Goyette et al. (1978) to a 48-item version of CPRS by eliminating some items and combining similar items according to previous factor analysis. This version consists of five subscales assessing (1) Conduct (behavioral) Problems, (2) Learning Problems, (3) Psychosomatic, (4) Impulsive/Hyperactive, and (5) Anxiety. Items in the CPRS are rated by parents on a 4-point Likert scale as 0 (not at all present), 1 (just a little present), 2 (pretty much present), and 3 (very much present), with a higher score indicating greater symptomatology (Goyette et al. 1978). The validity and reliability study of the CPRS was conducted in Turkey and the Cronbach's alpha coefficient was found to be 0.90 (Dereboy et al. 2007).
Conners' Teacher Rating Scale
The first 39-item version of the CTRS scale developed by Conners shortened by Goyette et al. (1978) and a new 28-item version was developed. This version consists of three subscales that evaluate (1) Conduct Problems, (2) Cognitive Problems/Inattention, and (3) Hyperactivity. The items in the scale are graded by the teachers on a 4-point Likert scale like CPRS (Goyette et al. 1978). The validity and reliability study of the CTRS was conducted in Turkey and the Cronbach's alpha coefficient was found to be 0.95 (Dereboy et al. 2007).
The Revised Olweus Bully/Victim Questionnaire
Olweus (1996) developed the scale for the assessment of peer bullying in 1983 and revised it in 1996. The OBVQ consists of 39 items with Likert-type responses to determine the type, frequency, nature of bullying perpetration and victimization, the child's help-seeking, and the reactions of third parties. The status of being a bully or victim is defined as two to three times a month accepted as the cutoff point to be a victim, bully, or bully/victim (Olweus 1996). The validity and reliability study of the OBVQ in Turkey was conducted and the Cronbach's alpha coefficient was found to be 0.81 (Sipahi and Karababa 2018).
Peer Bullying Parent and Teacher Form
From the perspective of parents and teachers, the involvement of children in bullying perpetration and victimization is evaluated with four items in this form. After a detailed definition of bullying perpetration and victimization, the four questions are presented about bullying victimization (“How often has your child or student been bullied in the last few months?”), the child's request for help from their parents or teacher (“Has your child/student asked you for help regarding bullying in the past few months?”), parents' and teacher's attitudes (“What did you do if asked?”), and bullying perpetration (“How often has your child/student bullied others in the past few months?”). Being bullied two or more times a month was accepted as being a victim and bullying others two or more times a month was accepted as being a bully.
Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version
The K-SADS-PL is a semi-structured interview scale to diagnose mental health disorders in children and adolescents aged 6–18 years, according to the diagnostic criteria in DSM III-R and IV (Kaufman et al. 1997). The validity and reliability study of the Turkish form was performed by Gökler et al. (2004).
Statistical analysis
Data obtained in the study were analyzed statistically using SPSS version 21 software. The chi-square test was used to analyze categorical variables with Bonferroni adjustment for multiple pairwise comparisons. Conformity of numerical data to normal distribution was analyzed with the Kolmogorov–Smirnov and Shapiro–Wilk normality tests. Normally distributed numerical data belonging to more than two groups were analyzed using analysis of variance (ANOVA), and non-normally distributed numerical data were analyzed with the Kruskal–Wallis test. Tamhane and Dunn tests were used for multiple comparisons between groups.
Changes in categorical data before and after treatment were analyzed with the McNemar test. The Wilcoxon signed-ranks test was used to compare CPRS and CTRS subscale scores before and after treatment. For the multivariate analysis, the CPRS and CTRS subscale values were entered into the logistic regression analysis to determine independent predictors of treatment outcome. In all analyses, the statistical significance level was set as p < 0.05.
Ethics
Ethical approval for this study (Ethical Committee OMU KAEK 2017/338) was provided by the Ondokuz Mayıs University Clinical Research Ethics Committee, Samsun, Turkey, on October 26, 2017.
Results
The evaluation was made of 50 children and adolescents with ADHD, comprising 34 (68%) boys and 16 (32%) girls with a mean age of 11.06 ± 2.36 years. The sociodemographic characteristics of the participants according to the peer bullying groups are given in Table 1. According to the pretreatment OBVQ, 10 (20%) of the cases were bullies, 25 (50%) were victims, and 15 (30%) were in the bully/victim group. The mean age of the bullying groups was compared with the ANOVA test, and a significant difference was found [F(2, 47) = 8.737, p = 0.001]. Post hoc comparisons using the Tamhane test were applied and a significant difference was determined between the victim and bully/victim groups, with a lower mean age of the victim group than the bully/victim group.
Sociodemographic Characteristics of the Participants in the Peer Bullying Groups
Chi-square test.
Significance values adjusted by Bonferroni correction. Significance values analyzed with the Tamhane test.
Analysis of variance.
Values are given as n (%) and mean ± standard deviation.
The participants' education levels were compared with the chi-square test among the groups, and a significant difference was found [χ 2(4, N = 50) = 13.79, p = 0.008]. Bonferroni adjustments were applied for post hoc comparisons. It was determined that more of the participants in the victim group were at the primary school level than in the bully/victim group.
ADHD subtypes and comorbid diagnoses in the peer bullying groups were compared with the chi-square test, and Bonferroni adjustments were applied for post hoc comparisons (Table 2). In children and adolescents with ADHD, the combined subtype was 74%, the inattention subtype was 20%, and the hyperactivity/impulsivity subtype was 6%. Hyperactivity/impulsivity subtype was higher in the bully group than in the victim and bully/victim groups [χ 2(4, N = 50) = 19.65, p = 0.001]. Comorbid psychiatric diagnoses were found in 82% of the participants. The most common comorbidity detected in the study group was anxiety disorders (AD), which was more common in the victim group than in the bully/victim group [χ 2(2, N = 50) = 6.54, p = 0.038].
Attention-Deficit/Hyperactivity Disorder Subtypes and Comorbid Disorders in Peer Bullying Groups
Chi-square test.
Significance values adjusted by Bonferroni correction.
ADHD, attention-deficit/hyperactivity disorder.
Reports of involvement in peer bullying before and after treatment were compared with the McNemar test. According to the OBVQ, being a bully (bullying perpetration two or more times in the last month) decreased from 50% to 18% (p < 0.001) and being a victim (bullying victimization two or more times in the last month) decreased from 80% to 46% (p = 0.031). Being a bully decreased from 30% to 12% according to the parent peer bullying form (p < 0.001) and from 50% to 26% according to the teacher form (p < 0.001). The cases were also compared as bully-only, victim-only, and bully/victim groups. After treatment, according to the OBVQ, the rate of bully only decreased from 20% to 4% (p = 0.008), bully/victim decreased from 30% to 14% (p = 0.039) and noninvolvement increased from 0% to 36% (p < 0.001).
According to the parental bullying form, the rate of bully only decreased from 20% to 4% (p < 0.001) and noninvolvement increased from 38% to 64% (p < 0.001). According to the teacher peer bullying form, the rate of bully only decreased from 30% to 6% (p < 0.001) and noninvolvement increased from 26% to 54% (p < 0.001) (Table 3). Considering the change in peer bullying involvement pre- and posttreatment, it was found that 27%–40% of the bullies, 40%–58% of the victims, and 27%–40% of the bullies/victims were not included in any peer bullying situations (Fig. 2).
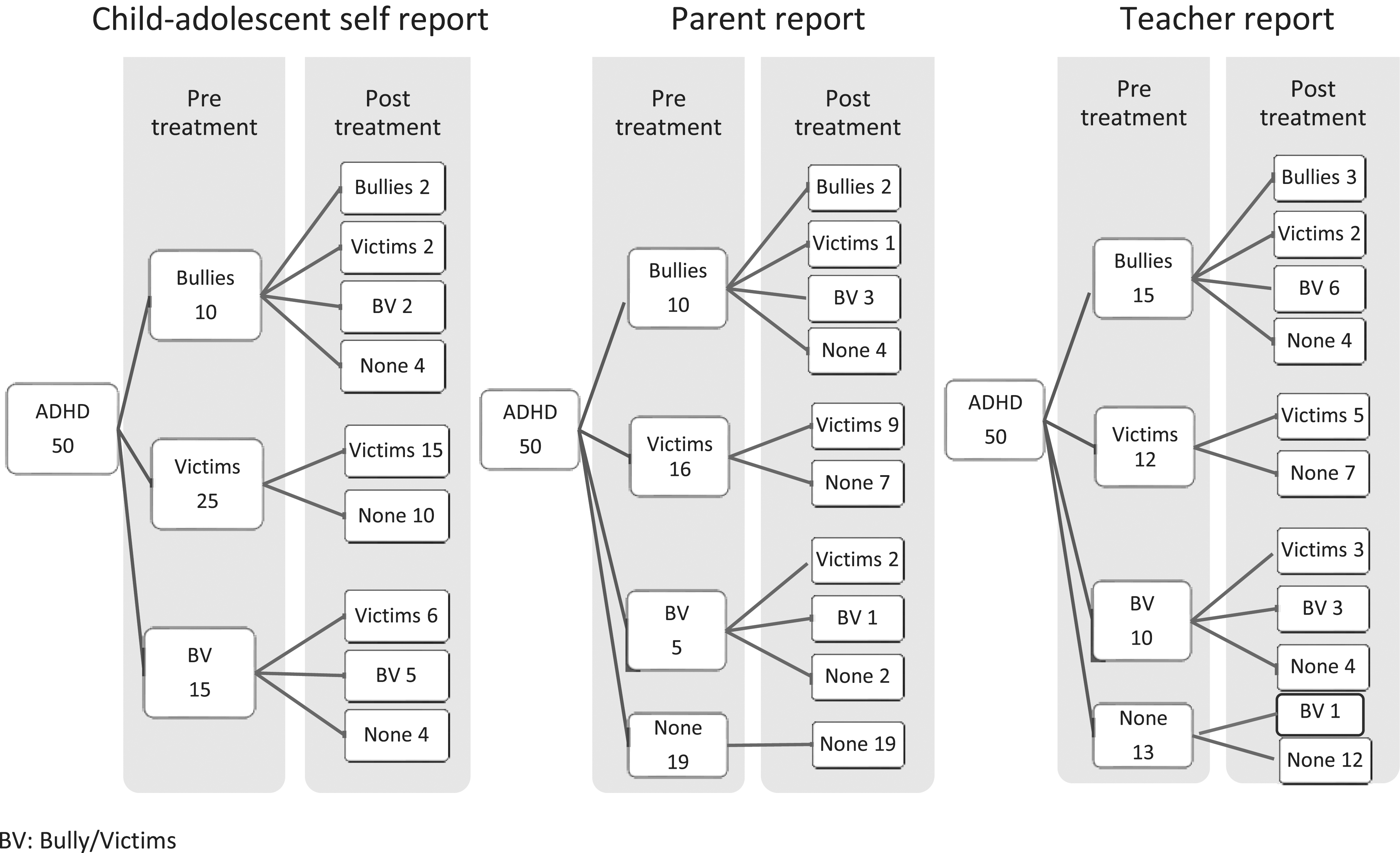
Change in reports of involvement in peer bullying pre- and posttreatment. ADHD, attention-deficit/hyperactivity disorder.
Pre- and Posttreatment Peer Bullying Involvement Reports
McNemar test.
The pretreatment CPRS and CTRS subscales were compared among the bullying groups using the Kruskal–Wallis test (Table 4). The results showed a statistically significant difference in CPRS Conduct Problems (CPRS-CP) [H(2) = 11.31, p = 0.004] and CPRS Impulsive/Hyperactive [H(2) = 8.31, p = 0.016] and CTRS Conduct Problems [H(2) = 7.66, p = 0.022] subscales between the peer bullying groups. Dunn's pairwise tests were applied to the three pairs of groups. The differences leading to significance in these three subscales were determined to be between the bully and victim groups.
Pretreatment Conners' Parent Rating Scale and Conners' Teacher Rating Scale Scores Among the Peer Bullying Groups
Kruskal–Wallis test.
Significance values adjusted by Bonferroni correction for multiple tests.
A, anxiety; CP, conduct problems; CPRS, Conners' Parent Rating Scale; CTRS, Conners' Teacher Rating Scale; H, hyperactivity; HI, hyperactive-impulsive; IQR, interquartile range; LP, learning problems; P, psychosomatic.
The mean dose of MPH given to the study group during the 3-month follow-up was 0.72 ± 0.21 mg/kg. The mean doses of MPH were 0.71 ± 0.23 mg/kg in bullies, 0.76 ± 0.22 mg/kg in victims, and 0.66 ± 0.18 mg/kg in bully/victim, with no difference determined between the groups [F(2, 47) = 1.287, p = 0.286]. The pre- and posttreatment subscale scores of CPRS and CTRS were compared with the Wilcoxon signed-rank test, and significant differences were found for all parameters (p < 0.001) (Supplementary Table S1). The subscale scores of the CPRS and CTRS were compared pre- and posttreatment among the peer bullying groups, and the significance remained in all parameters except the CPRS Psychosomatic subscale in the bullies group (Table 5). Ten (20%) children and adolescents scored 12 and above on the CTRS Hyperactivity or Inattention subscales after treatment, which can be interpreted as not showing sufficient improvement (Supplementary Figs. S1 and S2).
Pre- and Posttreatment Subscales of Conners' Parent Rating Scale and Conners' Teacher Rating Scale in Peer Bullying Groups
Wilcoxon signed-rank test.
A, anxiety; CP, conduct problems; CPRS, Conners' Parent Rating Scale; CTRS, Conners' Teacher Rating Scale; H, hyperactivity; HI, hyperactive-impulsive; IQR, interquartile range; LP, learning problems; O, oppositional; P, psychosomatic.
Logistic regression analysis was performed to determine the effects of change in the CPRS and CTRS subscales after MPH treatment in reducing bullying perpetration (Table 6). In the model, those being a bully before treatment and not being a bully after treatment were taken as reference. No significant predictor was found when all the subscales were included in the model with the enter method. The model was statistically significant when these variables were analyzed with the forward Wald method [χ 2(1) = 8.564, p = 0.003]. It explained 39.8% (Nagelkerke R 2) of the variance decreasing bullying perpetration and correctly classified 80.0% of cases. In this model, it was found that each decrease of 1 point in the CPRS-CP subscale after MPH treatment reduced the risk of being a bully approximately twofold (OR = 0.488, 95% CI [0.26–0.914], p = 0.025).
Logistic Regression Analysis of the Relationship Between Changes in the Conners' Parent Rating Scale and Conners' Teacher Rating Scale Subscales and Being a Bully and Being a Victim Posttreatment
Accuracy = 84.0%; Nagelkerke R 2 = 63.6%.
Accuracy = 80.0%; Nagelkerke R 2 = 39.8%, reference: not being a bully.
Accuracy = 75.0%; Nagelkerke R 2 = 39.6%.
Accuracy = 72.5%; Nagelkerke R 2 = 21.7%, reference: not being a victim.
95% CI, 95% confidence interval; A, anxiety; CI, cognitive problems/inattention; CP, conduct problems; CPRS, Conners' Parent Rating Scale; CTRS, Conners' Teacher Rating Scale; H, hyperactivity; HI, hyperactive–impulsive; LP, learning problems; OR, odds ratio; P, psychosomatic.
Logistic regression analysis was performed to determine the effect of the change in the Conners' subscales on reducing bullying victimization. In the model, those who were victims before treatment and were not victims after treatment were taken as reference. When all subscales were included in the model with the enter method, the model was statistically significant [χ 2(1) = 5.478, p = 0.019] and explained 39.6% (Nagelkerke R 2) of the variance in decreasing bullying perpetration and correctly classified 75.0% of cases.
The model was statistically significant when these variables were analyzed with the forward Wald method [χ 2(1) = 6.847, p = 0.003]. It explained 21.7% (Nagelkerke R 2) of the variance decreasing bullying perpetration and correctly classified 72.5% of cases. It was found that each decrease of 1 point in the CPRS Anxiety (CPRS-A) subscale after MPH treatment reduced the risk of being a victim 2.44-fold (OR = 0.409, 95% CI [0.194–0.866], p = 0.019) in the model with the enter method.
Discussion
In this study, the effect of the stimulant MPH used in the treatment of ADHD on bullying perpetration and victimization in children and adolescents with ADHD was investigated. There are very few studies on the effect of MPH treatment on peer bullying, and those have been cross-sectional studies. To the best of our knowledge, this is the first longitudinal study to have examined the effect of MPH treatment on peer bullying. Hesapcıoglu and Kandemir (2020) compared being involved in traditional and cyberbullying in male subjects who had not received MPH treatment for ADHD in the last year. The results of that study showed that bullying in the form of damaging the property of others and being victimized in the form of physical and damage to the property by others were more common in the group who did not receive drug treatment (Hesapcıoglu and Kandemir 2020).
However, that study did not include data on the change in ADHD symptoms with MPH treatment. In another study conducted with a smaller sample, no significant difference was found between the groups treated and not treated with MPH with respect to both peer bullying rates and CPRS and CTRS scores (Orengul and Sabuncuoglu 2018). The researchers attributed the results of that study to the explanation that the treated group may have consisted of more severe ADHD cases or that adequate symptom control could not be achieved with drug therapy.
In this study, a significant decrease was observed in all subscale scores of CPRS and CTRS after 3 months of MPH treatment. According to the OBVQ, being a bully decreased from 50% to 18% and being a victim decreased from 80% to 46%. Being a bully decreased from 30% to 12% according to the parent peer bullying form and from 50% to 26% according to the teacher report form. In addition, the cases were compared as bully-only, victim-only, and bully/victim groups. According to the OBVQ, the rate of bully only decreased from 20% to 4%, bullies/victims decreased from 30% to 14% and noninvolvement increased from 0% to 36%. According to the parental bullying form, the bully-only rate decreased from 20% to 4% and noninvolvement increased from 38% to 64%.
According to the teacher peer bullying form, the bully-only rate decreased from 30% to 6% and noninvolvement increased from 26% to 54%. Although there was a decrease in bullying after treatment according to the OBVQ, there was no significant decrease in the victims group. It was thought that the decrease in victims was masked owing to the transition from cases in other groups to the victims group after treatment. The fact that 20% of the bullies and 40% of the bully/victim became victims only after 3 months of treatment is remarkable, showing that although these cases are no longer bullying, they may be bullied by others. In the same context, Hoza et al. also suggest that negative peer regard is not easily reversed, even with intensive evidence-based treatments that reduce the symptoms of ADHD (Hoza et al. 2005).
The improvement in conduct problems after MPH treatment was found to be associated with a decrease in bullying, and a 1 point decrease in CPRS-CP (behavioral problems) reduced the risk of being a bully approximately twofold. Many studies examining the relationship between ADHD and peer bullying have not included behavioral problems (Bacchini et al. 2008; Taylor et al. 2010; Unnever and Cornell 2003). The few studies examining the relationship between bullying perpetration and victimization and both ADHD and ODD symptoms have suggested that ODD symptoms more than ADHD symptoms predict participation in bullying (Fite et al. 2014; Sciberras et al. 2012; Wiener and Mak 2009).
These findings support the fact that the decrease in behavioral problems predicts the decrease in bullying, although there was also a decrease in ADHD symptoms in this study. In addition, interventions for comorbid externalizing diagnoses and ODD symptoms are recommended for peer relationship and bullying problems in children with ADHD (Fite et al. 2014; Velő et al. 2021). Previous meta-analyses have shown that MPH treatment has a large effect on aggression-related behaviors, including oppositional behavior and behavioral problems (effect size = 0.80), similar to its effect on the core symptoms of ADHD (Connor et al. 2002; Pringsheim et al. 2015).
The improvement in anxiety symptoms after MPH treatment was also found to be associated with a decrease in victimization, and each decrease of 1 point in the CPRS-A subscale reduced the risk of victimization 2.44-fold. It has been reported in previous studies that internalizing problems are more common in the victims of bullying and the existence of a bi-directional relationship between peer victimization and internalizing problems, in which internalizing problems both increase the risk of victimization and may arise as a result of peer victimization (Becker et al. 2017; Monopoli et al. 2019; Reijntjes et al. 2010; Siebecker et al. 2010). Monopoli et al. (2019) examined the risk factors for the victimization of students with ADHD and found that anxiety symptoms and relational aggression were the strongest risk factors for bullying victimization.
Becker et al. (2017) found that both physical and relational victimization predicted higher anxiety symptoms in a study examining the relationship between victimization and internalizing symptoms in students with ADHD. Consistent with these studies, higher rates of AD were determined in victims in this study. In previous studies, MPH has been shown to reduce general anxiety symptoms (Abikoff et al. 2005) and social anxiety symptoms in children and adolescents with ADHD (Golubchik et al. 2014). That a reduction in anxiety symptoms predicts not continuing to be a victim may be related to the fact that with lower anxiety levels after MPH treatment, victims were able to better defend themselves, or that they were no longer seen as weak by the bullies and were therefore not chosen as victims.
This study had some limitations, primarily the open-label naturalistic design and that there were cases who did not complete the study for reasons such as not returning the pre- and posttreatment forms or dropping out of follow-up. This limitation may have resulted in the bias in the sample, owing to the inclusion of predominantly stimulant responders who were most likely to remain in treatment for 3 months and complete all the forms. However, posttreatment ADHD severity of 12 points or more on the CTRS Hyperactivity or Inattention subscales in 20% of the participants may have slightly reduced the likelihood of bias. In addition, the inclusion of participants with treatment compliance problems and those who had previously discontinued medical treatment may have led to an increase in the number of those who did not complete the study.
Another limitation was that the 3-month follow-up period determined to evaluate the effect of MPH treatment on peer bullying behaviors may have been insufficient, considering that no significant reduction in victims was detected. Other limitations of this study were the lack of any evaluation for the diagnosis of learning disability, which is one of the common comorbidities in ADHD, that the study was conducted on a clinical sample, and the relatively low sample size. There is a need for further longitudinal, large-scale, longer follow-up studies to confirm these findings and evaluate the long-term effects of MPH on bullying perpetration and victimization. Studies are also needed to examine the effects of MPH treatment on different forms of peer bullying such as physical, relational, and cyberbullying.
Conclusions
The results demonstrated that MPH treatment may have an effect on bullying perpetration and victimization in MPH-responsive ADHD patients. Although there was a significant decrease in being a bully and being a victim after 3 months of MPH treatment, longer MPH therapy or other intervention methods might be needed in cases where improvement could not be achieved. In addition, the fact that the decrease in behavioral problems reduced the risk of being a bully and the decrease in anxiety symptoms reduced the risk of being a victim, suggests that prevention and intervention programs for bullying perpetration and victimization should target these problem areas.
Clinical Significance
There are very limited studies on the effect of MPH treatment on peer bullying. To our knowledge, this is the first longitudinal study to have examined the effect of MPH treatment on bullying perpetration and victimization in children and adolescents with ADHD. This study reveals that MPH may be an effective treatment method in children and adolescents with ADHD for bullying perpetrations and victimization. It is noteworthy that the effect of the decrease in behavioral problems on being a bully and the effect of the decrease in anxiety symptoms on being a victim.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.