
Abstract
Objectives:
While long-lasting antipsychotics (LLA) were specifically developed to address the problem of adherence in patients with chronic psychiatric disorders, their role in pediatric populations is not clear.
Methods:
To document the efficacy, tolerance, and acceptance of LLAs in children and adolescents, a literature search was conducted using several databases for published studies (PubMed, PsycINFO) from January 1965 to December 2020. Twenty-two studies were identified (16 case reports/series, 3 open label studies, 2 controlled studies, and 1 retrospective analysis of national database).
Results:
Demographic features were widely heterogeneous across studies (total N = 480, 58% male, mean age = 15.0 ± 1.8). Case reports/series presented positive therapeutic outcomes in noncompliant youths with severe mental illness. Three open-label one-arm studies supported the clinical efficacy of risperidone long-acting injection in patients previously stabilized with oral risperidone. One study showed lower clinical symptoms and higher functioning at 12 months in youths treated for an acute psychotic episode with paliperidone palmitate compared to oral risperidone. The types and rates of side effects of LLA were comparable to those observed for oral antipsychotics. Two studies suggested better metabolic and neurological tolerance of LLA compared to an oral form. Preliminary evidence supported a satisfactory level of treatment satisfaction in patients treated with LLA and their families, while concerns were raised regarding practical administration in outpatient services. However, the average quality of the evidence based on the RoB2 tool was low.
Conclusions:
The level of evidence was low for the efficacy of LLA in pediatric populations and very low for the tolerance and acceptance. It concerned mostly the effect of risperidone long-acting injection in adolescents with psychotic disorders. Randomized maintenance clinical trials using noninferiority analysis would be more appropriate for further research.
Introduction
Antipsychotics is one of the most widely prescribed classes of psychotropics in children and adolescents (Rani et al. 2008; Olfson et al. 2010). Indications for antipsychotics at these ages encompass several disorders such as early-onset schizophrenia (EOS), bipolar disorder (BD), chronic tics, and aggressive behaviors in youths with neurodevelopmental disorders (Findling et al. 2011; Dinnissen et al. 2020).
Nonadherence among youths treated with an antipsychotic is particularly common, both in patients treated for BD (Coletti et al. 2005; Patel et al. 2005; Drotar et al. 2007; Bhowmik et al. 2013; Goldstein et al. 2016) and psychotic disorders (Cornblatt et al. 2007; Gearing and Charach 2009; Gearing et al. 2018). One study estimates a mean percentage of treatment time in full adherence to be around 56% over 1 year in bipolar adolescents in maintenance therapy (Patel et al. 2005). Using an electronic weekly pillbox, Goldstein et al. (2016) showed that 42% of doses were not taken as prescribed over 3 months in adolescents with BD.
A low rate of medication adherence in children and adolescents treated for severe mood or psychotic disorders is generally associated with a lower rate of symptom remission, increased functional impairment, poorer quality of life, and a higher rate of hospital readmission (Fontanella 2008; Taddeo et al. 2008; Edgcomb and Zima 2018). Nonadherence was associated with higher incidence of relapse (Robinson et al. 1999) and incomplete remission (Andreasen et al. 2005) in adolescents treated with antipsychotics for a first acute psychotic episode.
The first antipsychotics formulated as a long-acting injectable form were developed in the mid-60s. Since then, several new long-lasting antipsychotics (LLA) have been developed in adults (Table 1). Because LLA reduce the burden of a daily oral intake for the patient, it reduces the likelihood of omissions and treatment gaps. Adults with schizophrenia treated with LLA have reduced relapse rates and rehospitalizations compared to patients with oral antipsychotics both in randomized controlled trials (RCT) (Bai et al. 2007; Olivares et al. 2011) and in naturalist cohort studies (Tiihonen et al. 2011; Grimaldi-Bensouda et al. 2012).
Currently Available Long-Lasting Medication, Adapted from Crocq (2015)
No need for oral overlap if loading dose is used. If no loading dose given, supplement with oral antipsychotic for up to 3 months.
Risk Evaluation and Mitigation Strategy requires the patient to remain in the health care setting for 3 hours after administration because of the risk of olanzapine overdose (specifically sedation and/or delirium).
IM, intramuscular.
To date, national agencies for health product safety have not approved the use of LLA in pediatric populations. However, the American Academy of Child and Adolescent Psychiatry recommended in 2013 the off-label use of LLA in adolescents with schizophrenia and history of poor medication adherence (McClellan et al. 2013). In the same time, cumulative evidences have shown that poor treatment adherence at an early phase of chronic psychiatric disorders is essential to prevent a faster transition to a more advanced phase (Fusar-Poli et al. 2014; Benarous et al. 2016).
The possible use of LLA as a maintenance therapy after a manic or psychotic episode is mentioned in international guidelines for the clinical management of adults with BD (Malhi et al. 2015) and psychotic disorders (American Psychiatric Association 2020). While these recommendations concern patients aged 15–18 years, so far, no guideline regarding the use of LLA in a pediatric population has been established.
In 2017, Lytle et al. (2017) published in this journal a nonsystematic review of literature of LLA in children and adolescents. Only seven published reports were reported. The authors noted the paucity of well-designed and well-conducted studies to provide evidence for the efficacy and tolerability of LLA in children and adolescents. In addition, the majority of the publications were within the last 5 years, reflecting the increasing availability of LLA in clinical settings. The development of new molecules over the last 5 years and the need to review data with a systematic approach prompted us to proceed to an updated review of literature.
Methods
Search strategy
The systematic review was conducted following the recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline (Fig. 1) (Moher et al. 2009). Titles and abstracts were scanned for relevance. Full texts were ordered in case of uncertainty so as to maximize sensitivity. Reference lists of retrieved systematic reviews were checked. All full texts were checked for eligibility. Any original study (open trial, double-blind trial whether randomized control or not), case-report, case-series, meta-analysis, and systematic review was eligible for inclusion in this review. Abstracts and editorials were excluded.
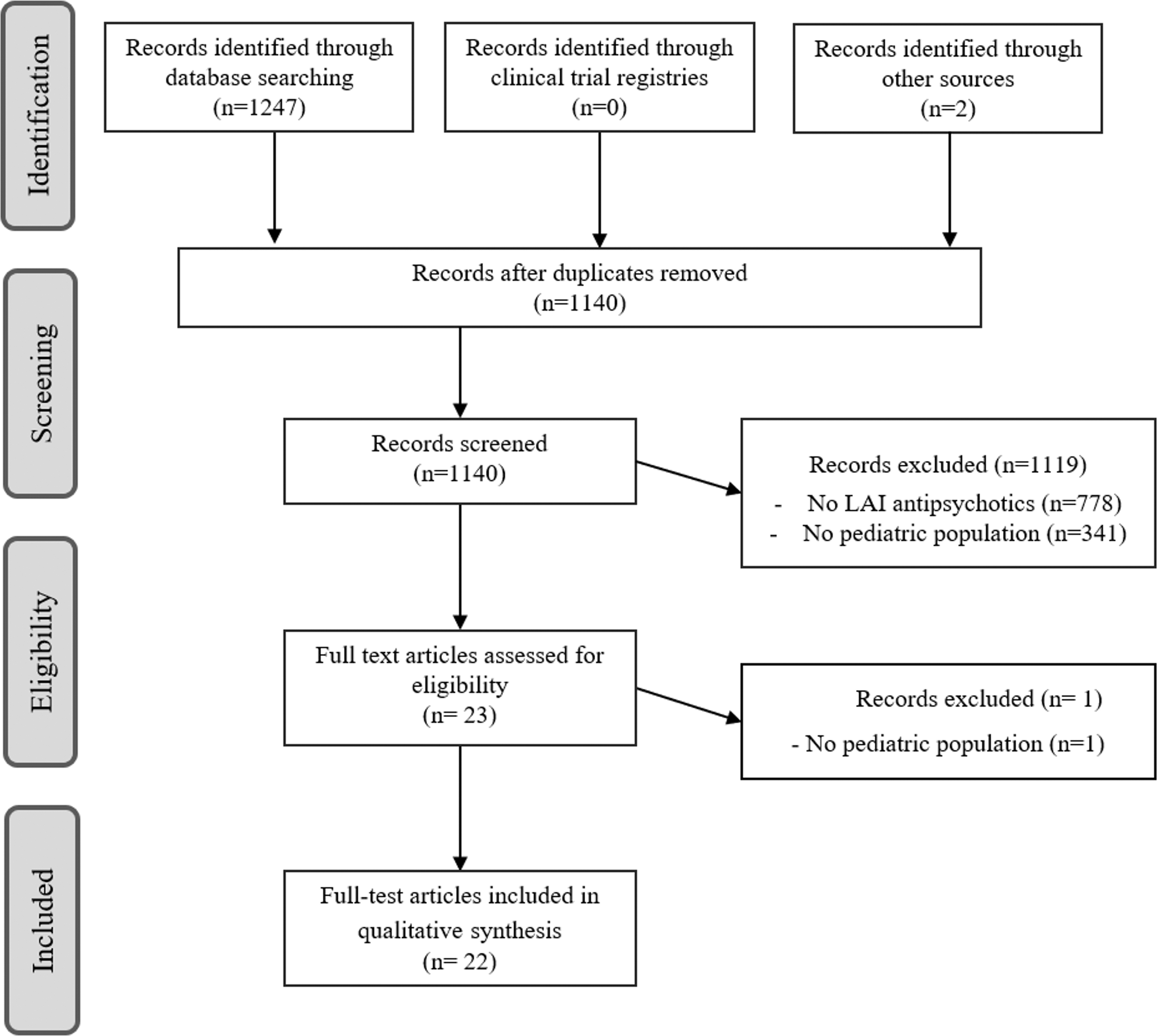
PRISMA flow diagram for the systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Relevant articles for this study were obtained through Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, PsychINFO, PsychINDEXplus, and Dissertation Abstracts. Each database was searched from January 1965 to December 2020. In addition, we hand-searched reference lists of identified articles and pertinent reviews for additional studies. Furthermore, the clinical trial registry of the U.S. National Institutes of Health (
Study eligibility
All original studies were eligible if they examined the effects of LLA in children and adolescents. Study participants had to receive LLA and to be younger than 18 years of age, or the mean age of the participants had to fall within the aforementioned age range.
Study selection
A first researcher screened for the potential studies. The full articles of selected studies were independently reviewed by a second reviewer. Discrepancies were resolved through discussion with a third reviewer. The references of each full article were extracted to search for additional references. In a second time clinical trial, registries were examined.
Data extraction
The following data from all included studies were entered in Excel following the strategy used by Lytle et al. (2017): (i) description of the medication (name, duration, and dose received), (ii) participants' features (gender, mean age, main psychiatric diagnoses, treatment setting), (iii) efficacy outcomes (clinical and functioning scales), (iv) tolerance outcomes (rates and types of side effects), and (v) acceptance outcomes (drop-out rate, main reasons mentioned, and scores).
Risk of bias assessment
The two first authors independently assessed the quality of the clinical trials and resolved differences through discussion with a third reviewer with specific expertise in clinical methodology. RCT were assessed using the revised Cochrane collaborations tool (RoB2) and non-RCT with the Cochrane tool for non-RCT (ROBINS-1) (Higgins et al. 2011; Sterne et al. 2016). Results of risk of bias assessments were visualized using the Cochrane risk-of-bias visualization tool (Higgins et al. 2011) and presented as Supplementary Table S1.
Results
Studies included
The systematic review yielded 1140 hits after having removed duplicates. Based on the information in the title or the abstract, 23 studies were retained. The critical reviews of these 23 articles led to the exclusion of one article because outcomes in youths and adults were pooled. No ongoing trials conducted in children or adolescent were found in clinical trial registries. A list of 22 studies was generated.
Study design
Sixteen case reports/series (Erermis et al. 2007; Fu et al. 2009; Kowalski et al. 2011; Tutkunkardaş and Abali 2011; Wisniewski 2011; Patel et al. 2013; Umehara et al. 2014; Fàbrega et al. 2015; Demirkaya and Zoroğlu 2016; Pope and Zaraa 2016; Demirkaya et al. 2017; Fortea et al. 2018; Mirza et al. 2018; Akram and Mitchell 2019; McInnis and Kasinathan 2019; Jacob et al. 2021), three open-label one-arm studies (Ruan et al. 2010; Boarati et al. 2013; Ceylan et al. 2017), one retrospective analysis of national database (Modesitt et al. 2018), and two controlled studies (Suzuki et al. 2017; Petrić et al. 2019).
Medication
All 22 studies except 5 concerned second-generation antipsychotics (Erermis et al. 2007; Fàbrega et al. 2015; Mirza et al. 2018; McInnis and Kasinathan 2019; Jacob et al. 2021) (Table 1).
Psychiatric diagnoses
The most frequent psychiatric disorders targeted by LLA were EOS or other psychotic disorders (n = 152, k = 11), followed by conduct disorder (CD) (n = 60, k = 7) and BD (n = 54, k = 8), and then intellectual disability and/or autistic spectrum disorder (n = 41, k = 6) (Fig. 2). One case report reported the use of LLA in a child with prepubertal anorexia (Umehara et al. 2014). The vast majority of studies (k = 21) were conducted in nonclinically stable patients. Participants were recruited among outpatients (k = 9) and inpatients (k = 13).
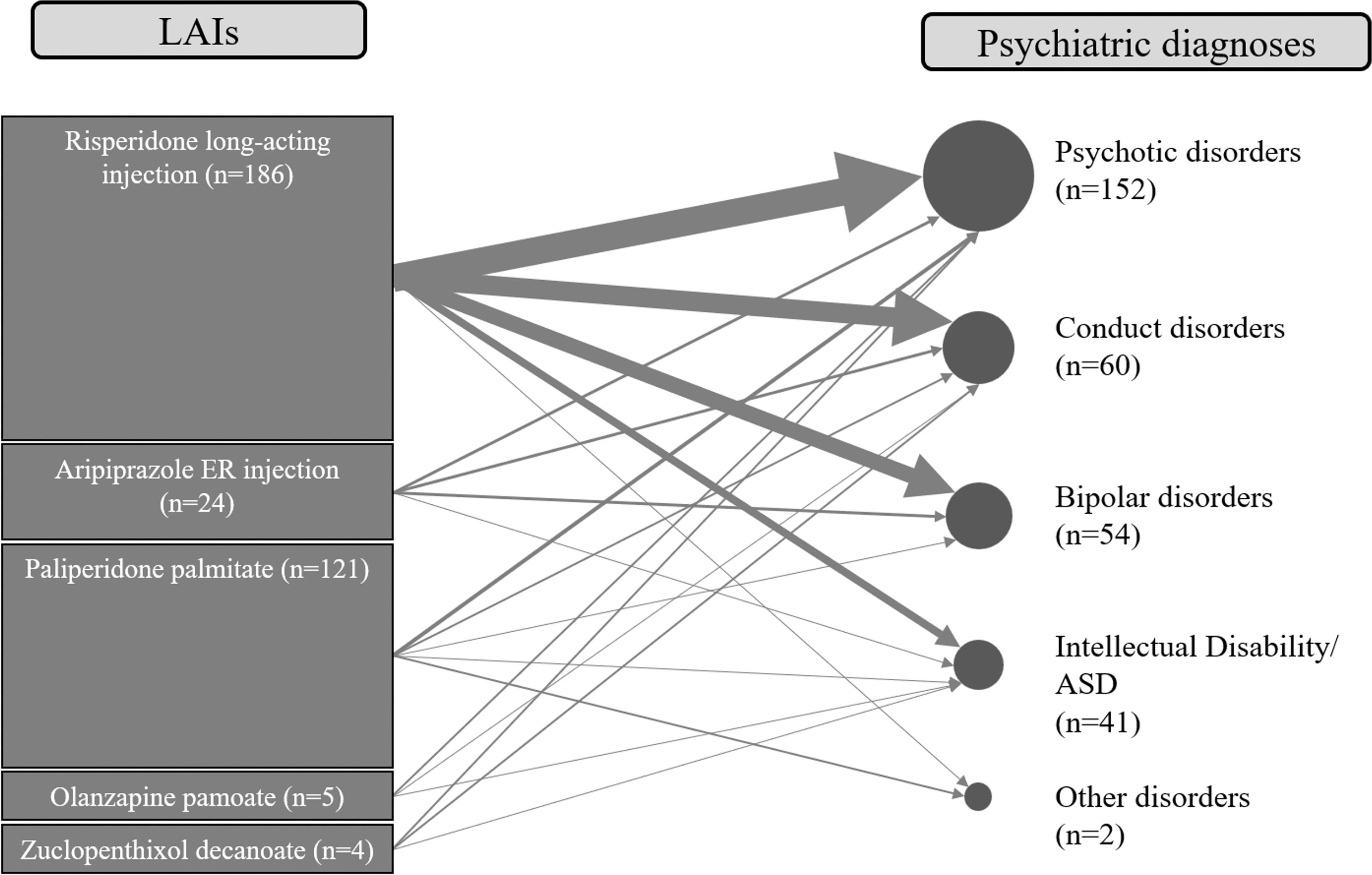
Correspondence between the LLAs prescribed and associated psychiatric disorders for the participants of reviewed studies. LLA, long-lasting antipsychotics.
Demographic features
The mean age of the total sample studied was 15.0 ± 1.8 with 58% being male. Ethical characteristics were not systematically reported but participants were recruited from varied geographical backgrounds, that is, European countries and United Kingdom (k = 6), North America (k = 4), South America (k = 2), Asian countries (k = 3), Middle-East countries (k = 5), and Australia (k = 1).
Risk of bias assessment
A standardized assessment of therapeutic outcomes was only available for 12 of the 22 reviewed studies, with 11 of them having a single-arm study design (Fu et al. 2009; Ruan et al. 2010; Kowalski et al. 2011; Boarati et al. 2013; Fàbrega et al. 2015; Demirkaya and Zoroğlu 2016; Pope and Zaraa 2016; Ceylan et al. 2017; Demirkaya et al. 2017; McInnis and Kasinathan 2019; Jacob et al. 2021).
The two controlled studies (Suzuki et al. 2017; Petrić et al. 2019) were rated as having moderate risk of bias. Suzuki et al. (2017) compared time until discontinuation of treatment due to all causes for 12 youths with EOS compared to 20 adults with schizophrenia. Possible biases due to missing data and selection of the reported result may be suspected considering the lack of information about the method of selection of the control group. Petrić et al. (2019) compared the efficacy of oral risperidone versus paliperidone palmitate in adolescents with a first acute psychotic episode. The study suffered from high risk of bias as no information was provided on the concomitant treatment authorized in both groups. It was not possible to calculate pooled effect size of the study outcomes due to the diversity of measurement practices, study heterogeneity and low quality.
Efficacy of LLA
Case reports/series
Sixteen case reports/series reported treatment with LLA in children and adolescents (Table 2). In two case reports, the LLA was discontinued at a very early point due to severe side effects (Erermis et al. 2007; Patel et al. 2013). Risperidone long-acting injection was associated with a substantial clinical improvement in patients with various psychiatric disorders in six case reports (Fu et al. 2009; Tutkunkardaş and Abali 2011; Umehara et al. 2014; Demirkaya and Zoroğlu 2016; Pope and Zaraa 2016). Other case reports illustrated the efficacy of other LLAs. One case series (N = 30) showed substantial functional improvement in adolescent inpatients with various psychiatric disorders treated with different LLAs (aripiprazole, risperidone long-acting injection, paliperidone palmitate) (Fortea et al. 2018).
Case Reports and Case Series Studies on Long-Lasting Antipsychotics in Children and Adolescents
ABC, Aberrant Behavior Checklist; ADHD, attention-deficit/hyperactivity disorder; ASD, autistic spectrum disorder; BD, bipolar disorder; BL, baseline; BPRS, Brief Psychiatric Rating Scale; CD, conduct disorder; CGI-I, Clinical Global Impression Improvement scale; CGI-S, Clinical Global Impression Severity scale; FU, follow-up; ID, intellectual disability; NR, not reported; ns, no standardized assessment; PANSS, Positive and Negative Syndrome Scale; PTSD, posttraumatic stress disorder; SCZ, schizophrenia; SUD, substance use disorder; UKU, UKU side effects rating scale.
Open-label one-arm studies
Ruan et al. (2010) switched antipsychotic treatment of 31 clinically stable adolescents with EOS from oral forms (olanzapine or risperidone) to risperidone long-acting injection. After 24 weeks, authors reported a statistically significant change in the Positive and Negative Syndrome Scale (PANSS) score (primary outcome). Authors found a slight but significant reduction of the Clinical Global Impression Severity scale (CGI-S) score from baseline to endpoint. Boarati et al. (2013) examined the clinical efficacy of risperidone long-acting injection in 19 adolescent outpatients with severe form of BD previously treated with risperidone with good tolerability.
After 24 months, the authors noted a significant decrease in the CGI-S score and increase in CGAS score. Ceylan et al. (2017) examined the clinical efficacy of risperidone long-acting injection in 42 adolescent inpatients with various psychiatric disorders who received at least four intramuscular injections. At 2 months, 81% of patients were considered to be much improved or very much improved based on Clinical Global Impression Improvement scale (CGI-I) score.
Controlled studies
Suzuki et al. (2017) showed that the drop-out rate at 1 year among 12 adolescents with EOS treated with risperidone long-acting injection was only half the rate observed in their counterpart adults (respectively, 30% vs. 60%, while the difference was not statistically significant). In the case-control study, conducted by Petrić et al. (2019), 18 adolescents treated for a first acute psychotic episode with an oral antipsychotic were compared to 18 adolescents treated with injections of paliperidone palmitate. The authors noted that the changes in CGI-S, PANSS, and Personal and Social Performance Scale scores were stronger in those treated with paliperidone palmitate compared to those with oral risperidone at 12 months. A lower readmission rate at 12 months was noted in patients treated with paliperidone palmitate compared to those with oral risperidone (respectively, 11% vs. 50%).
Tolerance
Only three studies used standardized reports of side effects (Ruan et al. 2010; Boarati et al. 2013; Ceylan et al. 2017) (Tables 2 –4).
Open-Label One-Arm Study and Retrospective Database Analysis on Long-Lasting Antipsychotics in Children and Adolescents
ADHD, attention-deficit/hyperactivity disorder; BD, bipolar disorder; BL, baseline; CD, conduct disorder; CGI, Clinical Global Impression scale; CGI-S, Clinical Global Impression Severity scale; ESRS, extrapyramidal symptom rating scale; FU, follow-up; ID, intellectual disability; IM, intramusuclar; NR, not reported; ns, no standardized assessment; PANSS, Positive and Negative Syndrome Scale; SATEES, Systematic Assessment for Treatment Emergent Effects Scale; SCZ, schizophrenia; VAS, visual analogue scale.
Controlled Studies on Long-Lasting Antipsychotics in Children and Adolescents
BL, baseline; CGI, Clinical Global Impression scale; CGI-S, Clinical Global Impression Severity scale; FU, follow-up; LUNSERS, Liverpool University Neuroleptic Side Effect Rating Scale; NR, not reported; ns, no standardized assessment; PANSS, Positive and Negative Syndrome Scale; PSP, Personal and Social Performance Scale; SCZ, schizophrenia; TSQM, Treatment Satisfaction Questionnaire for Medication.
A slight decrease in extrapyramidal symptom rating scale was observed in 31 clinically stable adolescents when their oral antipsychotic (risperidone or olanzapine) was switched to risperidone long-acting injection during 24 weeks (Ruan et al. 2010). A decrease in weight (on average, −4.5 kg) and in prolactin serum level were also observed over the study period. Such improvement in metabolic profiles of participants might be overestimated, as 18 patients were switched from olanzapine to risperidone long-acting injection.
Boarati et al. (2013) used the Systematic Assessment for Treatment Emergent Effects to track the emergence of side effects in 19 adolescents treated with risperidone long-acting injection for severe BD. During the 24 months of the study period, the most frequent side effects were weigh gain (on average, +5.7 kg), hyperprolactinemia, and neurological symptoms. Of note, only patients with a good tolerance to oral risperidone were eligible, restricting the generability of this study.
Ceylan et al. (2017) used the Liverpool University Neuroleptic Side Effect Rating Scale to assess the tolerance of risperidone long-acting injection in 42 adolescents with various psychiatric disorders. After 2 months of treatment, almost one quarter of participants presented significant weigh change (on average, +1.6 kg). Other side effects were asthenia or sleepiness, neurological symptoms, dysmenorrhea/galactorrhea, and sexual problems.
No study reported side effects specifically due to local injection in children and adolescents while two studies sought it (Ruan et al. 2010; Boarati et al. 2013). The case-report by Akram and Mitchell (2019) was the only one to mention patient level of distress at receiving the injection as a possible limitation of providing LLA. Ceylan et al. (2017) noted that injection fear was a reason for drop out in 17% of adolescents treated with risperidone long-acting injection.
Acceptance
In the naturalistic studies conducted by Ruan et al. (2010) and by Boarati et al. (2013), the drop-out rate was, respectively, 19% and 26% after a 6-month follow-up period. In the study conducted by Ceylan et al. (2017), 43% of patients had withdrawn from LLA treatment at final endpoint (i.e., 19 weeks after initiation on average). The chart review of 12 Japanese adolescents treated with risperidone long-acting injection showed a 30% drop-out rate at 1 year (Suzuki et al. 2017). As presented in the Tables 2 to 4, the principal reasons for drop-out were side effects, the lack of clinical improvement, and other/unknown reasons. Petrić et al. (2019) noted that the patients treated with paliperidone palmitate achieved significantly higher scores on the convenience subscale, the global satisfaction subscale, and total score of the Treatment Satisfaction Questionnaire for Medication compared to patients treated with oral risperidone.
Discussion
Main findings on efficacy
Generally, the quality of evidence of these 22 studies was low (Supplementary Table S1). The two controlled trials reviewed (Suzuki et al. 2017; Petrić et al. 2019) were both based on retrospective analyses of the medical charts of small samples of adolescents with psychotic disorders (Petrić et al. 2019). Considering the limitation of retrospective chart reviews (Gearing et al. 2006), these findings should be interpreted with caution. The observation reported by Petrić et al. (2019) of a stronger decrease in the severity of psychiatric symptoms and lower readmission rate in patients treated with paliperidone palmitate compared to those with oral risperidone is, however, encouraging.
As previously mentioned by Lytle et al. (2017), the lack of standardization in participant selection could explain that most participants were youths with very severe forms of psychiatric disorders. How these findings could apply to nonobservant patients with less impairing psychiatric disorders remains to be known (Kishimoto et al. 2018). Except the study conducted by Ruan et al. (2010), all reviewed studies were conducted in patients who had not received an antipsychotic at the time of admission. It is therefore difficult to disentangle the benefit of long-acting formulation from the molecule itself.
The initial overlap during the initiation of the long-acting treatment may also result in confounding bias when the assessment of therapeutic outcomes occurs in the 2–3 weeks following the onset of LLA (Wisniewski 2011; Demirkaya and Zoroğlu 2016; Pope and Zaraa 2016; Ceylan et al. 2017; Fortea et al. 2018; Akram and Mitchell 2019; McInnis and Kasinathan 2019).
One study compared LLAs between them. In a retrospective chart review, Fortea et al. (2018) observed no difference in the changes of CGAS total score during the hospital stay of patients treated with long-acting risperidone versus long-acting aripiprazole versus paliperidone palmitate. Considering the wide heterogeneity of the reviewed studies in terms of participants' characteristics, it is difficult to attribute different outcomes to specific sociodemographic or clinical features. The most robust evidence supporting the efficacy of LLAs in pediatric populations was gained from studies in adolescents. As shown in Figure 2, the efficacy of LLAs was mainly documented for psychotic disorders (in particular, the impact of risperidone long-acting injection), and to a lesser extent for CD and BD. Evidence for the efficacy of other LLAs molecules and/or in other psychiatric diagnoses were much more marginal.
Main findings on tolerability and acceptance
A more stable blood level and a lack of first pass metabolism should theoretically result in a better tolerance of a long-acting formulation compared to oral antipsychotics (Ereshefsky et al. 1984; Kane et al. 2003). Some lines of evidence gained from observational studies in adults support this assumption. A lower rate of extrapyramidal side effects was noted in adults with schizophrenia treated with long-lasting risperidone compared to the observed rates in RCT for oral antipsychotics (Emsley et al. 2008). A reduction in serum prolactin was observed in adults who switched from oral risperidone therapy to 12 weeks of long-acting therapy (Knox and Stimmel 2004).
Studies where a standardized assessment of side effects was conducted (Ruan et al. 2010; Boarati et al. 2013; Fàbrega et al. 2015; Ceylan et al. 2017) showed that LLA-induced side effects are similar to those observed for oral antipsychotics (Cohen et al. 2012). Only one study used a measurement instrument not developed for oral antipsychotics (Boarati et al. (2013) and only one study mentioned side effects due to injection (e.g., inflammation, local pain or fear) (Akram and Mitchell 2019).
The lack of information about the time between the first injection of LLA and the onset of side effects makes it difficult to determine whether early-onset side effects are related to LLA or initially to coprescribed oral antipsychotic. The development of LLAs in a pediatric population requires better knowledge of long-term safety, in particular, how doses should be adapted to a pediatric population (Fernandez et al. 2011).
One may regret that so little attention has been devoted to the acceptance of LLAs in pediatric populations. Negative apriori could exist from the patient and his/her family due to a confusion between LLA and emergency treatment for agitation. The study conducted by Petrić et al. (2019) showed a better acceptance of a monthly injection of an LLA in its sample of adolescents treated for a first acute psychotic episode compared to daily intake of an oral antipsychotic. The drop-out rates reported in observational studies were roughly comparable to those observed for oral antipsychotics in usual settings in adolescents (Edgcomb and Zima 2018; Menard et al. 2019).
Barriers to use an LLA in pediatric populations should also be examined among professionals. Child and adolescent psychiatrists could feel less comfortable than their adult counterparts to prescribe an LLA considering the diagnostic challenges at these ages or a lack of clinical habit (Brissos et al. 2014). Modesitt et al. (2018) showed that psychiatrists specializing in pediatrics were less prone to prescribe an LLA in children and adolescents than professionals specialized in adult psychiatry. The lack of training of paramedical teams is also a barrier to the development of LLA as noted by Akram and Mitchell (2019) or Velligan et al. (2021).
Strengths and limitations
This is the first study that systematically reviewed the literature on LLAs in children and adolescents. We used a standard checklist to appraise the quality of the reviewed studies. The major limitation of this review is the poor quality of the studies reviewed, with open-label design, small sample size, and lack of controls. Considering the wide heterogeneity of the reviewed studies in terms of participants' features and study designs, it was difficult to determine whether the differences among studies could be attributed to differences between participants (e.g., psychiatric diagnoses). We tried to address these limitations by interpreting our results in light of findings from studies using an oral form of antipsychotics in pediatric samples or studies conducted in adults. Finally, it is possible that we missed relevant studies that should have been included in this review, in particular, unpublished ones resulting in publication bias.
Clinical Significance
Future clinical studies should focus on youths with EOS, first psychotic episode or BD. The use of an LLA in youths with severe CD was surprising (Kowalski et al. 2011; Fàbrega et al. 2015; Ceylan et al. 2017; Demirkaya et al. 2017) as most experts recommend a time-limited prescription of an antipsychotic in this indication (Gurnani et al. 2016). The lack of a study specifically conducted in youths with severe neurodevelopmental disorders is to be regretted, as this population faces substantial challenges in terms of medication adherence (Edgcomb and Zima 2018; Dinnissen et al. 2020).
According to our review, maintenance study using a noninferiority statistical analysis following a run-in period with an oral antipsychotic will be best-adapted to determine the benefit of using an LLA compared to an oral antipsychotic. Further clinical trials would also be well inspired to determine whether LLA are equivalent in terms of efficacy. Longitudinal observational studies could help determine the temporal sequence of side effects and possible dose-effect relationship. Concurrent repeated assessment of plasma level of the antipsychotic could clarify the pharmacokinetic profiles of LLA according to age.
Finally, considering the social and economic burdens indirectly related to poor adherence in children and adolescents (Edgcomb and Zima 2018), medico-economic studies would be worth performing. A better knowledge on the clinical utility of LLAs may be particularly important in low- and middle-income countries where a shortage of child and adolescent psychiatrists exists.
Conclusions
From this review, it can be concluded that the empirical evidence supporting the use of LLAs in children and adolescents are scarce, with preliminary findings for the efficacy of risperidone long-acting injection in psychotic disorders. Further research is needed to determine the effect of other LLAs in children and adolescents and their indications.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.