
Abstract

Introduction
Aripiprazole is an atypical neuroleptic with partial agonist activity at the dopamine 2 and serotonin 1A receptors, which is metabolized by the cytochrome p450 2D6 (CYP2D6) and CYP3A4 enzymes. Co-administration of aripiprazole and fluoxetine, a commonly prescribed serotonin reuptake inhibitor and a potent inhibitor of CYP2D6, may significantly increase plasma concentrations of aripiprazole through phenoconversion, increasing the risk of adverse events (AEs) (Jallaq et al. 2021). One possible AE is aripiprazole-induced hypersexuality; previously reported only in adult persons based on a recent systematic review (Reddy et al. 2018). We present a case of a 12-year-old male with a diagnosis of autism spectrum disorder (ASD) without intellectual disability who developed hypersexuality after initiation of aripiprazole as adjunctive treatment to fluoxetine.
Case
Psychiatry was consulted to evaluate a 12-year-old male due to worsening physical aggression. The patient's clinical course is outlined in Figure 1.
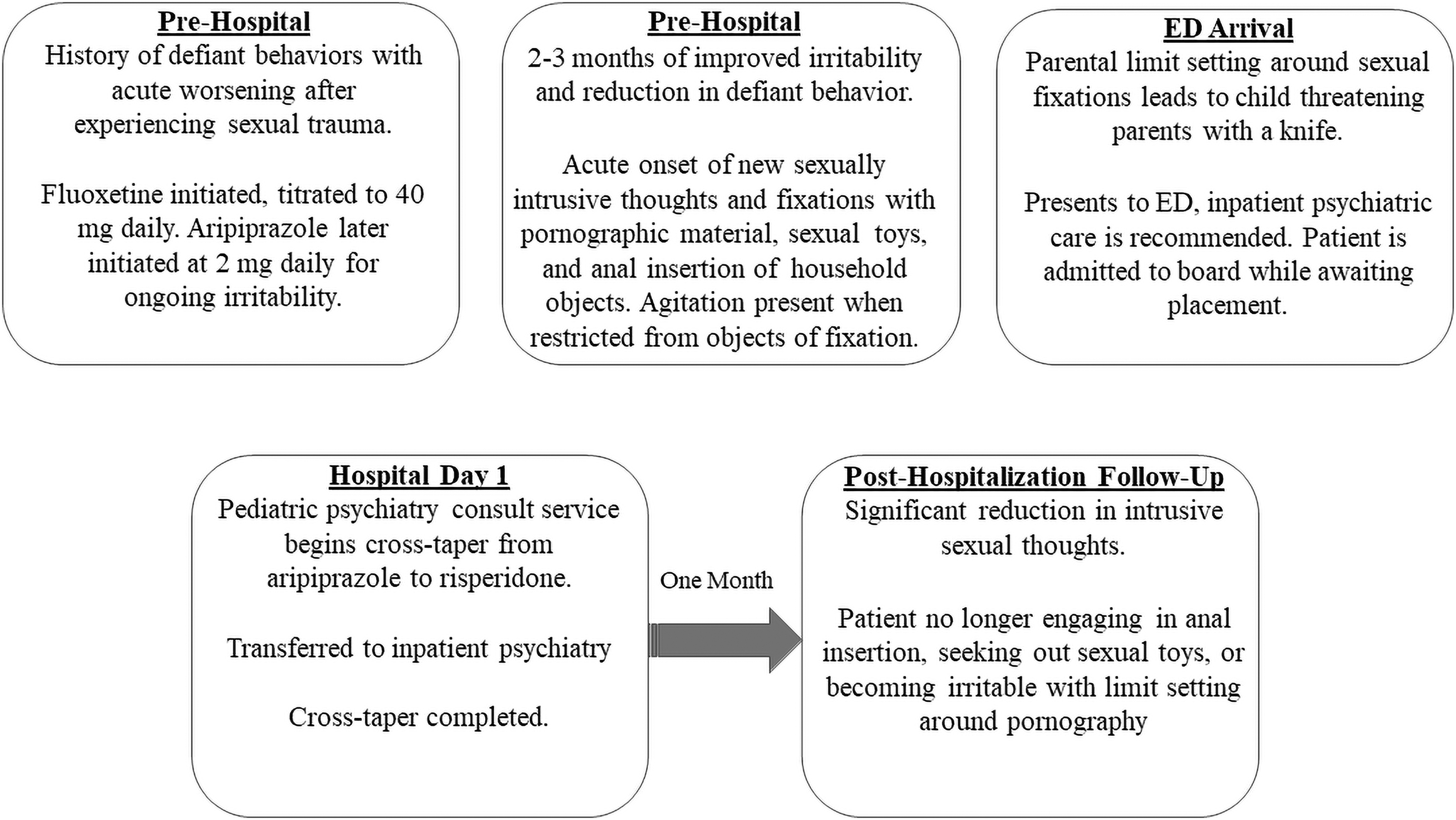
Course of illness.
Per report, the patient had experienced sexual trauma 3 years before the date of consultation and subsequently engaged in psychotherapy. He was also started on fluoxetine, which was increased to 40 mg daily. He overall demonstrated a fair clinical response, although continued to struggle with irritability leading to aripiprazole initiation at 2 mg daily. He soon developed new fixations with pornography, use of sexual toys, and anal insertion of household objects. When parents set limits around these behaviors, the patient developed suicidal ideation and homicidal ideation directed toward parents. The patient was cross-titrated from aripiprazole to risperidone, which was accompanied by a return to his baseline sexual interests and behaviors. To avoid further AEs, risperidone was slowly uptitrated given its CYP2D6 activity as well.
Discussion
In the adult literature, multiple mechanisms for aripiprazole-induced hypersexuality have been proposed. These include a possible link between compulsive gambling, hypersexuality, and treatment with dopaminergic agonists in Parkinson's disease (Moore et al. 2014); as well as use of high-potency dopaminergic antagonists before initiation of aripiprazole. The latter could result in upregulation of dopamine receptors, which would increase the risk of hypersexuality if aripiprazole was rapidly added after high-potency antagonist discontinuation (Mohan et al. 2017).
Given that aripiprazole and risperidone are the only two Food and Drug Administration-approved treatments for irritability in ASD, awareness of this possible interaction when transitioning from risperidone to aripiprazole is paramount. Furthermore, recent literature suggests that individuals with ASD commonly experience dopaminergically driven side effects of neuroleptics such as tremor, akathisia, and tardive dyskinesia (Alfageh et al. 2019). Thus, it is possible that baseline dopaminergic dysfunction or neuroleptic sensitivity may be a neurobiological sequelae of ASD; increasing the risk of other dopaminergically driven side effects such as hypersexuality.
To our knowledge, there are no other case reports of aripiprazole-induced hypersexuality in pediatric persons with ASD (Reddy et al. 2018). This case highlights the importance of CYP monitoring and consideration of hypersexuality as an AE related to aripiprazole, which in adults presents within 1–2 weeks of drug initiation and may continue for 3 weeks after discontinuation (Reddy et al. 2018). Finally, this case demonstrates the importance of establishing a baseline of sexual behavior in young persons with or without a trauma history or neurodevelopmental disorder when evaluating for possible hypersexuality.
Footnotes
Authors' Contributions
Conceptualization, investigation, and writing—original draft by J.R.S. Conceptualization, writing—review and editing by D.L.P.
Acknowledgments
All authors have authorized the submission of this article. The authors thank the patient and their parents for allowing publication of their course of illness.
Disclosures
No competing financial interests exist.