
Abstract
Objective:
Anxiety disorders are among the most common co-occurring conditions in autism spectrum disorder (ASD). Despite their prevalence and impact, there are no randomized controlled trials (RCTs) aimed at evaluating the efficacy of selective serotonin reuptake inhibitors (SSRIs) for anxiolysis in this population, who may have a different biological basis for anxiety.
Methods:
Secondary analyses of the STAART double-blind, placebo-controlled RCT of citalopram in children with ASD examined whether citalopram reduced anxiety measured on the parent-reported Child and Adolescent Symptom Inventory-4 (CASI-4) as the primary outcome. An intention-to-treat analysis involving all 149 participants used multiple imputations for missing data and included baseline stratification factors of age group and site, among others. We prespecified as clinically significant a 33% reduction in anxiety in citalopram versus placebo, coinciding with 80% power. We tested whether communicative ability on the Vineland Communication score moderated treatment effect and explored whether initial anxiety was associated with greater adverse events, which could impact on dose titration and achieving optimal dose.
Results:
Both groups showed substantial reduction in anxiety. Citalopram was associated with a nonsignificant 16.5% greater reduction (observed coefficient = −0.181, bootstrap standard error = 0.126, p = 0.151, confidence interval = −0.428 to 0.066). Anxiety reports were significantly lower in children with reduced communicative ability, but communicative ability did not moderate the treatment effect (interaction p = 0.294). Initial anxiety levels were not associated with increased adverse effects (interaction ps 0.162–0.954).
Conclusion:
Citalopram did not statistically significantly improve anxiety in children with ASD. Clinicians should be cautious in their use of SSRIs for this indication. There remains a need for well-powered clinical trials testing the efficacy of SSRIs among autistic children with anxiety disorders.
Introduction
Autism spectrum disorder (ASD) is a heterogeneous condition characterized by impairments in social communication, restricted, repetitive behaviors and interests and sensory abnormalities. ASD begins early in development and typically has lifelong impact on a range of domains including socialization, cognition, adaptive function, and physical, and mental health (Lord et al. 2020).
Anxiety disorders are one of the two most common co-occurring conditions in autism (Simonoff et al. 2008; Lai et al. 2019). Indeed, anxiety was highlighted in Kanner's (1943) first description of autism as a disorder of affective control. Prevalence estimates of anxiety vary but converge around 40%–50%, with a substantial additional proportion exhibiting subdiagnostic symptoms (Kent and Simonoff 2017). Anxiety symptoms and disorders in people with ASD can be present from the preschool period (Gadow et al. 2004; Salazar et al. 2015), remain common across the lifespan (Lever and Geurts 2016), and appear to be stable over time (Simonoff et al. 2013a; Stringer et al. 2020).
There is considerable inconsistency about whether the prevalence of anxiety disorders varies according to the presence of intellectual disability (Kent and Simonoff 2017) with methodological concerns that anxiety may be particularly under-recognized and under-reported in those with low levels of verbal ability (Gadow et al. 2004; Sukhodolsky et al. 2008; Hallett et al. 2013a; Salazar et al. 2015). Anxiety can cause high levels of distress and autistic people and their parents/caregivers have ranked the study of anxiety and its interventions as one of the most important research areas (Wallace et al. 2014).
In nonautistic individuals, there is an established evidence base demonstrating benefits of pharmacological interventions for anxiety disorders in nonautistic children (Walkup et al. 2008) and adults (Baldwin et al. 2011). However, to date, no randomized controlled trials (RCTs) have focused on their use in children with ASD and co-occurring anxiety. There are important biological and psychological differences in the ASD population that may alter the efficacy and safety of using selective serotonin reuptake inhibitors (SSRIs) in this patient group. About one-quarter of people with ASD have hyperserotonemia (Gabriele et al. 2014), but the role of this variability on SSRI treatment response is not well understood.
More generally, patients with ASD may be more susceptible to adverse effects related to pharmacological treatments, as shown for methylphenidate (Research Units on Pediatric Psychopharmacology Autism Network 2005; Simonoff et al. 2013b). Because of the impairments in communication, interoception, and emotional literacy, it may be more difficult to ascertain both internally experienced treatment response and adverse effects in people with ASD.
There are also cautions about SSRIs in younger people. In the nonautistic population, younger people (Strawn et al. 2014) and children compared with adolescents are more sensitive to treatment-emergent adverse effects, particularly behavioral activation (Safer and Zito 2006). Although current guidelines do not recommend the use of SSRIs in the routine treatment for anxiety in ASD (National Collaborating Centre for Mental Health 2013; Williams et al. 2013; Vasa et al. 2014; Howes et al. 2017), in the United States and United Kingdom SSRIs account for at least 10%–20% of psychiatric prescriptions for youth and 20%–50% in adults with ASD (Aman et al. 2005; Oswald and Sonenklar 2007; Hsia et al. 2014; Houghton et al. 2017).
To explore the efficacy and adverse effects of SSRIs in treating anxiety in people with ASD, we make use of previously collected data from an RCT of citalopram in children with ASD, aimed at evaluating its efficacy in reducing core symptoms of repetitive and stereotyped behavior (King et al. 2009). We capitalize on the blinded parent-reported measures of anxiety collected before randomization and at 12 weeks to examine the effects of citalopram compared with placebo.
Methods
Study design
A detailed description of the STAART citalopram trial has been published previously (King et al. 2009). The clinical trial (identifier: NCT00086645) was registered at
The mean (standard deviation [SD]) dosages of citalopram and placebo at week 12 were 16.5 (6.5) mg (mode, 20 mg) and 18.5 (3.5) mg (mode, 20 mg), respectively (p = 0.05). Parent-reported adherence to treatment was high in both groups (mean [SD], 96.1% [7.8%] for the citalopram-treated group and 98.6% [3.1%] for the placebo group; p = 0.03).
The primary analyses found no significant difference in response on the Clinical Global Impressions—Improvement (CGI-I) scale between the citalopram (32.9% response rate) and placebo group (34.2% response rate) (King et al. 2009). However, compared with placebo, the citalopram group was significantly more likely to exhibit adverse events (97.3% reported at least one treatment-emergent adverse event) than the placebo group (86.8%, p = 0.03).
For the present secondary analyses, the aim was to determine whether citalopram reduced levels of parent-reported anxiety symptoms in comparison with placebo and whether anxiety response was moderated by adverse effects.
Subjects
A total of 149 children (128 males) aged between 5 and 17 years (mean = 9.4 years, SD = 3.1 years) who (1) met Diagnostic and Statistical Manual-IV-TR (DSM-IV-TR) criteria for autistic disorder (American Psychiatric Association 2000), Asperger disorder, or pervasive developmental disorder, not otherwise specified (determined by an experienced clinician and informed by the Autism Diagnostic Interview—Revised [ADI-R (Lord et al. 1994)] and the Autism Diagnostic Observation Schedule [ADOS (Lord et al. 2000)]), (2) had an illness severity rating of at least moderate on the Clinical Global Impressions—Severity (CGI-S) of Illness Scale (Guy 1976), and (3) at least moderate on compulsive behaviors (≥8 on the sum of items 1A, 2, 3, and 5) scores measured with the Children's Yale-Brown Obsessive Compulsive Scales modified for pervasive developmental disorders (CYBOCS-PDD) (Scahill et al. 2006). Exclusion criteria can be found in the primary paper (King et al. 2009) and at
Each of the six participating sites received ethical approval from their institutional review board (IRB) and informed consent was obtained from all study participants and/or legal representatives before data collection. An external board convened by the National Institute of Mental Health monitored the trial. No additional approval was sought for these secondary analyses.
Study assessments
Primary outcome
The primary outcome measure for the current analysis was parent-reported anxiety at 12 weeks postrandomization, based on a total score for 20 items from the Child and Adolescent Symptom Inventory-4 (CASI-4) (Gadow and Sprafkin 2002). Items are scored from 0 to 3 (0 = Never; 1 = Sometimes; 2 = Often; 3 = Very Often), allowing a potential score range of 0–60. These items were used in previous studies of the parent-reported anxiety subscale in children with ASD (Sukhodolsky et al. 2008; Hallett et al. 2013a) (see Supplementary Table S1 for individual items) and include domains of generalized anxiety disorder, simple phobia, social phobia, and separation anxiety disorder, but not obsessive-compulsive disorder or posttraumatic stress disorder, in line with the inclusion of disorders in pharmacological studies in typically developing anxious children (Research Units on Pediatric Psychopharmacology 2001; Walkup et al. 2008). Furthermore, the obsessive compulsive disorder (OCD) symptoms have potential overlap with restricted and repetitive behaviors, for which no treatment effect was identified in the primary analysis.
For the present analysis, as participants had not been selected to have high anxiety levels, we looked for a treatment-related decrease in symptoms that was proportional to each participant's level at baseline (thus no reduction being expected for those without symptoms) with a positive clinical response defined as a 33% decrease in the total anxiety score at week 12 postrandomization.
For exploratory analyses, we also defined a subgroup of participants whose questionnaire scores were above the predetermined threshold for a likely anxiety disorder in at least one of the above categories (Gadow and Sprafkin 1997).
Adverse events
Treatment-emergent adverse events were elicited at each biweekly visit using the Safety Monitoring Uniform Report Form completed by the clinician with the parent and on examination (Greenhill et al. 2004). We grouped the individual adverse events into three categories in line with their original description: neuropsychiatric adverse events (increased energy level, disinhibited or impulsive behavior, decreased attention, hyperactivity, and stereotypy), insomnia-related adverse events (any insomnia, initial, midcycle or terminal), and non-central nervous system (CNS) adverse events (diarrhea, vomiting or nausea, and dry skin or pruritus).
Additional included measures
The additional measures were used to improve efficiency, reduce bias associated with missing data, and to examine potential masking of treatment effect arising from the difficulty of reporting on anxiety symptoms of children with poor communication. These measures were the parent-reported Vineland Adaptive Behavior Scale (VABS) communication scale age equivalent, the ADOS module (which is selected based on spoken language competence), chronological age and nonverbal IQ, measured variously on the Leiter—Revised, Wechsler Intelligence Scale for Children-IV, Wechsler Abbreviated Scale of Intelligence, Mullen Scales of Early Development, and Stanford-Binet Test.
The severity of repetitive and stereotyped behavior, measured on the CGI-S, was weighted to consider repetitive behaviors, as well as the CGI-I score at 12 weeks. As behavioral disturbance has also been associated with parent reports of anxiety symptoms (Sukhodolsky et al. 2008) and could affect parents' ability to identify anxiety, the baseline irritability subscale of the parent-reported Aberrant Behavior Checklist (ABC) (Aman and Singh 1985) was added. Body mass index (BMI), in conjunction with age, accounts for baseline weight differences that could be related to therapeutic drug levels.
Statistical analysis
Drawn up by A.P., F.M., and E.S. who were not involved in the original trial and without knowledge of participants' treatment assignment, the Statistical Analysis Plan was preregistered on The Open Science Framework (
This model is likely statistically more powerful than limiting the analysis to the high scorers only. As a post hoc sensitivity analysis (added after preregistration of the analysis plan), we also fitted a model just to those participants whose questionnaire scores were above the predetermined threshold for a likely anxiety disorder as described previously. The models were estimated using a structural equation modeling (SEM) framework in which baseline and endpoint are allowed a nonzero covariance, and no treatment group difference is allowed for the response prerandomization. Although yielding the same estimates as analysis of covariance (ANCOVA) when data are complete, this method incorporates incomplete observations.
Analyses were performed in Stata version 17.0 (StataCorp 2021) using the sem command option, method(mlmv), which is consistent with ITT. Original stratification variables were included in the analysis model (age group and site). Residuals were checked using normal probability plots. Statistical tests and 95% confidence intervals (CIs) were two sided.
We then examined whether the effect of citalopram on anxiety is moderated by communicative level, following our hypothesis that parents may find it more difficult to discern their children's anxiety when they cannot directly communicate these experiences. We used the VABS Communication age equivalent score and report both the VABS main effect and the group (citalopram vs. placebo) by VABS interaction. Finally, exploratory analysis examined whether initial levels of anxiety might be associated with higher levels of adverse events, which could have interfered with achieving optimal dose for anxiety reduction. We examined whether the three adverse events profiles were influenced by prerandomization CASI-4 score and whether this differed by group (group-by-baseline anxiety score interaction). This used Poisson regression analysis conducted separately for each of the three adverse event categories, adjusting for dose-by-weight.
Missing data
We used single imputation of occasional missing items by chained equations and predictive mean matching (White et al. 2011). The items were imputed in a single model incorporating both baseline and outcome. Nonverbal IQ, VABS Communication age equivalent, CGI-S at baseline as well as CGI-I at week 12, ABC irritability, BMI, sex, site, treatment group and chronological age were included in the imputation model.
Total scores were then calculated using the complete and imputed item values for participants with 6 or fewer missing items (30% or fewer items missing out of the 20 items). For those with >30% of missing items, their total score was set to missing before the main analysis, thus being treated as Missing-At-Random (MAR) within full maximum likelihood model estimation.
Sensitivity analysis
The main analysis was repeated with missing baseline and endpoint data in the treatment group replaced by a 10% worsening of scores (i.e., 10% greater anxiety). This provided a further test of the robustness of the primary analysis.
Power
Using the ITT sample of 149, power was calculated, subsequent to specifying the level of clinically significant treatment effect, using an ANCOVA approach for two-tailed alpha = 0.05, assuming a correlation of 0.5 between measurement time points. This gave 80% power for an effect size of −0.4 on the log scale, equating to a 100(1 − exp(−0.4)) ≃33% reduction in anxiety in the citalopram group compared with placebo. Using the same calculation adjusting for the number of complete cases specified in the primary paper (i.e., 13 cases missing in each group), the power would be 73% to detect the same effect size.
Results
Efficacy
Table 1 provides the sample characteristics of the 149 participants. At baseline screening, 118 (citalopram n = 60, placebo n = 58) had complete data on all anxiety items, a further 19 had 6 or fewer missing items that were imputed, and 12 were left missing (See Supplementary Table S2). Corresponding numbers for the week 12 endpoint were 94 (citalopram n = 49, placebo n = 45), with 20 imputed and 35 left missing. The distribution of anxiety scores by group and time point are given in Figure 1.
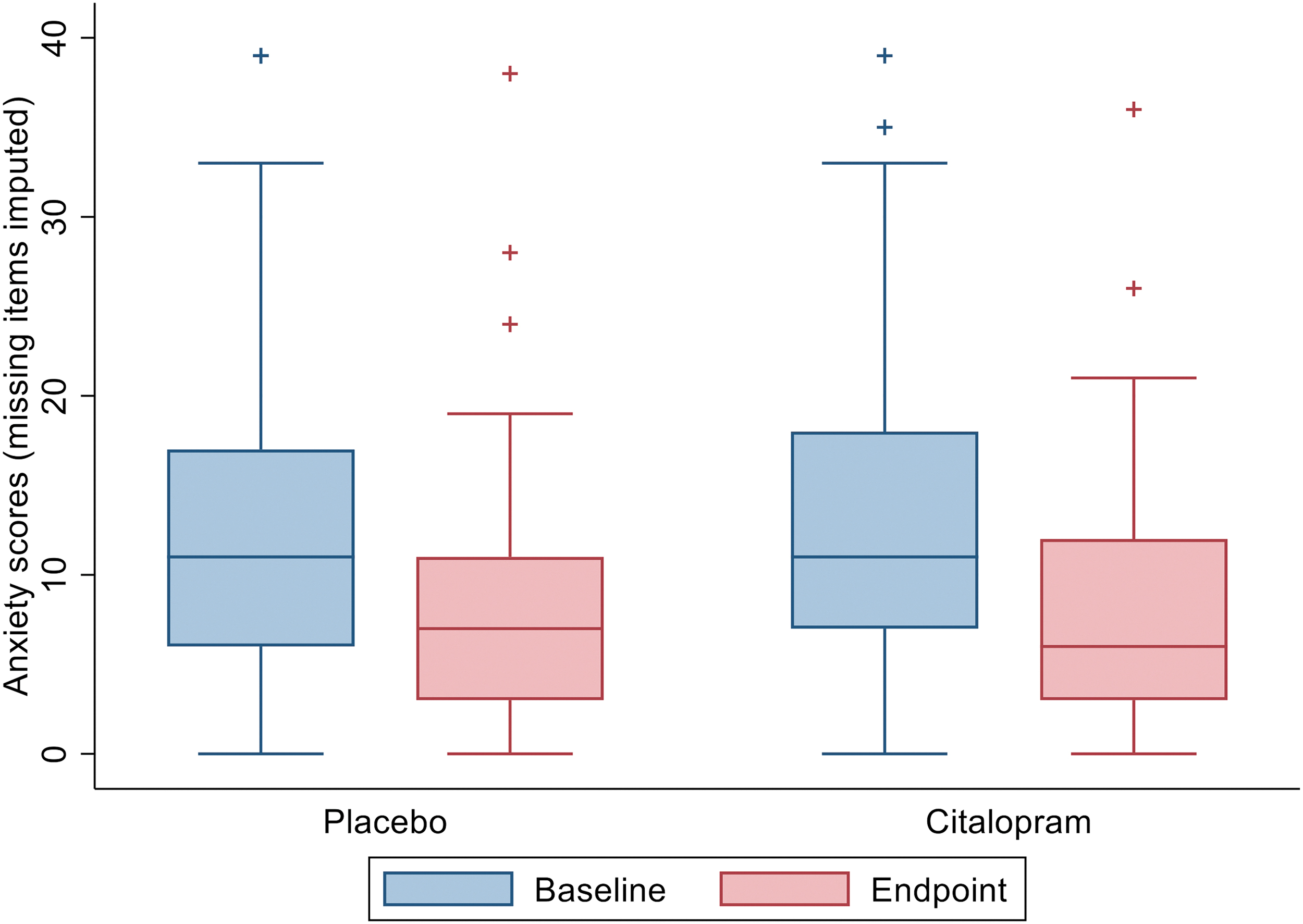
Primary outcome (anxiety as measured with the CASI-4) for baseline (Screener: placebo n = 70, citalopram n = 67) and endpoint (week 12: placebo n = 58, citalopram n = 56)—missing items imputed for those with 6 or fewer missing of the 20 items. CASI-4, Child and Adolescent Symptom Inventory-4.
Characteristics of the Citalopram-Treated and Placebo Groups
Measures of nonverbal IQ and the ADOS module were completed at one of the following time points (ranging from screener, baseline, week 2 or week 4).
These measures were completed at the screening time point.
ADOS, Autism Diagnostic Observation Schedule; BMI, body mass index; CGI-S, Clinical Global Impressions-Severity; SD, standard deviation; VABS, Vineland Adaptive Behavior Scale.
There was a substantial decrease in parent-reported anxiety symptoms in both groups over the course of the trial. The estimated baseline mean of 11.1 symptoms (95% CI, 9.7 to 12.5) fell by 32% in the placebo group to 7.5 (95% CI, 6.0 to 8.9), and by 44% in the citalopram group to 4.7 (95% CI, 2.6 to 6.8). The estimated effects are given in Figure 2, using the log scale on which the analysis was undertaken in the left panel. The simple additive treatment effect on this log scale corresponded to a proportional/multiplicative effect on the raw total score scale. The placebo group experienced a substantial reduction in symptoms, falling almost exactly on the red-dashed line for 67% of baseline.
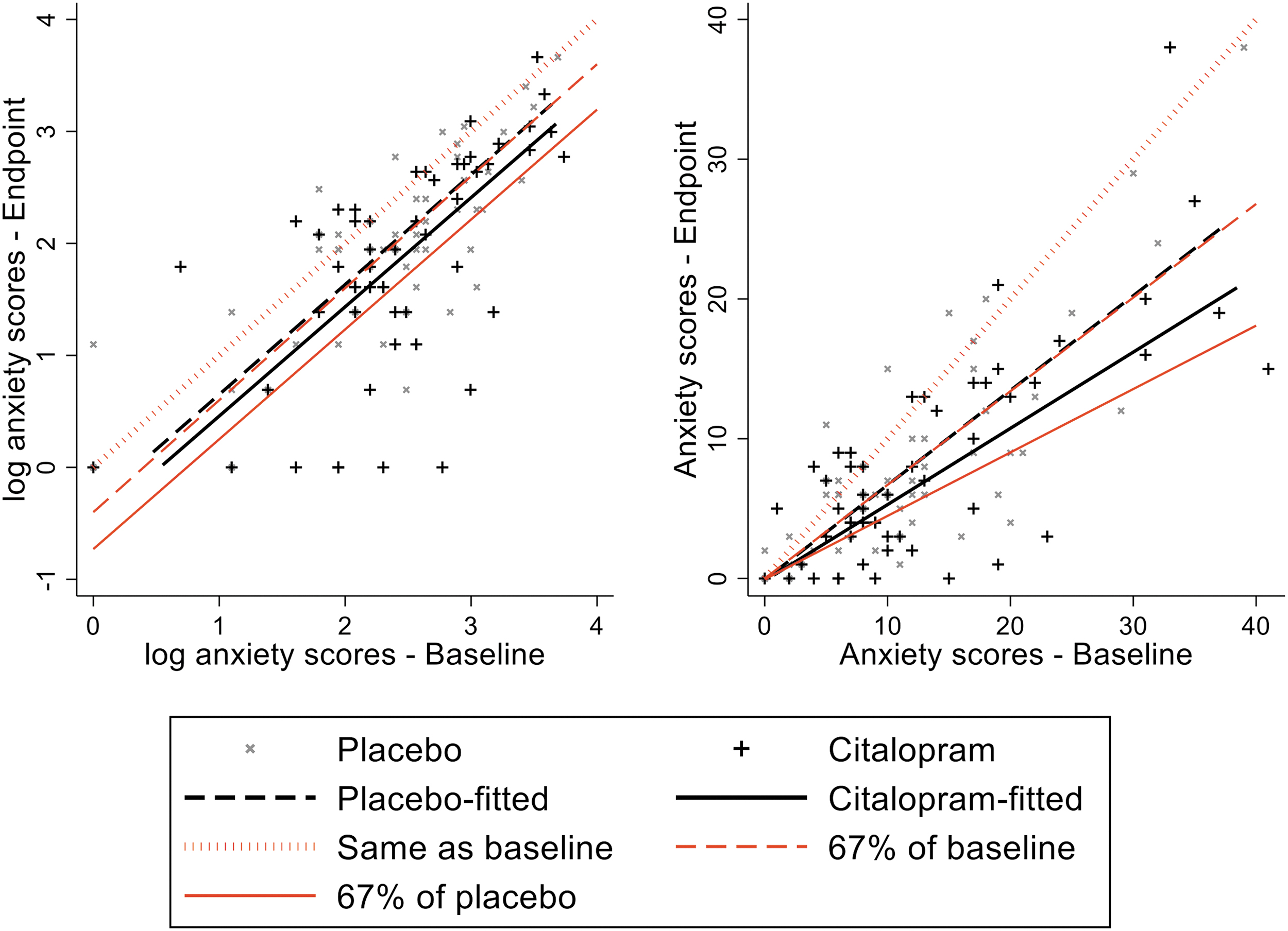
Estimated effects of citalopram versus placebo on anxiety (as measured with the CASI-4), compared with hypothetical levels of change between baseline and endpoint: Log-transformed scores (left) and back transformed to raw scores (right). The figure provides the actual reduction in placebo and citalopram arms against predictions for no change (same as baseline), a reduction to 67% of baseline (just achieved by placebo—the “placebo effect”) and a further 33% treatment effect, not achieved by citalopram. This proportional effect on the raw score scale is given on the right panel, the size of the expected treatment effect on the raw score increasing with the baseline level of symptoms and no effect expected for those with no symptoms. The red-dotted diagonal line indicates hypothetical continuity of the same level of anxiety. CASI-4, Child and Adolescent Symptom Inventory-4.
The line for the citalopram group, although lower than placebo, does not achieve the additional 33% reduction we set as the minimum clinical requirement (solid red line). Model estimates found no significant difference in the reduction of anxiety symptoms from baseline to week 12 between the citalopram-treated and placebo group (observed coefficient = −0.181, bootstrap standard error [SE] = 0.126, p = 0.151, 95% CI = −0.428 to 0.066). This corresponded to a 16.5% greater reduction in the citalopram group, less than the level of 33% between-groups difference preidentified as clinically significant. However, this clinically significant threshold fell within the CI of our estimate, which spanned a relative reduction of 36.8% to an increase of 3.7% (1000 replicate bootstrap CI).
The questionnaire algorithm for likely disorder indicated 86 of the 149 (58%) children met threshold for at least one anxiety disorder (Fig. 3). The model fitted to this subset estimated the initial symptom score of 16.5, declining by 40.2% (95% CI, 31.8 to 48.5) in the placebo group and 49.5% (95% CI, 37.7 to 61.4) in the citalopram group, corresponding to 15.6% greater reduction (95% CI −8.1 to 38.3) in the citalopram group, very close to the whole sample estimate.
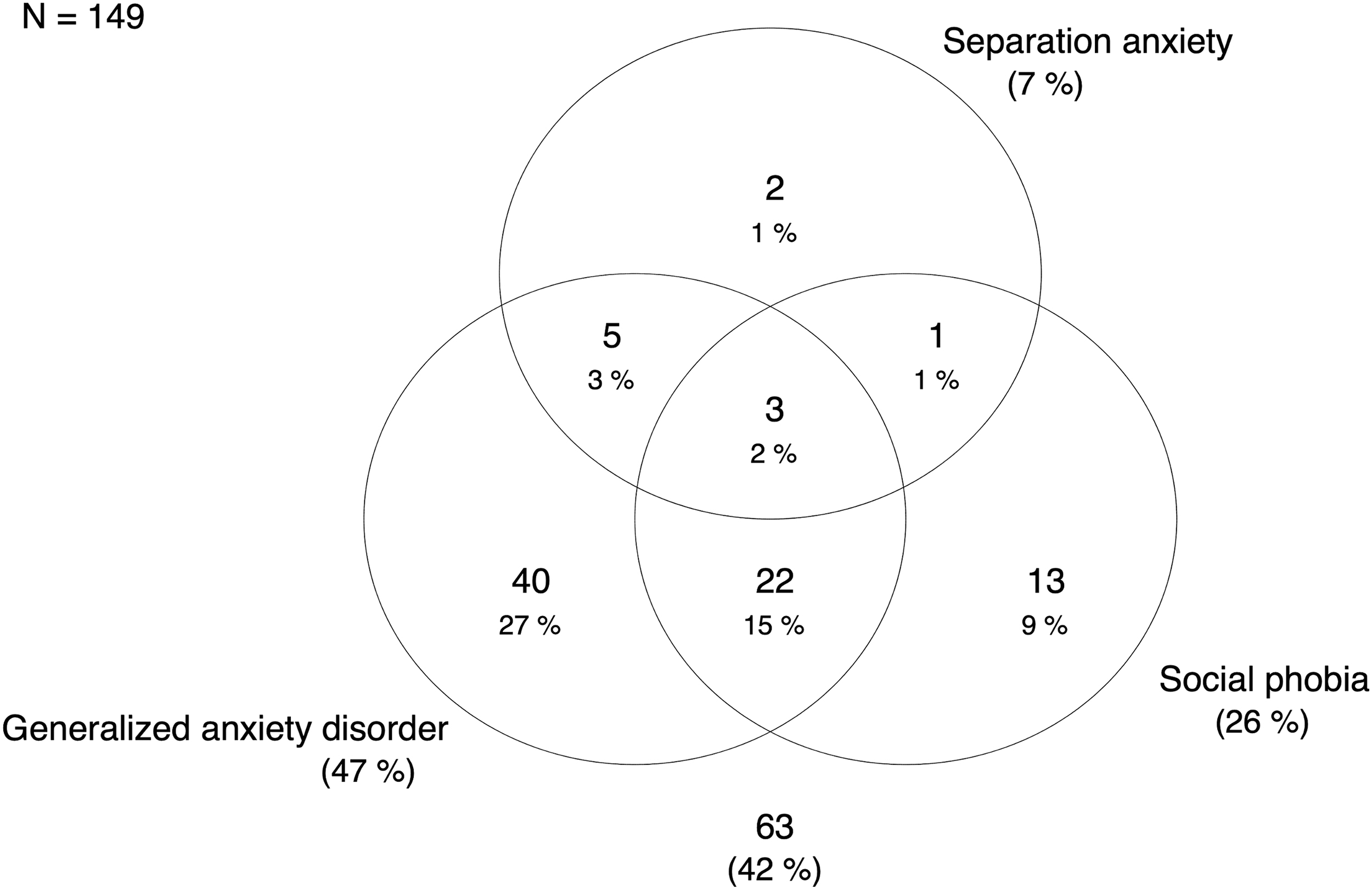
Venn diagram of anxiety disorders according to the diagnostic algorithm of the CASI-4. CASI-4, Child and Adolescent Symptom Inventory-4.
A sensitivity analysis, using total scores, where scores for those in the citalopram-treated group with more than six missing items for screener or outcome anxiety were replaced with a 10% worsening of their total anxiety score, produced similar results to the main analysis, with a 13.4% reduction in the citalopram group compared with placebo (observed coefficient = −0.144, bootstrap SE = 0.099, p = 0.144).
Moderation of treatment effect by communication level
We identified a main effect of VABS communication level on anxiety score at week 12 (coefficient = 0.006, SE = 0.002, p = 0.018, 95% CI = 0.001 to 0.010), supporting the idea that parent-reported anxiety symptoms are lower in children with reduced communication ability. However, the effect of citalopram on reducing anxiety from screen to week 12 was not moderated by communication level (group-by-communication level interaction: coefficient = −0.003, SE = 0.003, p = 0.294, 95% CI = −0.009 to 0.003), indicating that the lower anxiety scores in low-functioning children does not mask a significant treatment effect.
Adverse events
As detailed in the primary paper, adverse events were more likely to be exhibited in the citalopram-treated group. Table 2 describes the number of participants from the citalopram and placebo groups exhibiting at least one adverse event in each of the three domains. Poisson regression analysis, examining whether the adverse event score is influenced by baseline anxiety and if this differs by group (adjusting for final prescribed dose by weight: citalopram n = 51, mean = 0.51, SD = 0.26; placebo n = 51, mean = 0.54, SD = 0.24), did not show a significant group-by-baseline anxiety score interaction for any of the adverse events categories (neuropsychiatric: coefficient = −0.45, SE = 0.32, p = 0.162, 95% CI = −1.08 to 0.18; insomnia: coefficient = −0.40, SE = 0.34, p = 0.248, 95% CI = −1.07 to 0.28; non-CNS: coefficient = −0.02, SE = 0.43, p = 0.954, 95% CI = −0.87 to 0.82).
The Number of Participants Experiencing at Least One of the Following Adverse Event Types
Participants experienced at least one of the following: increased energy level, disinhibited or impulsive behavior, decreased attention and concentration, hyperactivity, stereotype.
Participants experienced at least one of the following: initial, midcycle or terminal insomnia.
Participants experienced at least one of the following: diarrhea, vomiting or nausea, dry skin or pruritus.
CNS, central nervous system.
Discussion
Anxiety symptoms and disorders are one of the most common co-occurring conditions in children and adolescents with ASD and SSRIs are frequently prescribed, despite an absence of RCT-based evidence. Here, we tested for a treatment-specific reduction in parent-reported anxiety symptoms in youth receiving citalopram versus placebo using data from an RCT aimed at assessing the efficacy of citalopram for repetitive behaviors. We predefined a clinically meaningful effect size of −0.4, which for our log-transformed scores approximated a 33% reduction in symptoms compared with the placebo group. Both groups showed a reduction in CASI anxiety symptom scores across the 12-week trial, suggesting substantial placebo effect, regression to the mean or both. The observed greater improvement in the citalopram compared with placebo group of 16.9% was robust to missing data assumptions, and selection of participants for disorder, increasing confidence in the estimated group difference. This difference had wide CIs but was not statistically significant and did not meet our threshold for clinical significance.
The previous literature on SSRIs in ASD using randomized and blinded designs is extremely limited. In a placebo-controlled crossover trial of fluoxetine in 45 children with ASD designed to examine effects on core symptoms and repetitive behaviors, there was a lower rate of treatment-emergent anxiety on active treatment versus placebo (Hollander et al. 2005). Another tiny (N = 6) placebo-controlled crossover RCT of fluoxetine in children reported significant anxiety reduction on active medication (Buchsbaum et al. 2001). Other findings are limited owing to open-label or case review designs. The case review literature may be over-optimistic in describing benefits of SSRI treatment because it does not account for placebo effects, which were of moderate magnitude in this study (Thorkelson et al. 2019).
We confirmed the finding from other studies using the CASI-4 (Sukhodolsky et al. 2008; Hallett et al. 2013a) that parent-reported levels of anxiety symptoms are higher in children with greater communicative ability. However, the current analyses do not identify a stratification effect, or that the inclusion of lower communication ability children masked a treatment effect. Furthermore, the finding that initial anxiety scores neither predicted level of adverse events, nor showed an interaction with treatment group, provides some reassurance that achieving effective dosing was not limited by levels of anxiety.
Strengths of this study include its moderately large sample size. The original study was well-conducted and described; it used an ITT design with comparatively high levels of completion and careful medication dose adjustments. The present statistical analysis was prespecified and lodged on Open Science Framework, except for the additional sensitivity analysis that was restricted to the participants with a likely anxiety disorder. The structural equation modeling and imputation provided efficient and unbiased estimates of ITT effects. The selection of anxiety items from the parent-reported CASI-4 is consistent with that used in other autism studies (Sukhodolsky et al. 2008) and has minimal if any overlap with repetitive behaviors examined in the primary paper.
An important limitation is that the original study was not designed to address the present question of efficacy of SSRIs for anxiety disorders. We therefore tested for a treatment effect that was proportional to the initial severity of anxiety symptoms, avoiding the dilution effect of participants with little anxiety on treatment effect estimation. Our sensitivity analysis limited to those with symptom levels indicative of an anxiety disorder provided a similar point estimate, but with expected wider CIs. The CASI-4 is not a diagnostic instrument and the use of questionnaire scores to identify a subgroup with likely disorder should be treated with caution. This study did not include blinded clinician ratings of global improvement focusing on anxiety, currently the gold standard in many psychiatry studies. Furthermore, it is unclear whether the CASI-4 is the most sensitive measure of anxiety symptoms in children with ASD (Hallett et al. 2013b).
Consistent with other research groups using the CASI-4, we found reduced levels of parental symptom reports in those with lower communication levels, which may reflect measurement insensitivity in children with significantly reduced communication. New measures focusing on observable behaviors may be more sensitive to nonverbal manifestations of anxiety (Scahill et al. 2019). In evaluating treatment effects in people with ASD and significant impairments in communication, an optimal measurement strategy would also include objective measures. Children with ASD and anxiety often have high levels of irritability and maladaptive behaviors and previous research has shown these characteristics are difficult for parents to distinguish on questionnaires (Mikita et al. 2015). Future consideration of measures and experimental paradigms that discriminate anxiety- and anger-mediated arousal will be important.
Finally, the criterion of a Cohen's d effect size of 0.4 on the log-scale (corresponding to a 33% reduction) that we chose was in part in order that the analysis would have adequate power for any possible positive finding to be reliable. However, Cohen's d is scaled by baseline SD, and an effect size of 0.4 may correspond to a substantially greater change where participants are not selected on baseline score (as here) than that found in the typical purpose designed trial where participants are recruited to be uniformly high scorers. For example, Wagner et al. (2004) report data for a similarly sized but purpose-designed RCT for non-ASD adolescents, all with high scores, corresponding to symptom reductions of ∼28% for placebo and ∼38% for citalopram, effects a little smaller than those that we found (32% and 44%). However, with their more homogeneous participants, these effects gave a statistically significant citalopram advantage and provided a Cohen's d effect size of more than 1.
Conclusions
The present study finds a modest, nonsignificant benefit of citalopram over and above that achieved by placebo for reducing parent-reported anxiety symptoms in children with ASD. Although the sample size is relatively large and the effect robust to different model assumptions, the CIs on the estimated effect were very wide and hence this finding still leaves uncertainty about the potential of SSRIs to provide benefit for patients with ASD and anxiety. Moreover, this study did not specifically enroll children with anxiety disorders.
Our findings indicate that there is a need for an authoritative trial of SSRIs for the treatment of anxiety in children with ASD.
Clinical Significance
This study finds a modest, nonsignificant benefit of citalopram over and above that achieved by placebo for reducing parent-reported anxiety symptoms in children with ASD. The original study showed that SSRIs can have significant adverse effects. Therefore, clinicians should be cautious in their use of SSRIs for the treatment of anxiety in children with ASD. This study does not alter current guidance suggesting that cognitive behavior therapy (CBT)-based psychological interventions should be the first line of treatment and SSRIs should be reserved for those who cannot make use of or do not respond to CBT, even when adapted or mediated by a parent/caregiver, or where levels of anxiety are so severe that a psychological approach cannot be implemented (National Collaborating Centre for Mental Health 2013). Our findings highlight the need for an authoritative trial of SSRIs for the treatment of anxiety in people with ASD.
Footnotes
Acknowledgments
The authors thank Dr. Kenneth Gadow for providing algorithms to calculate disorder cutoffs from the CASI-4. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Disclosures
E.S. and A.P. currently receive support from the National Institute of Health Research (NIHR) Biomedical Research Centre at South London and Maudsley Foundation Trust (IS-BRC-1215-20018), the NIHR through a program grant (RP-PG-1211-20016) and Senior Investigator Awards (NF-SI-0514-10073 and NF-SI-0617-10120), the European Union Innovative Medicines Initiative (EU-IMI 115300), Autistica (7237)m Medical Research Council (MR/R000832/1, MR/P019293/1), the Economic and Social Research Council (ESRC 003041/1) and Guy's and St Thomas' Charitable Foundation (GSTT EF1150502) and the Maudsley Charity. B.H.K. receives support from the University of California San Francisco. E.H. receives support from the Department of Defense Autism Research Program (AR160104), Orphan Products Division of Food and Drug Administration (FD-R-05106), and Roche Pharmaceuticals and GW Pharma. L.S. currently receives support from Duke University, the U.S. National Institutes of Health (P50HD093074-03) and (HHSN275201000003I TO), and Roche Pharmaceuticals and Boehringer-Engelheim to conduct Industry Sponsored Trials. All other authors have no competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.