
Abstract
Objective:
Antipsychotic-related prolactin changes may expose children and adolescents to severe adverse reactions (ARs) related to pubertal development and growth. We therefore aimed to assess the effects of antipsychotics on prolactin levels and associated somatic ARs in children and adolescents.
Methods:
We systematically searched PubMed and CENTRAL for placebo-controlled randomized trials of antipsychotics in children and adolescents aged ≤18 years, reporting prolactin levels and related ARs. We conducted a random-effect meta-analysis and assessed risk of bias version 2 (ROB2).
Results:
Thirty-two randomized controlled trials with an average trial duration of 6 weeks, covering 4643 participants with an average age of 13 years and a male majority of 65.3%. Risk of bias across domains was low or unclear. The following antipsychotic compounds: aripiprazole (n = 810), asenapine (n = 506), lurasidone (n = 314), olanzapine (n = 179), paliperidone (n = 149), quetiapine (n = 381), risperidone (n = 609), and ziprasidone (n = 16) were compared with placebo (n = 1658). Compared with placebo, statistically significant higher prolactin increase occurred with risperidone (mean difference [MD] = 28.24 ng/mL), paliperidone (20.98 ng/mL), and olanzapine (11.34 ng/mL). Aripiprazole significantly decreased prolactin (MD = −4.91 ng/mL), whereas quetiapine, lurasidone, and asenapine were not associated with significantly different prolactin levels than placebo. Our results on ziprasidone are based on a single study, making it insufficient to draw strong conclusions. On average, 20.8% of patients treated with antipsychotic developed levels of prolactin that were too high (hyperprolactinemia), whereas only 1.03% of patients reported prolactin-related ARs. Data were highly limited for long-term effects.
Conclusions:
In children and adolescents, risperidone, paliperidone, and olanzapine are associated with significant prolactin increase, whereas aripiprazole is associated with significant decrease. Despite the significant changes in prolactin level, few ARs were reported. Study protocol on PROSPERO: CRD42018116451.
Introduction
Hyperprolactinemia due to antipsychotic treatment is an adverse reaction (AR) related to dopamine-D2 antagonism in the anterior pituitary gland (Byerly et al, 2007; Haddad and Wieck, 2004; Meaney and O'Keane, 2002). Hyperprolactinemia is associated with clinical symptoms. Typical for females are menstrual disturbances and hirsutism, for males gynecomastia and oligospermia, whereas galactorrhea, infertility, acne, migraine, and sexual dysfunction occur with both genders (Bobes et al, 2003; Byerly et al, 2007; Galdiero et al, 2012; Gazerani, 2021; Haddad and Wieck, 2004; Meaney and O'Keane, 2002; Misra et al, 2004; Nakonezny et al, 2007). Longer term health consequences such as increased risk of reduced bone density, breast (and other forms of) cancer, and cardiovascular disease are suspected, based primarily on studies in adults (Calarge et al, 2013; De Hert et al, 2016; De Hert et al, 2014; Grigg et al, 2017; Johnston et al, 2018; Matalliotakis et al, 2019; Pottegard et al, 2018).
There appears to be both gender- and age-specific differences in prolactin concentrations.
Antipsychotic-induced hyperprolactinemia appears more common in females (up to 90%), compared with males (up to 70%), possibly due to estrogen-related increases in prolactin (Alfaro et al, 2002; Bushe et al, 2008; Smith et al, 2002). In children and adolescents, more substantial antipsychotic-related prolactin increases have been found compared with adults (Caccia et al, 2011; Correll and Carlson, 2006; Pagsberg et al, 2017b; Roke et al, 2009; Woods et al, 2002; Wudarsky et al, 1999). However, the possible short- and long-term implications of hyperprolactinemia in children and adolescents, including adverse effects on growth, pubertal development, and bone density, are understudied (Caccia et al, 2011; De Hert et al, 2016; Fideleff et al, 2009).
Normal pubertal development might be delayed by hyperprolactinemia-induced disturbance of gonadotropin-releasing hormone (GnRH release), and lowered concentrations of estrogen and testosterone may prevent attainment of peak bone mass, increasing the risk of osteopenia and osteoporosis later in life (Correll and Carlson, 2006; Davies et al, 2005; Ducharme and Collu, 1982; Emiliano and Fudge, 2004; Maranghi et al, 2013; Meaney and O'Keane, 2002; Mosekilde et al, 2013; Naidoo et al, 2003; O'Keane and Meaney, 2005; Sambrook and Cooper, 2006). The existing evidence is inconclusive, for instance, a study found no delay in growth or pubertal development (Dunbar et al, 2004), whereas another study found prolactin to be inversely correlated with bone mass (Calarge et al, 2010).
Hypoprolactinemia due to antipsychotic treatment is related to partial dopamine-D2 agonists, by antipsychotics such as aripiprazole (Argo et al, 2004; Hoffer et al, 2009; Pagsberg et al, 2017a; Sogawa et al, 2016). The literature on antipsychotic-induced hypoprolactinemia is scarce. However, treatment with the D2-receptor agonist bromocriptine shows an association with hypoandrogenism, low sperm quality/count, erectile dysfunction, and infertility, and surgically induced hypoprolactinemia has been associated with delayed puberty and inability to lactate (Hargreaves and Harleman, 2011; Safer et al, 2013).
Since children and adolescents treated with antipsychotics are at risk for many years of exposure, and there is a suspected risk of severe ARs relating to pubertal development and growth, we conducted a meta-analysis exploring the following: Potential changes in serum/plasma prolactin concentrations in children and adolescents treated with antipsychotics versus placebo. Associations between potential changes in prolactin concentrations and somatic ARs.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al, 2021) was followed. Before conducting the meta-analysis, a protocol was registered in PROSPERO: CRD42018116451 (
Eligibility criteria
The included studies had to meet the following criteria:
Inclusion criteria: (1) double-blinded, randomized controlled trials (RCTs); (2) children and adolescents aged ≤18 years; (3) antipsychotic treatment listed in the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) Classification System versus placebo; (4) data on prolactin concentration change reported.
Exclusion criteria: (1) articles in non-English languages; (2) no online abstract; (3) placebo-controlled withdrawal studies; (4) no data for separate treatment arms; (5) crossover studies with no data available from the first period (to eliminate potential carryover effects); (6) conference abstracts or posters.
Information sources and search strategy
The search was conducted in PubMed and Cochrane Central Register of Controlled Trials (CENTRAL), which obtains results from other databases. We searched from database inception to 14/07/2021, using different combinations of the terms “Antipsychotic,” “Children and Adolescents,” and “Randomized Controlled Trial” (for full search strategy, refer Appendix 1). Reference lists from studies included in the meta-analysis and systematic review reports on the same topic were examined for further studies.
Selection process
Covidence systematic review software was used for duplication identification and exclusion. Articles not meeting the inclusion criteria based on title and abstract screening were excluded by one reviewer (S.M.K.). Remaining articles were reviewed in full text by two reviewers independently (S.M.K. and A.K.P.). Disagreements were resolved by involving a third reviewer (S.T.).
Data collection process
Two reviewers (S.M.K. and S.T.) independently extracted data. Inconsistencies were resolved by discussion or involvement of a third reviewer (A.K.P.).
Data items
Data extracted from each included study when available:
Study: Authors, publication year, number of patients, study design, intervention duration, blinding methods (single-blinded or double-blinded). Patients: Mean age, age range, gender distribution. Interventions: Antipsychotic drug, indication, mean dose, dose range, concomitant medication. Outcomes: Mean prolactin concentrations measured at baseline and end point (standard deviation [SD]), mean change in prolactin concentrations from baseline to end point (SD), incidence of study defined hypo- or hyperprolactinemia, and ARs related to changes in prolactin including galactorrhea, gynecomastia, menstrual disturbances, sexual dysfunction, changes in bone composition, delay or disturbance of pubertal development, and/or growth.
When multiple follow-up data were reported, data from the follow-up point nearest to the average follow-up point of the remaining studies were used to achieve comparability. When the number of participants with prolactin information was not available, the number of participants treated at baseline was extracted as default. All average values across studies with regard to age, male percentage, and the frequency of hypo- and hyperprolactinemia were weighted according to the number of participants (weighted average [WA]).
In the literature, different reference ranges are applied for determining hypo- and hyperprolactinemia. When individual patient data were not available, the study-defined thresholds for hyperprolactinemia and hypoprolactinemia were used. Both serum and plasma are used for prolactin assays. No differentiation between plasma and serum prolactin was made since the difference between values is negligible and should not affect the overall outcome (L. Bathum, Chief Physician at Department of Clinical Biochemistry, PhD, Cand.Med, personal communication). All reported blood–prolactin concentrations are referred to as prolactin concentrations.
Study risk of bias assessment
Risk of bias was assessed using the Cochrane Collaboration tool for risk of bias, version 2 (RoB 2) (Sterne et al, 2019), in which risk of bias in five domains are evaluated: randomization process, deviations from intended interventions, missing outcome data, measurements of the outcome, and selection of the reported results. Three reviewers (S.M.K., S.T., and L.C.) individually performed the risk of bias assessment. Disagreements were resolved by discussion.
Effect measures and synthesis methods
We analyzed the results as mean differences (MD) and standardized mean differences (SMD) in prolactin with 95% confidence interval (CI) between antipsychotics and placebo with conventional pairwise meta-analysis. We used MD as our primary measure as all trials reported prolactin using the same scale. All active trial arms (of the same antipsychotic) within each study were combined. Treatment arms of subtherapeutic doses were excluded (e.g., paliperidone 1.5 mg/day). The meta-analysis was performed by applying random-effect models by default to accommodate the anticipated heterogeneity among study results.
MDs in prolactin concentrations were compared among antipsychotics (i.e., subgroups), and between males and females using a test for subgroup differences (i.e., applying the standard Q-test statistic). When both change and end point data were available, end point data were used, unless baseline data were skewed (p > 0.05), in which case we used change data. This was performed to avoid group differences at baseline as a confounding variable. Studies reported prolactin measurements in ng/mL (μg/L). If SDs were missing, we derived it using the reported p-value or used the WA of the SDs of the other studies with the same antipsychotic, as suggested by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al, 2022). All data were entered into Review Manager V5.3, provided by the Cochrane Collaboration. We reviewed forest plots and analyzed heterogeneity of the data using the Cochran Q-test and interpreted these via the I 2 index for inconsistency, that is, the percentage of variance in the meta-analysis that is attributable to study heterogeneity.
In addition, we calculated the frequencies of hyperprolactinemia, hypoprolactinemia, and prolactin-related ARs.
Results
Study selection
For detailed study selection, see flow diagram (Fig. 1).
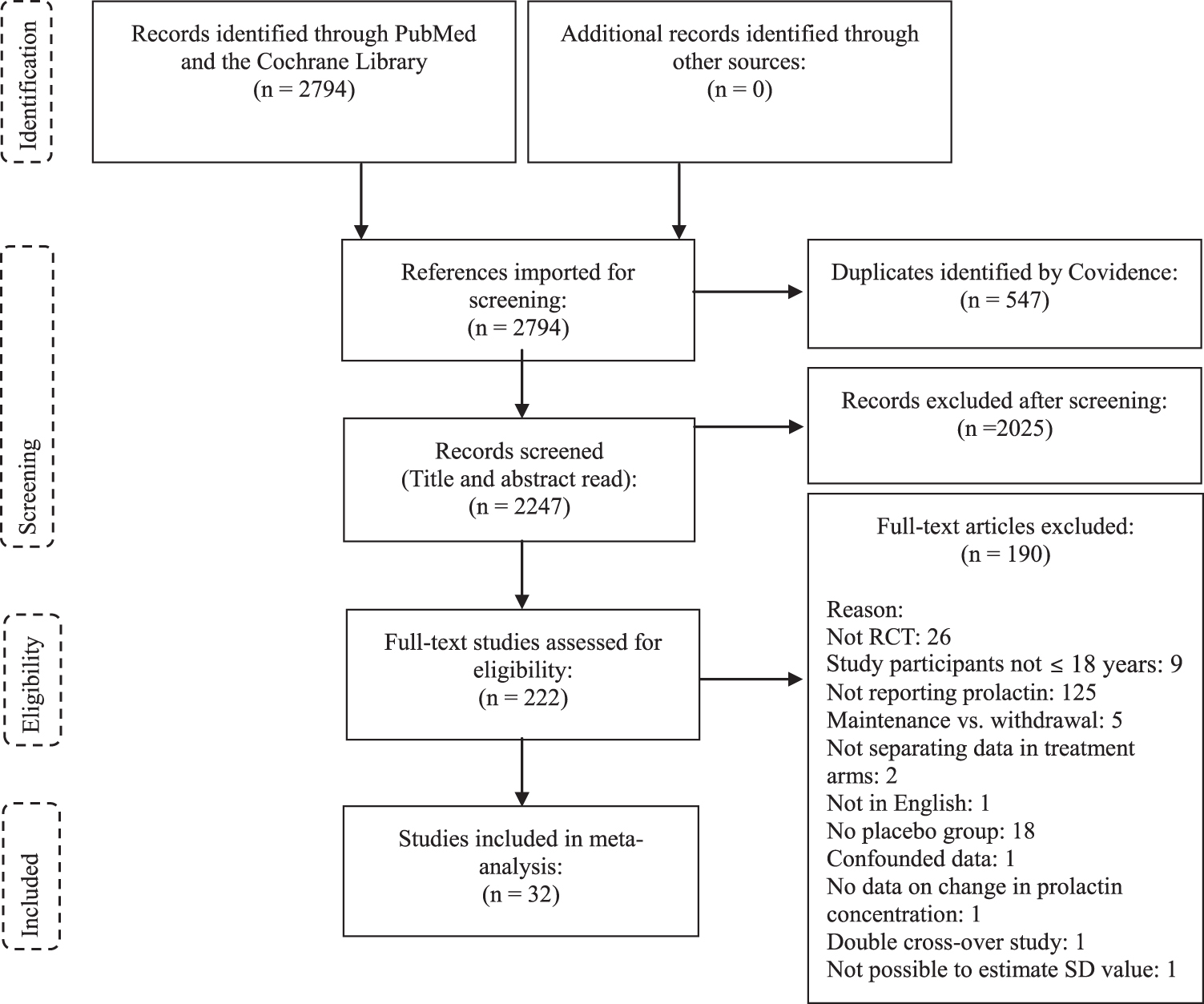
Flow diagram.
Study, participant, and treatment characteristics
The selected 32 studies (Table 1) eligible for meta-analysis of prolactin concentrations (n = 4643) were double-blinded, placebo-controlled trials with an intervention period of 3–26 (WA = 6) weeks, with only 2 placebo-controlled studies lasting 10 weeks or longer (Findling et al, 2017b; Yoo et al, 2013). The age range was 2.5–18 (WA = 13) years, and the male percentage was between 31% and 90% (WA = 65.3%). Interventions included risperidone, aripiprazole, quetiapine, lurasidone, asenapine, olanzapine, paliperidone, and ziprasidone. Ten studies presented data separately for males and females (Table 1). Twenty-eight studies (87.5%) were industry sponsored, and the remaining four studies were not (Aman et al, 2014; Anderson et al, 2007; Jahangard et al, 2017; Kowatch et al, 2015).
Study Characteristics of the 32 Studies Included in the Meta-Analysis of Antipsychotic-Induced Hypo- and Hyperprolactinemia in Children and Adolescents
Number of participants in the group at randomization, blood samples might not have been collected from all participants at baseline and end point.
The studies used different reference ranges for estimating the frequency of prolactin above upper limits. Only data presented by the studies as above upper limits or below lower limits based on their reference ranges were included.
Participants receiving valproic acid were not included in the analysis.
Standard deviations are estimated from the standard errors reported in the study.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorders; BD I, bipolar disorder I; BP-NOS, bipolar disorder not otherwise specified; CD, conduct disorder; CTD, chronic motor or vocal tic disorder; CYC, cyclothymic disorder; DBD, disruptive behavior disorder; f, female; m, male; n = number of patients; na, not available; ODD, oppositional defiant disorder; S-IQ, subaverage Intelligence Quotient (IQ = 36–84); SD, standard deviation, SZ, schizophrenia; TS, Tourette's syndrome; —, data were not reported in the study.
Only one study had prolactin as the main area of interest (Anderson et al, 2007), whereas the remaining measured prolactin as part of secondary safety assessments. Eleven studies evaluated risperidone (n drug = 609/n placebo = 483), 8 aripiprazole (n = 810/451), 5 quetiapine (n = 381/206), 2 lurasidone (n = 314/163), 2 asenapine (n = 506/203), 2 olanzapine (n = 179/89), 1 ziprasidone (n = 16/12), and 1 paliperidone (n = 149/51) (Table 1). In two studies, risperidone was used as an add-on to psychostimulant treatment (Aman et al, 2014; Jahangard et al, 2017), and in one study, quetiapine was used as add-on to divalproex (Delbello et al, 2002). Indications included are as follows: bipolar spectrum disorders, schizophrenia, autism spectrum disorder, tic disorders, and disruptive behavior disorders. Subaverage IQ was a comorbidity in some patients with disruptive behavior disorders or autism spectrum disorders (Table 1).
Thirty-one studies allowed concomitant medication, whereas the remaining study included only medication-free subjects (Anderson et al, 2007). Thirty-one studies excluded the use of other antipsychotics, and the remaining study was unclear (Jahangard et al, 2017). Twenty-five studies had a washout period before the trial, and the remaining studies were unclear (Aman et al, 2002; Buitelaar et al, 2001; Goldman et al, 2017; Jahangard et al, 2017; Loebel et al, 2016; Luby et al, 2006; Snyder et al, 2002). Antidepressants were allowed in two studies (DelBello et al, 2009; Findling et al, 2012) and were unclear in seven studies (Aman et al, 2014; Buitelaar et al, 2001; Jahangard et al, 2017; Luby et al, 2006; Snyder et al, 2002; Tohen et al, 2007; Yoo et al, 2013) and not allowed in the remaining studies. (Although Neuroscience-based nomenclature is preferred, we used the term antidepressants since this was most widely used in the included studies.)
Risk of bias
Risk of bias across domains was low or unclear. (For further details, refer Figs. 2 and 3).

Forest plot of the 32 studies included in the meta-analysis on mean change in prolactin levels (antipsychotic versus placebo), reported using mean difference. CI, confidence interval; SD, standard deviation.

Summary of risk of bias in the 32 studies, assessed using the Cochrane Collaborations tool for risk of bias, version 2 (RoB 2).
Prolactin concentrations
Antipsychotics (n = 2964) as a group were associated with significantly higher prolactin concentrations versus placebo (n = 1658) (MD = 10.10 ng/mL, 95% CI = 6.97–13.23) (Fig. 2 and Table 2). However, significant differences among individual antipsychotics were found (test for subgroup differences: p < 0.001). Risperidone, paliperidone, and olanzapine were associated with significantly higher prolactin concentrations than placebo. Risperidone showed the largest difference from placebo (MD = 28.24 ng/mL), with significant heterogeneity among studies (I 2 = 94% [MD]), followed by paliperidone (20.98 ng/mL) and olanzapine (11.34 ng/mL). Aripiprazole was significantly associated with decreased prolactin (MD = −4.91 ng/mL), whereas quetiapine, lurasidone, asenapine, and ziprasidone were not associated with significantly different prolactin concentrations than placebo (Fig. 2 and Table 2).
Summarized Data on the Effect of Different Antipsychotics on Mean Change in Prolactin Level, Frequency of Hypo- and Hyperprolactinemia, and Adverse Reactions in the Included 32 Randomized Controlled Trials
The studies used different reference ranges for estimating the frequency of prolactin above upper limits. Data presented by the studies as above upper limits or below lower limits based on their reference ranges were used to calculate the weighted average.
CI, confidence interval; MD, mean difference; WA, weighted average; —, insufficient data available for analysis.
A test for subgroup differences was performed for each of the antipsychotics with gender-segregated data. Although all crude changes in prolactin concentrations were higher for females than for males, this difference was only significant for quetiapine (males vs. females): aripiprazole (MD = −3.63 ng/mL, 95% CI = −5.47 to −1.80 vs. MD = −4.68 ng/mL, 95% CI = −13.34 to 3.97, p = 0.82), lurasidone (MD = 0.32 ng/mL, 95% CI = −0.73 to 1.37 vs. MD = 7.12 ng/mL, 95% CI = −2.45 to 16.69, p = 0.17), olanzapine (MD = 10.84 ng/mL, 95% CI = 8.16 to 13.52 vs. MD = 12.71 ng/mL, 95% CI = 7.69 to 17.73, p = 0.52), quetiapine (MD = 0.01 ng/mL, 95% CI = −5.79 to 5.81 vs. MD = 20.73 ng/mL, 95% CI = 5.18 to 36.28, p = 0.01), risperidone (MD = 26.44 ng/mL, 95% CI = 17.20 to 35.67 vs. MD = 36.73 ng/mL, 95% CI = 11.93 to 61.53, p = 0.45). We therefore combined male and female data for all antipsychotics in the analysis.
Dose dependence
Fourteen studies included more than one active arm with different doses of antipsychotics (k = 3, risperidone; k = 4, aripiprazole; k = 2, lurasidone; k = 2, asenapine; k = 2, quetiapine; k = 1, paliperidone); however, few reported on prolactin changes related to dose. Two of the studies on risperidone reported a dose-dependent increase in prolactin concentrations (Haas et al, 2009a; Haas et al, 2009b); however, results were insignificant. No significant dose dependence was found in a study on aripiprazole (Findling et al, 2008). A study on lurasidone found increased effects on prolactin with 60 mg/day, whereas treatment with 20 mg/day was generally similar to placebo (Loebel et al, 2016). The two studies on asenapine found no dose dependence (Findling et al, 2015a; Findling et al, 2015b).
Hyper- and hypoprolactinemia
Fourteen studies, including aripiprazole, asenapine, olanzapine, quetiapine, risperidone, and ziprasidone, reported the frequency of hyperprolactinemia (Tables 1 and 2), and three studies reported the frequency of hypoprolactinemia, two on aripiprazole, and one on asenapine (Tables 1 and 2). Despite differences in study-defined thresholds of hypo- and hyperprolactinemia, there was reasonable consensus of a lower threshold of 0.0–3.2 ng/mL for females and 0.0–2.8 ng/mL for males, and an upper threshold of 20–39 ng/mL for females and 11–24 ng/mL in males. The overall WA of hyperprolactinemia was 20.8%, the frequency was highest with olanzapine WA = 59.5% (range: 25.7%–81.0%), followed by ziprasidone: 31.3% (based on only one study), risperidone WA = 29.46% (range: 0.0%–68.0%), asenapine WA = 16.8% (range: 11.1%–23.0%), quetiapine WA = 11.6% (range: 2.5%–47.0%), and aripiprazole WA = 0.53% (range 0.0%–2.4%).
With placebo, the WA proportion of hyperprolactinemia was 6.5% (0.0%–60.0%). One study defined and reported pathological prolactin concentrations above a threshold of 100 ng/mL (Haas et al, 2009a) (i.e., three to four times higher than the defined thresholds for hyperprolactinemia in the other studies) and found hyperprolactinemia in 0%–5% of males and 23.8%–36.4% of females treated with risperidone, compared with 0% of males and females treated with placebo.
Two studies investigated gender-segregated data for hyperprolactinemia. A study on risperidone reported more cases of hyperprolactinemia in females compared with males (WA = 30.7% vs. WA = 2.8%) (Haas et al, 2009a), whereas an olanzapine study reported more cases in males compared with females (WA = 62.5% vs. WA = 25.7%) (Tohen et al, 2007).
The studies reporting proportions of hypoprolactinemia found a total WA of 20.2%. WA of 31.4% (range: 9.5%–45.5%) with aripiprazole and WA = 5.3% (range: 3.5%–6.7%) with asenapine (based on only one study), compared with WA = 5.1% (range: 0.0%–8.0%) with placebo.
One study investigated gender-segregated data for hypoprolactinemia and found more cases of hypoprolactinemia in males compared with females (WA = 42.8% vs. WA = 21.5%).
Prolactin-related ARs
Thirteen studies (participants n = 1719) covering five different antipsychotics reported on possible prolactin-related ARs (Table 1). AR were reported from 1.2% (n = 6/512) of the patients receiving risperidone, consisting of galactorrhea (n = 4), oligomenorrhea (n = 1), and ejaculation disorder (n = 1); 2.0% (n = 3/149) of the patients receiving paliperidone, consisting of galactorrhea (n = 2) and amenorrhea (n = 1); 6.25% (n = 1/16) of the patients receiving ziprasidone, consisting of mild gynecomastia (n = 1); 0.51% (n = 1/197) of the patients receiving aripiprazole, consisting of dysmenorrhea (n = 1), and finally, none of the participants receiving quetiapine reported prolactin-related ARs (Table 2).
In total, 1.03% (11/1067) of the patients receiving antipsychotic treatment reported prolactin-related ARs. With regard to placebo, 0.32% (n = 2/631) of these patients reported prolactin-related ARs, consisting of dysmenorrhea (n = 1) and breast enlargement and breast pain (n = 1). In total, 0.77% (13 of the 1698 participants) of all patients reported prolactin-related ARs. In 7 of the 13 studies (6 on risperidone and 1 on quetiapine), no possible prolactin-related ARs were reported.
Discussion
This meta-analysis is the first to specifically study changes in prolactin concentration and associated prolactin-related ARs, in children and adolescents treated with antipsychotics. It includes 32 placebo-controlled RCTs covering data from 4622 patients ≤aged 18 years, of whom 2964 were treated with antipsychotics.
Despite high mean increases in prolactin and the high prevalence of hyperprolactinemia for some antipsychotics, only few patients with clinical prolactin-related ARs were identified. The reported ARs consisted of galactorrhea, gynecomastia, and menstrual disturbances, ARs that are expected to normalize, once the treatment with antipsychotics ends and prolactin normalizes. Nevertheless, these ARs should be taken seriously since there could be secondary consequences for the patient such as bullying and low self-esteem. However, the number of reported ARs was too scarce to make meaningful comparisons between individual antipsychotics. The studies provided no data on prolactin-related effects on growth, bone mineral density, or pubertal development.
The disconnect between a low prevalence of prolactin-related ARs and elevated prolactin concentrations and hyperprolactinemia could be due to underreporting of ARs, elevated prolactin concentrations not being sufficiently high to disrupt the gonadal axis, or, in contrast to expectations, that prolactin concentrations are only moderately associated with sexual and reproductive dysfunction. The reported clinical ARs were all related to sexual and reproductive functioning, and unsolicited patient reporting of personally sensitive ARs might be challenged by patients not feeling comfortable bringing up symptoms spontaneously, or not having realized that the symptoms could be related to the antipsychotic treatment since the ARs might be difficult to differentiate from normal pubertal development (Abdelmoty et al, 2015; Santen and Mansel, 2005).
Overall, our findings are in line with previous reports on antipsychotic-induced changes in prolactin in youth (Almandil et al, 2013; Balijepalli et al, 2018; Druyts et al, 2016; Fraguas et al, 2011; Krause et al, 2018; Pagsberg et al, 2017b; Pringsheim et al, 2011a; Roke et al, 2009). Almandil et al (2013), Pringsheim et al (2011a), and Roke et al (2009) reported significant increases in prolactin concentrations with risperidone and olanzapine compared with placebo. However, the increase in the mean prolactin concentration with risperidone compared with placebo is higher in the present meta-analysis (MD = 28.25 ng/mL, 95% CI = 21.14–35.36, p < 0.01) than in the meta-analysis by Pringsheim et al (2011a) (MD = 20.70 ng/mL, 95% CI = 16.78–24.62, p < 0.01).
Furthermore, Fraguas et al (2011) reported the highest increase in prolactin concentrations with risperidone, and the second highest with olanzapine, which converges with our results. “The heterogeneity across studies is high (95%), this is due to high heterogeneity within the risperidone studies (94%), which, unfortunately, we cannot explain. However the focus is primarily on subgroup analysis and not antipsychotics as a group, thus the high heterogeneity is not a concern when discussing the remaining antipsychotics. Furthermore, even though the heterogeneity is high with risperidone, an increase in prolactin concentration with antipsychotic treatment was seen in all the risperidone studies.” Almandil et al (2013) and Pringsheim et al (2011a) reported a significant decrease in the mean prolactin concentrations with aripiprazole compared with placebo (MD = −5.03 ng/mL, 95% CI = −7.80 to −2.26, p < 0.01), which was similar to our findings (MD = −4.70 ng/mL, 95% CI = −6.40 to −3.01, p < 0.01).
Similar to our conclusions, no differences compared with placebo were found for quetiapine and ziprasidone in the reviews by Fraguas et al (2011) and Pringsheim et al (2011a). However, our results on ziprasidone are based on only a single study (Sallee et al, 2000) and are therefore not possible to conclude upon. Furthermore, despite finding no significant group differences in prolactin concentration, 30% of the ziprasidone group had elevated prolactin concentrations. Nevertheless, similar to the included ziprasidone study, an open label study found that ziprasidone was not associated with an increased prolactin concentration (Malone et al, 2007).
A descriptive review by Roke et al (2009) covered 29 small, open-label observational or double-blinded studies (n = 1786) published 1965–2008 including clozapine, haloperidol, olanzapine, pimozide, quetiapine, risperidone, and ziprasidone and is the only other study to report the proportion of antipsychotic-induced hyperprolactinemia and related ARs across different studies and antipsychotics in youth. We found similar proportions of hyperprolactinemia for quetiapine (11.6% vs. 12%) but lower (36.6% vs. 62%) for risperidone and higher (60.5% vs. 31%) for olanzapine. We found a lower proportion of prolactin-related ARs (1.2% vs. 5.1%) for risperidone. We cannot directly compare our results on mean change in prolactin concentration with the study by Roke et al since they reported prolactin concentrations descriptively.
Previous studies have found antipsychotic changes in prolactin concentrations to be greater in females versus males (Alfaro et al, 2002; Smith et al, 2002). We found that for quetiapine, a single study showed discrete changes that might have been invalidated by a short washout period.
Some studies have raised concerns, that during maturation, a higher density of dopamine D2 receptors in the central nervous system might make youth more prone to hyperprolactinemia than adults (Caccia et al, 2011; Woods et al, 2002; Wudarsky et al, 1999). Our findings support this hypothesis, as we found a greater increase in prolactin concentrations in youth for risperidone, olanzapine, and quetiapine, and a greater decrease for aripiprazole compared with the findings in adults with schizophrenia in a meta-analysis by Leucht et al (2013) (We converted our results to SMD to compare them with Leucht et al). For asenapine, lurasidone, paliperidone, and ziprasidone, the increase appeared greater in adults. However, our findings were not limited to patients with schizophrenia but covered a broad range of child and adolescent mental disorders, making the comparison less unassailable.
The main strengths of our study are the large sample size, the use of RCTs, all with low or unclear risk of bias, and the focus on antipsychotic effect on prolactin concentration and related ARs in youth ≤18 years without diagnostic restrictions of the participants. It is the first meta-analysis to compare prolactin data from aripiprazole, asenapine, lurasidone, olanzapine, paliperidone, quetiapine, risperidone, and ziprasidone.
The generalizability of certain conclusions are limited by the lack of systematic reporting of data on hypo- and hyperprolactinemia, prolactin-related ARs, gender and dose dependency (Masi et al, 2001; Molitch, 2005; Smith et al, 2002), and the general short duration of the studies. Several studies were excluded since they did not report results on prolactin, indication reporting bias. Few of the studies were conducted before the mid-1970s when the association between antipsychotics and prolactin had become common knowledge. Furthermore, we cannot rule out the risk of publication bias. In addition, we were unable to estimate the frequency of hypo-and hyperprolactinemia with several antipsychotics since 15 of the 32 included studies did not report this outcome, and the remaining studies used different thresholds.
In this study, we examined both potential changes in serum/plasma prolactin concentrations and associated ARs related to antipsychotic use. Changes in serum/plasma prolactin is an objective outcome, and we could have strengthened the power of the study of this outcome by including nonblind studies as others have done (Huhn et al, 2020), therefore not including such data in the meta-analysis of serum/plasma prolactin is a limitation. We included only RCTs, to have the same basis of comparison for our assessment of ARs, a subjective outcome, associated with greater risk of bias, meeting the need of only including RCTs. Furthermore, we failed to include Embase in the literature search as recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al, 2022). However, we subsequently cross-referenced all included studies and found no additional studies meeting inclusion criteria.
Another limitation is the scarce access to data on long-term prolactin-related ARs. Long-term ARs could be severe and include disturbances in pubertal development, bone mineral density, and growth, as observed in youth with prolactinomas (Colao and Loche, 2010; Colao et al, 2000; Di Somma et al, 1998; Fideleff et al, 2000; Saranac et al, 2010). However, prolactin concentrations seen with prolactinomas are higher (>200–250 ng/mL) (Ali et al, 2010; Schlechte, 2003) than with antipsychotic treatment (20–200 ng/mL), and extension studies on risperidone, providing data up to week 52 to 55, indicate that prolactin concentrations peak early and then decrease continuously to values within or close to normal range (Findling et al, 2017a; Findling et al, 2003; Kent et al, 2013a).
The included studies used different washout periods for patients already treated with antipsychotics, which could account for part of the variation between studies. Few studies reported whether blood samples were taken in a standardized manner: time, fasting status, and menstrual status, and whether the same laboratory was used.
To ensure comparability, in studies with multiple follow-up data, we used data from the follow-up nearest to the average follow-up point of the remaining studies (WA = 6 weeks). Data assessed at a time point of around 6 weeks treatment in the studies are probably a valid choice, as long-term studies find that the change in prolactin concentration from baseline peaks between week 3 and 6 (Aman et al, 2014; Findling et al, 2017a; Findling et al, 2016; Findling et al, 2015a; Findling et al, 2013; Findling et al, 2009; Kent et al, 2013a; Kent et al, 2013b; Snyder et al, 2002; Turgay et al, 2002).
Finally, our review on dose dependence might be limited by the lack of information related to pharmacogenetics, for example, how the individual patient metabolizes the antipsychotic drug, depending on the patients CYP2D6-phenotype. If the antipsychotic is metabolized too quickly, it may decrease the drug's efficacy, and if metabolized too slowly, might lead to an increased risk of ARs (de Leon et al, 2005).
Conclusions
In conclusion, this large meta-analysis including 4622 participants investigated prolactin concentrations and prolactin-related ARs reported in placebo-controlled RCTs in children and adolescents receiving any antipsychotic treatment. It is the first meta-analysis focusing specifically on prolactin while covering patients aged <18 years with any mental disorder treated with antipsychotics.
Risperidone induced the highest increase in the mean prolactin concentration compared with placebo, followed by paliperidone and olanzapine. Aripiprazole was associated with a significant decrease in the mean prolactin concentrations, and no significant differences were found for asenapine, lurasidone, and quetiapine. Our results on ziprasidone are based on a single study, making it insufficient to draw strong conclusions. Compared with studies in adults, differences in prolactin concentrations appeared greater in children and adolescents for risperidone, olanzapine, quetiapine, and aripiprazole.
Olanzapine showed the highest frequency of hyperprolactinemia, followed by risperidone, whereas data were not reported for paliperidone. Aripiprazole and asenapine were the sole antipsychotics investigated with respect to hypoprolactinemia. Despite significant changes in prolactin concentrations and high rates of hyperprolactinemia, prolactin-related ARs were rare and mainly demonstrated in participants treated with risperidone and paliperidone. Sufficient data were not available to draw conclusions concerning long-term effects on pubertal development, growth, or bone mineral density.
Future studies examining long-term prolactin changes, dose dependency, gender effects, and the possible related clinical ARs including effects on pubertal development, growth, and bone mineral density are needed. Special attention should be paid to systematically monitoring ARs in children and adolescents in both trials and clinic since relying on self-reporting increases the risk of underreporting, due to the sensitive nature of ARs related to pubertal development.
Clinical Significance
Hypo- and hyperprolactinemia in youth treated with antipsychotics occur frequently, but the prevalence and severity of long-term ARs are underinvestigated. Currently, the CAMESA guidelines (Pringsheim et al, 2011b) provide recommendations for monitoring prolactin concentrations, based on a systematic review including results for prolactin concentrations on risperidone, olanzapine, quetiapine, aripiprazole, clozapine, and ziprasidone. The recommendations include monitoring prolactin at baseline, after 3 months of treatment with risperidone or olanzapine, and after 6 months with ziprasidone and, if normal, on a yearly basis thereafter in asymptomatic children. When the patient is displaying clinical symptoms of hyperprolactinemia, they recommend more frequent monitoring. Recommendations for ziprasidone were, given the paucity of both short- and long-term data, based on consensus rather than evidence. Furthermore, the guideline emphasizes that prolactin concentrations should be determined after fasting with scheduled blood work.
The National Institute for Health and Care Excellence (NICE) guideline (Health, 2013) for psychosis and schizophrenia in children and young people recommends monitoring prolactin concentrations at baseline before initiation of an antipsychotic, at 12 weeks, and every 6 months thereafter. There are no specific recommendations for assessing prolactin-related clinical symptoms; however, side effects in general should be monitored regularly throughout treatment, and especially during titration. Furthermore, the management of hyper- and hypoprolactinemia is not stated.
A more recent Australian consensus guideline (Grigg et al, 2017) primarily concerning the use of antipsychotics in adults recommend a systematic monitoring of prolactin concentrations based on an algorithm. Moreover, the guideline recommends caution in the use of prolactin-increasing drugs in people aged <25 years. The guideline also provides suggestions for management of hyperprolactinemia.
While acknowledging the paucity of specific guidelines for the monitoring and management of antipsychotics-induced hyperprolactinemia, we suggest: (1) at baseline before initiation of antipsychotic treatment, monitor prolactin concentration (fasting) and systematically assess clinical prolactin-related symptoms (for females typically menstrual disturbances and hirsutism, for males gynecomastia and oligospermia, for both genders disturbed pubertal development and growth, galactorrhea, infertility, acne, migraine, and sexual dysfunction); (2) repeat this after 12 weeks and every 6 months thereafter if the child/adolescent is asymptomatic. If iatrogenic hyperprolactinemia occurs, consider monitoring sex hormones and monitor prolactin concentrations and clinical symptoms closer, depending on severity. Hyperprolactinemia may be transient.
The most obvious intervention if significant hyperprolactinemia and/or clinical symptoms occur is dose reduction or shifting the antipsychotic to a drug that is less prone to produce hyperprolactinemia, that is, aripiprazole, lurasidone, quetiapine, or asenapine. Another possibility, if a shift is undesirable, is to add sex hormone treatment (contraceptive pills/testosterone) or add a small dose of aripiprazole (Grigg et al, 2017). Hyperprolactinemia must be managed but should not hinder antipsychotic treatment since the consequences of an untreated mental disorder that requires pharmacological intervention may be grave.
Footnotes
Acknowledgments
Lise Bathum, MD, PhD, MHM, Department of Clinical Biochemistry, Amager and Hvidovre Hospital, Capital Region, Denmark, for her help on methodical differences between serum and plasma prolactin measures.
Authors' Contributions
S.M.K.: Conceptualization (supporting); writing—original draft (lead); formal analysis (equal); writing—review and editing (equal); methodology (equal). L.C.: Formal analysis (equal); writing—review and editing (equal); methodology (equal). S.T.: Formal analysis (equal); writing—review and editing (equal); methodology (equal). A.K.P.: Conceptualization (lead); writing—review and editing (equal); methodology (equal).
Disclosures
No competing financial interests exist.