
Abstract
Objective:
This study, with a case–control design, investigates the impact of attention-deficit/hyperactivity disorder (ADHD) comorbidity on the phenomenology and treatment outcomes in a clinical sample of pediatric obsessive-compulsive disorder (OCD).
Methods:
The data were derived from an evaluation of the sociodemographic and clinical characteristics of 364 children with OCD who were regularly followed up over a 4-year period. Between-group analyses of psychiatric scales were used to compare patients with ADHD comorbidity (n = 144, 39.5%) with their ADHD-free opponents. The clinical course and treatment outcomes of each patient were evaluated based on 4-year clinical follow-up data.
Results:
Substantial clinical variations in pediatric OCD caused by ADHD comorbidity were identified, including a male preponderance, higher rates of concurrent conduct problems, tic disorders, and learning disabilities, as well as prolonged symptom and treatment durations accompanied by poor response to first-line treatments and higher rates of treatment resistance. Contrary to previous findings, ADHD comorbidity had no impact on the age of OCD onset, and the severity of OCD symptoms was lower in ADHD. With ADHD comorbidity, the OCD symptom course tended to be chronically stable, which may have resulted in complaints persisting into adulthood. In ADHD-free patients, contamination, doubt, religious, somatic obsessions, and cleaning were all more common than in those with ADHD. There was a positive correlation between compulsion scores and the severity of ADHD symptoms, which may be related to increased compulsive coping in ADHD. Impulsivity or compulsivity dominance in the symptom presentation of OCD-ADHD comorbidity may determine phenomenological distinctions such as whether concurrent traits are more prone to tics, conduct problems, or internalizing problems. The primordial associations for clinical characteristics, which were independently associated with ADHD comorbidity, were adjusted using multivariate logistic regression analysis. Clinical variables such as being male, absence of cleaning compulsion, the existence of concurrent conduct problems, tic disorders, and dyslexia, as well as longer treatment duration and poorer treatment response, were all independent predictors of ADHD comorbidity. With an 80.8% accurate classification and relatively fine goodness-of-fit model, the regression model consisting of those predictors had good predictiveness for ADHD comorbidity (R 2 = 0.543).
Conclusions:
The close association between pediatric OCD, ADHD, and tic disorders can be defined as a specific subtype of pediatric OCD, characterized by more conduct problems, a chronically stable course of OCD symptoms, and poorer treatment outcomes. Correlational analyses in a longitudinal design and the inclusion of an impulsivity scale would be beneficial for further research to interpret the impulsivity-related correlates in the findings on tic and conduct problems.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is the leading concomitant psychiatric condition in pediatric obsessive-compulsive disorder (OCD), however with quite conflicting findings on co-occurrence rates ranging between 0% and 60% (Abramovitch et al, 2015). ADHD and OCD are distinct psychiatric conditions lying at opposite ends of the impulsive–compulsive continuum. However, both exhibit common neuropsychological findings such as impulsivity, inattentiveness, and relevant executive dysfunctions, although they contradict their distinct pathophysiological and phenomenological underpinnings (Cabarkapa et al, 2019). There is substantial evidence concerning several overlapping features between ADHD and OCD, including a background of familial transmission/heritability (Geller et al, 2007a; Geller et al, 2007b), similar abnormalities in neuropsychological findings (Brem et al, 2014), and high comorbidity with tic disorders.
Despite the two disorders' opposing clinical and neurobiological profiles (e.g., opposing patterns of frontostriatal pathophysiology) (Rubia et al, 2011), patients with OCD and ADHD frequently exhibit similar neuropsychological profiles such as impaired working memory, planning, and response inhibition (Abramovitch et al, 2015; Abramovitch et al, 2013a; Chamberlain et al, 2005). However, the frontostriatal hypermetabolism observed in adult OCD cases was not demonstrated in child OCD patients, suggesting that pediatric OCD differs from that of adolescents and adults in terms of neurobiology (Abramovitch et al, 2012). Furthermore, given the evidence of inflated comorbidity rates of OCD and ADHD, hypotheses regarding a distinct familial subtype of either that is inherited together (Geller et al, 2007b), shares common genetic predisposing factors (Mathews and Grados, 2011), or is associated with similar dysfunctions in neurotransmitter pathways (Carlsson, 2001) appear plausible.
ADHD comorbidity has been linked to resistance to conventional treatments in OCD (Farrell et al, 2020; Sheppard et al, 2010), and treating one without the other results in a poor prognosis for both (Cabarkapa et al, 2019). Authors who reported specific clinical characteristics peculiar to OCD and ADHD concurrency proposed that ADHD comorbidity represents a distinct subtype of OCD (Blanco-Vieira et al, 2019; Çelebi et al, 2016; Mersin Kilic et al, 2016). Pediatric OCD with ADHD comorbidity has been associated with an episodic course, more prevalent religious and sexual obsessions, and higher comorbidities with bipolarity, social anxiety, and tic disorders (Çelebi et al, 2016). Furthermore, adult OCD patients with ADHD comorbidity had a significantly distinct symptom profile compared with ADHD-free cases, with an early-onset of OCD and a preponderance of impulsivity (Blanco-Vieira et al, 2019; Mersin Kilic et al, 2016).
In addition, Blanco-Vieira et al (2019) likewise emphasized in their study that pediatric patients with ADHD comorbidity were more likely to present with severe and early-onset OCD symptoms, exhibit increased academic difficulties and risk of suicidal attempts, and were more accompanied by sensory phenomena, as well as concurrent conditions such as acute rheumatic fever or Tourette syndrome (Blanco-Vieira et al, 2019). However, some authors have argued that inflated rates reported for OCD and ADHD comorbidity may be owing to misdiagnosis of conflicting symptoms, particularly those mediated by tic comorbidity (Abramovitch et al, 2013b). Furthermore, impaired neuronal maturation processes in pediatric OCD may cause a transient phenotypic expression resembling ADHD symptomatology (Perestrelo et al, 2017). Therefore, clinicians should also consider the possibility that ADHD-like symptoms caused by OCD-specific symptomatology may be misdiagnosed as ADHD, particularly in pediatric OCD (Abramovitch et al, 2015; Perestrelo et al, 2017).
The paucity of data on the influence of prevalent neurodevelopmental comorbidities on the phenomenology and treatment outcomes of pediatric OCD prompted us to examine the phenomenological differences and variation in treatment outcomes associated with ADHD comorbidity. We hereby investigated how ADHD comorbidity correlated with demographics and a variety of clinical characteristics such as other psychiatric comorbidities and treatment outcomes in a relatively large clinical sample consisting of pediatric OCD patients who were followed for clinical course and treatment outcomes on a regular basis for ∼4 years. The current findings can help clinicians gain clinical foresight into noteworthy issues to be considered in the clinical follow-up of pediatric OCD, particularly with prevalent neurodevelopmental psychopathologies, and may benefit clinicians in structuring effective treatment combinations on time and managing variable lifelong prognosis and clinical outcomes.
Materials and Methods
Sample and data collection
A cross-sectional study with a case–control design was conducted based on an evaluation of a sociodemographic and clinical database of 364 children and adolescents with OCD (aged between 8 and 18 years) who were regularly followed up in child and adolescent psychiatry outpatient clinics during the period from January 2018 to August 2021. The research protocol was approved by the local ethics committee (date: July 2, 2021, number of ethics committee: 2020-KAEK-141/180, and protocol number: E-21/06-174). The study was conducted in line with the Declaration of Helsinki. All participants and their parents/legal custodians provided written informed consent before beginning the study.
The inclusion criterion was mainly having a primary diagnosis of OCD at baseline psychiatric assessment, according to the psychiatric background and symptom ratings based on a structured clinical interview in line with “the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version, DSM-5 November 2016, Turkish Version” (K-SADS-PL-DSM-5-T). The OCD diagnosis of each participant was reviewed and confirmed if they met the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria for OCD and had a total score >16 on the Children's Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) at their first baseline diagnostic evaluation for OCD.
Participants with subthreshold OCD symptoms and a total CY-BOCS score of <16 were taken out of participation owing to failure in diagnostic confirmation (n = 2). The presence of ADHD comorbidity was confirmed primarily through clinical interviews based on K-SADS-PL-DSM-5-T and controlled by baseline total scores on Conner's 28-item Teacher Rating Scale (CTRS) both in the study group (OCD with ADHD group, n = 144) and control group (ADHD-free OCD group, n = 220). Exclusion criteria included declined participation and data unavailability owing to follow-up discontinuation, deficient file information, and/or missing diagnostic scales (see CONSORT-Flow Diagram; Fig. 1).
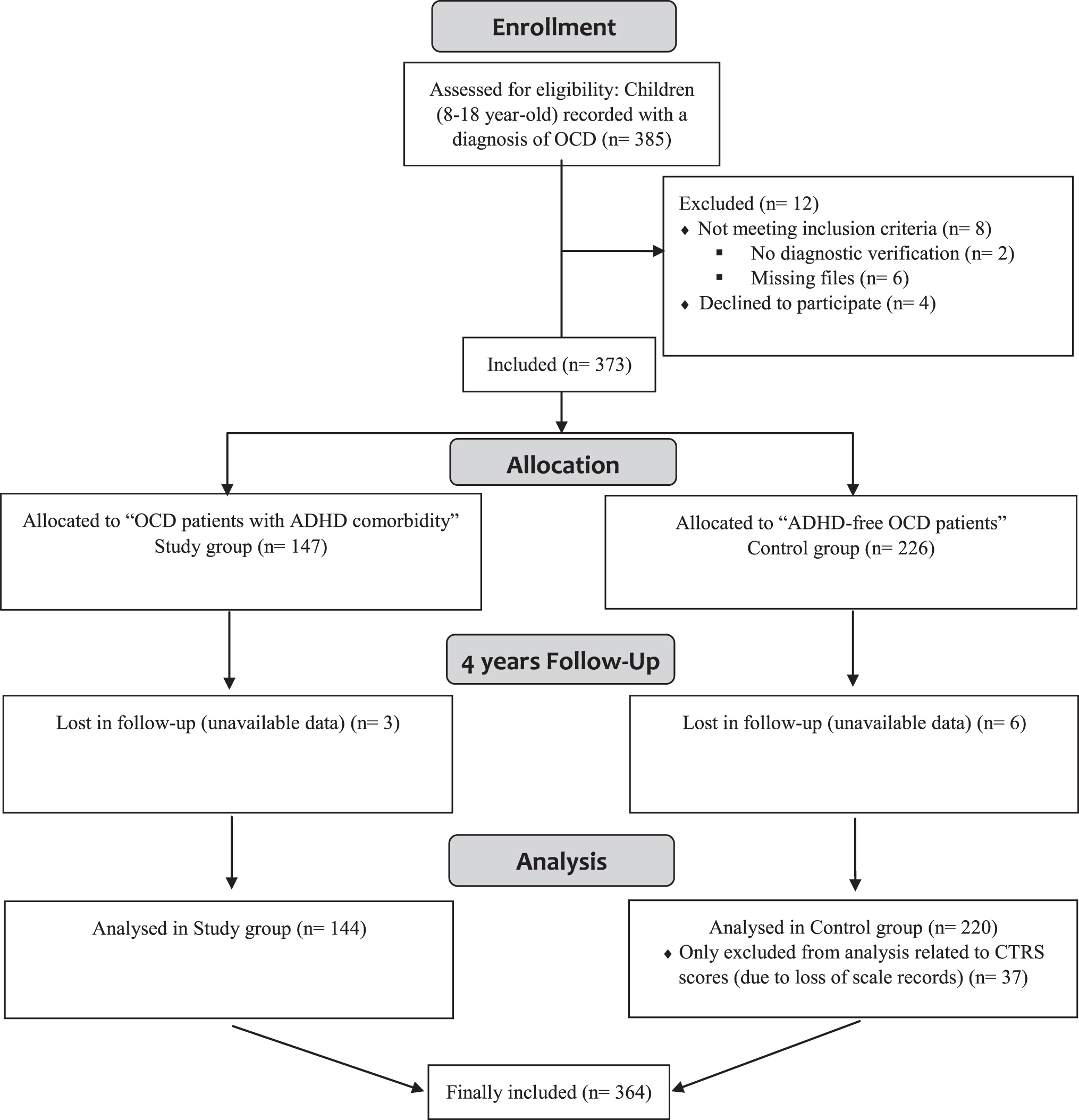
CONSORT—flow diagram.
Measures
The sociodemographic and clinical data were gathered by reviewing existing patients' files, administering relevant diagnostic scales, and conducting face-to-face structural interviews. The Hollingshead–Redlich Index was used to determine socioeconomic status (SES), which was simply divided into three categories: low, medium, and high levels of SES. At the first visit, the K-SADS-PL-DSM-5-T, Clinical Global Impression Scale-Severity Score (CGI-S), and Children's Global Assessment Scale Score (C-GAS) were used for diagnostic verification and assessment of current overall functioning. The phenomenology and symptom course were described using the CY-BOCS, a clinician-rated, criterion-standard dimensional measure of the severity and psychometric properties of OCD with a separate developmentally modified version (Storch et al, 2004).
CTRS, which consists of 28 items describing problem behaviors to be rated by the teacher on a 4-point Likert scale from “0: not at all present” to “3: very much present” (Conners et al, 1998), was used to determine the severity of behavioral symptoms associated with ADHD. Higher scores on CTRS indicate the intensity of symptoms typical for disruptive behavior disorders. A three-factor structure composed of “cognitive problems/inattention,” “hyperactivity,” and “conduct problems,” which was proposed in the reliability and validity of the Turkish version (Cronbach's alpha: 0.95) (Dereboy et al, 2007), was preferred for determining sub-dimensions of ADHD symptoms. In this study, the CTRS data records of 37 participants in the control group were missing. Therefore, the remaining CTRS data of 183 controls could be included in CTRS-related analyses.
In the field of psychiatry, subtyping OCD patients based on their clinical course is an important criterion in delineating pathology. Longitudinal follow-up studies on OCD, on the contrary, were scarce, and the majority were conducted through retrospective chart reviews. Despite the limitations of the available data, four OCD-course categories have been described in the literature and used to define the clinical course of OCD symptoms in this study (American Psychiatric Association, 2013; Rasmussen and Eisen, 1992). A symptom-free interval is defined as a CY-BOCS total score decrease of >50% from baseline. The least amount of time for a symptom-free interval definition is considered as the minimum asymptomatic period in complete remission (if the total score on CY-BOCS is <8 for >2 months), being confirmed by two subsequent assessments, insofar as the sample is not treated with any specific therapy and in the absence of any other indication.
First-line/conventional treatment options for pediatric patients with OCD include at least two adequate pharmacologic treatments of serotonin-reuptake inhibitors (SRIs) in consecutive use, one SRI in conjunction with an antipsychotic augmentation, or more than one OCD medication combined with an adequate trial of cognitive-behavioral therapy (CBT) (Jenike and Rauch, 1994). The participants were deemed adequately treated with pharmacotherapy if they had been taking a clinically effective dose of SRIs for at least 12 weeks or had been unable to tolerate the maximum dose on account of side effects (based on record review). The mean effective doses of SRIs established in double-blind trials in pediatric OCD patients were deemed sufficient for SRI-based pharmacotherapy (Geller et al, 2003; Varigonda et al, 2016).
The adequacy of the CBT trial was confirmed by the authors according to the definition of an adequate CBT trial, consisting of 20 hours of exposure-based psychotherapy in an individual setting (Lewin et al, 2005; Piacentini et al, 2002). A clinically significant improvement (remission: a total CY-BOCS score of <10) after an adequate CBT and/or SRI trial, as well as sustaining a minimum of 3 months of therapeutic gains, was considered treatment responsive. The partial (moderate) treatment response is defined as a 35% to 50% reduction in the CY-BOCS score after achieving the optimal tolerated dose of SRIs for a minimum of 10 weeks. Low treatment response/unresponsiveness is defined as having <35% symptom remission. And finally, treatment resistance is defined as an unsatisfactory response to first-line treatments even after administering augmentation therapies.
Data analysis
Data were analyzed using SPSS (version 22.0 for Windows; SPSS, Inc., Chicago, IL). Normality of distribution was determined with the Kolmogorov–Smirnov test. Descriptive analyses, which consisted of frequencies, percentages, means, and standard deviations, were used to evaluate the demographic and clinical characteristics of the whole sample. Pearson chi-square test (χ 2) or Fisher exact test (when expected frequencies were less than five per cell) was performed on categorical variables and a Mann–Whitney U-test (Z) or Kruskal–Wallis test on continuous variables to explore group differences. The nonparametric Spearman's rank correlation analyses were used to compute the degree to which the OCD clinical features were associated with the ADHD symptom presentation. The p-values were based on two-tailed tests with α = 0.05.
And finally, the bivariate analyses were followed by a multivariate logistic regression analysis to adjust the crude associations for clinical characteristics independently associated with ADHD comorbidity. Logistic regression models were built considering the presence of ADHD comorbidity as the dependent variable, as well as including all variables with a statistical significance (p < 0.05) in the univariate analyses (between-group analyses) as independent variables in the model. The procedure of the variable selection was performed following the backward method. The absence of multicollinearity between the independent variables was confirmed by the analyses, testing the variable inflation factors (VIFs) and tolerance. The independent variables that ensured the conditions of “VIF <10 and tolerance >0.1” were included in the regression model. The fit of the regression model was tested with Hosmer–Lemeshow goodness-of-fit statistics.
Results
Among participants with pediatric OCD (n = 364, mean age: 14.3 ± 2.7 years), 39.5% presented comorbidity with ADHD (n = 144), which was compared with others without ADHD comorbidity (ADHD-free group, n = 220) in terms of clinical features. The sociodemographic and clinical expletory variables of the entire sample, as well as relevant findings from between-group analyses, are summarized in Tables 1 –3. The most remarkable finding in the sociodemographic variables was the male preponderance among patients with ADHD comorbidity (p < 0.001).
Sociodemographic and Clinical Expletory Variables
Chi-square tests (χ 2) for comparison of groups. Values in parentheses indicate degrees of freedom (df).
p < 0.05 indicates statistical significance, which was demonstrated in bold.
ADHD, attention-deficit/hyperactivity disorder; CBT, cognitive-behavioral therapy; HRS, Hollingshead–Redlich Scale; n (%), number of the participants with frequencies in parentheses; OCD, obsessive-compulsive disorder; SES, socioeconomic status; SRIs, serotonin-reuptake inhibitors.
Comparison Among Subjects According to Attention-Deficit/Hyperactivity Disorder Comorbidity in Terms of Clinical Features
Descriptive results of the whole sample in the second column, OCD with ADHD group in the third column, and ADHD-free OCD group in the fourth column.
Data are presented as mean ± SD, or the number of clients along with frequencies. Mann–Whitney U (Z) and chi-square tests (χ 2) for comparison of groups. Values in parentheses indicate degrees of freedom (df).
ADHD, attention-deficient/hyperactivity disorder; CGI-S, Clinical Global Impression Scale-Severity Scores, C-GAS, Children's Global Assessment Scale; CTRS, Conner's Teacher Rating Scale; CY-BOCS, Childhood Yale-Brown Obsessive-Compulsive Scale; n (%), number of the participants along with the demonstration of frequency in parentheses; OCD, obsessive-compulsive disorder.
Comparison Among Subjects According to Attention-Deficit/Hyperactivity Disorder Comorbidity in Terms of Obsessive-Compulsive Disorder Symptoms and Comorbidities
Descriptive results of the entire sample in the second column, OCD with ADHD group in the third column, and ADHD-free OCD group in the fourth column.
Data presented as mean ± SD, or the number of clients along with frequencies. Mann–Whitney U (Z) and chi-square tests (χ 2) for comparison of groups. Values in parentheses indicate degrees of freedom (df).
p < 0.05 indicates statistical significance, which was demonstrated in bold.
ADHD, attention-deficit/hyperactivity disorder; n (%), number of the participants along with the demonstration of frequency in parentheses; OCD, obsessive-compulsive disorder.
The distribution of symptom courses was similar between groups; however, patients with ADHD comorbidity were more likely to present with a chronically stable course, whereas their opponents were more likely to present with an episodic or a chronic fluctuating course. Contamination, doubt, religious, and somatic obsessions, as well as cleaning compulsions, were significantly more prevalent in ADHD-free patients. A vast majority of the sample (86%) had at least one psychiatric comorbidity (including ADHD), 23.4% (n = 85) had a concomitant medical disorder, and 14.6% (n = 53) had a recurrent infection background. The groups differed in terms of psychiatric comorbidity (χ 2 = 38.82, df = 1, p ≤ 0.001), despite having a similar background in medical disorders (χ 2 = 3.49, df = 1, p = 0.062) and recurrent infections (χ 2 = 2.34, df = 1, p = 0.126). About half of the participants had a concomitant general anxiety disorder (GAD), and the participants with ADHD comorbidity were more likely to have concurrent oppositional defiant disorder (ODD), conduct disorder (CD), tic disorders, intellectual disability, and dyslexia compared with ADHD-free participants.
The distribution of OCD-clinical subtype and number of obsessions varied between the two groups, with a mixed subtype of OCD being the most prevalent in both. The symptom severity of OCD was strikingly higher in ADHD-free participants within the scope of severity indicators such as CY-BOCS total score and obsession subscore, whereas the CY-BOCS compulsion subscores were comparable between groups. Despite comparable global functioning (C-GAS) between the two groups, the global symptom severity (CGI-S) was found to be greater in the ADHD comorbid group; these findings were consistent with considerably higher CTRS scores in the ADHD comorbid group.
Total symptom and treatment durations were significantly elongated in patients with ADHD comorbidity. As expected, the groups differed in their use of antipsychotic drugs (χ 2 = 9.004, df = 1, p = 0.003) and ADHD medications. Furthermore, patients with ADHD comorbidity were more likely to exhibit resistance to first-line treatments (p < 0.001). In support of this, treatment responses tended to be lower in the ADHD comorbid group, but rather higher in the control group. Besides, statistical differences remained between groups stratified by ADHD comorbidity when cases of “unknown treatment response” were excluded from both groups, and treatment response was analyzed for other subcategories, including low (unresponsiveness), moderate (partial), and high (adequate) responses (χ 2 = 6.47, df = 2, p = 0.039).
The Spearman correlation analyses among the total and subcategorical scores of scales are given in Table 4 (bivariate analyses). The most important point here is the positive correlation being detected between the compulsion subscores of CY-BOCS and the hyperactivity, conduct problems, and other problems related to subscores, as well as the total scores of CTRS. In the logistic regression analyses (Table 5), by performing the backward method, the following characteristics remained significantly associated with ADHD comorbidity: gender (the first condition was determined to be male, whereas the reference condition as female) (odds ratio [OR] = 2.91, p < 0.001); cleaning/washing compulsion (OR = 0.33, p < 0.001); ODD (OR = 27.85, p < 0.001); CD (OR = 7.56, p = 0.078); tic disorder (OR = 3.25, p = 0.01); dyslexia (OR = 14.83, p < 0.001); treatment duration (OR = 1.07, p < 0.001); treatment response (the first condition was determined as having low response or to be unresponsive, whereas the reference condition as having treatment response in moderate, high, or unknown categories) (OR = 2.28, p = 0.029).
Spearman Correlation Between Attention-Deficit/Hyperactivity Disorder Symptoms Scores (Conner's Teacher Rating Scale) and the Childhood Yale-Brown Obsessive-Compulsive Disorder, Clinical Global Impression Scale-Severity Scores, and Children's Global Assessment Scale Scales
Bold values represent the statistically significant results.
Correlation is significant at the 0.01 level (two-tailed).
Correlation is significant at the 0.05 level (two-tailed).
C-GAS, Children's Global Assessment Scale; CGI-S, Clinical Global Impression Scale-Severity Scores; CTRS, Conner's Teacher Rating Scale; CY-BOCS, Childhood Yale-Brown Obsessive-Compulsive Scale; pr, problems; r, Spearman's rank correlation coefficient.
Regression Analysis of Clinical Characteristics Related to the Attention-Deficit/Hyperactivity Disorder Comorbidity
β, regression coefficient; CI, confidence interval; OR, odds ratio; SE, standard error.
Other variables were excluded because of high levels of multicollinearity. The regression-model fit was fairly well according to the Hosmer–Lemeshow goodness-of-fit statistics (p = 0.765). As a result of the logistic regression analysis, a model predicting ADHD comorbidity in pediatric OCD, which had adequate model data compatibility and a moderately good predictiveness (Nagelkerke R 2 = 0.543, Cox and Snell R 2 = 0.401), was developed with an 80.8% accurate classification.
Discussion
Comorbidity between OCD and ADHD has been debated for a couple of decades, with evidence indicating highly heterogeneous and inconsistent co-occurrence rates that also varied by developmental stage (such as 0%–60% in children, 2%–63% in adolescents, and 0%–22.9% in adults). Despite numerous studies pointing to OCD/ADHD comorbidity at different developmental stages, only a few studies have examined comorbidity exclusively in adolescent populations, and an etiological explanation for ADHD-OCD comorbidity, which was primarily genetic in nature, has been attempted only in the pediatric population (Abramovitch et al, 2015; de Mathis et al, 2013; Ivarsson et al, 2008). ADHD comorbidity was identified in ∼40% of the participants with pediatric OCD. However, all the participants were recruited from outpatient clinics, which might also account for the high ADHD prevalence in our sample.
High ADHD prevalence in pediatric OCD may be mediated by the existence of tic disorders, and evidence of impaired neuronal maturation processes in the pediatric population with OCD may lead to transitory phenotypic expressions that look like ADHD symptomatology. Thus, ADHD-like symptoms resulting from OCD-specific symptomatology may be misdiagnosed as ADHD in pediatric patients. This may explain the lower co-occurrence rates reported in adolescents and adults. On the contrary, not including patients with a childhood ADHD background, whose ADHD symptoms might have improved in parallel with neuro-maturation, may result in lower OCD-ADHD comorbidity. However, not including patients with a childhood ADHD background, whose ADHD symptoms might have improved in parallel with neuro-maturation, may result in lower OCD-ADHD comorbidity rates in adults.
From a different point of view, there is further evidence for the validation of a real ADHD-OCD comorbidity even after stabilizing the potential confounding variables such as gender and age (Park et al, 2011). Nevertheless, an inflated and extreme range of comorbidity rates, which casts doubt on the reality of co-occurrence, may be partially attributable to referral biases, whether the samples are drawn from specialized clinics or the general population. In addition, several methodological concerns (such as data acquisition, sample size, age range, recruitment sources, and inclusion criteria) have been identified in the literature as potential explanations for the aforementioned conflicting data on comorbidity rates or relevant phenomenological consequences, but not enough to rule out the reality of comorbidity. The requirement for further studies on OCD-ADHD comorbidity that attempt to mitigate these biases was particularly highlighted by previous data. In this regard, we aimed to contribute to the literature by investigating the impacts of ADHD comorbidity on clinical implications and treatment outcomes in a clinical pediatric sample with OCD, as well as by reviewing phenomenological and theoretical issues concerning co-occurring OCD and ADHD.
The most prominent findings of this study on the aforementioned phenomenological issues were as follows: the male preponderance; higher rates of other concurrent psychiatric conditions such as ODD, CD, tic disorders, intellectual disability, and dyslexia; and elongated symptom and treatment durations, with higher rates of treatment resistance and likely lower or moderate responses to first-line conventional treatments in patients with ADHD comorbidity compared with their ADHD-free opponents. The majority of our findings affirm the earlier evidence (Masi et al, 2006), however with the exception of higher rates of intellectual disability and dyslexia, which may depend on the differences in sample composition. Other notable, original points in the current findings include the positive correlation between compulsion and ADHD symptom severity, and the good predictability of the presence of ADHD comorbidity by the current regression model consisting of being male; the absence of cleaning; the existence of concurrent conduct problems, tic disorders, and dyslexia; as well as longer treatment duration and poorer treatment response, with an 80.8% classification accuracy and good model fit.
In addition, the means of age, age of diagnosis, and age of symptom onset did not differ by ADHD comorbidity. Even so, the majority of previous findings have proposed an earlier onset of OCD symptoms in the context of ADHD comorbidity (Masi et al, 2006; Walitza et al, 2008). Contamination, religious, and somatic obsessions, as well as doubt and cleaning compulsions, the most prominent symptoms, varying by ADHD comorbidity, however, tended to be more prevalent in ADHD-free participants. According to the findings of a recent study on adult OCD, the rates of religious and sexual obsessions were higher in OCD patients with a background of childhood ADHD than in their opponents without a childhood ADHD background (Çelebi et al, 2016).
Lower severity scores for OCD symptoms (CY-BOCS) and a lower count of obsessions are strikingly inconsistent with prior data, which predominantly reported higher OCD symptom severity and symptom count in ADHD comorbidity (Walitza et al, 2008). Detection of lower OCD symptom severity despite higher global symptom levels (CGI-S) in the ADHD comorbid group may be attributable to the fact that predominantly severe ADHD symptom severity (CTRS) impairs global functionality in these patients. Although the reasons for these discrepancies with previous data are unclear, they may be owing to sample composition differences.
The findings of higher rates of presentation predominantly with compulsions (or pure compulsions), particularly in patients with ADHD comorbidity, appear noteworthy in terms of supporting previous hypothetic evidence regarding the overly overlapping symptoms between pediatric OCD and ADHD that may be dependent on compulsive coping mechanisms (such as excess controlling and perfectionism) frequently developing in the inattentive subtype of ADHD (Kooij et al, 2010; Pallanti et al, 2011). To avoid misdiagnosis, it is essential to distinguish these behaviors based on perfectionist coping styles from ego-dystonic compulsions. As in this example, both OCD and ADHD have a lot in common with some other psychiatric disorders within the impulsive–compulsive continuum that are either highly impulsive or have compulsive traits, such as pathological gambling and substance use disorders (Pallanti et al, 2011). Therefore, the impulsivity or compulsivity dominance in the symptom presentation of OCD-ADHD comorbidity may determine phenomenological differences, such as whether concurrent traits are more prone to tics, conduct problems, or internalizing problems.
Higher antipsychotic use in participants with ADHD comorbidity is also in accordance with the high rates of concurrent disruptive behavior disorders and tic disorders, as well as higher treatment resistance detected in the ADHD comorbid group, in which antipsychotic use might be requisite for SRI augmentation or managing comorbidities. The first strategy recommended for the treatment nonresponders is augmentation with additional agents, such as antipsychotics or tricyclic antidepressants. Another strategy is to ascertain the presence of comorbidities such as ADHD, tics, mood, or CDs. As previously reported in OCD, comorbidities were demonstrated to be associated with treatment unresponsiveness/resistance (Pallanti and Quercioli, 2006). Although bipolarity and ADHD comorbidity are encountered in treatment-resistant cases, few studies have addressed this issue (Magalhães et al, 2010; Sheppard et al, 2010).
Concurrent ADHD and OCD cause an unfavorable clinical course, increased susceptibility to substance abuse, and worse treatment response. Therefore, it is essential to diagnose and manage ADHD symptoms in OCD patients to improve the treatment outcomes and patients' quality of life (de Mathis et al, 2013). In the case of ADHD comorbidity, the tendency toward chronicity and stability in the symptom course of OCD, as well as longer symptom duration, may also be reflected in prolonged treatment durations. However, remarkable results regarding treatment resistance and poorer treatment responses appear to be associated with real negative impact of ADHD comorbidity on treatment outcomes of pediatric OCD. Furthermore, a recent study has confirmed that tight co-occurrence between OCD and ADHD can persist into adulthood (Ibrahim et al, 2020), which may be indicative of a tendency toward chronic-stable clinical course of OCD symptoms in the context of ADHD comorbidity.
Impulsivity could be one of the most important indicators of this comorbidity (Ibrahim et al, 2020; Mersin Kilic et al, 2016). Intriguingly, the findings revealed higher impulsivity scores (particularly in attentional and motor impulsivity) and more internalizing symptoms in adult OCD patients with a childhood ADHD background (even if the ADHD symptoms did not continue till adulthood) than in those without a childhood ADHD background (Ibrahim et al, 2020). However, separate impulsivity or internalizing symptom-related measurements were not included in this study, primarily owing to its naturalistic design. To address the same points reported in adult studies, it may be beneficial to conduct further research on the correlates associated with ADHD subtypes and impulsivity scores in pediatric OCD samples.
A close relationship between OCD, disruptive behavior disorders, and tic disorders, characterized by a distinct clinical course, specific phenomenological differences, and poorer treatment outcomes, has been amply documented by prior research (Lebowitz et al, 2012; Masi et al, 2006; Mathews and Grados, 2011; Sheppard et al, 2010) and was also supported by our related findings. Besides this specific relationship between chronic stable OCD, tics, and disruptive behavior disorders (ADHD, ODD, and CD) in the pediatric population, the diagnostic validity of a subtype comprising episodic OCD, bipolar disorder, and ADHD in both pediatric and adult populations has been debated for several years on a different side of the OCD literature (Amerio et al, 2014; Masi et al, 2007). This clinical relevance in pediatric OCD may be mediated by the presence of ADHD comorbidity in particular, given the specific comorbidity patterns that can represent distinctive subtypes of disorders in terms of phenomenology and treatment outcomes.
Current findings from between-group analyses also supported the striking impact of ADHD comorbidity on treatment outcomes (such as treatment options, drug use, treatment duration, treatment response, and treatment resistance). In multivariate logistic regression analysis, however, only longer treatment duration and low response/unresponsiveness predicted the presence of ADHD comorbidity. The influence of psychiatric comorbidities on treatment outcomes as an individual clinical characteristic of the patients has received considerable attention in the pediatric OCD literature. Among the numerous psychiatric comorbidities investigated, only the presence of tic disorders has received support for a differential effect on CBT response in pediatric OCD.
The majority of the studies investigating the influence of comorbidity on treatment outcomes using a single categorical variable for comorbidity failed to demonstrate a significant impact of comorbidity on treatment efficacy in pediatric OCD (Kemp et al, 2020). Therewithal, a positive association of treatment efficacy with the rates of concurrent anxiety disorder or tic disorder (McGuire et al, 2015; Öst et al, 2016) and a negative association with autism spectrum disorders (Iniesta-Sepúlveda et al, 2017) were reported in a few studies evaluating specific diagnostic categories.
Taken together, this evidence on the close association between tics, disruptive behavior disorders, and OCD, which may be particularly mediated by the presence of ADHD comorbidity, is essential for clinicians to get insight into descrying this specific subtype of pediatric OCD, which is more likely to present with symptoms in high impulsive and compulsive patterns, as well as worse treatment outcomes and chronicity in the course, persisting into adulthood. In terms of treatment adherence, clinicians should also closely monitor the potential for presentation of more severe conduct problems in pediatric OCD with ADHD comorbidity. Moreover, previous reports concerning the prediction of childhood psychiatric traits associated with social isolation, internalizing, and conduct problems for later OCD diagnosis in adulthood are consistent with these recommendations (Grisham et al, 2011; Saad et al, 2017).
On the contrary, our findings regarding the high comorbidity rates of GAD in the entire sample, as well as relevant results demonstrating no difference in prevalence by ADHD comorbidity, are consistent with previous reports (Masi et al, 2006; Masi et al, 2004). However, they only conflict with the common sense of some authors, who reported more severe anxiety symptoms in OCD patients with ADHD comorbidity (Diniz et al, 2012; Ibrahim et al, 2020). Further studies concerning the clinical implications of internalizing traits at the intersection of OCD and ADHD comorbidity may be beneficial to explore the higher rates of conduct problems.
The retrospective and cross-sectional evaluation of diagnostic scales are one of the several limitations that make the results susceptible to recall bias. Cross-sectional and naturalistic evaluation of clinical features at the first visit of patients is a significant limitation when debating the relationship between those and longitudinally assessed parameters such as treatment outcomes and clinical course in 4 years. However, the potential bias caused by this limitation was attempted to be mitigated by having the clinicians responsible for each patient's clinical follow-up collect their data. With all these, it is difficult to distinguish treatment effects in an observational study design, as they are not randomized. Therefore, longitudinal studies concentrating on the comparison of the clinical implications of different treatment options (methylphenidate vs. SRIs, etc.) would aid in the comprehension of the actual relationships between treatment options and treatment response.
Our findings are restricted to treatment-seeking patients referred to child and adolescent psychiatry outpatient clinics, which limits the generalizability of the findings to the broader youth OCD population. A longitudinal design would allow for a more thorough examination of correlational analyses between the severity of symptoms for both disorders and other clinical variables. For further research on the clinical implications of pediatric OCD in the presence of ADHD, it would be advantageous to include an impulsivity scale to interpret the impulsivity associated correlates in the findings on tic and conduct problems.
Conclusions
ADHD comorbidity was associated with several differences in clinical implications and treatment outcomes of pediatric OCD. The findings particularly highlight a shred of separate evidence on subtyping pediatric OCD according to ADHD comorbidity linked to concurrent tic and CDs, which is essential for clinicians to get insight into descrying this specific subtype of pediatric OCD that is more likely to present with symptoms in a high impulsive and compulsive pattern, as well as worse treatment outcomes and chronicity in the course, persisting into adulthood.
Clinical Significance
The close association between pediatric OCD, ADHD, and tic disorders can be defined as a specific subtype of pediatric OCD characterized by more severe conduct problems, a chronically stable course, and worse treatment outcomes. The impulsivity or compulsivity dominance in the symptom presentation of OCD-ADHD comorbidity may determine the phenomenological differences, such as whether concurrent traits are more prone to tics, conduct problems, or internalizing problems.
Footnotes
Ethical Approval
University of Health Sciences, Dr. Sami Ulus Maternity, Children's Health and Diseases Training and Research Hospital, Ethic Committee for Clinical Researches granted approval for this study (date: July 2, 2021, ethics committee number: 2020-KAEK-141/180, protocol number: E-21/06-174). Approval for the design and data collection procedures was obtained from the ethics review committee at the University of Health Sciences, Dr. Sami Ulus Maternity, Children's Health and Diseases Training and Research Hospital. The study was conducted in accordance with the Declaration of Helsinki, and the written informed consent was obtained from all participants and their parents before the onset of study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available owing to their containing information that could compromise the privacy of research participants.
Disclosures
No competing financial interests exist.