
Abstract
O
This study was approved by the local Institutional Review Board (HUPES: 4.261.651; UNIFESP: 46657415.0.3001.5505). A chart review was conducted (accessed September 2020/April 2021) of patients of any gender, aged ≤18 years, with a current diagnosis of MDD, according to the Diagnostic and Statistical Manual of Mental Disorders, presenting with SI. The exclusion criteria were bipolar depression, schizophrenia, substance use disorder, severe neurological condition, or a recent electroconvulsive therapy.
Esketamine administration (0.5 mg/kg, IV or SC) took 40 minutes, followed by an observation time of 2 hours. Blood pressure and emergent side effects were constantly monitored by a trained psychiatrist. The Montgomery–Åsberg Depression Rating Scale (MADRS) was used to assess the severity of depressive symptoms (total score) and SI (item 10) before esketamine administration and after 24 hours. Results were compared using a paired-samples t-test. Measures of effect size are given by Cohen's d. Significant results are set as p < 0.05. Statistical analysis was conducted using R version 4.0.4.
Records from 10 patients were included. Eight patients receive SC esketamine, whereas the remaining received IV. The mean age of the sample was 15.5 years (±1.35); 70% were females and 50% self-reported as mixed ethnicity. Three patients (30%) presented with psychiatric comorbidity and four (40%) had at least one medical comorbidity. Patient number 10 had a diagnosis of MDD with psychotic symptoms. The sample characteristics are presented in the Supplementary Table ST1.
There was a significant reduction in depressive symptoms (mean total MADRS score) from baseline to 24-hour postadministration (39.1 ± 6.30 to 26.8 ± 8.40; mean difference = 12.3; t = 4.22; p = 0.002; d = 1.33). In addition, we found a significant decrease in SI (mean MADRS item 10 score) when comparing baseline and 24-hour results (5.0 ± 1.16 to 2.7 ± 1.95; mean difference = 2.3; t = 3.14; p = 0.011; d = 0.99). Individual changes in depressive symptoms and SI scores can be seen in Figure 1.
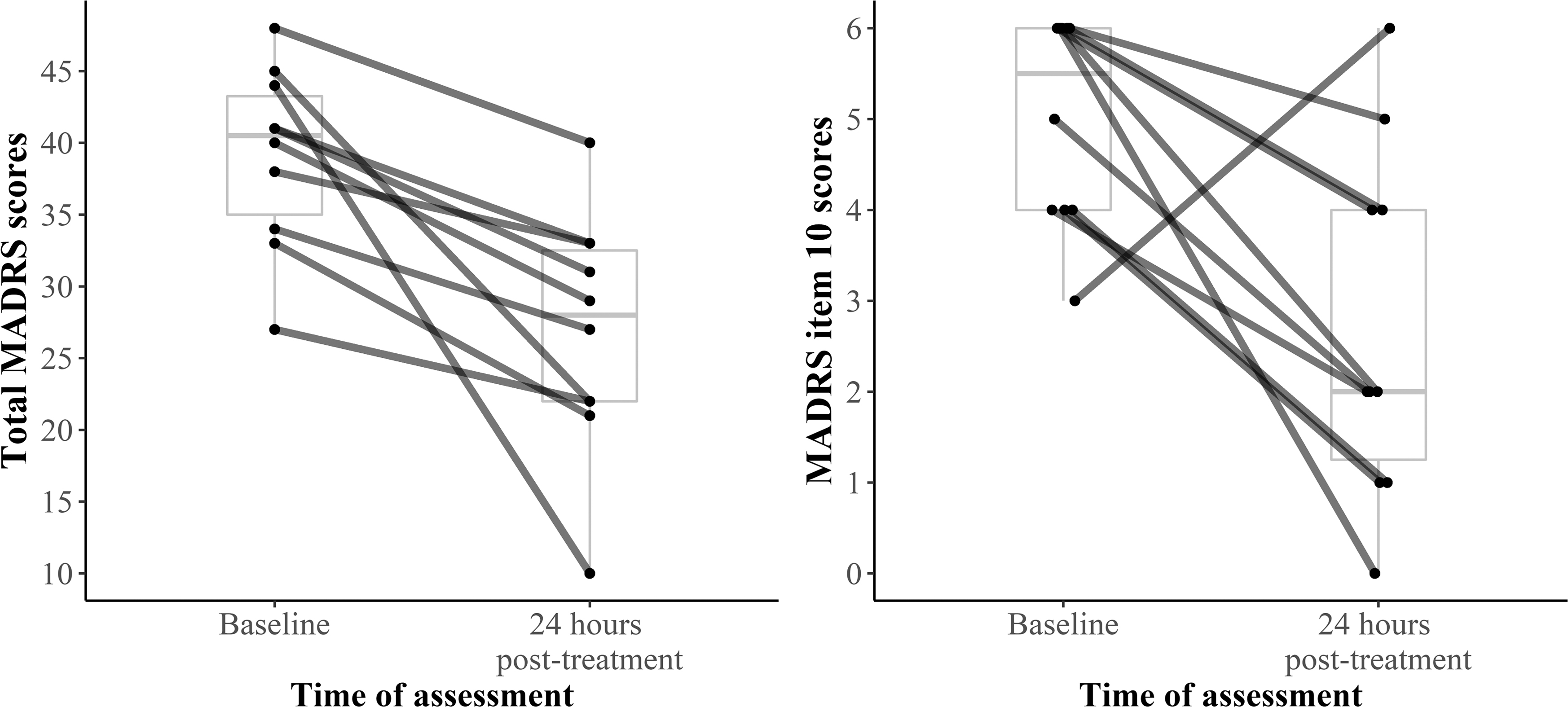
Total and item 10 MADRS scores at baseline and 24h post-treatment. Scores are given for each patient.
Most patients reported side effects only during esketamine administration or following the observational period. Dissociation was the most frequently self-reported symptom (50%), followed by dizziness (40%) and drowsiness (30%). Side effects were considered mild to moderate since they were short-lived, and no patients had treatment-emergent SI or suicidal behavior.
To the best of our knowledge, this is the first report of a rapid-onset antidepressant and antisuicidal effect of esketamine in depressed adolescents. The few studies that investigated the antisuicidal effects of ketamine in this population used the racemate and were restricted to single case reports. Nonetheless, repeated ketamine infusions in adolescents with treatment-resistant depression appear to improve depressive symptoms and SI (Kim et al. 2020).
Our results suggest that a single dose of parenteral esketamine can rapidly reduce the severity of depression and SI symptoms in adolescents with MDD and SI. Regardless, larger adequately controlled studies are needed, in addition to the investigation of multiple administrations of esketamine, and its long-term safety for this age group in different aspects, such as cognitive impairment and risk of recreational use.
Footnotes
Acknowledgment
The authors would like to thank Coral Rakovski for language review.
Authors' Contributions
All authors certify that they have participated sufficiently in the study to take public responsibility for the content.
Research Data
Anonymized data and analysis scripts are publicly available at
Disclosures
L.C.Q. reports consulting fees from Allergan, Abbot, Janssen Pharmaceutical, and Lundbeck, and research fees from Janssen Pharmaceutical. A.L.T.L. reports grants and personal fees from Janssen Pharmaceutical, personal fees from Daiichi Sankyo, Cristalia Produtos Químicos e Farmacêuticos, Libbs, Pfizer, Myralis Farma, Aché Laboratórios, Hypera Pharma, and Sanofi-Aventis, grants from Eli Lilly, H. Lundbeck A/S, Servier Laboratories, Hoffman-La Roche, Forum Pharmaceuticals, and from public programs: CNPq and FAPESP. The other authors report no conflicts of interest.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.