
Abstract
Objectives:
To assess characteristics and correlates of metabolic syndrome (MetS) in adolescents with major depressive disorder (MDD) or bipolar disorder-depressive episode (BP-d).
Methods:
Case–control study, using national inpatient sample data, including adolescents (age, 12–18 years) with a primary diagnosis of MDD or BP-d. Using propensity score matching (based on age, sex, and race/ethnicity), we extracted cases with MetS (≥3 of the following conditions: obesity, diabetes, hypercholesterolemia, and hypertension) and controls without MetS. We used a multivariable logistic regression model calculating adjusted odds ratios (aORs) for potential correlates of MetS, focusing on primary mood disorders and psychiatric comorbidities.
Results:
In 607 age-/sex-/race/ethnicity-matched adolescents (MDD = 83.5%, BP-d = 16.5%), comparing those with (N = 332) versus without MetS (N = 275), MetS was most prevalent in later-age adolescents (mean age 16.3 years), females (58.1%), Whites (40.3%), and Blacks (31.5%). MetS was characterized by obesity (84.9% vs. 3.6%), hypertension (81% vs. 1.8%), diabetes (72.8% vs. 9.1%), and hypercholesterolemia (67.2% vs. 3.6%) (all p < 0.001). MetS was associated with a primary diagnosis of BP-d versus MDD (aOR 2.42, 95% confidence interval [CI] 1.47–3.97) and comorbid disruptive behavior disorders (DBD) (aOR 4.45, 95% CI 1.55–12.78), while comorbid substance use disorder reduced MetS risk (aOR 0.31, 95% CI 0.19–0.50).
Conclusion:
In adolescents with MDD or BP-d, MetS was associated with a primary BP-d diagnosis, and comorbid DBD. MetS-related parameters should be screened for early in adolescents with depression-spectrum disorders aiming to prevent the development or effects of MetS.
Introduction
Metabolic syndrome (MetS) is a widely prevalent, multifactorial disorder and a public health concern characterized by a conglomeration of signs/symptoms of obesity, hypertension, dyslipidemia, hyperuricemia, and abnormalities of glucose homeostasis (i.e., insulin resistance, glucose intolerance, or diabetes mellitus) (Gupta and Gupta, 2010). There exists an association of various cardiometabolic parameters with mood disorders (Coello et al, 2019; Mansur et al, 2020; McIntyre et al, 2010). As per a national survey, an increased body mass index was associated with a higher risk of major depressive disorder (MDD) and suicidal ideation (Carpenter et al, 2000).
Obesity and diabetes are more prevalent among patients with bipolar and depressive disorders than in the general population (Elmslie et al, 2000; Talbot and Nouwen, 2000). MetS is one of the critical predictors of cardiovascular mortality/morbidity due to its proinflammatory and prothrombotic properties (Coello et al, 2019; Gupta and Gupta, 2010). Unfortunately, the prevalence of MetS has increased by more than 30% among U.S. adolescents between 1988–1992 and 1999–2000 (Duncan et al, 2004).
As per the current literature, MetS is seen in 35%–50% of patients with bipolar disorder (BP), a prevalence that is almost double compared to the general population (Coello et al, 2019; Dalkner et al, 2021; Kesebir, 2018; Prillo et al, 2021; Vancampfort et al, 2013). Multiple factors, such as sedentary and other unhealthy lifestyle, diet, genetic susceptibility, and several psychiatric medication groups, are associated with the development of MetS (Birmaher et al, 2022; Correll et al, 2015; Firth et al, 2019; Postolache et al, 2019; Rodriguez-Monforte et al, 2017). Specifically in BP, a history of trauma, sedentary habits, and various side effects of psychotropic medications has been found to be associated with an increase in the risk of MetS (Kesebir, 2018).
Importantly, a meta-analysis, including 29 studies, reported a bidirectional association between depression in adults and MetS (Pan et al, 2012), with similar results having been reported by another meta-analysis of 34 studies of adults with BP (Gimenez-Palomo et al, 2021).
Obesity, diabetes, and cardiovascular disorders were more common among children and adolescents with BP compared to the general population (Jerrell et al, 2010). As per a small cross-sectional study (N = 162), the prevalence of MetS was 19.8% in adolescents and young adults with BP, with low high-density lipoprotein (HDL)-cholesterol (56.5%) and abdominal obesity (46.9%) being the most common criteria present (Li et al, 2019).
The co-occurrence of MetS in individuals with BP has been associated with a more complex illness presentation (Gimenez-Palomo et al, 2021; McIntyre et al, 2010). There is a bidirectional relationship between MetS and psychiatric disorders, and the association is attributed to various factors, including inflammatory pathway activation, brain-derived neurotropic factors, medication side effects, or disease-related unhealthy lifestyle modifications (Nousen et al, 2013). Although there is sufficient literature on MetS in adults with mood disorders (Vancampfort et al, 2015; Vancampfort et al, 2014; Vancampfort et al, 2013), there are limited data in adolescents (Li et al, 2019).
The goals of this study were to (1) evaluate the association of MetS with the two primary mood disorders and psychiatric comorbidities; and (2) delineate the differences in demographic characteristics and cardiometabolic as well as psychiatric comorbidities in adolescents with MetS stratified by the primary mood disorder.
Methods
Data source and patient selection
We used the health care cost and utilization project's national inpatient sample (NIS), which consist of the largest inpatient database covering 4411 hospitals and 44 states in the United States, to determine hospital outcomes and comorbidities related to the disease of interest (Overview of the National [Nationwide] Inpatient Sample, 2019b). The NIS data were utilized from January 1, 2010, to December 31, 2014.
Our initial sample included 248,348 adolescent inpatients (age, 12–18 years old) with a primary discharge diagnosis of mood disorders (Kesebir, 2018), that is, MDD (91.1%) and BP-depressive episode (BP-d, 8.9%) based on the international classification of disease, ninth revision (ICD-9) diagnosis codes. We excluded patients with unspecified diagnoses to increase the validity of diagnoses in youth.
As cardiometabolic comorbidities, we considered diabetes, obesity, hypercholesterolemia, and hypertension, defining “MetS” in this study by having at least three of these conditions. The cardiometabolic comorbidities were identified from patient data using the ICD-9 diagnostic codes. From the study sample, 9.3% (N = 23,127) had at least one of the four cardiometabolic comorbidities, and only 0.1% (N = 332) had MetS. We used propensity score matching using SPSS version 27 to extract cases (MDD or BP-d with MetS, N = 332) and controls (MDD or BP-d without MetS, N = 275). The matching was performed based on demographic characteristics of age, sex, and race/ethnicity with a match tolerance of zero for exact matches.
Variables of interest
Psychiatric comorbidities were considered conditions coexisting with the primary MDD or BP-d diagnosis and were identified using ICD-9 codes. As psychiatric comorbidities, we included anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), disruptive behavior disorders (DBD), autism-spectrum disorders, and substance use disorders (SUD). We further included as a continuous variable the number of “chronic conditions” from the patient discharge records. In the NIS, chronic condition is defined as a physical or mental health condition that lasts ≥12 months and meets one or both of the following criteria: (1) limits self-care, independent living, and social interactions and (2) leads to the need for therapeutic intervention (NIS Description of Data Elements, 2019).
Data analysis
Descriptive statistics and cross-tabulation were used to assess in univariate analyses differences in primary and comorbid psychiatric diagnoses, as well as in chronic conditions with regard to MetS status among adolescents with MDD or BP-d. Pearson's Chi-square test and independent-sample T-test were used for categorical and continuous data, respectively. Next, we used a binomial logistic regression model to estimate the adjusted odds ratio (aOR) for potential categorical risk factors of MetS, including primary psychiatric mood disorder diagnosis and adjusted for psychiatric comorbidities (anxiety disorders, ADHD, DBD, and SUD), and considered the non-MetS group as the reference category. The regression model had a Nagelkerke R square of 0.094, which is considered moderate association.
Since the NIS-defined “chronic conditions” overlap with both MetS criteria/components and all psychiatric comorbidities, including MDD and BP-d, the number of chronic conditions, although significantly associated with MetS status in univariate analyses, was not included in the multivariable regression analyses of associations with MetS status. Finally, we used descriptive statistics and cross-tabulation to assess differences in demographic characteristics and cardiometabolic as well as psychiatric comorbidities by primary psychiatric diagnosis among the adolescents with MetS. All statistical analyses were conducted using SPSS version 27 (IBM Corporation, Armonk, NY, USA), with two-sided testing and alpha <0.05.
Ethical approval
NIS data are publicly available in de-identified format, and, to protect the privacy of patients, physicians, and hospitals, the state and hospital identifiers were removed. According to the agency for health care research and quality (AHRQ) of the U.S. department of health and human services, the use of NIS does not require approval from the institutional review board (Overview of the National [Nationwide] Inpatient Sample, 2019b).
Results
Characteristics and univariable associations of MetS in adolescents with mood disorders
Table 1 describes the overall characteristics and distribution of cardiometabolic and psychiatric comorbidities in adolescents with and without MetS. No statistically significant difference was observed in both groups for age, gender, and race/ethnicity. The mean age of overall sample was 16.3 (standard deviation 1.7). Majority of the sample were females (58.2%), and White by race/ethnicity (40.1%). Statistically significant differences in terms of cardiometabolic comorbidities were observed among both the groups. Patients with Mets were significantly more likely to report diabetes (72.8% vs. 9.1%), hypertension (81.0% vs. 1.8%), hypercholesterolemia (67.2% vs. 3.6%), and obesity (84.9% vs. 3.6%) (all p-values <0.001) (Table 1 and Fig. 1).
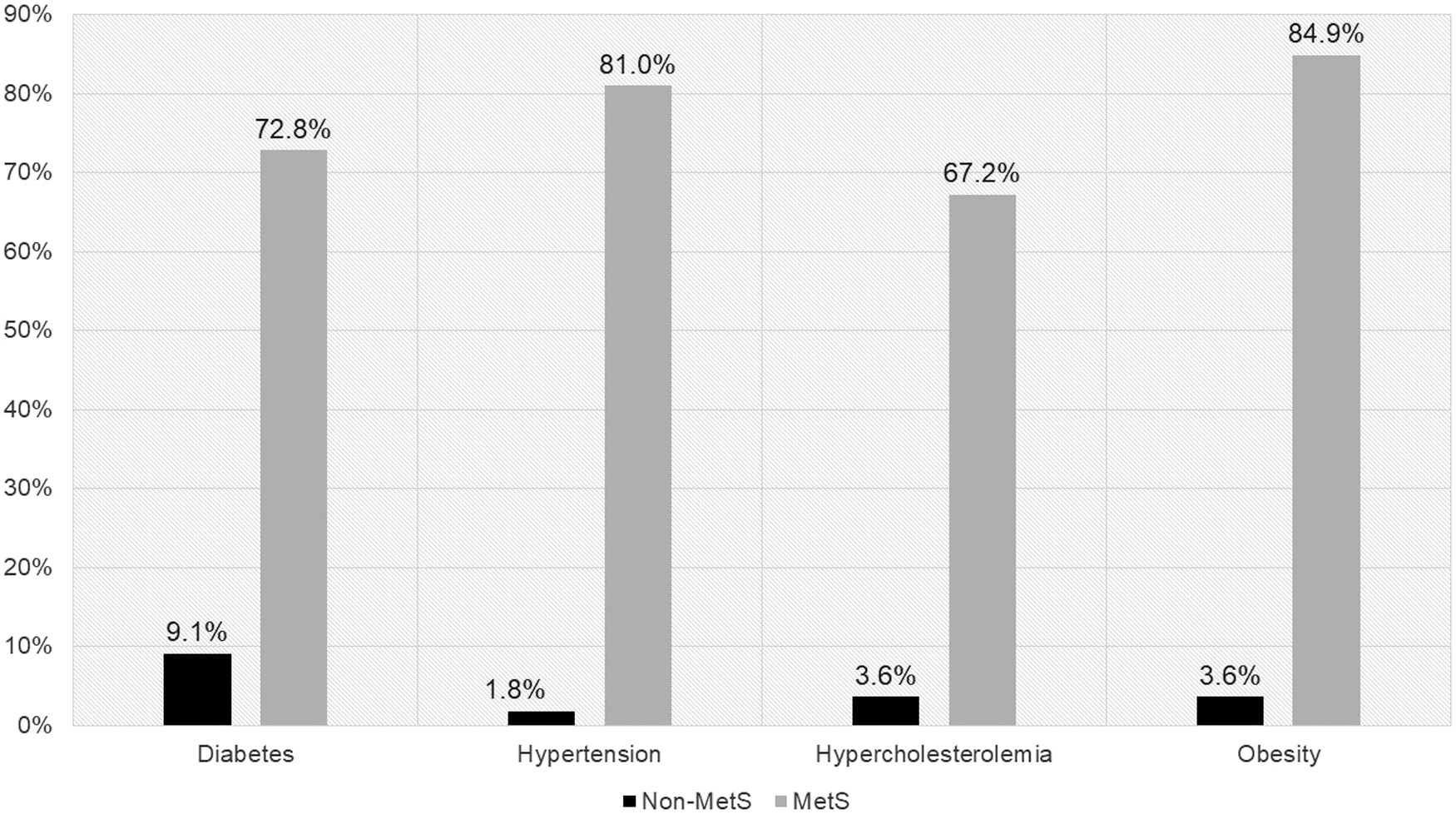
Distribution of cardiometabolic comorbidities used as MetS criteria in adolescents with mood disorders. The proportion between MetS and non-MetS groups was obtained using cross tabulation and the Pearson Chi-square (χ 2) test and was significant with p-value ≤0.001. MetS, metabolic syndrome.
Sample Characteristics and Distribution of Cardiometabolic and Psychiatric Comorbidities in Adolescents with Mood Disorders by Metabolic Syndrome Status
ADHD, attention-deficit/hyperactivity disorder; BP-d, bipolar disorder, depressive episode; MDD, major depressive disorder; MetS, metabolic syndrome; SD, standard deviation.
Among patients with MetS, the proportion of MDD was less (78.9% vs. 89.1%; p < 0.001) compared to those without MetS, while the proportion of BP-d was greater (21.1% vs. 10.9%; p < 0.001). In addition, a significantly greater proportion of patients with DBD (6.0% vs. 1.8%; p = 0.009) and mean number of chronic conditions (6.4 ± 1.6 vs. 3.1 ± 1.9; p < 0.01) and lower proportion of SUD (9.0% vs. 21.8%, p < 0.001) were observed among patients with MetS compared to patients without MetS.
Multivariable associations with MetS status in adolescents with mood disorders
In multivariable regression analyses, MetS status was associated with a primary diagnosis of BP-d (aOR 2.42, 95% confidence interval [CI] 1.47–3.97) compared to the adolescents with MDD. Among psychiatric comorbidities, DBD (aOR 4.45, 95% CI 1.55–12.78) was associated with a statistically significant higher likelihood for MetS, while SUD comorbidity reduced the risk of MetS (aOR 0.31, 95% CI 0.19–0.50) (Table 2).
Adjusted Multivariable Associations of Metabolic Syndrome Status with Primary and Comorbid Psychiatric Diagnoses in Adolescents with Mood Disorders
ADHD, attention-deficit/hyperactivity disorder; aOR, adjusted odds ratio; BP-d, bipolar disorder-depressive episode; MDD, major depressive disorder.
Demographic variables and cardiometabolic as well as psychiatric comorbidities in adolescents with MDD versus BP-d and MetS
Comparing adolescents with MetS and MDD versus BP-d, a diagnosis of BP-d was significantly associated with a slightly higher age (16.9 ± 1.5 years vs. 16.1 ± 1.8 years, p < 0.001), a higher proportion of Blacks (69.7% vs. 19.6%), and a lower proportion of Whites (15.2% vs. 47.8%), Hispanics (7.6% vs. 16.3%), and others (7.6% vs. 16.3%) (p < 0.001); higher proportion of patients had obesity (92.8% vs. 82.8%, p = 0.040) and lower proportion of patients had hypercholesterinemia (56.5% vs. 70.1%, p = 0.031); as well as greater number of psychiatric comorbidities (6.9 ± 1.7 vs. 6.3 ± 1.5, p = 0.002) and comorbid ADHD (35.7% vs. 11.5%) (Table 3).
Demographic Characteristics and Distribution of Psychiatric Comorbidities in Adolescents with Mood Disorders and Metabolic Syndrome
ADHD, attention-deficit/hyperactivity disorder; BP-d, bipolar disorder-depressive episode; MDD, major depressive disorder; SD, standard deviation.
Discussion
This matched nationwide case–control study of adolescents with MDD or BP-d had the following main findings: (1) from the entire NIS sample (N = 248,348), 9.3% had at least one of the four defined cardiometabolic comorbidities, and 0.1% (N = 607) had MetS defined by the presence of at least three of the four defined cardiometabolic comorbidities; (2) adolescents with a primary diagnosis of BP-d compared to those with MDD, and those with comorbid DBD had higher odds of MetS by 2.4 and 4.5 times, respectively; (3) comparing adolescents with MetS and either MDD versus BP-d, adolescents with BP-d were slightly older, and had a higher proportion of blacks, more comorbid ADHD, as well as obesity, whereas adolescents with MDD had a higher proportion of all other racial/ethnic groups and a higher prevalence of hypercholesterolemia.
As per the third national health and nutrition examination survey (1988–1994) in the general population, 4.2% of adolescents demonstrated MetS (Cook et al, 2003). A meta-analysis found a higher prevalence of MetS in adults with BPs (37.3%) and the rate increased with age (Vancampfort et al, 2013). The fact that our inpatient sample population had a lower proportion of MetS was very likely due to the fact that we used presence of at least three of the following four diagnosed cardiometabolic conditions, diabetes, obesity, hypercholesterolemia, and hypertension, as a proxy for MetS. Moreover, it is also possible that the risk of MetS is lower among children with mood disorders and that the risk increases with age. We had to employ this approach due to lacking laboratory data. Therefore, our data highly likely only generalize and apply to adolescents with mood disorders who have advanced/more severe MetS.
In our study, adolescents with BP-d had a higher odd of MetS compared to those with MDD. This finding is supported by a cross-sectional study that found a prevalence of MetS of 19.8% in 162 adolescents and young adults with BP, which is estimated to be almost double compared to the general population. The most common criteria met in these study participants for MetS were low HDL (HDL cholesterol, 56.5%) and obesity (46.9%) (Li et al, 2019).
The symptoms of depression and anxiety have been seen in relation to a low level of HDL cholesterol and a higher waist circumference, and higher low-density lipoprotein cholesterol (Kim et al, 2019; Vancampfort et al, 2013). As per the data from the South Carolina Medicaid program, obesity, type 2 diabetes mellitus, and cardiovascular disorders were more common among children and adolescents with BP compared to other psychiatric disorders (Jerrell et al, 2010).
The fact that BP-d was associated with significantly greater odds of MetS than MDD is probably due to several likely interactive factors. These include the slightly higher age of the population in BP-d group, greater proportion of Blacks (70% vs. 20%), higher proportion of patients with ADHD, and greater number of chronic conditions. As per the course and outcome of bipolar youth (COBY) study, non-White race was independently associated with obesity and overweight (Goldstein et al, 2008), and Black race has been associated with more obesity/higher fat mass and diabetes risk, but lower lipid abnormalities compared to White race in adults in the general population (Li et al, 2008; Lin et al, 2011; Selvin et al, 2011; Sentell et al, 2012; Sumner et al, 2010; Tsugawa et al, 2012; Yu et al, 2012; Ziemer et al, 2010) and first-episode schizophrenia (Correll et al, 2014).
Data derived from the COBY study have indicated that the use of atypical antipsychotic agents was the only class of medication that was associated with significant weight gain and obesity. Youths with BP are often treated with second generation antipsychotic agents, whereas the youth with MDD are not routinely taking an antipsychotic agent, which can explain, in part, the differences in the metabolic abnormalities between youths with BP and MDD (Goldstein et al, 2008). Since obesity is central to insulin resistance and the development of MetS (McElroy and Keck, 2014; Rask Larsen et al, 2018), the higher prevalence of obesity in adolescents with BP-d likely contributed to the higher odds of MetS.
Previous studies have found a higher prevalence of obesity and MetS among patients with BP and depression (Elmslie et al, 2000; Kesebir, 2018; Kinder et al, 2004). Also, shared neurobiological abnormalities, common genetic vulnerability, and the side effects of psychotropic medications can account for the higher association of MetS among patients with BP-d (McElroy and Keck, 2014).
The fact that a greater number of psychiatric comorbidities were associated with MetS has been described before in a meta-analysis of adults with depression (Vancampfort et al, 2014). In addition, more complex mood disorders with more comorbid psychiatric conditions are also more likely to receive more medications, including mood stabilizers and antipsychotics (Cervesi et al, 2017; Correll et al, 2010), which have been associated with a greater risk of MetS (Correll et al, 2015; De Hert et al, 2011).
Interestingly, there exists an association of obesity and hypertension with ADHD and as per a meta-analysis, the pooled prevalence of obesity was increased by 40% in children with versus those without ADHD (Cortese et al, 2016; Kase et al, 2021; Landau and Pinhas-Hamiel, 2019). Finally, adverse childhood experiences have been associated with both a higher risk of psychiatric disorders as well as MetS, which could provide a further reason for the association between psychiatric comorbidities and MetS (McIntyre et al, 2012). However, since no information about adverse childhood experiences was available for our study, this argument is therefore speculative.
The significant association between comorbid DBD and a 4.5-times higher odds of MetS in adolescents with mood disorders is likely related to more complex clinical presentations and frequent symptomatic expression of DBD as anger outbursts and aggressive behaviors, for which antipsychotics are frequently used (Olfson et al, 2014; Olfson et al, 2012; Park et al, 2016; Scotto Rosato et al, 2012), which have the greatest cardiometabolic risk profile among psychotropic medications (Correll et al, 2014; Galling et al, 2016; Maayan and Correll, 2011). Moreover, DBD are a heterogeneous group of conditions and encompass a wide variety of symptoms and can co-occur with ADHD and autism (Stadler et al, 2010). These patients are at higher risk of weight gain, which remains elevated when they transition from childhood to adulthood (Anderson et al, 2006).
The association of SUD and MetS is complex and data are limited and contradictory among adolescents (Virmani et al, 2007). Adolescents with SUD are at a higher risk of developing energy and nutrient inadequacy (Yung and Lau, 2019). However, other studies have found that substance-using adolescents and young adults consume higher calories and fat (Arcan et al, 2011; Nolan and Stolze, 2012). The apparent disparity of findings could be due to the study design, with cross-sectional studies not showing an association between substance use and obesity (Lanza et al, 2015).
In addition, however, SUD have been identified as a risk factor for nonadherence with psychiatric medications (Kane et al, 2013) so that the lower risk of MetS could also be due to less adverse cardiometabolic medication effects of prescribed medications. Therefore, adherence should be measured in future studies, including youth or adults with SUD. Data derived from the COBY study have also indicated SUD as one of the robust predictors of overweight/obesity (Goldstein et al, 2008). Conversely, interpreting the data from the Canadian Community Health Survey-Mental Health and Well-Being (CCHS), it was found that the overweight or obese bipolar individuals had a significantly lower rate of SUD than those with appropriate or normal weight (McIntyre et al, 2007).
Our study results should be considered within its limitations. First, this is a cross-sectional and retrospective study. Therefore, the association between MetS and primary mood disorders as well as psychiatric comorbidities represents a statistically significant association and not a causal relationship. Second, the diagnosis of MetS and inclusion of metabolic comorbidities was only based on diagnostic codes of four cardiometabolic comorbidities, which may have led to underreporting of the MetS. In this sense, results are likely most applicable to adolescents with MDD or BP-d with advanced or more severe forms of MetS.
Third, since the NIS definition of chronic conditions includes both somatic and mental disorders that last ≥12 months and either is associated with relevant functional impairment and/or need for therapeutic intervention, chronic conditions could not be entered into the multivariable regression analyses, as they overlapped substantially with MetS components as well as the MDD, BP-d, and psychiatric comorbidities. Finally, due to the administrative nature of the NIS data, we were restricted in our inclusion of demographic and clinical variables as potential correlates of MetS, including lacking variables like lifestyle, diet, smoking and substance use frequency, genetic susceptibility, adverse childhood experiences, illness duration and severity, and psychotropic medication use.
Nevertheless, despite these limitations, this is one of few studies of MetS risk factors in adolescents with mood disorders, comparing patients with MDD with those diagnosed with BP-d, employing a case–control design nested in a large representative U.S. data set, providing useful information on diagnostic associations with MetS.
Conclusion
Among the adolescents with mood disorders, a primary diagnosis of BP-d and comorbid DBD increases the odds of MetS, while comorbid SUD lower the odds of MetS. Among the various parameters of MetS, the rates of obesity were significantly higher among adolescents with BP-d, whereas hypercholesterolemia was higher among those with MDD.
Clinical Significance
Our study results indicate the need for proactive screening of various cardiometabolic parameters starting early in the illness to prevent the development and serious adverse physical effects of MetS.
Footnotes
Acknowledgment
We would like to thank Dr. Jenil Patel MBBS, MPH, PhD (Assistant Professor, Center for Pediatric Population Health at University of Texas Health Dallas), for reviewing the statistical analysis and dataset, and recommending his input on the results and limitations of this study.
Disclosures
R.S.P. and P.M. report no conflicts of interest. C.U.C. has been a consultant and/or advisor to or has received honoraria from AbbVie, Acadia, Alkermes, Allergan, Angelini, Aristo, Axsome, Cardio Diagnostics, CNX Therapeutics, Compass, Damitsa, Gedeon Richter, Hikma, Holmusk, IntraCellular Therapies, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedAvante-ProPhase, MedInCell, Medscape, Merck, Mindpax, Mitsubishi Tanabe Pharma, Mylan, Neurocrine, Noven, Otsuka, Pfizer, Pharmabrain, Recordati, Relmada, Reviva, Rovi, Seqirus, Servier, SK Life Science, Sumitomo Dainippon, Sunovion, Supernus, Takeda, Teva, and Viatris. He provided expert testimony for Janssen and Otsuka. He served on a Data Safety Monitoring Board for Lundbeck, Relmada, Reviva, Rovi, and Teva. He has received grant support from Janssen and Takeda. He received royalties from UpToDate and is also a stock option holder of Cardio Diagnostics, Mindpax, and LB Pharma.