
Abstract
Introduction:
Pediatric bipolar disorder (PBD) is a severe psychiatric illness diagnosed before the age of 18, which is associated with extreme shifts in mood characterized by manic and depressive episodes. In 2005, AACAP published algorithms to guide pharmacological treatment of manic/mixed episodes associated with PBD. At that time, lithium was the only Food and Drug Administration (FDA)-approved treatment for pediatric bipolar manic/mixed episodes. The goal of this article is to review evidence that has emerged since the AACAP algorithm in 2005.
Methods:
Literature searches were conducted through PubMed and limited to studies published between 2005 and 2021, using keywords that focused on randomized controlled trials (RCTs) for available psychopharmacological medications. In addition, the authors conducted in-depth searches for articles providing evidence for agents included in the 2005 AACAP algorithm.
Results:
Since the publication of the AACAP algorithm in 2005, multiple RCTs have been conducted in PBD, leading to FDA approval of five medications (aripiprazole, asenapine, olanzapine, quetiapine, and risperidone) for the treatment of manic/mixed episodes and two medications (lurasidone and olanzapine-fluoxetine combination) for the treatment of depressed episodes. Divalproex sodium and oxcarbazepine were studied in pediatric RCTs and failed to separate from placebo.
Conclusions:
We offer an update to the 2005 AACAP algorithms for the treatment of pediatric bipolar mixed/manic episodes and added an evidence-based algorithm for the treatment of depression in PBD. In addition to treatment algorithms, we review current evidence for efficacy of agents proposed in the AACAP algorithm and provide tables summarizing medication side effects and efficacy.
Introduction
Bipolar I disorder (BD) is a major lifelong psychiatric illness that causes significant shifts in mood, energy level, and ability to function. A diagnosis of BD requires the patient to have at least one lifetime manic episode, which may precede or follow a hypomanic or depressed episode (American Psychiatric Association 2013). Manic or hypomanic episodes are defined by distinct periods of elevated, expansive, or irritable mood and abnormally and increased goal-directed activity or energy, which must last at least 1 week, or require hospitalization, for a full manic episode. Most patients with BD will experience depressed episodes, although lifetime occurrence of a depressed episode is not required for a diagnosis of BD (American Psychiatric Association 2013). Mixed features can occur during a manic, hypomanic, or depressive episode (American Psychiatric Association 2013).
Psychotic symptoms are common during a severe episode of bipolar disorder (Kowatch 2016; Lee 2016). BD is associated with high rates of morbidity, impairments in psychosocial functioning, suicidal behavior, and consequent mortality. Acute manic episodes are associated with high-risk behaviors, such as gambling, drug use, vehicle accidents, and risky sexual behavior. Depressed episodes are associated with high risk of suicide (American Academy of Child and Adolescent Psychiatry 2009; Connor et al. 2017; Singh 2019).
Pediatric bipolar disorder (PBD) is characterized by the same symptoms as adult BD, but must be diagnosed before the age of 18 years. PBD has an estimated prevalence rate of 1.8% (Van Meter et al. 2011). As many as 55%–60% of adults with BD report an onset of symptoms before the age of 18 years (Perlis et al. 2004). Patients with PBD are likely to experience 10 or more mood episodes over their lifetime, with more than 75% experiencing lifetime suicidal ideation (Axelson et al. 2006). Due to the severe negative impact of PBD on quality of life as well as increasing the risk of premature mortality, appropriate and timely diagnosis and treatment are essential.
Over the last two decades, randomized controlled trials (RCTs) of multiple agents for the treatment of PBD have been conducted and published. However, the most recent algorithm to guide psychopharmacological treatment of PBD, manic/mixed episodes, was published by AACAP in 2005 (Kowatch et al. 2005). At that time, lithium was the only medication approved by the Food and Drug Administration (FDA) for acute manic/mixed episodes with positive randomized controlled studies in children and adolescents (Gram and Rafaelsen 1972; Geller et al. 1998). Therefore, the AACAP algorithm was based on adult RCTs and data from open-label trials and retrospective chart reviews in children and adolescents.
Since 2005, data from RCTs resulted in the FDA approval of five additional medications [aripiprazole (Findling et al. 2009), asenapine (Findling et al. 2015b), risperidone (Haas et al. 2009; Geller et al. 2012), olanzapine (Tohen et al. 2007), and quetiapine (Pathak et al. 2013)] for the treatment of manic/mixed episodes in PBD. Several agents (divalproex sodium [DVX] and oxcarbazepine) that were recommended by the AACAP algorithm have failed to separate from placebo in RCTs (Wagner et al. 2006, 2009). Other treatments (carbamazepine, topiramate, clozapine, and ECT) recommended by the AACAP algorithm still do not have published high-quality RCTs to evaluate their usefulness.
There has been less research into the treatment of PBD, depressed episodes. The first two agents for treatment of PBD depression were approved in 2013 (olanzapine-fluoxetine) and 2018 (lurasidone). In addition, lamotrigine showed efficacy in delaying recurrence of depressed episodes in PBD (Findling et al. 2015a). Quetiapine, a useful agent for the treatment of adult bipolar depression, failed to separate from placebo in PBD RCTs (DelBello et al. 2009; Findling et al. 2014).
This article reviews research on the efficacy of agents proposed for the treatment of PBD in the AACAP algorithm and proposes adjustments based on high-quality evidence from RCTs. The AACAP algorithm does not provide guidance for the treatment of PBD, depressed episodes. We propose a stepwise approach to treatment of PBD, depressed episodes based on currently available high-quality evidence.
Methods
Literature review
The authors reviewed RCTs for medications used for PBD published between 2005 and 2021. Literature searches through PubMed were conducted using the following keywords: “pediatric,” “adolescent,” “bipolar,” “mania,” “depression,” and “randomized controlled” with “lithium,” “divalproex,” “risperidone,” “quetiapine,” “olanzapine,” “aripiprazole,” “asenapine,” “lamotrigine,” “olanzapine-fluoxetine,” “lurasidone,” “carbamazepine,” “oxcarbazepine,” “ziprasidone,” and “topiramate.” The filters for “Clinical Trial,” “English,” and “Child: Birth-18” were selected. A separate search was conducted for clozapine due to its unique role in the pharmacological treatment of PBD. The keywords “bipolar,” “mania,” “depression,” “randomized controlled,” and “clozapine” were searched with the filters “Clinical Trial” and “English.”
Evidence for nonpharmacological treatment strategies, including psychotherapy, bright light therapy, omega-3 fatty acids (O3FAs), and electroconvulsive therapy (ECT), was reviewed as well. The authors searched PubMed for RCTs in children for each strategy. If RCTs could not be found, the authors searched for open-label or chart review evidence in children. If there was no available evidence in children, data in adults with bipolar disorder were reviewed.
Evidence evaluation and grading
The evidence was categorized into four categories according to The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) System (The GRADE Working Group 2013). The GRADE approach classifies evidence as high, moderate, low, or very low. This system has been adopted by several well-respected organizations such as the World Health Organization and the Cochrane Collaboration.
GRADE Quality of Evidence Guide (2013): High: “We are very confident that the true effect lies close to that of the estimate of the effect.” Moderate: “We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different” Low: “Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.” Very Low: “We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect”
High-quality evidence was reviewed and used to develop the algorithm presented in this article. Nonpharmacological treatment strategies with best available evidence were incorporated into the algorithm.
Definition of response rates and remission
In the algorithms, partial response, response, and remission rates were defined analogously to commonly used standards in RCTs for PBD (DelBello et al. 2009, 2017; Findling et al. 2009, 2014; Haas et al. 2009; Patino et al. 2021). For manic/mixed episodes, full response is defined as ≥50% reduction in Young Mania Rating Scale (YMRS) total score from baseline to endpoint. Partial response is defined as a decrease in YMRS score >0%, but <50%. Remission is defined as a YMRS total score ≤12. For depressive episodes, full response is defined as ≥50% reduction in Children's Depression Rating Scale-Revised (CDRS-R) total score (after subtracting 17 from raw scores). Partial response is defined as a decrease in CDRS-R total score >0%, but <50%. Remission is defined as CDRS-R total score ≤28, and YMRS total score ≤8.
Augmentation strategies
Currently available medications studied for PBD do not produce full response for all patients when used as monotherapy, necessitating augmentation with other agents. Combination therapies have not been well studied in clinical trials of PBD. Therefore, in developing our algorithms, we relied on principles of rational polypharmacy in psychiatry when recommending augmentation strategies (Preskorn and Lacey 2012; Zigman and Blier 2012). These principles include the following:
Optimize monotherapy (i.e., avoid subtherapeutic dosing).
Avoid pharmacodynamic redundancy (i.e., avoid combining medications with largely the same mechanism of action).
Consider pharmacodynamic interactions (i.e., avoid combining medications with opposing mechanisms of action).
Consider pharmacokinetic interactions (i.e., beware of how prescribed medications are metabolized and whether they induce or inhibit each other's metabolic pathways).
Regularly reassess, reduce, and simplify.
Results
Treatment of manic/mixed episodes
Table 1 summarizes the high-quality studies that appeared in the literature search for manic/mixed episodes. Studies were included if they were RCTs in children and adolescents. A study was given a GRADE of “high” if it was an RCT in children or adolescents without important limitations, such as small size or concerns about reliability. More detail on the factors that can justify downgrading a study can be found in the GRADE handbook (2013). The length of study, age of participants, number of patients enrolled, average medication dose, response rates, mean weight gain, and common adverse events for the studies listed in Table 1 can be found in Table 2. If effect size was reported, it can be found in Table 3.
High-Quality Studies for Medications Used in the Treatment of Pediatric Bipolar Disorder, Manic/Mixed Episodes
CoLT, the collaborative lithium trials; FDA, Food and Drug Administration; RCT, randomized controlled trial; SGA, second-generation antipsychotic; TEAM, Treatment of Early Age Mania.
Randomized Controlled Trials from 2005 to 2021 for the Treatment of Pediatric Bipolar Manic/Mixed Episodes
Studies 1–7 and 9–11 included participants diagnosed with bipolar I disorder, mixed or manic episode. Study 8 included participants with bipolar I disorder, manic episode.
Studies 4, 5, and 8 had fixed dosing.
Study 6 had flexible dosing within randomly assigned fixed dose ranges. Fixed dose ranges are provided.
Studies 2, 3, 7, 9, and 10 had flexible dosing. Average dose is provided.
Studies 1 and 11 had weight-based flexible dosing. Average dose per weight group is provided.
Studies 3–6, 7–8, and 9–11 defined response as ≥50% decrease in YMRS total score from baseline to endpoint. Study 2 defined response as CGI-BP-I mania score of 1 or 2. Study 1 defined response as ≥50% decrease in YMRS total score from baseline to endpoint AND CGI-I score of 1 or 2.
In divided doses.
At the request of the FDA due to study drug overdoses, an independent audit was conducted. The independent audit found that all data were reliable for safety and 81.4% of data were reliable for efficacy. However, the FDA concluded that they do not consider the study reliable.
CGI-BP-I, clinical global impression for bipolar illness-improvement; CGI-I, Clinical Global Impression–Improvement; Divalproex sodium ER, divalproex sodium extended release; EPS, extra-pyramidal symptoms; FDA, Food and Drug Administration; TEAM, Treatment of Early Age Mania; YMRS, Young Mania Rating Scale.
Reported Effect Sizes from Randomized Controlled Trials for the Treatment of Pediatric Bipolar Disorder, Manic/Mixed Episodes
Mean dose by weight group are reported for lithium and ziprasidone. Fixed doses are reported for aripiprazole and quetiapine. Fixed dose ranges are provided for risperidone. Mean daily dose is reported for olanzapine.
FDA-approved medications for the treatment of PBD, manic/mixed episodes
Mood stabilizers
Lithium
Lithium is thought to have been grandfathered in by the FDA in the early 2000s for the treatment of PBD, manic or mixed episodes in children 12 years of age and older due to data from positive adult clinical trials. In 2018, the FDA approved lithium for the treatment of mania in children and adolescents 7–17 years of age based on positive results in pediatric RCTs. Findling et al. (2015a) enrolled 81 participants with mania and assigned participants to lithium or placebo. The change in YMRS score was significantly larger for the lithium group compared to the placebo group. On a measure of overall improvement, 47% of lithium-treated participants (n = 25) achieved a score of very much or much improved (1 or 2) on the Clinical Global Impression–Improvement (CGI-I) scale, compared to 21% of placebo participants (n = 6).
The response rate for lithium was numerically higher than the response rate for placebo, but it did not achieve statistical significance. The most common adverse events associated with lithium were vomiting (45%), nausea (43%), and headache (36%). Lithium was associated with a statistically significant increase in thyrotropin concentration compared to placebo (increase of 3.0 mIU/L and −0.1 mIU/L, respectively). No weight gain was observed in the lithium group compared to placebo.
In another study that made a direct comparison of lithium, risperidone, and divalproex sodium for the initial treatment of PBD, lithium was the second most effective medication in treating pediatric mania (Geller et al. 2012). Lithium had a higher discontinuation rate (32.2%) than risperidone (15.7%) or divalproex sodium (26.0%), suggesting lower tolerability. Lithium-treated participants had a higher response rate than divalproex sodium-treated participants, but a lower response rate than risperidone-treated participants.
A recent study made a direct comparison of lithium and quetiapine for the treatment of manic or mixed episodes in children 10–17 years of age with a recent diagnosis of bipolar disorder (Patino et al. 2021). There was a statistically significant difference in response rates; 72% of participants responded to quetiapine and only 49% responded to lithium. Remission rates did not significantly differ between treatment groups. The most common adverse events among lithium-treated participants were headaches, nausea, somnolence, tremor, and emesis. The most common adverse events among quetiapine-treated participants were somnolence, headaches, tremor, dizziness, and nausea. Weight gain was higher for quetiapine-treated participants. There was a significant difference in completion rates, 59% of lithium-allocated participants completed the study compared to 79% of quetiapine-allocated participants. The lower completion rate in the lithium arm of the study might indicate lower efficacy, slower response rate, and/or poor tolerability of lithium.
Even though lithium underperformed in comparison to second-generation antipsychotics (SGAs) in RCTs evaluating acute treatment of manic/mixed episodes in PBD, lithium continues to be an important medication to consider due to its unique positive attributes. One significant and unique benefit of lithium is its ability to reduce suicidal behavior in adults (Lewitzka et al. 2015) and children (Hafeman et al. 2020). In addition, lithium was shown to have neuroprotective benefits in vitro and in vivo (Ochoa 2022). In vivo, neuroprotective benefits were measured by imaging morphological changes in the brain (Sun et al. 2018) and measuring markers of cytotoxicity (Hajek et al. 2012) in adult patients treated with lithium. In addition, lithium is associated with higher levels of neurotrophins in animal models (Zanni et al. 2017). However, at this time, there are no studies demonstrating clinical significance of changes in neuroprotective markers induced by lithium (Ochoa 2022).
Of note, lithium and aripiprazole are the only two medications with an FDA indication for the maintenance treatment of PBD.
SGAs with mood stabilizing properties
Aripiprazole
Aripiprazole was FDA approved in 2008 for the treatment of manic/mixed episodes in PBD based on a large randomized, double-blind, placebo-controlled, multicenter trial (N = 296) (Findling et al., 2009). This study compared treatment with aripiprazole 10mg, 30mg, and placebo over the course of four weeks. Aripiprazole performed significantly better than placebo. Cohen's d effect sizes in this study were 0.60 for aripiprazole 10 mg/day and 0.93 for aripiprazole 30 mg/day (Youngstrom et al. 2013). The most common adverse events associated with aripiprazole treatment were extra-pyramidal symptoms (EPS) (12.2% of 10 mg group and 27.3% of 30 mg group) and somnolence (19.4% of 10 mg group and 26.3% of 30 mg group). Mean weight gain was not significantly different between groups.
Asenapine
Asenapine was approved by the FDA for mania associated with bipolar disorder in children in 2015 following one large multicenter, randomized, double-blind, placebo-controlled study (Findling et al. 2015b). This study evaluated the efficacy of three doses of asenapine compared to placebo in treating children diagnosed with BD, mixed or manic episodes, with or without psychosis. Four hundred three children 10–17 years of age were enrolled in a 3-week acute treatment phase and randomized to asenapine 2.5 mg B.I.D, asenapine 5 mg B.I.D, asenapine 10 mg B.I.D, and placebo. All three doses of asenapine were superior to placebo in improving YMRS total score, YMRS responder rate, Clinical Global Impressions for Bipolar Illness (CGI-BP) severity, and CGAS score.
The most common (≥5% and twice the rate of placebo) treatment emergent adverse events were somnolence, sedation, increased appetite, loss of sensation of the mouth, and abnormal sensation of the mouth. Clinically significant weight gain (≥7%) was observed in all three asenapine groups significantly more than in the placebo group.
Risperidone
Risperidone is one of the most studied SGAs for PBD, mixed or manic episodes. Risperidone was approved by the FDA in 2007 following a multicenter, randomized, double-blind, placebo-controlled trial comparing the efficacy of two doses of risperidone to placebo (Haas et al. 2009). One hundred sixty-nine children 10–17 years of age were enrolled in a 3-week acute treatment phase and assigned to low-dose risperidone (0.5–2.5 mg/day), high-dose risperidone (3–6 mg/day), or placebo. YMRS response rates in this study for low-dose risperidone, high-dose risperidone, and placebo were 59.2%, 63.3%, and 26.3%, respectively.
Observed effect sizes were 1.04 in the low-dose group and 0.90 in the high-dose group, suggesting that a lower dose of risperidone may be sufficient for many patients. Adverse events most commonly reported with risperidone treatment were somnolence (21% low dose, 34% high dose, and 11% placebo), headache (20% low dose, 23% high dose, and 19% placebo), and fatigue (9% low dose, 18% high dose, and 2% placebo). Mean weight gain for the low-dose group, high-dose group, and placebo group was 1.9, 1.7, and 0.7 kg, respectively.
In the 2012 Treatment of Early Age Mania (TEAM) study (Geller et al. 2012), described in detail above, the risperidone group had the highest completion rate, suggesting relatively better tolerability compared with lithium or divalproex. In addition, the risperidone group had the highest Clinical Global Impressions for Bipolar Illness-Improvement (CGI-BPI-IM) response rate for the study population as a whole and in the subset of participants with psychosis. The adverse events more common for risperidone compared to lithium and divalproex sodium were increased weight gain and elevated prolactin level. Mean weight gain for risperidone (3.31 kg) was significantly greater than lithium (1.42 kg) and divalproex sodium (1.67 kg).
Olanzapine
Olanzapine is an SGA that was approved by the FDA in 2008 for the treatment of BD, mixed or manic episodes for ages 13–17 years following a three-week, large (N = 161), multicenter, double-blind, parallel group, randomized, placebo-controlled study for adolescents diagnosed with BD, mixed or manic episode (Tohen et al. 2007). A greater number of participants in the olanzapine group completed the study (79.4%) compared to the placebo group (64.8%). The most common treatment-emergent adverse events were appetite increase, weight gain, somnolence, and sedation. Mean weight gain was significantly greater for participants treated with olanzapine (3.7 kg) compared to placebo (0.3 kg). In addition, clinically significant weight gain (≥7%) was higher for olanzapine-treated participants (41.9%) compared to placebo-treated participants (1.9%). Other olanzapine-related adverse events included elevation of prolactin, fasting glucose, fasting total cholesterol, uric acid, and hepatic enzymes.
Quetiapine
Quetiapine is an SGA that was approved for the treatment of acute manic/mixed episodes in 2009 for children and adolescents 10–17 years of age following one three-week, large (N = 284), randomized, double-blind, placebo-controlled clinical study (Pathak et al. 2013). Participants received quetiapine 400 mg/day in divided doses, quetiapine 600 mg/day in divided doses, or placebo. The YMRS response rates of quetiapine 400 mg/day (55%) and quetiapine 600 mg/day (56%) were significantly higher than the response rate of placebo (28%). The observed effect sizes were 0.54 for quetiapine 400 mg/day and 0.87 for quetiapine 600 mg/day.
The most common adverse events associated with quetiapine treatment were somnolence, sedation, dizziness, and headache. The mean weight gain for the quetiapine 400 mg/day and 600 mg/day treatment groups was 1.7 kg and the mean weight gain for the placebo group was 0.4 kg. Mean increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides were observed more in the quetiapine groups than in the placebo group.
An additional study by Patino et al. (2021) found that quetiapine had a better response rate and was more tolerable than lithium when directly compared in a double-blind, randomized trial. Please refer to the lithium section for further details.
Medications not FDA approved for the treatment of PBD, manic/mixed episodes
Carbamazepine
No RCT for the use of carbamazepine in PBD was identified through a literature search. One study compared the effectiveness of carbamazepine to lithium and divalproex sodium by randomly assigning patients to three open treatment arms (Findling and Ginsberg 2014). In this study, patients improved in all three treatment arms. Carbamazepine performed less well than divalproex sodium and comparable to lithium. No placebo comparison was available. While this study is encouraging, RCTs need to be conducted before carbamazepine can be strongly recommended for the treatment of pediatric bipolar manic/mixed episodes.
Divalproex sodium
DVX is an anticonvulsant FDA approved for the acute treatment of manic/mixed episodes in adult bipolar disorder. However, currently, DVX is not FDA approved for any indication in PBD due to poor efficacy demonstrated in RCTs in pediatric patients with Bipolar Disorder.
In one RCT, divalproex sodium extended release (ER) did not separate from placebo in treating pediatric bipolar mania (Wagner et al. 2009). There was no significant treatment effect on change in primary or secondary efficacy measures. Rates of adverse events were similar. The most common adverse events observed were headache and vomiting. Results of this study did not support the use of DVX ER for the treatment of pediatric bipolar mania. Of note, the conclusions of this study are limited by the fact that measured serum divalproex sodium concentrations were in the range of 77–90 μg/mL, which were below the target range of 80–125 μg/mL.
In 2012, the TEAM study, risperidone, lithium, and divalproex sodium were evaluated as initial treatment for BD, mixed or manic phase (Geller et al. 2012). Divalproex sodium had a significantly lower CGI-BP-I response rate than risperidone. There was no difference in the response rates between divalproex sodium and lithium. The adverse event more common for divalproex sodium compared to lithium and risperidone was difficulty waking up in the morning. Mean weight gain for divalproex sodium was not different from lithium and lower than risperidone. Results of this study appeared to suggest that DVX may be statistically equivalent to lithium for the treatment of acute pediatric bipolar manic/mixed episodes.
Oxcarbazepine
For the overall population (ages 7–18), oxcarbazepine did not separate from placebo in a RCT for treatment of PBD, manic/mixed episodes, as measured by reduction in YMRS scores (Wagner et al. 2006). Of note, in the younger age group (ages 7–12), 41% of patients receiving oxcarbazepine achieved at least 50% reduction in YMRS scores in comparison to 17% of patients receiving placebo. In the adolescent age group (ages 12–18), the response rates were 43% for oxcarbazepine and 40% for placebo. The authors did not report whether the differences in the younger age group were statistically significant.
Topiramate
No RCT was identified for the use of topiramate as monotherapy for the treatment of PBD. A small open-label trial comparing olanzapine to topiramate plus olanzapine did not show differences in effects on symptoms of mania (Wozniak et al. 2009). However, augmentation with topiramate did lead to significantly lower weight gain.
Ziprasidone
A clinical trial was conducted looking at the efficacy and safety of ziprasidone for the treatment of PBD, mania in children and adolescents 10–17 years of age (Findling et al. 2013). There was a significant treatment effect of ziprasidone, measured by change from baseline scores on the YMRS. Fifty-three percent of the ziprasidone-treated participants were considered responders compared to 22% of placebo-treated participants. The most common adverse events in the ziprasidone group were sedation, somnolence, headache, fatigue, and nausea, all of which were more commonly reported by the ziprasidone group compared to placebo.
An independent audit was conducted by request of the FDA and dosing errors were found at three sites. Six participants in the ziprasidone group and four subjects in the placebo group were considered to have “overdosed,” defined as exceeding the total maximum daily dose allowed by the protocol. The independent audit reviewed the data and found that all safety data and 81.4% of efficacy data were reliable. However, due to the errors in the conduct of the trial, the FDA did not issue an indication for using ziprasidone for the treatment of PBD, manic/mixed episodes.
Treatment of depressed episodes
Randomized, controlled trials for the treatment of pediatric bipolar depression were identified for lurasidone, olanzapine-fluoxetine, and quetiapine. An RCT was given a rating of “high” if it did not have important limitations. The GRADEs of these studies can be found in Table 4 and a description of results of each study can be found below. Details on the duration, age of participants, number of study participants, dose of medication, response rate, effect size, average weight gain, and common adverse events can be found in Table 5.
High-Quality Studies for Medications Used in the Treatment of Pediatric Bipolar Disorder, Depression
Randomized Controlled Trials from 2005 to 2021 for the Treatment of Pediatric Bipolar Depressed Episodes
Studies 1–3 included participants diagnosed with bipolar I disorder, depressed episode. Study 4 included participants diagnosed with bipolar I or II disorder, most recent episode depressed.
Response criteria for study 1, 3, and 4: ≥50% decrease in CDRS-R total score from baseline to endpoint. Response criteria for study 2 ≥ 50% decrease in CDRS-R total score from baseline to endpoint and YMRS item 1 score ≤2 at endpoint.
CDRS-R, Children's Depression Rating Scale-Revised; quetiapine XR, quetiapine extended release; YMRS, Young Mania Rating Scale.
FDA-approved medications for the treatment of PBD, depressed episodes
Lurasidone
Lurasidone was approved by the FDA in 2018 for the treatment of pediatric bipolar depression in children and adolescents 10–17 years of age following a RCT of lurasidone for acute treatment of pediatric bipolar depression (DelBello et al. 2017). Three hundred forty-seven participants 10–17 years of age were enrolled in a 6-week randomized, double-blind, placebo-controlled trial comparing lurasidone and placebo. The lurasidone treatment group had a significantly higher response rate (60%) compared to the placebo group (37%). Cohen's d effect size was 0.44. Weight gain was similar for the two groups. The most common adverse events were nausea and somnolence.
Olanzapine-fluoxetine
Olanzapine-fluoxetine was approved for the treatment of depressed episodes associated with PBD in 2013 following an eight-week, large (N = 255), RCT comparing olanzapine-fluoxetine and placebo (Detke et al. 2015). Seventy-eight percent and 59% of participants were considered responders in the olanzapine-fluoxetine group and the placebo group, respectively. The Cohen's d effect size was 0.46. Mean weight gain was significantly greater for the olanzapine-fluoxetine group (5.1 kg) compared to placebo (0.6 kg). The most common adverse events were weight gain, somnolence, hyperlipidemia, elevated hepatic enzymes, elevated prolactin, and QT prolongation.
Medications not FDA approved for the treatment of PBD, depressed episodes
Quetiapine
In a randomized, double-blind, placebo-controlled, large (N = 193) clinical trial of quetiapine extended release (XR) for the treatment of pediatric bipolar depression, there was no significant difference in decrease in depressive symptoms as measured by CDRS-R scores between the placebo and treatment groups (Findling et al. 2014). Sixty-three percent of the quetiapine XR group was considered responders compared to 55% of the placebo group, which was not statistically significant. The most common adverse events in the quetiapine XR group were headache, diarrhea, fatigue, and nausea (Findling et al. 2014).
Before the above RCT, a pilot study was conducted, also examining the efficacy of quetiapine for PBD, depression (DelBello et al. 2009). There was no significant difference between the two groups in CDRS-R scores from baseline to endpoint. Response rates were also not significantly different, with 71% of the quetiapine group and 67% of the placebo group considered responders. The only adverse event with a significant difference between the two groups was dizziness. However, gastrointestinal upset and sedation were also commonly reported in both groups.
Adjunctive treatment
Lamotrigine
Lamotrigine was studied in a discontinuation trial for the treatment of PBD as an add-on medication to one or two concomitant bipolar disorder medications (Findling et al. 2015a). The first phase of the study was open-label treatment to stabilize participants on adjunctive lamotrigine. The most common concomitant bipolar disorder medication was aripiprazole. In phase 1, 301 children and adolescents 10–17 years of age, currently experiencing a manic/hypomanic, depressed, or mixed mood episode, were enrolled. Participants who maintained a stable dose of lamotrigine for at least 2 weeks and had a CGI-BP-S score ≤3 for at least 6 weeks were considered to be in remission and were eligible to be randomized into phase 2, a randomized, placebo-controlled, double-blind phase.
In phase 2, 173 participants were randomized to either lamotrigine or placebo. The primary endpoint in the randomized phase of the study was time to occurrence of bipolar event (TOBE). A bipolar event was defined as occurrence of one of the following: intervention was required to treat the emergence or change in manic/hypomanic, depressive, or mixed symptoms, the patient withdrew due to a bipolar-related adverse event or serious adverse event, or the patient withdrew because of a lack of efficacy. A secondary endpoint was time from randomization to intervention for a mood episode (TIME), which was calculated for the subgroup of participants who experienced a bipolar event and required intervention. For the overall population, the primary outcome (TOBE) was not significantly different from placebo. However, a secondary endpoint (TIME) was significantly improved by lamotrigine for the overall population.
In addition, in post hoc analyses, lamotrigine lengthened time to relapse on both measures (TOBE and TIME) for the 13- to 17-year-old age group. As youth with both manic/hypomanic, depressed, and mixed mood episodes were enrolled, these results indicate that lamotrigine can be a useful adjunct medication for multiple types of bipolar episodes in adolescents. The most common adverse events were headache, upper abdominal pain, nausea, and oropharyngeal pain.
Nonpharmacological treatments
Family-focused therapy (FFT) is the most studied form of psychotherapy for PBD (Miklowitz et al. 2008, 2013, 2014, 2020a, 2020b; Lunsford-Avery et al. 2012; O'Donnell et al. 2020). In RCTs comparing psychoeducation to FFT, patients who received FFT showed improvements in time to depressive episodes (Miklowitz et al. 2020b), family cohesion (O'Donnell et al. 2020), rate of recovery from baseline depressive symptoms (Miklowitz et al. 2008), and longer intervals without suicidal behaviors (Miklowitz et al. 2020).
Bright light therapy has not been studied in PBD. However, in adults with bipolar depression, bright light therapy resulted in significant decrease in depressive symptoms (Sit et al. 2018; Wang et al. 2020). Considering the low cost and low side effect burden, bright light therapy could be considered an adjunct treatment for patients with PBD, depressed episodes.
Several small studies in children and adults with bipolar depression showed that O3FA supplementation may be useful in improving depressive symptoms, while administered in conjunction with other treatments (Montgomery and Richardson 2008; Osher and Belmaker 2009; Fristad et al. 2015; Wozniak et al. 2015). However, a recent review by Nasir and Bloch (2019) notes substantial methodological shortcomings in studies of O3FAs in psychiatric disorders in adults. The authors caution against the use of O3FAs since using ineffective treatments, no matter how benign, carries an opportunity cost (e.g., medications with proven efficacy not being utilized) and could reduce patient compliance with evidence-based treatments.
Options for treatment-resistant PBD
Clozapine
At this time, clozapine is FDA approved for treatment of adults with refractory schizophrenia and for reducing suicidal behavior in adults with schizophrenia or schizoaffective disorder. Safety and efficacy of clozapine in pediatric patients have not been established. There is no RCT for the use of clozapine for the treatment of PBD.
Despite lack of research, clozapine is frequently used in treatment-resistant PBD with psychotic symptoms. A recent multicenter retrospective chart review of hospitalized pediatric patients in the United States and Australia identified 82 patients who were started on clozapine while in the hospital. On average, these patients failed 3.5 antipsychotics before receiving clozapine treatment. Twenty-five percent of patients in this study had bipolar disorder. A majority of patients showed significant (31.7%) or moderate (32.9%) improvement on clozapine (Steinauer et al. 2018).
Statistically significant improvement in CGI scores was seen in a case series of 10 children (6–15 years old) who were treated with clozapine (Kowatch et al. 1995). Five of these patients had PBD and all failed multiple medication trials. Clozapine was particularly effective in reducing aggression and psychosis (Kowatch et al. 1995).
A limiting factor for the use of clozapine in children and adults is the frequency and severity of side effects. While clozapine is less likely to cause EPS than other antipsychotics, it carries risks of several serious, and potentially life-threatening side effects, such as agranulocytosis, myocarditis, seizures, and diabetes mellitus (Kapur and Mamo 2003; Nucifora et al. 2017).
Electroconvulsive therapy
ECT is currently classified by the FDA as a class II device for the treatment of bipolar depression in adolescents 13 years of age and older, who are “treatment resistant or who require a rapid response due to the severity of their psychiatric or medical condition” (Food and Drug Administration 2018). These regulations are equivalent to the “on-label” uses of drugs (Espinoza and Kellner 2022).
Currently, there is no RCT for the use of ECT in PBD. Several retrospective chart review studies suggest that ECT is a safe and effective treatment for treatment-resistant depression, mania, and catatonia in PBD (Puffer et al. 2016).
Puffer et al. (2016) identified 51 adolescents, 12–19 years of age, who received ECT. Three patients in this study were diagnosed with bipolar affective disorder manic/mixed. The most common diagnosis in this study was major depressive disorder (N = 21). Following acute treatment, 77% of patients were rated as much or very much improved on the CGI-I.
Ghaziuddin et al. (2020) reviewed charts of 54 adolescents who received ECT. Eighteen patients had a primary diagnosis of bipolar disorder. Response was achieved by 52.8% of cases after index treatment. The most reported adverse event was headache (77%), followed by memory loss (66%) and fatigue (62%).
Pierson et al. (2021) reviewed charts of 107 adolescents who received ECT for PBD (23 patients), major depressive disorder (MDD), psychotic disorder, catatonia, or neuroleptic malignant syndrome. The overall response rate was 77%. This study found that patients with depression (MDD or BD) had a response rate of 74% and patients in a manic/mixed episode had a response rate of 88%. The most common adverse events reported were headache (75%), memory problems (65%), nausea/vomiting (50%), and muscle soreness (29%).
Algorithms for the acute treatment of pediatric bipolar manic/mixed episodes, without psychosis, with psychosis, and pediatric bipolar depressive episodes
These algorithms are intended to summarize current evidence to guide decision-making with regard to treatment of acute episodes of PBD (Figs. 1 –3). Current research into the maintenance treatment of PBD is summarized elsewhere (Dorfman and Robb 2016). Clinicians should consider patient variables, while making treatment decisions and not use these guidelines rigidly. There is a paucity of evidence regarding augmentation strategies in PBD. Therefore, when research was lacking, we based our recommendations on principles of rational polypharmacy summarized in the methods section.

Pediatric bipolar disorder, manic/mixed episodes without psychosis.

Pediatric bipolar disorder, manic/mixed episodes with psychosis.
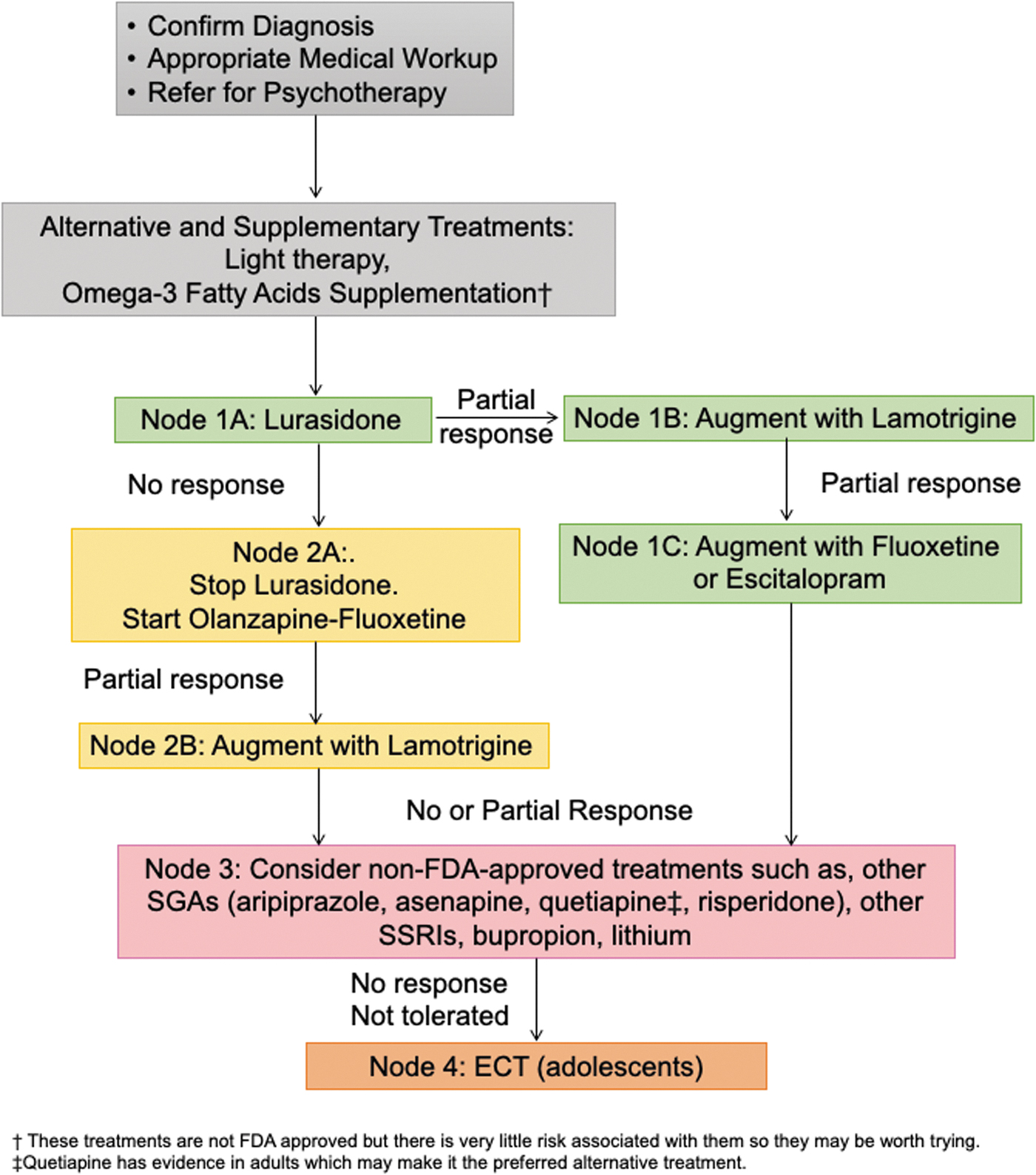
Treatment algorithm for pediatric bipolar disorder, depressive episode.
Before initiating medication, a clinician should firmly establish diagnosis of Bipolar disorder by integrating information obtained from diagnostic interview, family history, trauma history, collateral information, and possibly including a medical workup and genetic screening to rule out medical causes of emotional dysregulation, especially in the presence of psychotic symptoms. Most patients and families can benefit from a referral to psychotherapy early in the course of treatment for PBD.
Algorithm 1 treatment of acute manic/mixed episodes without psychosis
Node 1A
The first line of treatment for an acute manic/mixed episode without psychosis is monotherapy with an FDA-approved SGA (aripiprazole, asenapine, olanzapine, quetiapine, or risperidone) (Fig. 1). The choice of SGA can be tailored to the needs of the individual patient based on side-effect profile and efficacy evidence, which is summarized in Table 2.
Node 2A
If there is no response or the initial SGA is not tolerated, we recommend switching to monotherapy with another FDA-approved SGA.
Node 2B
If the SGA is well tolerated and partial response is achieved, but better control of symptoms is desired, the clinician can augment SGA treatment with lithium.
The recommendation to use lithium as augmentation agent is due to its unique neuroprotective (Ochoa 2022) and antisuicidal properties (Lewitzka et al. 2015; Hafeman et al. 2020). In addition, lithium can be continued as a maintenance medication once acute episode is resolved and the SGA can be tapered off to avoid metabolic adverse events. The strategy of augmenting SGA with lithium has not been studied in RCTs. However, this combination is frequently and successfully used in clinical practice and does not violate principles of rational polypharmacy. Despite unique positive attributes of lithium, we do not recommend lithium as a first-line monotherapy for an acute manic/mixed episode in PBD due to its lower efficacy in comparison to SGAs.
Node 3A
If there is no response to the second SGA, the SGA should be discontinued, and a trial of lithium initiated. SGAs are recommended as first-line treatment because they were shown to have higher efficacy than lithium in multiple RCTs (Geller et al. 2012; Patino et al. 2021). Both SGAs and lithium have significant side effect burden. However, lithium has fair efficacy for manic/mixed episodes and therefore is a reasonable alternative to try if SGAs failed, were not tolerated, or did not produce sufficient response.
Node 3B/3C/3D
Augmentation with lamotrigine was shown to significantly delay time to recurrence of bipolar mood episodes, for adolescents more than children (Findling et al. 2015a). Lamotrigine is well tolerated, but requires slow titration to minimize the risk of Stevens-Johnson Syndrome. Therefore, lamotrigine is recommended as an augmentation strategy in combination with an SGA and/or lithium.
Node 4
If lithium and lamotrigine are not tolerated, an SGA can be augmented with second-line agents such as divalproex, carbamazepine, or oxcarbazepine. Second-line agents are medications that are commonly used in adults with bipolar disorder and were previously recommended in the AACAP 2005 algorithm. However, they are not FDA approved for PBD and do not currently have good evidence of efficacy in the pediatric population. If FDA-approved SGAs and lithium were not tolerated, consider monotherapy with second-line agents listed above or ziprasidone, which showed good efficacy in an RCT, but was not approved due to concerns over the conduct of the study (Findling et al. 2013).
Node 5
Patients who are treatment resistant to interventions discussed above can be considered for ECT or clozapine. Refer to the discussion of ECT and clozapine in the article above.
Algorithm 2 treatment of acute manic/mixed episodes with psychosis
For patients presenting with psychosis, in addition to manic/mixed symptoms, we suggest that SGAs should be used as core treatment with other classes of mood stabilizers acting as augmenting agents (Fig. 2). This recommendation is based on the recognition of the fact that antipsychotic medications are best suited to treating psychotic symptoms. In addition, the RCT conducted by Geller et al. (2012) found that a higher proportion of participants presenting with psychosis in an acute manic/mixed episode of PBD responded to risperidone compared to lithium or divalproex sodium.
Node 1A
The first line of treatment for an acute manic/mixed episode with psychosis is monotherapy with an FDA-approved SGA (aripiprazole, asenapine, olanzapine, quetiapine, or risperidone). The choice of SGA can be tailored to the needs of the individual patient based on side-effect profile and efficacy evidence, which is summarized in Table 2.
Node 2A
If there is no response, or the initial SGA is not tolerated, we recommend switching to monotherapy with another FDA-approved SGA.
Node 2B/3A/3B
If the SGA is well tolerated and partial response is achieved, but better control of symptoms is desired, the clinician can augment SGA treatment with lithium and/or lamotrigine.
Node 4
If lithium and lamotrigine are not tolerated or additional augmentation is needed, second-line agents such as divalproex, carbamazepine, or oxcarbazepine can be considered. These medications are commonly used in adults with bipolar disorder and were previously recommended in the AACAP 2005 algorithm. However, they are not FDA approved for PBD and do not currently have good evidence of efficacy in the pediatric population.
Node 5
For patients who fail two or more SGAs, treatment with ECT or clozapine can be considered.
Algorithm 3 treatment of depressive episodes
Low-risk supplementary treatments, such as light therapy (Sit et al. 2018; Wang et al. 2020) and O3FAs (Montgomery and Richardson 2008; Osher and Belmaker 2009; Wozniak et al. 2015), can be recommended early in the course of treatment, in addition to psychotherapy and pharmacotherapy, for patients who are interested in supplementary therapies (Fig. 3). It should be emphasized that these treatments cannot replace psychopharmacology, but might be able to augment it.
Node 1A
Lurasidone is a first-line treatment for PBD, depression. While lurasidone and olanzapine-fluoxetine combination (OFC) are both FDA approved and have similar efficacy, with effect sizes of 0.45 and 0.46, respectively, lurasidone appears to have a significantly lower metabolic side effect burden relative to OFC (Detke et al. 2015; DelBello et al. 2017).
Node 1B
If treatment with lurasidone resulted in a partial response, it can be augmented with lamotrigine.
Node 1C
If depressed symptoms are still present with the addition of lamotrigine to lurasidone, a selective serotonin reuptake inhibitor (SSRI) that is FDA approved for pediatric MDD, such as escitalopram or fluoxetine, can be added. Addition of an SSRI can precipitate a manic switch. Therefore, it should be done with careful monitoring and only in combination with a mood-stabilizing agent.
Node 2A
If lurasidone resulted in treatment failure, we recommend cross tapering to OFC. OFC is clinically underused, despite available evidence of efficacy and FDA approval for pediatric bipolar depression. Weight gain and metabolic changes associated with OFC could be reduced by the addition of topiramate (Wozniak et al. 2009) and careful diet and lifestyle management. In addition, OFC can be tapered off once acute episode is resolved and replaced by another mood-stabilizing agent.
Node 2B
If there is a partial response to OFC, augment with lamotrigine.
Node 3
If FDA-approved treatments have failed, consider non-FDA-approved treatments such as quetiapine, aripiprazole, asenapine, risperidone, other SSRIs, bupropion, and lithium. SSRIs should only be used in combination with mood-stabilizing agents to reduce the risk of manic switch. Quetiapine is FDA approved for adult bipolar depression. However, quetiapine failed to separate from placebo in two RCTs in children and adolescents. Therefore, even though it is not a first-line medication, quetiapine is a reasonable choice to try for an older adolescent with bipolar depression.
Node 4
For patients who fail two or more SGAs, treatment with ECT can be considered.
Discussion
This article reviews evidence from 2005 to 2021 for the psychopharmacological treatment of PBD, acute manic/mixed and depressive episodes. Based on this evidence, we updated the AACAP 2005 algorithms for the treatment of PBD, acute manic/mixed episodes, and proposed a novel evidence-based algorithm for the treatment of pediatric bipolar depression. The algorithms presented in this article prioritize FDA-approved treatments and medications that showed efficacy in RCTs.
The AACAP algorithms for treatment of acute mixed/manic episodes of PBD that were published in 2005 were primarily based on adult data and open-label studies. However, adult findings cannot be safely generalized to children and adolescents. For example, while quetiapine separated from placebo in the treatment of bipolar depression in adults, it did not separate from placebo in children (DelBello et al. 2009; Findling et al. 2014). Similarly, divalproex sodium, which is a highly effective medication for manic/mixed episodes in adults, did not separate from placebo in studies of pediatric manic/mixed episodes (Wagner et al. 2009). Other medications included in the AACAP algorithm, such as topiramate and carbamazepine, still do not have RCTs showing efficacy in children.
In the current algorithms for the treatment of acute manic/mixed episodes, we propose SGAs as the first-line treatment, with the choice of a specific agent left up to clinician's judgment. This recommendation is based on consistently superior efficacy of SGAs in comparison to other agents in RCTs for the treatment of mixed/manic episodes in PBD. However, once patient is stabilized, other medications might be considered. Currently, lithium is one of two medications with an FDA indication for maintenance treatment of PBD. In addition, there is evidence that lithium might provide neuroprotective and antisuicidal benefits.
Therefore, to minimize adverse metabolic side effects of SGAs in vulnerable patients, clinician might consider initiating lithium and tapering off SGAs for long-term maintenance treatment of PBD. This strategy might be particularly pertinent for risperidone and olanzapine, both highly effective agents for the treatment of acute manic/mixed episodes, but associated with high risk of weight gain and metabolic changes with long-term use. Detailed discussion of maintenance treatment of PBD is outside the scope of this article and can be found elsewhere (Dorfman and Robb 2016).
In 2005, at the time of publication of AACAP algorithm, there was no FDA-approved agent available for the treatment of bipolar depression. Now we have two agents, lurasidone and OFC, which were FDA approved based on positive results in well-conducted RCTs in pediatric patients. Clinically, both agents are currently underutilized. Although lurasidone and OFC demonstrated similar efficacy for pediatric bipolar depression in RCTs, lurasidone is recommended as a first-line treatment due to its more favorable side-effect profile compared to OFC. For patients who did not respond to lurasidone, OFC should be considered the next evidence-based choice before off-label medications are attempted.
There are limitations to the algorithms presented in this article. First, the proposed algorithms heavily prioritize RCT data and FDA guidelines and are not based on a systematic meta-analysis. Second, the scope of this article is limited to the treatment of acute episodes of PBD and not for maintenance treatment, even though PBD is a lifelong illness that requires long-term, even life-long, medication management. Third, potentially useful agents might have been overlooked due to lack of high-quality evidence.
Some of these medications are currently used off-label (e.g., ziprasidone, carbamazepine, cariprazine, buproprion, etc.). At this time, cariprazine is being actively investigated for PBD. Unfortunately, an open-label study of bupropion for PBD was terminated due to a lack of recruitment. Finally, evidence for treatments of pediatric bipolar depression is currently lagging. Currently, there are only two FDA-approved agents for this indication and one promising augmentation agent (lamotrigine). Therefore, our algorithms provide a snapshot of best-available research at this time. They are intended to be updated as new research becomes available. We encourage clinicians to not only use these algorithms as a guide but also to incorporate their clinical judgment and experience to individualize treatment to each patient.
Most of the advancements in the treatment of acute PBD have come from conducting RCTs and open-label trials of efficacy of medications already used for adult bipolar disorder. The majority of these agents were developed before 2005. Only two novel medications (lurasidone and asenapine) were developed since the 2005 AACAP algorithm. Both of those agents are SGAs and therefore their mechanisms of action and side effect profiles are similar to those of other existing treatments.
Evidence from structural and functional neuroimaging suggests that the brain undergoes significant developmental changes during puberty (Paus et al. 2008; Ernst et al. 2015; Casey et al. 2017; Vijayakumar et al. 2018). These changes might lead to differential sensitivity to psychopharmacological agents before and after puberty. In fact, several agents showed differences in efficacy in children versus adolescents. For example, lamotrigine is more efficacious in adolescents (Findling et al. 2015a) and oxcarbazepine might be more efficacious in younger age group (Wagner et al. 2006). Therefore, more tailored approach might be needed toward children versus adolescents in both research and clinical care of psychiatric disorders.
Despite these limitations, we hope that the algorithms presented in this article can provide a user-friendly guide to clinicians treating acute PBD, manic/mixed and depressive episodes. Marked progress has been made in the last 20 years in our understanding of the psychopharmacological treatment options for PBD, and we look forward to additional advances to come.
Footnotes
Authors' Contributions
E.H.: writing—original draft. R.R.: writing—original draft. B.L.: writing—reviewing and editing. A.R.: writing—reviewing and editing, and supervision. J.D.: writing—original draft, supervision, and conceptualization.
Disclosures
No competing financial interests exist. A.R. reports the following: Actavis/Forest Laboratories (consultant, research support); AACAP (honorarium and travel support); AAP (honorarium, Bracket (consultant); Eli Lilly (stock in ira); GlaxoSmithKline (stock in ira); Johnson & Johnson (stock in ira); Lundbeck/Takeda (advisor and research support); Neuroscience Education Institute (honorarium and travel support); National Center for Advancing Translational Sciences (research support); NICHD (advisor); NIMH (data safety monitoring board and research support); NACCME (honorarium and travel support); Pfizer, Inc. (stock/equity); Sunovion Pharmaceuticals, Inc. (advisor and travel support); Supernus Pharmaceuticals, Inc. (research support and advisor); and SyneuRx (research support).