
Abstract
Objective:
Increased mental health problems among children and adolescents during the COVID-19 pandemic may have impacted psychotropic medication use. This study describes trends in monthly psychotropic medications before and early in the COVID-19 pandemic among 2- to 17-year-old children and adolescents with mental health disorders.
Methods:
A cross-sectional study design using the 2019–2020 IQVIA™ prescription and medical commercial claims data to estimate the proportion of children and adolescents with any psychotropic prescription in the month out of all with any mental health-related medical or prescription services in the month and the year-over-year percent change. We assessed monthly proportions of youth who filled a psychotropic prescription overall and by psychotropic class, stratified by age and gender.
Results:
Of the 8,896,713 children and adolescents in the sample, 24.7% received psychotropic medication during the study period. The proportion of the cohort prescribed a psychotropic medication in a given month averaged 27%–28% from January 2019 to February 2020, peaked at 36.9% in April 2020, and gradually declined to 28.7% in September 2020. The largest year-over-year percent change was in April for antipsychotic (41.9%) and antidepressant (37.9%) medication, which remained higher in September 2020 compared to September 2019, particularly among ages 6 years or older and females.
Conclusion:
The proportion of youth with a psychotropic prescription increased at the onset of the COVID-19 pandemic, later returning to prepandemic levels. However, antipsychotics and antidepressants remained higher than prepandemic, highlighting the need to further understand the long-lasting effects of the pandemic on children and adolescents.
Introduction
The COVID-19 pandemic imposed social isolation, an economic recession, and a public health crisis that had a devastating effect on children's mental health. For children and adolescents with psychiatric disorders, the difficulty of coping with lockdown may worsen existing mental health problems (Golberstein et al, 2020; Guessoum et al, 2020) or increase their risk for posttraumatic stress disorder, depression, and anxiety (Guessoum et al, 2020). Disruption to the daily structure and COVID-19 restrictions (e.g., social distancing) can lead to frustration and intensify mood and behavioral problems (Guessoum et al, 2020).
Following the isolation and confinement of stay-at-home orders and school closures, elevated psychiatric symptoms (Aman and Pearson, 2020; Fegert et al, 2020; Guessoum et al, 2020) and increased mental health-related emergency department (ED) visits (Leeb et al, 2020; Ridout et al, 2021; Yard et al, 2021), and hospitalizations were observed (Gill et al, 2021; Krass et al, 2021; Reece and Sams, 2022). Still, it remained higher for females, youth 12–17 years old, and those diagnosed with suicide and depressive disorders (Leeb et al, 2020; Zima et al, 2022). Although these shifts in mental health-related care services are broadly documented, less is known about the changes in psychotropic medication dispensing during this period of confinements and lockdowns.
The public health restrictions to prevent COVID-19 exposure and transmission limited access to needed care for many children in the United States (Torres-Pagán and Terepka, 2020). School closure during lockdown meant 13%, or 3 million youth, did not have access to school mental health services (Golberstein et al, 2020). Of the youth who receive mental health services, 57% receive some school-based mental health services, and 35% receive mental health services exclusively in school (Golberstein et al, 2020). Limited space for social distance requirements meant that fewer patients could be seen, leading to long wait times and reduced access to mental health care providers and psychotherapy (Fegert et al, 2020; Rubin, 2020).
These major shifts in access to services during the COVID-19 pandemic may have changed psychotropic medication use patterns among children and adolescents. Pharmacies operated as an essential service during the pandemic, and medication was a readily accessible mental health treatment. However, evidence of changes in psychotropic prescriptions during the pandemic is scarce. This study's overall objective was to describe trends in the proportion of U.S. children and adolescents with psychotropic prescription before and early in the COVID-19 pandemic. We describe the monthly proportion of children and adolescents receiving mental health services who were prescribed psychotropic medication, overall and by class, and examine changes in use by age and gender.
Methods
Study design and data sources
In a cross-sectional design using the IQVIA™ longitudinal prescription and medical claims data, we evaluated psychotropic medication trends from January 1, 2019, through September 30, 2020. The data were provided as part of the IQVIA Human Data Science Research Collaborative (IQVIA, 2022) to support research on the health system impact of the COVID-19 pandemic. Under this program, data were made available up through September 2020. The prescription claims data cover over 90% of retail pharmacies, 60%–85% of mail-order pharmacies, and 75%–80% of long-term care, and provide information on the medication name and strength, the date dispensed, quantity dispensed, and the days of supply. The medical claims data include all outpatient and inpatient care with patient-level information on diagnoses and procedures.
A unique and masked identifier enabled the linkage of medical and prescription claims to create a person-level analytic file. The study was deemed nonhuman subjects research by the University of Maryland Baltimore Institutional Review Board. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies (von Elm et al, 2007).
Study sample
The study sample of children and adolescents aged 2–17 was selected among all who had at least one claim during the study period with (1) an International Classification of Disease 10th Revision (ICD-10) code for a psychiatric disorder, (2) a Current Procedural Terminology (CPT) or Healthcare Common Procedure Coding System (HCPCS) code for a mental health service (e.g., 90832 for psychotherapy), or (3) a pharmacy claim for a psychotropic prescription dispensing (Supplementary Table S1). The IQVIA Human Data Science Research Collaborative applied the selection criteria to generate the final analytic cohort. All medical and mental health claims for the analytic cohort were included in the data provided.
Psychotropic medication classification
Psychotropic medications from the four classes most commonly prescribed for children and adolescents were included in this study (dosReis et al, 2020; Jonas et al, 2013; Sultan et al, 2018). The four classes are (1) stimulant and nonstimulant attention-deficit/hyperactivity disorder (ADHD) medications (i.e., clonidine, guanfacine, atomoxetine), (2) antidepressants (selective serotonin reuptake inhibitors, e.g., sertraline, fluoxetine; serotonin-norepinephrine reuptake inhibitors, e.g., duloxetine, venlafaxine; and other medication, e.g., bupropion), (3) antipsychotics (first and second-generation), and (4) mood stabilizers (e.g., lithium, carbamazepine) (Supplementary Table S2). We excluded anxiolytics from this analysis since these were prescribed in <1% of the sample. We categorized individual medications into these psychotropic classes using the American Hospital Formulary System (AHFS, 2020).
Measure of monthly psychotropic prescription
We estimated the proportion of children and adolescents in each month who were prescribed a psychotropic medication (i.e., monthly psychotropic prescription) from January 2019 through September 2020, overall, and for each psychotropic class. We calculated overall monthly psychotropic prescription as the number of children and adolescents with any psychotropic prescription claim in the month divided by the total number of children and adolescents in the cohort with any service or prescription claim in the same month. We use the same approach to estimate the monthly psychotropic class prescription.
Data analysis
Descriptive statistics characterized the study sample overall, that is, those with any mental health diagnosis or psychotropic prescription, and the subgroup of those who received at least one psychotropic medication. We used graphs to display trends in monthly prescribed psychotropic medication, overall and for each psychotropic class (i.e., ADHD medications, antidepressants, antipsychotics, and mood stabilizers). Graphical display of the year-over-year percent change in monthly prescribed psychotropic class and stratified by gender and age groups (i.e., 2–5, 6–11, and 12–17 years old) illustrated changes after the COVID-19 pandemic, accounting for potential seasonal variations.
Statistical significance of the percent change in monthly psychotropic prescription in the period before relative to the period during the COVID-19 pandemic (i.e., January to September in 2019 vs. 2020) was evaluated by a Z test for two proportions, two-sided, and a p < 0.05 (Akritas, 2019). All analyses were performed using SAS 9.4 (SAS Institute, Inc., 2017), and graphs were created using R ggplot2 (Holtz, 2021; Wickham et al, 2016).
Results
Sample characteristics
A total of 8,896,713 children and adolescents had at least one medical or prescription claim with a psychiatric diagnosis, mental health-related procedure, or psychotropic medication at any time from January 2019 through September 2020 (Table 1). Most were school-age children 6–17 years old (86.4%), and just over half were male (51.5%). Of these youth, 2,200,694 (24.7%) received a psychotropic medication at some point during the study period. The proportional distribution of 12- to 17-year-olds and males was slightly higher in the psychotropic-treated subsample than in the overall sample (Table 1).
Characteristics of Children and Adolescents Receiving Mental Health Services for the Overall Sample and the Subsample Who Received Psychotropic Medication
The total number of females and males is 5,347 less than the overall sample because of missing values in the data.
Number of beneficiaries who received any mental health service or prescriber medication in the calendar year and the percent of the overall sample or the psychotropic-treated sample.
The number of children and adolescents with any mental health care, either a medical service or psychotropic prescription, in a month ranged from 3,866,980 (October 2019) to 2,471,444 (April 2020). The number of children and adolescents who had any mental health-related care in January and February was similar for 2019 and 2020. However, the monthly numbers of those who received any mental health-related care from March through September 2020 were lower than prepandemic levels (Supplementary Table S3).
Trends in monthly psychotropic prescription
The overall monthly proportion of children and adolescents prescribed psychotropic medications is illustrated in Figure 1. The monthly proportion prescribed a psychotropic medication averaged around 27%–28% from January 2019 to February 2020, peaked at 36.9% in April 2020, and gradually declined to 28.7% in September 2020 (Fig. 1 and Supplementary Table S3). The year-over-year percent change shows a generally higher psychotropic prescription in 2020 than in 2019 (including in the prepandemic months of January and February), except for September 2020 (−0.3% change), suggesting lower use in 2020 relative to 2019. Relative to the same months in 2019, psychotropic prescription was 10% higher in March 2020 and 26.9% higher in April 2020.
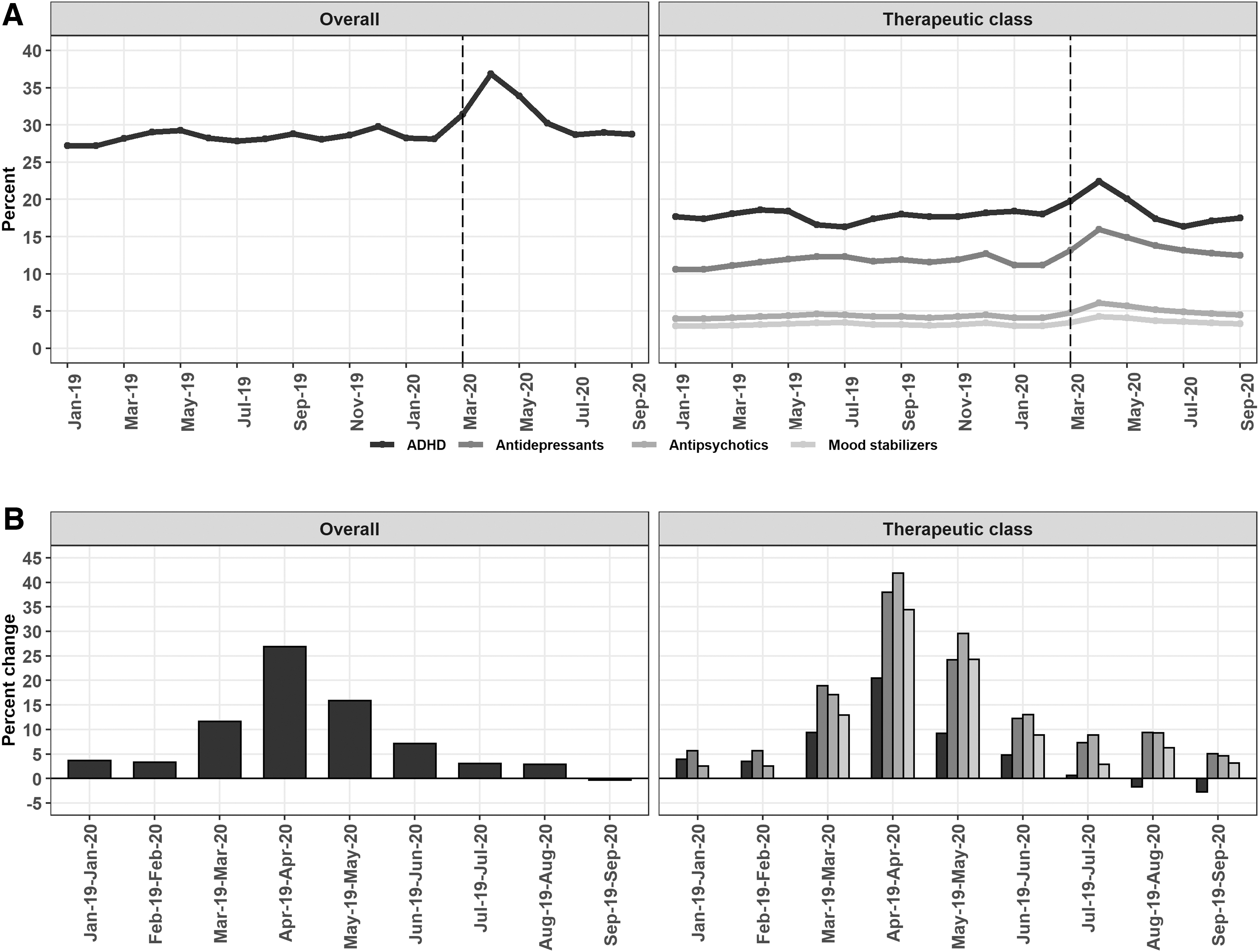
Monthly proportion of psychotropic use and YoY percent change by therapeutic class, 2019–2020.
Monthly trends for each psychotropic class followed similar patterns to overall psychotropic prescription (Fig. 1 and Supplementary Table S4). For children and adolescents with any mental health-related care after the pandemic onset, prescription for all four psychotropic classes increased in April 2020, with the largest for ADHD medications (22.4%), followed by antidepressants (16.0%), antipsychotics (6.1%), and mood stabilizers (4.3%). When comparing April 2020 to April 2019, antipsychotics had the largest year-over-year percent change (41.9%), followed by antidepressants (37.9%), mood stabilizers (34.4%), and ADHD medications (20.4%). In September 2020, where the actual number of youths receiving care was similar to prepandemic levels, the year-over-year percent change in ADHD medication prescription decreased −2.8%, while other psychotropic classes increased between 3.1% and 5.0% compared to September 2019.
Psychotropic trends by age and gender
Monthly trends for each psychotropic class are shown by age group and gender (Fig. 2, Supplementary Fig. S2, and Supplementary Tables S5–S8). Monthly psychotropic prescription was highest for children and adolescents ages 6–11 and 12–17 years relative to those aged 2–5 years (Fig. 2 and Supplementary Fig. S1). Trends in antipsychotic and mood stabilizer monthly prescription were similar for ages 6–11 and 12–17 years, whereas ADHD medication prescription was higher among 6- to 11-year-olds. Antidepressant prescription was higher among 12- to 17-year-olds.

Monthly proportion of psychotropic use and YoY percent change by therapeutic class and age, 2019–2020.
The year-over-year percent change in monthly psychotropic class prescription illustrates higher levels in April 2020 relative to April 2019 for all ages, except for antidepressant among 2- to 5-year-olds, which had very little change (2.6%). Monthly antidepressant prescription among 2- to 5-year-olds was lower January to September 2020 relative to the same period in 2019. The percent change in all psychotropic classes was similar for ages 6–11 and 12–17 years. Antidepressant, antipsychotic, and mood stabilizer prescription was 35%–45% higher in April 2020 relative to April 2019.
Notably, the percent change in antipsychotic prescription was large for all age groups with 37.4% (2–5 years old), 42.8% (6–11 years old), and 39.7% (12–17 years old). Despite the decline in monthly prescription after April 2020, antidepressant and antipsychotic prescription in September 2020 remained higher than in the prepandemic months for school-age children 6–17 years old; by comparison, ADHD medication prescription was lower in September 2020 relative to prepandemic levels.
The gender-stratified analysis (Supplementary Fig. S2) shows trends similar to the overall and age-stratified analysis, except for two psychotropic classes. The monthly proportional prescription of ADHD medications was higher among males, whereas the monthly proportional prescription of antidepressants was higher among females. The gender-stratified year-over-year percent change was similar to that observed for the entire sample and the age-stratified analysis, with the largest year-over-year percent change for antipsychotics (i.e., 45.6% for females and 40.4% for males).
Discussion
Psychotropic prescription among a cohort of privately insured U.S. children and adolescents who received mental health care increased sharply in April 2020, shortly after the onset of the COVID-19 public health emergency, but gradually decreased in the months following. The year-over-year change from 2019 to 2020 was greatest for antipsychotics, antidepressants, and mood stabilizers. Antipsychotic and antidepressant prescription remained higher in September 2020 relative to September 2019, suggesting that the increase observed after the pandemic did not return to baseline despite the number of youths who received any mental health-related care almost returning to prepandemic levels by September. Antipsychotic and antidepressant prescription was similar for children 6–11 years old and adolescents 12–17 years old, suggesting a broad impact of the pandemic for all school-age children.
Reports of pharmacy prescription dispensing data during the COVID-19 pandemic in the United States, which were highest in March/April 2020 and decreased through July 2020 (Chua et al, 2021; Rabeea et al, 2021), corroborate our person-level estimates for a cohort of children and adolescents with a mental health disorder. On the contrary, investigators who examined psychotropic medication dispensing for youth population in Manitoba did not report significant changes in quarterly prescription (Leong et al, 2022).
This study adds new context to the concerns about the rise in children's mental health services during the pandemic by describing the changes in psychotropic medication prescription. Our finding that antipsychotics and antidepressants had the largest year-over-year increase suggests that a larger proportion of children and adolescents who sought mental health care after the pandemic onset used psychotropic medication than the proportion who sought mental health care in 2019. Furthermore, the increased proportion of youth prescribed these medications did not return to prepandemic levels in August and September 2020. This finding might be explained by the increased mental health-related ED visits and hospitalizations during the fall months, particularly for suicide (12.8%) and psychotic disorders (10.8%) (Leeb et al, 2020; Zima et al, 2022). Further research should determine whether children and adolescents with ED visits or hospitalizations also account for those prescribed antipsychotics or antidepressants later in 2020.
The number of children and adolescents who received any mental health care in 2020 decreased, suggesting that those who received care may have had more acute emotional and behavioral distress by the pandemic. However, we also found that the number of children and adolescents who received any psychotropic medication also declined (e.g., 10.5% and 14.6% fewer in April and May 2020, respectively, relative to 2019). In September 2020, despite the similar number of children who received mental health care relative to September 2019, the proportion prescribed psychotropic medication was higher than prepandemic levels, which could indicate a greater need for treatment. Further study is warranted to determine how psychotropic patterns were influenced by the decline in mental health-related visits.
Psychotropic medication may have played a critical role in managing the increase in mental health symptoms experienced by children and adolescents (Guessoum et al, 2020) at the onset of the COVID-19 pandemic. However, mood stabilizers and antipsychotic use among children 6–11 years old during the pandemic relative to prepandemic is counter to national efforts to decrease antipsychotic medication prescription among children (Harrison et al, 2012; Spence et al, 2020). Given the safety concerns with antipsychotic use among children and adolescents (Bobo et al, 2013; Burcu et al, 2017), it will be important to monitor the potential long-term effects of the pandemic on antipsychotic use.
Our study has several limitations. Psychotropic prescription was identified based on claims, which may not fully reflect actual medication consumption. While we evaluated psychotropic prescription by age and gender, other important variables such as income, race, and ethnicity were not available from the data, which limited the evaluation of psychotropic prescription by other sociodemographic characteristics. Future research to identify social and clinical determinants of the observed patterns is needed to better understand the pandemic's impact on future trends of use and outcomes.
Data were available through September 2020, and so it was not possible to determine changes throughout the pandemic. We were unable to examine concurrent psychotropic prescriptions because the data structure provided under the IQVIA Human Data Science Collaborative did not include the actual dispensing date, just the month and year of the dispensing. We felt such an analysis would introduce measurement error, which would be misleading and problematic. Finally, the data represent privately insured children and adolescents and may not generalize to Medicaid enrollees or those without health insurance.
Conclusion
In this study of privately insured U.S. children and adolescents with mental health disorders, prescribed psychotropic medication was higher at the onset of the COVID-19 pandemic relative to prepandemic, and this varied by psychotropic class. The increase in antipsychotic, antidepressant, and mood stabilizer prescription provides additional context about the rise in child and adolescent emotional and behavioral problems during the pandemic. For privately insured children and adolescents with mental health disorders, the observed changes in prescribed psychotropic medication during the current pandemic may provide insight into the need for preventive measures in the event of future public health crises or periods of disruption to daily life.
Clinical Significance
The sustained increase in prescribed antipsychotics and antidepressants following the COVID-19 public health emergency suggests a greater need for treatments to manage child and adolescent mental health. This sustained increase, disproportionally higher among 6- to 17-year-olds and females later in 2020, draws attention to the awareness and monitoring of emotional and behavioral needs, including suicide risk, in these groups. The extent to which the increase in antipsychotic prescription is an add-on to existing psychotropic regimens warrants further review to assess the long-term impact on child and adolescent mental health.
Footnotes
Acknowledgments
The statements, findings, conclusions, views, and opinions contained and expressed in this article are based, in part, on data obtained under license from the IQVIA Institute, Human Data Science Research Collaborative's information service(s), U.S. Medical Claims, and U.S. Prescription Claims January 2019 to September 2020. All Rights Reserved.
Authors' Contributions
A.A.-R.: conceptualization (equal); data curation (equal); formal analysis (lead); methodology (equal); visualization (lead); writing—original draft (equal); and writing—review and editing (equal). H.L.: conceptualization (equal); data curation (equal); formal analysis (equal); methodology (equal); visualization (support); writing—original draft (support); and writing—review and editing (support). C.Z.: Conceptualization (support); data curation (support); formal analysis (support) methodology (support); visualization (support); writing—original draft (support); and writing—review and editing (support). S.R: conceptualization (equal); data curation (support); formal analysis (equal) methodology (equal); visualization (support); writing—original draft (equal); and writing—review and editing (equal).
Disclosures
The authors confirm no known conflicts of interest or presubmission approval requirements associated with this original research article, and there has been no significant financial or in-kind support for this work.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.