
Abstract
Background:
In response to concerns regarding psychotropic medication prescribing, California's foster care system implemented oversight strategies to improve prescribing and monitoring practice, particularly for antipsychotics. The impact of these policies has not been evaluated.
Objectives:
To examine foster youth psychotropic use data in California and their relationship to national and state policy initiatives.
Methods:
This study analyzed 2011–2020 data curated by the California Child Welfare Indicators Project. The platform matches Medicaid medication and laboratory claims with individual-level foster youth data to report rates of dispensed psychotropic medications, authorization status, and metabolic screening.
Results:
In 2011, there were 78,231 California youth in foster care, of which 10,435 (13.3%) received psychotropics and 5570 (7.1%) antipsychotics. In 2020, of 68,386 foster children, 7172 (12.2%) received psychotropics and 2068 (3.0%) antipsychotics. Proper authorizations for psychotropics were obtained for 5581 (77.8%) foster youth in 2020. Of those receiving antipsychotics, 904 (43.7%) underwent metabolic screening. The greatest declines in antipsychotic use occurred between 2013 (6.7%) and 2018 (3.1%). Overall 2011 to 2020 declines were similar for males (8.5% → 3.6%, 58% reduction, p < 0.001) and females (5.5% → 2.4%, 57% reduction, p < 0.001). Regarding age and race, greater declines occurred for children <10 years (2.33% → 0.84%, 64% reduction, p < 0.001) and Latino youth (5.4% → 2.2%, 59% reduction, p < 0.001).
Conclusions:
Temporal patterns in antipsychotic use suggest an impact of policies and guidelines. While 12.2% of foster youth continue to receive psychotropics, there were reductions in racial/ethnic disparities and declines in antipsychotic use. Lack of adherence to authorization and metabolic screening requirements continue to be concerning.
Introduction
There are increasing concerns that psychotropic medications are overprescribed to pediatric populations, particularly those in foster care. While 4% to 10% of Medicaid-enrolled children used psychotropic medications, 20% to 40% of foster care youth used such medications nationwide (Crystal et al, 2016; Ferguson et al, 2006; Leckman-Westin et al, 2018; Rubin et al, 2012; Zito et al, 2008). California has the largest population of children in foster care in the United States. In 2011, 13% of the California foster youth were on psychotropic medications, including 7% on antipsychotics (Webster et al, 2021).
Psychotropic medications are defined as having a primary intended effect on the central nervous system. Among these, antipsychotic medications stand out because of their significant metabolic side effects, including weight gain and predisposition to diabetes mellitus type 2 (Allaire et al, 2016; Skinner et al, 2015). The risk–benefit ratio for the use of antipsychotics may not be in the best interest of foster youth, particularly when other trauma-informed multidisciplinary interventions, such as psychotherapy, may be more effective but are frequently inaccessible to this population (Larsen et al, 2018; Leslie et al, 2004). Additional ethical problems may exist when a foster child's autonomy to decide is compromised by arrangements where housing is dependent on continued medication use (Szilagyi et al, 2015). Media reports in California suggested that acceptance and adherence to such medications was used as a condition for continued housing (Woolfolk, 2018).
California statutes determine that psychotropic medications cannot be used for the purpose of chemical restraint or discipline, except when acutely necessary in true psychiatric emergencies (California Code of Regulations, 2021). Nonetheless, there are concerns regarding coercive use of psychotropic medications (Woolfolk, 2018). Factors that may contribute to the overprescribing of psychotropic medications to foster youth may include lack of understanding of the effects of childhood trauma, caregiver demand for medication to manage disruptive behaviors, lack of pediatric mental health resources, and misdiagnosis of trauma symptoms as mental health disorders (Szilagyi et al, 2015; Webb, 2013).
Although antipsychotics were initially approved for the management of schizophrenia, their use has extended to other conditions, including other types of psychosis, bipolar disorder, treatment resistant depression, personality disorder, dementia, delirium, autism, and violent behavior. Recently, some antipsychotics have received limited FDA approval for the treatment of certain aspects of these conditions, although largely in adults. FDA approval in children remains centered on the indications of schizophrenia and acute bipolar disorder, mostly for those 10 years or older. Current evidence supporting off-label uses remains uncertain or lacking, particularly in vulnerable pediatric populations (Alexander et al, 2012; Radley et al, 2006; Walton et al, 2008).
Early California Medicaid program (Medi-Cal) changes, beginning in 2006, focused on coverage policies for psychotropic and antipsychotic medication for all pediatric Medi-Cal beneficiaries, not just those in foster care (The California Mental Health Planning Council, 2017). Initially, preauthorization using Treatment Authorization Request (TAR) Forms was required for psychotropic prescribing for children under 5 years. Subsequent changes expanded the TAR requirement to youth receiving two or more concomitant antipsychotics (2011) and then for all youth for any psychotropic or antipsychotic medication (2014).
In 2011, Medi-Cal cosponsored a California state-wide Quality Improvement Project (CQIP) (The California Department of Social Services, 2011) aimed at improving psychotropic medication prescribing. The multidisciplinary, multisectoral CQIP instigated additional authorization requirements, modified procedures for court-approved prescribing, and new minimum data reporting requirements (The California Department of Health Care Services and Department of Social Services, 2018). These additional measures were gradually implemented between 2013 and 2016, culminating in the 2018 publication of The California Guidelines for the Use of Psychotropic Medication with Children and Youth in Foster Care. Simultaneously, several areas of CQIP attention were taken up by the State Assembly and Senate, resulting in legislation making several recommendations obligatory. These state policy strategies grew out of earlier work by advocates, medication guideline developers, and the federal government that questioned the frequent use of psychotropic medications in foster youth and other pediatric populations (Department of Health Care Services, 2020).
This study describes annual trends of psychotropic medication prescribing in California's foster care system, particularly antipsychotics. We evaluated the potential impact of the CQIP policies on prescribing rates in a 10-year period, from 2011 to 2020. We also examined patterns of screening foster youth for metabolic disorders.
Methods
The data used in this analysis originate from the open-sourced platform curated by the California Child Welfare Indicators Project (CCWIP), an initiative by the University of California at Berkeley that resulted from the QIP process (Webster et al, 2021). The platform matches Medicaid medication claims (Medi-Cal Management Information System) with individual-level foster care data (Child Welfare Services/Case Management System) to determine the proportions of foster youth prescribed with psychotropic medications, their laboratory information, and demographic data. As in other states, Medicaid is the sole provider of health coverage for most foster youth (Department of Healthcare Services, 2020). The matching process uses a probabilistic, multistep algorithm based on combinations of name, social security number, and date of birth between the two systems.
Various metrics are available from different time points, but most were collected in quarters between 2011 and 2020. Information regarding metabolic screening is available for the years 2017 and 2020. Information regarding authorization for treatment is available from 2003 to 2021.
Children are included in psychotropic prescribing numbers if they have one or more claims for psychotropic medication and a concurrent open foster care episode during the 12 months of measurement. Medications are categorized as psychotropics as per the definitions of the California Guidelines for the Use of Psychotropic Medications with Children and Youth in Foster Care, which states: “psychotropic medication is defined by the Welfare & Institutions Code section 369.5 (d), as those medications prescribed to affect the central nervous system to treat psychiatric disorders or illnesses. They may include, but are not limited to, anxiolytic agents, antidepressants, mood stabilizers, antipsychotic medications, anti-Parkinson agents, hypnotics, medications for dementia, and psychostimulants” (The California Department of Health Care Services and Department of Social Services, 2018). A list of all included medications is available (Appendix A1). Our measure of prescribing is based on dispensed prescriptions and leaves out written prescriptions that were never filled. In addition, dispensed prescriptions may overstate use because not all dispensed prescriptions are consumed.
Regarding metabolic screening, the children are considered eligible if there are two or more prescription events for antipsychotic medication during the 12-month period. In addition, they are considered newly exposed to the medication if it is the first year the two prescription events occurred. Metabolic screening is considered complete if the child was tested for blood glucose and cholesterol at least once in the 12-month period. For newly prescribed youth, screening is considered complete if testing occurred between 90 days before and 15 days after starting a new antipsychotic. Finally, children are considered authorized for using psychotropics if a TAR form was filed by court order or placement home parental consent. These minimum metabolic screening requirements (blood glucose and cholesterol) follow CQIP recommendations. Additional tests, such as HbA1c, are encouraged but not mandated. CCWIP includes patients in the dataset of appropriate screening when their test results are documented.
The main variables of interest in this analysis are prescription rates per demographic group, metabolic screening rates, and the number of youths properly authorized to receive psychotropic medications. These outcomes reflect the legislations implemented by the CQIP and serve as indirect quality-of-care parameters concerning unauthorized psychotropic off-label use and the potential for metabolic consequences. We performed additional subgroup analyses assessing reductions in antipsychotic use between the 2011 and 2020 timepoints, considering time in care, sex at birth, age groups, geographic region, race, and ethnicity. Differences in means were assessed with two-tailed t-tests, assuming significance for p < 0.05.
This study analyzes publicly available data and is exempt of Institutional Review Board approval.
Results
In 2020, there were 68,386 children in California foster care, of which 7172 (12.2%) received psychotropics and 2068 (3%) antipsychotics. The majority of the children are of Latin-American ethnicity (54.0%) and are located in the Los Angeles region (43.3%). Sex at birth is equally represented between female (50.9%) and male (49.1%) groups. Time in foster care is broadly distributed, but the largest part of the youth has been in the system for <2 years (55.0%). Youth of all age groups are represented. Demographic information for the years of 2011 and 2020 is available on Table 1.
Reductions in Antipsychotic Prescription Between 2011 and 2020
The columns indicated by % represent the percentage of foster youth receiving antipsychotics in that given year. Numerators indicated in n columns and denominators in N columns. %Δ represents the relative reduction in antipsychotic prescribing between the observed periods (* p < 0.001; ** p = 0.015). Data obtained from the CCWIP; data aggregates from the Child Welfare Services-Case Management System and the Medi-Cal Management Information System.6
CCWIP, California Child Welfare Indicators Project.
There was a gradual decline in the proportion of antipsychotic prescribing between 2011 and 2020 (7.1% → 3.0%, 56.3% reduction, p < 0.001). Relative decline rates for psychotropic medications and antipsychotics are illustrated in Figure 1. An absolute reduction of 4.1 percentage points occurred for antipsychotic prescriptions, accompanied by only a 1.1 percentage point reduction in all psychotropic medications. The greatest consecutive annual decreases in antipsychotic medication use occurred between 2013 (6.7%) and 2018 (3.1%).
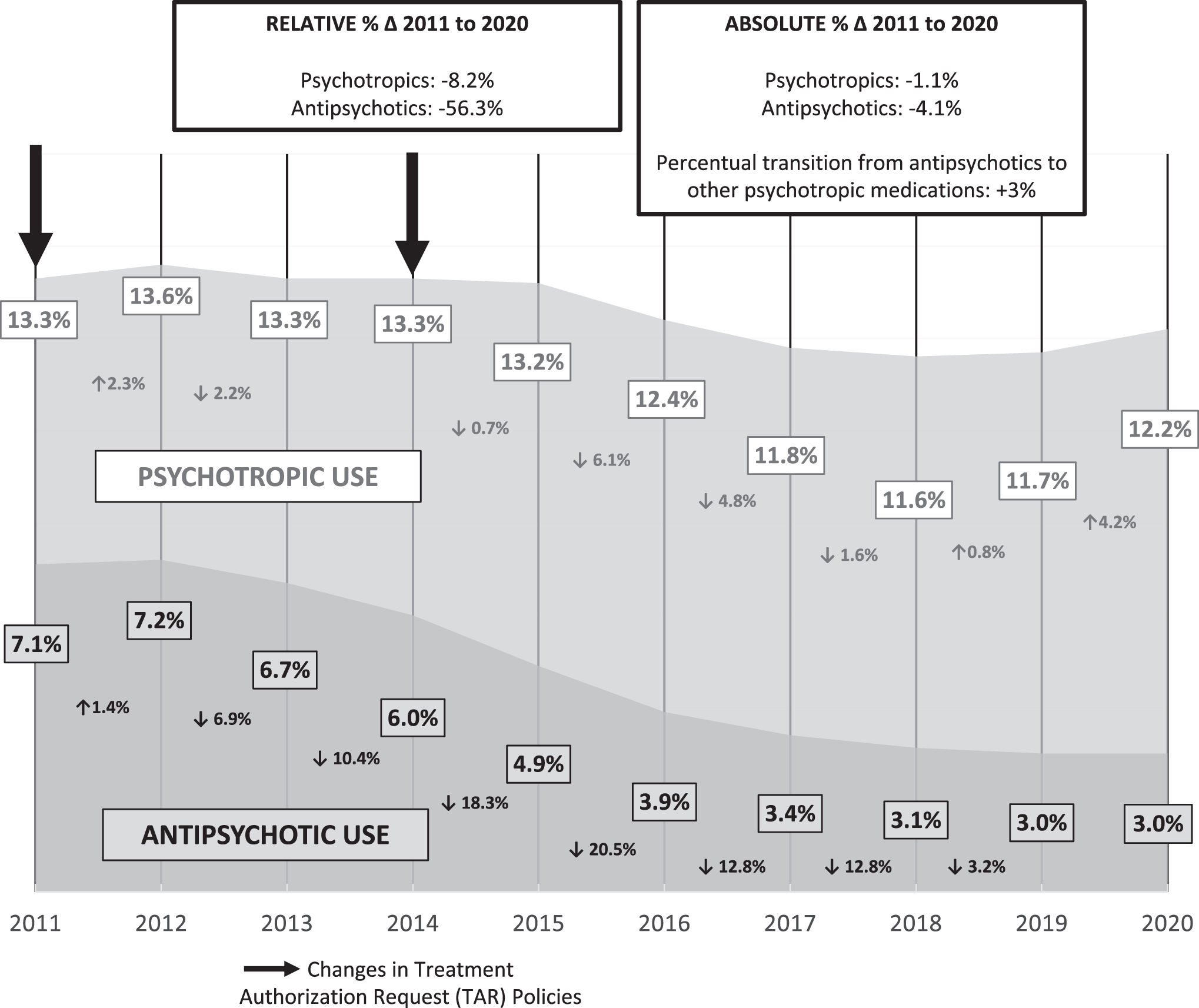
Trends of antipsychotic and psychotropic prescription rates (2011–2020). The arrows represent policies: in 2011 authorization is required for youth receiving two or more medications; in 2014 authorization is required for youth up to 18 years old. ↑(%) and ↓(%) represent relative increases and declines in prescription percentages between two consecutive years.
The decline rate is similar for males (8.5% → 3.6%, 58% reduction, p < 0.001) and females (5.5% → 2.4%, 57% reduction, p < 0.001). The lowest declines in prescription occurred for older youth aged 16–17 years (15.0% → 9.6%, 36% reduction, p < 0.001), Asian and Pacific Islander youth (4.3% → 2.7%, 38% reduction, p = 0.015), and for those located in Northern California (7.7% → 4.4%, 43% reduction, p < 0.001). The most significant declines occurred among children under 10 years (2.33% → 0.84%, 64% reduction, p < 0.001) and Latino youth (5.4% → 2.2%, 59% reduction, p < 0.001). Relative reductions in antipsychotic prescribing between 2011 and 2020 for different demographics are shown in Table 1. Trends by age group and race/ethnicity are illustrated in Figure 2.
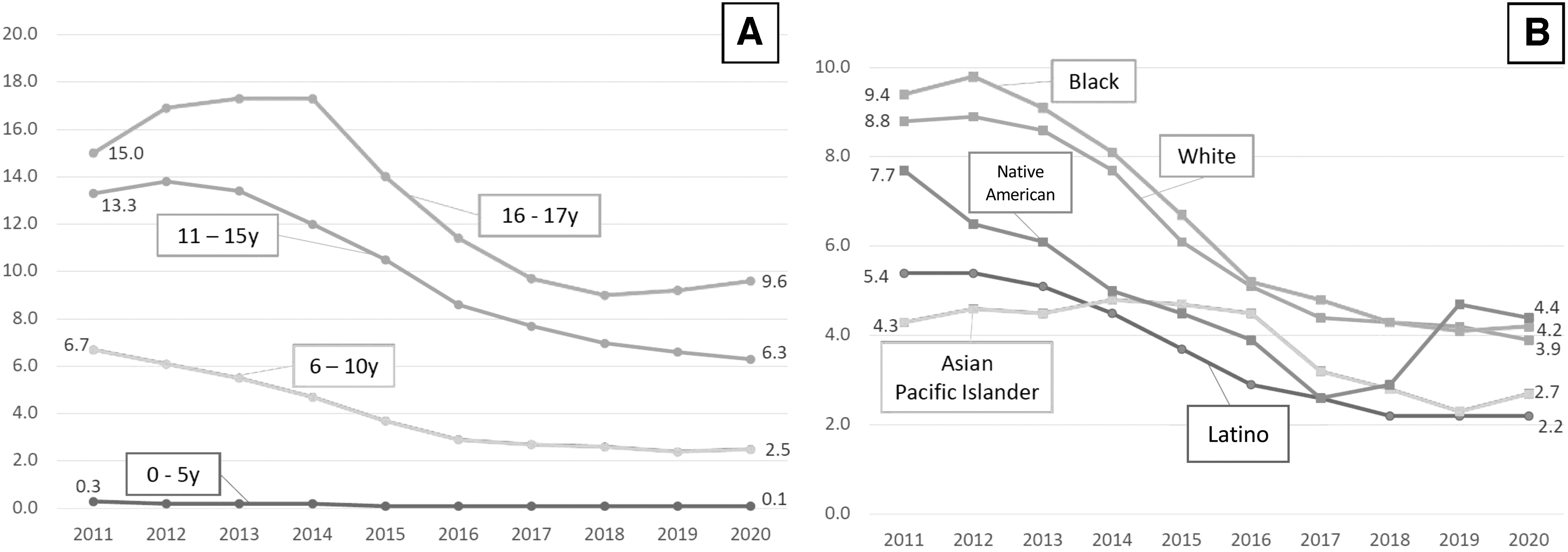
Antipsychotic prescription trends by age group, race, and ethnicity (2011–2020). All data labels depicted in %.
Of the 7172 children who received psychotropic medications in 2020, only 5581 (77.8%) had the necessary TAR forms. In addition, of the 1764 children receiving antipsychotics, only 904 (51.2%) underwent appropriate metabolic screening. When considering the youth newly prescribed with antipsychotics, only 150/811 (18.5%) received screening, a decrease in performance compared with 2017 (239/913 screened youth; 26.2%) (Fig. 3). There are no discrepancies in metabolic screening between youth of different race/ethnicity, age groups, geographic subregion, placement type, sex at birth, and length of time in foster care.

Children in foster care undergoing metabolic screening while receiving antipsychotics (2017 and 2020). All youth with two or more prescription events for antipsychotics during a 12-month period are eligible for metabolic screening. New prescriptions are defined as two or more prescription events during the period for treatment-naive children. Metabolic screening is considered complete if tested for blood glucose and cholesterol. For newly prescribed youth, screening is considered complete if testing occurs between 90 days before and 15 days after the start of a new antipsychotic.
Discussion
This analysis demonstrates a temporal relationship between the implementation of the California QIP and the reduced prescribing of antipsychotics in the foster care system. Although not causal, these temporal correlations suggest a QIP impact. Younger children experienced the largest relative declines, a CQIP focus. While 12% of foster youth continue to receive psychotropic medications, the decreased use since 2011 suggests improved prescription patterns; therefore, a possible net improvement in drug safety. To our knowledge, this is the first study to report on CQIP results, determine its strengths and weaknesses, and suggest next steps for quality improvement.
Several aspects of the CQIP guidelines could be considered for nationwide implementation, including its information completeness and publicly accessible data. When comparing California with 48 states, only California and 16 (35.4%) other Statal Child Welfare Agencies had specific psychotropic medication use policies or guidelines requiring appropriate metabolic screening (Mackie et al, 2020; Mackie et al, 2011; Zito et al, 2013). In addition, only one other state (2.1%) included children of all ages (<18 years) in the psychotropic use authorization requirements, a step also taken by the CQIP in 2014 (Mackie et al, 2020; Mackie et al, 2011; Zito et al, 2013). By 2020, only 29 of 50 states (58%) had developed specific psychotropic use oversight measures (Mackie et al, 2020; National Conference of State Legislatures, 2021).
The objectives of different statal child welfare policies/guidelines for psychotropic medication oversight significantly differ. Variation exists in the following areas: (1) the presence of a specific policy/guideline for psychotropic medication oversight; (2) the specific subpopulations covered by the policy/guideline (e.g., prioritization of different age groups); and (3) the components of the policy/guideline for psychotropic medication oversight and evaluation, such as screening and/or assessment, informed consent procedures, and other monitoring processes (Mackie et al, 2020; Mackie et al, 2011). These variations suggest that different states are taking flexible approaches when implementing oversight systems and policies, despite the overall lack of evidence to support whether these initiatives are working. These findings highlight the importance of the CCWIP and provide justification for this work.
In the analyzed 10-year period, a higher decline was observed in antipsychotic prescribing compared with overall psychotropic medications. Psychotropic use rates were relatively constant between 2012 and 2020, as decline only started in 2016, followed by new increases between 2019 and 2020. In contrast, antipsychotic prescription rates steadily declined between 2012 and 2020. This finding suggests that prescribers may be substituting antipsychotics for other drugs, which may reflect increased awareness regarding appropriate indications and risks of using antipsychotics. Since 2008, several publications have suggested leaving antipsychotics as second-line options for agitation in pediatric populations, culminating in the American Association for Emergency Psychiatry guidelines (2019) (Gerson et al, 2019).
Previous studies suggest that adolescents in the foster system have higher rates of psychotropic drug use than their younger peers (Brenner et al, 2014; Raghavan and McMillen, 2008; Zima et al, 1999). In this study, less marked declines in prescription occurred for older youth aged 16–17 years. Since one of the CQIP goals focused on reducing antipsychotic use among younger children, this finding could reflect lower prioritization. Prescribers need to be aware that age may play a role as a health disparity variable.
Geographic patterns of prescriptions and race/ethnicity prescribing trends may further indicate health disparities. Asian and Pacific Islander youth and those located in Northern California experienced the lowest rates of antipsychotic use decline. These findings are aligned with previous literature, and they suggest that structural, administrative, or systemic influences may play a role in variations of medication use, as opposed to clinical status (Leslie et al, 2011). Careful consideration of these data allows for informed policymaking in the following years, making way for improvements in the regions where the CQIP impact was less significant.
The most concerning findings from this analysis are related to the proper authorization for using psychotropics and rates of metabolic screening. A significant proportion (22.2%) of California foster youth received psychotropics in 2020 without the necessary authorization incorporated in the CQIP policies. Stricter regulations could further reduce prescription rates, ensure safety, and respect autonomy and decision-making principles.
Less than half of the California foster youth on antipsychotic medications received screening for metabolic disorders in 2020. When focusing on the youth with recent prescriptions, <20% received screening. The performance for both the overall and the newly prescribed groups was lower versus data from 2017 and reflects poor adherence to surveillance protocols. We acknowledge that these performance data correlate with structural challenges in public work, such as understaffing of teams, increasing case-workloads per provider, and the national shortage of children and adolescent psychiatrists and other behavioral specialists.
Limitations
There are several limitations to this study. First, this descriptive analysis is limited by the lack of comparative methods, as the variables of interest cannot be compared in an experimental model (i.e., comparing the implementation of policy changes in a case group vs. controls). Second, the available data elements are limited to those collected by child welfare agencies; thus, several desired variables, such as psychiatric diagnosis, are not included. We recognize that, if available, these variables might validate antipsychotic use in a subset of youth. We also acknowledge that these data reflect medication prescription data based on adjudicated pharmacy claims and do not necessarily indicate actual consumption of the medications. Finally, regarding metabolic screening, the data sources do not specify key monitoring activities, including health care provider review of the results.
Conclusions and Clinical Significance
In conclusion, our data suggest reductions in antipsychotic medication prescribing consistent with California initiatives to reduce psychotropic medication use in foster youth. Continuing differences by geographic area, race and ethnicity, age group, and time-in-care likely represent persistent health disparities in the prescribing of psychotropics in the foster care system. In addition, we highlight shortfalls in metabolic surveillance protocols and ensuring proper authorization for every child who receives psychotropic medications. The clinical significance of these findings lies on the adverse events associated with the use of such medications, particularly when metabolic screening does not follow the appropriate recommendations. These steps are needed to ensure safe prescribing of high-risk medications to an already vulnerable population.
Footnotes
Acknowledgments
The authors are grateful to Erin S. Keebaugh, Natalie Yu, and Pauline Chan for their contributions to this work. The authors acknowledge the University of California at Berkeley and those responsible for the California Child Welfare Indicators Project.
Data Availability Statement
The data underlying this article are available in the California Child Welfare Indicators Project Reports at
Disclosures
The authors disclose no financial conflict of interests. R.S.T. served as a member of the California QIP, as well as of its Clinical Practices subcommittee.