
Abstract
Objective:
To describe the results of the Sertraline Pediatric Registry for The Evaluation of Safety (SPRITES) outcome measures of cognitive, emotional, and physical development following long-term treatment with sertraline (for up to 3 years) in children and adolescents aged 6–16 years.
Methods:
SPRITES was a long-term, multicenter, open-label, prospective observational study designed to compare physical and psychological development in pediatric patients exposed to sertraline (with or without psychotherapy) or psychotherapy alone in usual care settings. Data were summarized descriptively, and outcomes were evaluated using a marginal structural model.
Results:
Between April 2012 and September 2020, 941 patients across 44 U.S. sites participated in the study. At baseline, 695 participants were exposed to sertraline (physician prescribed) with or without psychotherapy, and 245 participants were exposed to psychotherapy alone. Of these, 432 participants (46.0%) completed the full 3-year study follow-up. No significant changes across time were found in standardized height, BRIEF (Behavior Rating Inventory of Executive Function), Trails B, and Tanner stage based on cumulative sertraline exposure or exposure since the last visit. Change in mean standardized weight across time was positively associated with both cumulative sertraline exposure (p = 0.02) and exposure since the last visit (p = 0.029). The mean changes from baseline across time in standardized weight were standard deviations of 0.02, 0.03, 0.16, and 0.17 at months 3, 6, 30, and 36, respectively. However, this finding was not observed in the mean change across time in standardized body mass index, which was not statistically significant.
Conclusions:
Results are consistent with normal development. Although a statistically significant finding for standardized weight was observed in comparative analyses, the magnitude of the change is small and observed at higher doses of sertraline only. No other significant differences were observed between the “sertraline” group and the “no pharmacological therapy” group on other primary outcome measures.
ClinicalTrials.gov identifier:
NCT01302080.
Introduction
Diagnosis and treatment of pediatric mental illness are critical to returning children to a normal developmental trajectory insofar as possible. Current first-line treatments are psychotherapy and pharmacotherapy, including selective serotonin reuptake inhibitors (SSRIs) or serotonin–norepinephrine reuptake inhibitors (SNRIs), either alone or in combination with psychotherapy. Despite their frequent use, the long-term safety of antidepressants for the treatment of pediatric mental illness remains understudied (Locher et al, 2017). The safety of antidepressant medications is largely informed by brief, small, well-controlled randomized clinical trials in highly selective patients. A meta-analysis of placebo-controlled clinical trials of SSRIs and SNRIs in children and adolescents with common psychiatric disorders identified 36 eligible trials conducted between 1992 and 2013. The treatment duration of these studies ranged from 7 to 18 weeks, with only three trials (8.3%) evaluating outcomes after 16 weeks of treatment or longer (Locher et al, 2017).
Although few studies addressed the long-term impact of these compounds, safety data from these short-term trials have provided important information. In a pooled analysis of two short-term, 10-week placebo-controlled depression studies, Wagner et al (2003) found that children and adolescents treated with sertraline gained less weight (about 1 kg less) than those treated with placebo. Furthermore, about 7% of children and 2% of adolescents on sertraline experienced >7% body weight loss compared with 0% and 1% of children and adolescents, respectively, treated with placebo. However, the 68 patients who participated in both the 10-week trial and the 24-week open-label extension studies (for a cumulative sertraline exposure of 34 weeks) had weight gain comparable to age- and sex-matched norms. This outcome suggests that sertraline may not have persistent effects on weight loss (Wagner et al, 2003; Zoloft, 2021).
Hindered growth was also observed in other short-term SSRI studies. For example, after 19 weeks of treatment, fluoxetine was associated with an average of 1.1 cm less gain in height and 1.1 kg less gain in weight compared with children and adolescents treated with placebo (Nilsson et al, 2004). The product label for fluoxetine notes that height and weight should be monitored periodically in pediatric patients (Prozac 2021).
To the best of our knowledge, no studies have evaluated the long-term use of sertraline or any other SSRI/SNRI on pediatric physical and psychological development. The need for such studies in psychiatry is paramount, especially in pediatric patients who are not only underrepresented in clinical trials but also taking more antidepressant medication. Findings from the National Health and Nutrition Examination Surveys show that past-month antidepressant use increased from 7.7% to 12.7% of participants between the 1999–2002 and 2011–2014 periods, representing a 65% increase. Of past-month antidepressant users aged 12 years and older in the latter period, 68% received treatment for at least 2 years and 25.3% for 10 years or more (Pratt et al, 2017). However, the conduct of long-term controlled or uncontrolled clinical studies poses significant logistical and practical challenges, which are more pronounced in pediatric populations. Not surprisingly, such studies are seldom undertaken.
The Sertraline Pediatric Registry for The Evaluation of Safety (SPRITES) was a postapproval commitment to the European Medicines Evaluation Board. SPRITES was a long-term, multicenter, open-label, prospective observational study designed to compare physical (including pubertal maturation) and psychological development and safety outcomes in pediatric participants exposed to sertraline (with or without psychotherapy) or psychotherapy alone in the context of usual clinical treatment. Psychotherapy was chosen as the comparator since psychosocial interventions, including behavioral therapies such as cognitive behavioral therapy, are often first-line treatments for anxiety disorders in children, including mild-to-moderate obsessive-compulsive disorder (OCD) (Walkup et al, 2008).
This article presents the results of the study's main objective: to evaluate the long-term impact of treatment with sertraline (including dose–response relationships) on cognitive, emotional, and physical development and pubertal maturation. Specific safety-related outcomes derived from adverse events, including worsening of or newly emergent suicidality, will be presented in a separate report.
Methods
Study design
SPRITES was a prospective cohort study of pediatric patients aged 6–16 years who received outpatient treatment with sertraline and/or psychotherapy at study entry (baseline) per usual clinical care of their treating physician (Kolitsopoulos et al, 2021). Participants were recruited from ∼50 centers in the United States. Study entry criteria were previously described and allowed enrollment of participants eligible for sertraline treatment based on their physician's clinical judgment. Physicians were free to change regimens and dosing based on patients' responses to treatment. Use of other concomitant medications (e.g., antidepressants) was also permitted. Dosing guidance was provided to physicians via approved labeling (Zoloft, 2021). Regardless of treatment status, each participant was followed for up to 3 years. Postbaseline study assessments occurred at 3, 6, 12, 18, 24, 30, and 36 months. Primary outcomes included treatment status, sertraline exposure, changes in cognitive, emotional, and physical development, pubertal maturation, and adverse events (including suicidality).
Exposure groups
Enrollment into SPRITES required either sertraline treatment or psychotherapy initiated on or within 45 days of participation. Treatment was not randomly assigned and could be modified at the clinician's discretion at any time during study participation. To account for treatment changes, participants were classified into their actual treatment exposure categories (described below) at baseline and at each postbaseline visit. All analyses accounted for these exposure category changes.
Sertraline group
At baseline, the sertraline exposure group was composed of participants exposed to sertraline treatment within 45 days of enrollment in SPRITES. At a postbaseline visit, the sertraline group included participants who had received sertraline with or without other treatment(s) since the previous visit (e.g., psychotherapy or other psychotropic medication). At each study visit, sertraline exposure, reasons for dose adjustment, estimated compliance, and concomitant psychotropic medication prescriptions were also ascertained.
Other antidepressant group
At baseline and any follow-up visit, this participant group was exposed to only a non-sertraline antidepressant (with or without psychotherapy).
No pharmacological therapy group
At baseline, these participants were only receiving psychotherapy for the same spectrum of mental health conditions and were not taking any antidepressant medication on or within 45 days of enrollment. (This group also included 70 participants who were not taking sertraline and were missing information on psychotherapy sessions within 45 days of enrollment.) At a postbaseline visit, these participants were on psychotherapy only or no treatment at all since the previous visit.
At each study visit, all participants were assessed for the occurrence of adverse events, including suicidal ideation/behavior. The study was approved by the Copernicus Institutional Review Board, Western Institutional Review Board and 24 local Institutional review boards as well as the Duke University Health System Institute Review Board. The Duke University Health System Institute Review Board covers the Duke Clinical Research Institute's coordinating center activities.
Study outcomes
Physical development
Physical development was assessed via height and weight measurements, from which body mass index (BMI) was derived. Pubertal maturation (Supplementary Appendix Table SA1) was determined by self-rated pictures for adolescents (Dorn et al, 1990; Taylor et al, 2001). For children 12 years or younger and for adolescent participants who refused self-reported Tanner staging, the Pubertal Development Scale (PDS) was employed. The PDS is a widely used 8-item, gender-specific, self-report measure of pubertal development. The PDS reliably ascertains pubertal status and maps directly to Tanner stages (Petersen et al, 1988).
Psychological development: executive functioning and behavioral regulation
Differences in patient's executive functioning and behavioral regulation were assessed using the Trail Making Test B (TMT-B) (Mitrushina et al, 2006; Reitan and Wolfson, 2004; Rosin and Levett, 2001; Strauss et al, 2006; Tombaugh, 2004) and the Behavior Rating Inventory of Executive Function (BRIEF) (Gioia et al, 2000). The TMT-B provides a broadband behavioral measure of executive functioning and cognitive flexibility. The BRIEF is a standardized questionnaire that assesses behavioral manifestations of executive functioning deficits in children using ratings of their everyday behaviors. The individual BRIEF items load onto eight scales that are combined to generate two subfactors: the Behavioral Regulation Index (BRI) and the Metacognition Index (MI). Briefly, the Plan/Organized, Working Memory, Initiate, Organization of Materials, and Monitor scales contribute to the BRI, and the Emotional Control, Shift, and Inhibit scales contribute to the MI (Supplementary Appendix Table SA2) (Gioia et al, 2000).
Statistical analysis
The enrollment target for this study was ∼900 participants, with the expectation that 720 patients would be exposed to sertraline. The sample size was selected to ensure adequate statistical power to detect a between-group mean standardized difference in outcomes of 0.30. Baseline demographic and socioeconomic characteristics of participants and their families were summarized by exposure group with relevant descriptive statistics and compared using Fisher's exact tests for categorical variables and Kruskal–Wallis tests for continuous variables. Because the data were observational, the association between sertraline exposure and study outcomes was assessed using marginal structural models (MSMs).
Descriptive data summaries
Except for Tanner staging, study outcomes were summarized at each visit by treatment exposure at baseline and by exposure since the previous study visit (i.e., recent exposure), using the original unit as well as sex- and age-standardized units via a z-score or t-score transformation (Supplementary Appendix Table SA3). Changes in outcomes from baseline were summarized similarly. For Tanner staging, changes were assessed and summarized using shift tables that display the numbers and proportions of participants who transitioned sequentially to the next pubertal stage throughout the 36-month follow-up period.
Patients younger than 15 years received the younger age version of the TMT-B, whereas those older than 15 years received the adult age version. Of the 4787 TMT-B assessments collected, 155 total instances (3.2%) of the incorrect version were used and were excluded from analyses.
Descriptive summaries were performed in two data sets: (1) All participant data and (2) Continuous treatment exposure data. The first consists of all visits in the database from participants who signed informed consent. The second data set consists only of those visits in which there was no change in the treatment group from baseline (i.e., excluding data collected after a participant changed to another treatment). Missing data were left as missing and were not imputed for these descriptive summaries.
Dose–response analyses
MSMs were used to examine the association between sertraline exposure and change from baseline in study outcome variables at each visit. This repeated-measures model adjusts for potential time-varying confounders and accounts for treatment switches and dropouts using inverse probability weighting (Robins et al, 2000). These analyses were conducted using all participant data and included assessments throughout the 36-month follow-up. Participants with no follow-up data were excluded. Missed visits and visits occurring after a missed visit were also excluded.
Sertraline exposure used to examine dose–response relationships was included in models in two ways: (1) Cumulative exposure to sertraline, defined as the total amount of sertraline (mg) the patient took between the baseline visit and focal visit divided by the number of days between the baseline and focal visit; and (2) recent exposure to sertraline, defined as total amount of sertraline (mg) the patient took since the previous visit divided by the number of days between the previous visit and focal visit.
Sertraline exposure was modeled as both a continuous variable and a categorical variable. Outcomes were modeled as a function of the month associated with the visit, sertraline exposure, and their interaction.
The effect of sertraline on physical and psychological development was assessed while adjusting for a range of prespecified covariates. The MSMs were conducted via weighted repeated-measures models implemented using a generalized estimating equations approach and included interaction terms between relevant subgroups and sertraline exposure. The subgroup analyses were only performed for outcomes that were determined to have an overall statistically significant relationship with sertraline.
The following subgroups were evaluated: age (6–11 years; 12–17 years), sex (male; female), race (White; Combined Asian, Black or African American, Other, Multiple), mood disorder diagnosis (yes; no), OCD diagnosis (yes; no), anxiety disorder diagnosis (yes; no), prior psychotherapy (yes; no), previous treatment with psychotropic medications for SPRITES-treated disorders (yes; no), history of other neurological illness (yes; no), history of seizures (yes; no), past treatment with antipsychotics (yes; no), and past treatment with psychostimulants (yes; no). Additional covariates included were baseline CGI-S, C-SSRS, and HoNOSCA scores, and the baseline value of the outcome being analyzed. Also, when not being evaluated as a subgroup variable, age was used as a continuous covariate. Additional details on our MSM approach were described previously (Kolitsopoulos et al, 2021). Statistical analyses were conducted using SAS, version 9.4 (SAS Institute, Cary, NC), and all tests were two-sided with α = 0.05. p-Values were not adjusted for multiplicity.
Concomitant medication usage
SPRITES was designed to reflect real-world sertraline treatment patterns for anxiety and related disorders, including OCD. Thus, concomitant psychotropic medication use, including stimulants, antipsychotics, and other medications, was allowed. To assess the risk of potential confounding due to the effects of concomitant medications, post hoc descriptive analyses of the number and proportion of patients at each visit who were prescribed any concomitant psychotropic medication while also receiving sertraline were undertaken for outcomes with observed significant association. In addition, the number of patients at each visit who during the preceding treatment interval was prescribed sertraline plus a second antidepressant, sertraline plus a stimulant, or sertraline plus an antipsychotic medication was also summarized.
Results
Study population
Overall, 941 participants at 44 U.S. sites participated in the study between April 4, 2012, and September 9, 2020. At baseline, 696 participants were intended for the sertraline group, with or without psychotherapy, and 245 participants were intended for treatment with psychotherapy alone. Of these, 432 participants (46.0%) completed the full 3-year study follow-up.
Dropouts from the study comprised 365 of the 696 (52.4%) participants in the baseline sertraline group and 143 of the 245 (58.4%) participants in the baseline psychotherapy group. The two most common reasons for study withdrawal in both the sertraline and psychotherapy groups were lost to follow-up (52.6% and 65.0%, respectively) and withdrawal of consent (25.2% and 27.3%, respectively). At baseline, seven participants, all in the sertraline group, had adverse events or serious adverse events that contributed to their study discontinuation. Most participants (805/941 [85.5%]), including those who withdrew prematurely, contributed to postbaseline data during the study.
Treatment groups were comparable on all baseline characteristics except (1) age, with the “no pharmacological therapy” group being significantly younger than the sertraline group and (2) race, with Asian and Black/African American participants comprising a larger proportion of the sertraline group than the no pharmacological therapy group (Table 1). Most participants had a diagnosed anxiety disorder (78.4%) at baseline; 47.1% of participants had a diagnosed mood disorder, and 15.6% had been diagnosed with OCD (Table 2). The sertraline group was significantly more likely to have a mood disorder and significantly less likely to have OCD.
Baseline Demographic Summary (All Patients)
All patients = all patients enrolled in SPRITES.
The treatment categories were based on the actual treatment received at baseline. The sertraline group was defined as those patients on sertraline only or sertraline and any other treatment. The other antidepressant group was defined as those patients on another antidepressant only or another antidepressant and psychotherapy. The no pharmacological therapy group was defined as those patients on psychotherapy only or no treatment at all.
The p-value tests for differences between the sertraline and no pharmacological therapy exposure groups based on the actual treatment received at baseline. Fisher's exact tests were conducted for categorical variables and Kruskal–Wallis tests were conducted for continuous variables.
max, maximum; min, minimum; Q, quartile; SD, standard deviation; SPRITES, Sertraline Pediatric Registry for The Evaluation of Safety.
Baseline Primary Diagnosis and Psychiatric Comorbidities (All Patients)
All patients = all patients enrolled in SPRITES.
The treatment categories were based on the actual treatment received at baseline.
The p-value tests for differences between the sertraline and no pharmacological therapy exposure groups based on the actual treatment received at baseline. Fisher's exact tests were conducted for categorical variables and Kruskal–Wallis tests were conducted for continuous variables.
Diagnosis categories are not mutually exclusive; investigators could have reported more than one primary diagnosis.
No patients were reported to have the following comorbid conditions: acute stress disorder, anorexia nervosa, bulimia nervosa, eating disorder, alcohol abuse disorder, marijuana abuse disorder, nicotine abuse disorder, opioid abuse disorder, schizophrenia, psychosis, mental retardation, axis II: borderline personality disorder.
ADHD, attention-deficit/hyperactivity disorder; N/A, not applicable; NOS, not otherwise specified; OCD, obsessive-compulsive disorder; SPRITES, Sertraline Pediatric Registry for The Evaluation of Safety.
At baseline, the mean (standard deviation [SD]) and standardized height of patients in the sertraline group were 59.9 (6.4) inches and 0.3 (1.1), respectively (Supplementary Appendix Table SA4); the mean (SD) and standardized height of patients in the no pharmacological therapy group were 57.4 (6.4) inches and 0.3 (1.1), respectively. At baseline, the mean (SD) and standardized weight of patients in the sertraline group was 112.4 (47.4) pounds and 0.6 (1.2), respectively; and the mean (SD) and standardized weight of patients in the no pharmacological therapy group was 94.8 (39.2) pounds and 0.4 (1.0), respectively. These data reflect that the no pharmacological therapy group being, on average, younger than those in the sertraline group.
For boys, the modal Tanner stage was I for both the sertraline group and the no pharmacological therapy group (42.4% and 51.3%, respectively; Supplementary Appendix Table SA5). For girls, the modal Tanner stage was IV for the sertraline group (36.4%) and I for the no pharmacological therapy group (30.0%). The distribution of stages varied significantly between treatment groups for girls but not for boys.
At baseline, the sertraline group had significantly worse standardized scores than the no pharmacological therapy group on the Trails B test and both the BRIEF MI and BRI subscales (Supplementary Appendix Table SA6).
Physical outcomes
Weight
In the all participant data, descriptive statistics based on standardized weight showed that participants recently exposed to sertraline had a slightly higher weight gain from baseline compared with participants without recent exposure. Among the sertraline group, the mean change in the standardized weight from baseline increased from 0.02 SD at month 3, 0.03 SD at month 6, to 0.16 SD at month 30, and 0.17 SD at month 36 (Supplementary Appendix Table SA7). Compared with the no pharmacological therapy group, patients exposed to sertraline showed more weight gain, although the magnitude of the effect was small (mean change <0.2 SD in standardized weight z-scores) (Fig. 1).
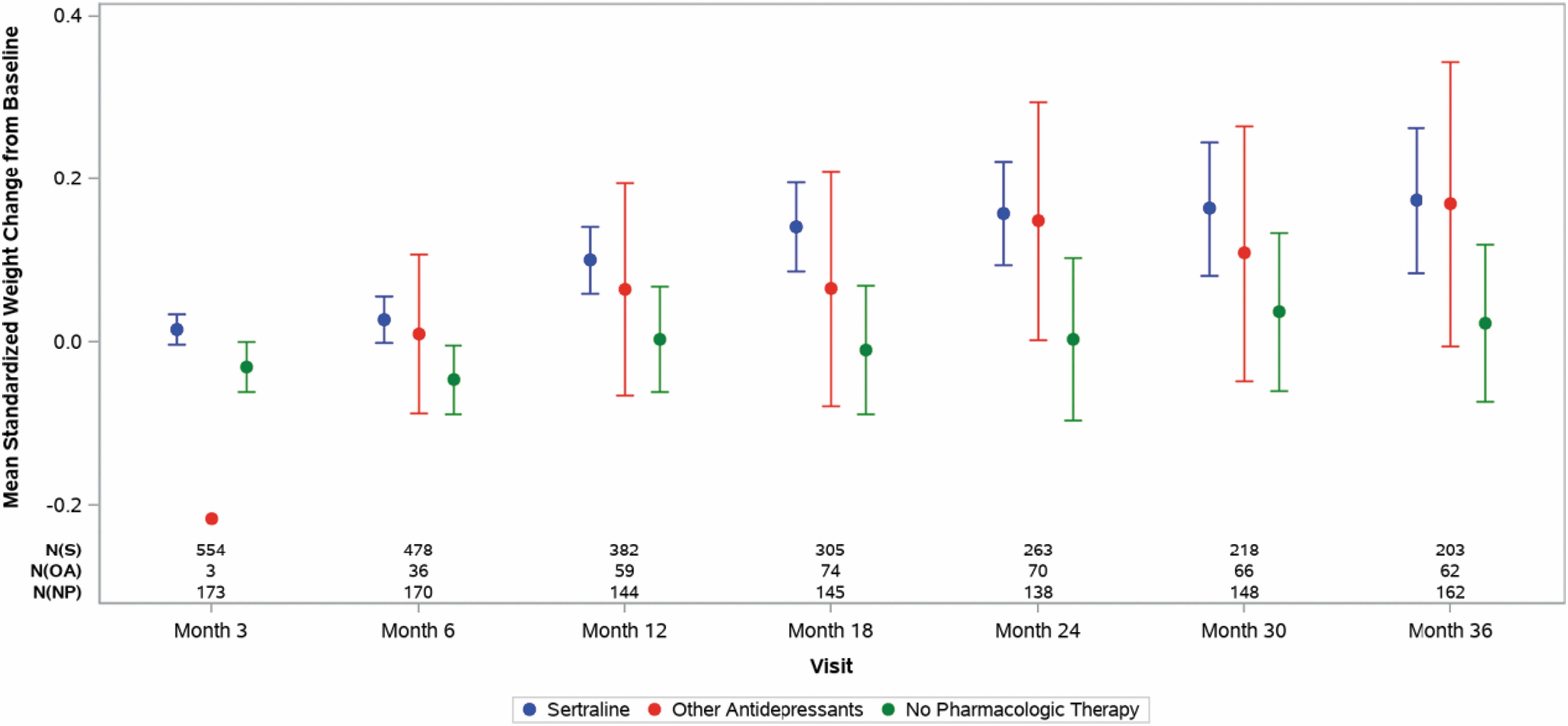
Change from baseline in standardized weighta by treatmentb and visit (mean and 95% CI) (all patients). The three rows of numbers at the bottom of this figure report the number of nonmissing values used to calculate the mean and 95% confidence limits at each visit by treatment. The top one reports the numbers for patients in the sertraline group, the middle one reports the numbers for patients in the other antidepressant group, and the bottom one reports the numbers for patients in the no pharmacological therapy group. If the number of nonmissing values is ≤5, 95% confidence limits are not displayed. aStandardized by age and sex; z-scores reported. bThe treatment categories for the baseline visit were based on the actual treatment received at baseline. The treatment categories for a given postbaseline visit are based on treatment exposure since the previous visit. The sertraline group was defined as those patients on sertraline only or sertraline and any other treatment. The other antidepressant group was defined as those patients on another antidepressant only or another antidepressant and psychotherapy. The no pharmacological therapy group was defined as those patients on psychotherapy only or no treatment at all. BMI, body mass index; CI, confidence interval; NP, no pharmacological therapy; OA, other antidepressants; S, sertraline.
Using the continuous treatment exposure data, participants exposed to sertraline also showed slightly more weight gain compared with the no pharmacological therapy group before changing treatment groups (data not shown).
The dose–response association between weight gain and sertraline exposure was statistically significant (p < 0.05) when cumulative sertraline dose was analyzed as a continuous variable (Table 3). Specifically, at month 36 (Supplementary Appendix Table SA8), each 5 mg/day increase in sertraline was associated with a 0.4 lb increase in body weight (95% confidence interval [CI]: 0.10 to 0.71 lb). Or equivalently, a 50 mg/day dose increment over the 36-month period was associated with a 4 lb (95% CI: 1.0 to 7.1 lb) weight gain. After body weight was standardized by age and sex, a 50 mg/day increase was associated with a 0.1 SD weight gain after 36 months (95% CI: <0 to 0.02 SD).
Results of Marginal Structural Model Analyses of Physical and Psychological Development Outcomes (p-Values or Not Statistically Significant): All Patient Population
p-Values are from an overall test across all visits. All patients = all patients enrolled in SPRITES.
The treatment categories were based on the actual treatment received at baseline.
The p-value tests for differences between the sertraline and no pharmacological therapy exposure groups based on the actual treatment received at baseline. Fisher's exact tests were conducted for categorical variables and Kruskal–Wallis tests were conducted for continuous variables.
Indicates age- and sex-standardized, z-score reported; t-score for BRIEF measures; Trails B standardized only by age.
Data from visits where patients had Trails B assessments administered according to the incorrect version for their age and where patients were beyond 12 months from being the correct age for the version administered are not included in this report.
Higher scores indicate worse executive functioning.
BMI, body mass index; BRI, Behavior Regulation Index; BRIEF, Behavior Rating Inventory of Executive Function; max, maximum; MI, Metacognition Index; min, minimum; NS, not statistically significant; SPRITES, Sertraline Pediatric Registry for The Evaluation of Safety.
When recent sertraline exposure was examined, a similar dose–response relationship was noted: an increase of 50 mg/day in recent exposure was associated with a 2.2 lb (95% CI: 0.3 to 4.2 lb) additional weight gain or a 0.1 SD (95% CI: <0 to 0.1 SD) standard weight gain at month 36.
To better understand what the dose relationship meant for the children in the study, weight gain was analyzed using sertraline exposure as a categorical variable: 0, 0.1–25, 25–50, 50–75, 75–100, or >100 mg/day (Tables 4 and 5). Using this approach, the overall relationship between sertraline dose and weight gain was no longer statistically significant. However, children taking 75–100 and >100 mg/day of cumulative sertraline were 3.5 and 8.3 lbs heavier, on average, at 36 months, respectively, when compared with children not taking sertraline. Children on 0.1–25 and 25–50 mg/day were 0.5 and 0.1 lbs lighter on average at 36 months, respectively, than children not taking sertraline. Similar findings were observed when standard weight was examined or when recent sertraline exposure was used, which indicates that the dose–response relationship may have been mainly driven by higher doses of sertraline.
Weight Change from Baseline to Month 36 in Participants Treated with Sertraline Based on Cumulative Exposure Compared with Participants Who Did Not Receive Sertraline
Total estimated weight change is determined by taking the weight change from baseline to month 36 for the patients who did not receive sertraline and then adding to it the shift in weight change for participants who received sertraline at each dose level.
CI, confidence interval; SD, standard deviation.
Weight Change from Baseline to Month 36 in Participants Treated with Sertraline Based on Recent Exposure Compared with Participants Who Did Not Receive Sertraline
Total estimated weight change is determined by taking the weight change from baseline to month 36 for the patients who did not receive sertraline and then adding to it the shift in weight change for participants who received sertraline at each dose level.
CI, confidence interval; SD, standard deviation.
Body mass index
As expected in growing children and adolescents, the mean patient BMI increased over the course of the study. However, changes in age- and sex-standardized BMI scores were small and of similar magnitude across groups (Supplementary Appendix Table SA9). At 18 months, the mean (SD) change in standardized BMI z-scores since the baseline for all participants were 0.2 (0.6) and −0.04 (0.6) in the sertraline and no pharmacological therapy groups, respectively (Fig. 2). The change from baseline in the mean sertraline BMI z-score was about 0.2 and was not statistically significant (Correll and Carlson, 2006). At 36 months, similarly, the mean (SD) changes in standardized BMI z-scores since baseline for all participants were 0.2 (0.8), 0.2 (0.9), and 0.01 (0.7) in the sertraline, other antidepressant, and no pharmacological therapy groups, respectively.
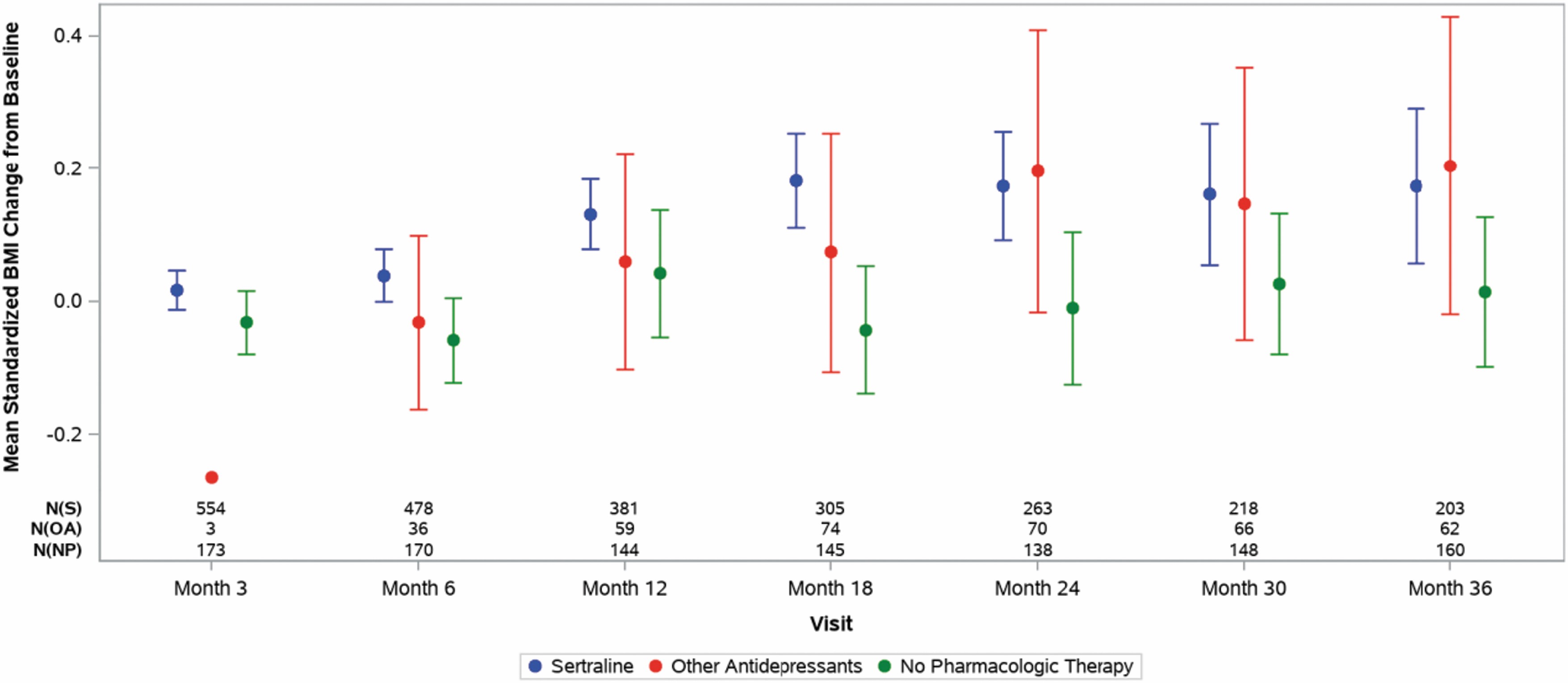
Change from baseline in standardized BMIa by treatmentb and visit (mean and 95% CI) (all patients). The three rows of numbers at the bottom of this figure report the number of nonmissing values used to calculate the mean and 95% confidence limits at each visit by treatment. The top one reports the numbers for patients in the sertraline group, the middle one reports the numbers for patients in the other antidepressant group, and the bottom one reports the numbers for patients in the no pharmacological therapy group. If the number of nonmissing values is ≤5, 95% confidence limits are not displayed. aStandardized by age and sex; z-scores reported. bThe treatment categories for the baseline visit were based on the actual treatment received at baseline. The treatment categories for a given postbaseline visit are based on treatment exposure since the previous visit. BMI, body mass index; CI, confidence interval; NP, no pharmacological therapy; OA, other antidepressants; S, sertraline.
A similar pattern emerged for participants continuously treated with sertraline or no pharmacological therapy (results not shown). When exposure was modeled continuously and as both cumulative and recent exposure, differences in nonstandardized BMI (but not in standardized BMI) were significant in MSM analyses (Table 3)
Post hoc analyses were undertaken to calculate the proportion of patients within each treatment group with a change from baseline in BMI z-score ≥0.5 at each visit, based on most recent sertraline exposure (Table 6). The results show that the proportions of patients with a change from baseline in BMI z-score ≥0.5 in the sertraline group range from 6.0% at month 3 to 28.6% at month 36 and are generally somewhat higher than the proportions in the no pharmacological therapy group except at months 6 and 12. Of note, the proportion of participants with ≥0.5 increase in BMI z-score was substantially higher in the other antidepressant group than both the sertraline group and the no pharmacological therapy group from month 12 to month 36.
Count and Percent of Participants with >0.5 Increase in Body Mass Index z-Score from Baseline by Study Visit and Treatment Exposure Category
The treatment exposure categories for the baseline visit are based on the actual treatment received at baseline. The treatment exposure categories for a given postbaseline visit are based on treatment exposure since the previous visit.
A post hoc logistic regression analysis of these data, including study visit and the interaction between treatment category and study visit, was conducted to assess for the possibility of an association between the treatment exposure category and the likelihood of a ≥0.5 change in BMI z-score. The p-value for comparison of sertraline to no pharmacological therapy was p = 0.471, indicating that there is insufficient evidence to conclude that there is any difference between these treatment exposure categories and the likelihood of a ≥0.5 change in the BMI z-score.
However, the p-value for comparison of other antidepressants to no pharmacological therapy was p = 0.036, suggesting that patients who received other antidepressants were more likely to have a ≥0.5 change from baseline in BMI z-score compared with patients on no pharmacological therapy. Although these post hoc analyses cannot account for the effect of treatment switching (which is addressed in the MSM), the results appear to be generally consistent with the MSM analysis of the BMI z-score data and point to a modest increase in BMI z-scores with sertraline treatment relative to no pharmacological therapy.
Post hoc analyses of concomitant medication use
Post hoc exploratory analyses conducted to assess the potential impact of concomitant medication use on the study outcomes revealed that about 20% of the children and adolescents enrolled in this study were prescribed concomitant psychiatric medication during the postbaseline follow-up period (Supplementary Appendix Table SA10). At month 3, 18.2% (101/554) of patients treated with sertraline were also prescribed concomitant psychotropic medication during the preceding treatment interval; the proportion of sertraline patients receiving concomitant medications increased to 21.5% (103/478) at month 6 and fell to 16.2% (33/203) at month 36.
Among patients prescribed any type of concomitant psychotropic medications in the same treatment interval they received sertraline, relatively few subjects were prescribed psychotropic medications such as stimulants (5.6% [31/554] at month 3 to 7.5% [36/478] at month 36), antipsychotics (4.8% [21/554] at month 3, 6.8% [26/381] at month 12, and 2.9% [6/203] at month 36), or additional antidepressants (4.0% [22/554] at month 3 to 9.8% [20/203] at month 36). Moreover, other than in the small subgroup of patients prescribed concomitant antipsychotic medications, no consistent differences were observed in postbaseline standardized weight gain between the patients who only received sertraline compared with those who received sertraline and a concomitant medication (Supplementary Appendix Table SA8), with the exception of month 24, when the mean (95% CI) standardized weight gain in the sertraline-only group (0.21 [0.14 to 0.28]) appeared to significantly exceed that of the sertraline plus concomitant medication group (−0.4 [−0.18 to 0.09]).
Among the small subgroup of patients who received concomitant antipsychotic medications, the mean increase in standardized weight gain was numerically greater in the sertraline+antipsychotic subgroup compared with the sertraline-only subgroup, with the greatest increase (mean [95% CI]) occurring at month 30 sertraline plus antipsychotics (0.75 [−0.81 to 2.3]) versus sertraline only (0.15 [0.07 to 0.24]). However, it should be noted that only six patients were receiving sertraline plus an antipsychotic medication at months 30 and 36 (Supplementary Appendix Table SA10).
Height
Although patient height increased over the study, age- and sex-standardized mean height remained relatively constant between the three treatment groups when treatment in each group was defined by treatment exposure since the previous visit (Supplementary Appendix Table SA11 and Supplementary Appendix Figure SA1). These data indicate no notable effect of sertraline on height. Similar findings were observed in treatment groups continuously on either sertraline or no pharmacological therapy (results not shown). MSM analyses of differences in height revealed no statistically significant differences (Table 3).
Tanner staging
Tanner staging progressed during follow-up in all the three treatment groups among boys and girls, both when treatment exposure was defined as since last visit (boys: Fig. 3 and Supplementary Appendix Table SA10; girls: Fig. 4 and Supplementary Appendix Table SA11) and among those continuously on their baseline treatment exposure (results not shown). No significant differences between treatment groups were detected regardless of the analytic approach (Table 3).
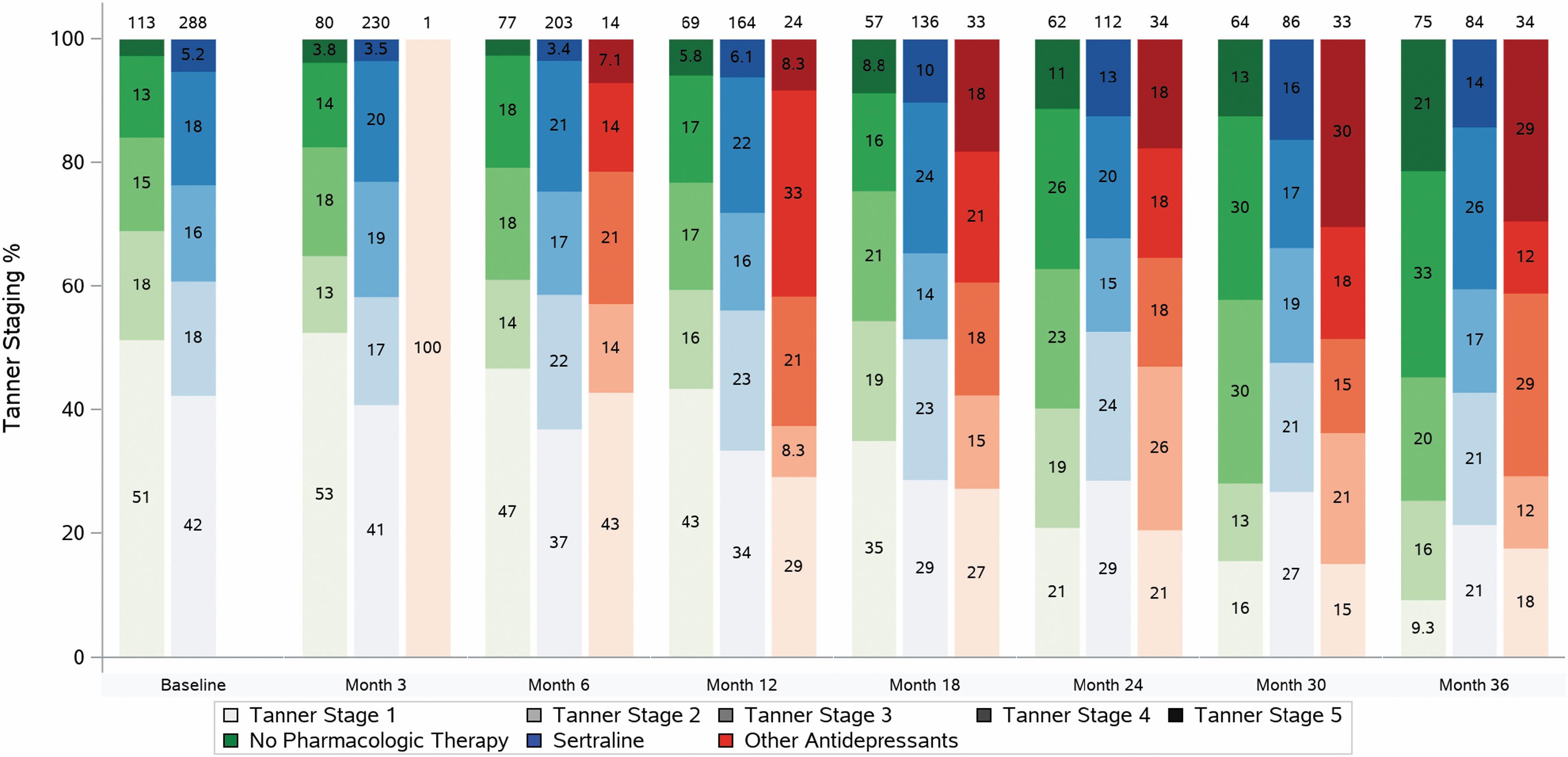
Primary outcome measures descriptive summary Tanner staging by treatmenta and visit (all patients: males). aThe treatment categories for the baseline visit were based on the actual treatment received at baseline. The treatment categories for a given postbaseline visit are based on treatment exposure since the previous visit.
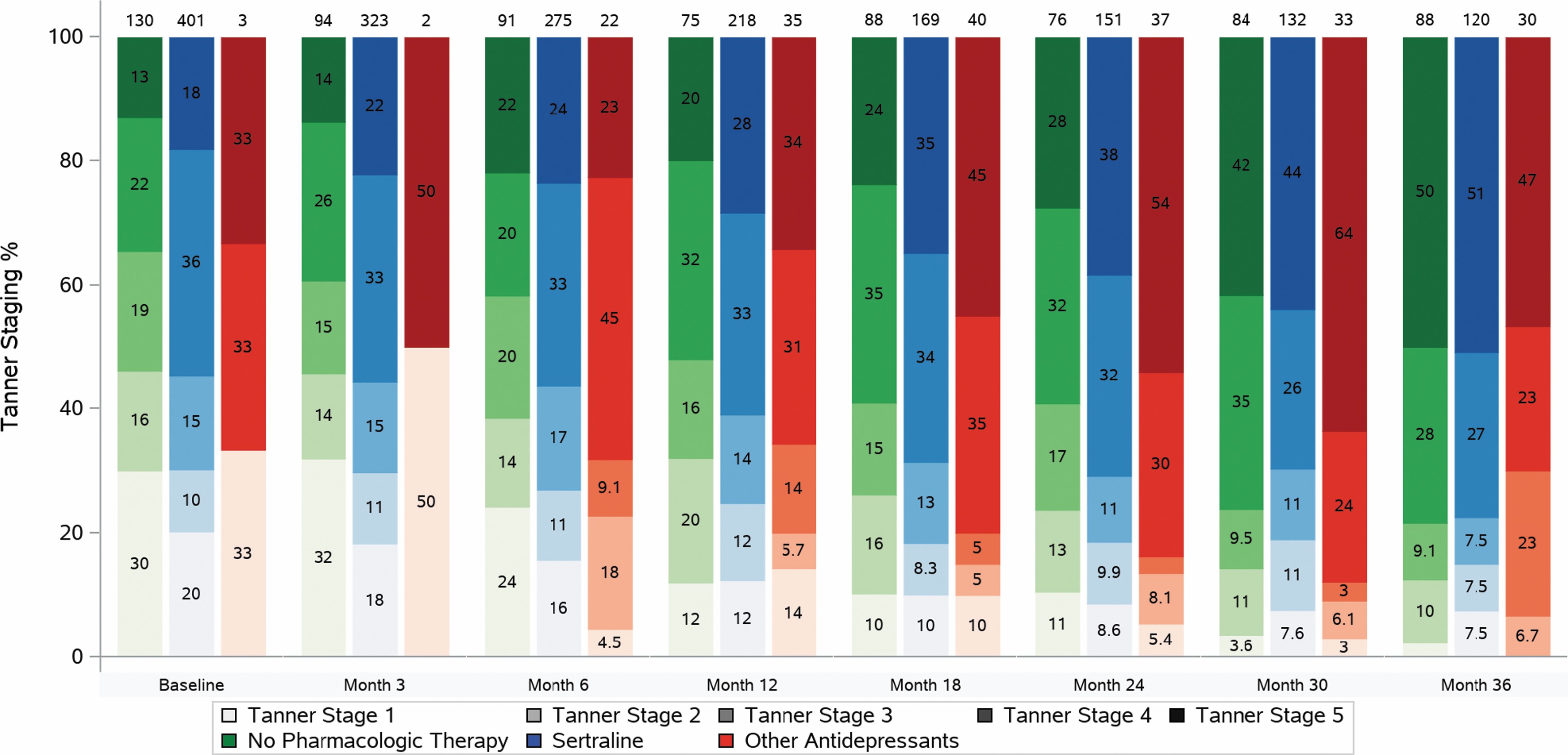
Primary outcome measures descriptive summary Tanner staging by treatmenta and visit (all patients: females). aThe treatment categories for the baseline visit were based on the actual treatment received at baseline. The treatment categories for a given postbaseline visit are based on treatment exposure since the previous visit.
Psychological outcomes
Trails B
Average change scores from baseline standardized, average Trails B scores did not vary significantly at any follow-up visit among the three treatment groups (Supplementary Appendix Figure SA2 and Supplementary Appendix Table SA12). Similarly, the MSM analyses indicated no significant treatment group differences, regardless of the analytic approach (Table 3).
BRIEF MI and BRI
For both indexes, there were no significant between group differences at any postbaseline time point (Supplementary Appendix Figure SA3 and SA4 and Supplementary Appendix Table SA13 and SA14). Likewise, no significant treatment group differences were detected in MSM analyses, regardless of the analytic approach (Table 3).
Subgroup analyses
No significant subgroup differences were observed for standardized weight or BMI (results not shown). There were significant subgroup differences for nonstandardized weight with respect to age and sex; however, these results were not significant for the standardized weight (Supplementary Appendix Table SA15).
Discussion
SPRITES is the first long-term observational study of the effect of sertraline use on children and adolescents' physical and psychological development. We assessed these outcomes in usual care settings over 3 years in a large U.S. sample of children and adolescents aged 6 to 16 years. The two main objectives of this study were (1) to evaluate the dose–response relationship between sertraline and physical and psychological development and (2) to compare the outcomes between sertraline-exposed and unexposed participants. Regarding the first, we have provided evidence that there is no dose–response relationship between sertraline exposure and height and numerous cognitive, emotional, and behavioral outcomes. We did find a modest association between sertraline exposure and weight and BMI.
On average, sertraline-treated participants tended to have greater weight gain compared with participants in the no pharmacological therapy group over the first 18 months of the study, with statistically significant differences in standardized weight occurring at months 6 and 18 and in BMI z-scores at month 18. However, the magnitude of the effect (a maximum difference of about 0.2 BMI z-score units between the sertraline and no drug treatment groups at month 18) appears modest, and its clinical relevance is unclear, especially because there were no differences between the two groups at later months of the study.
Of note, Correll and Carlson (2006) have proposed a threshold of a ≥0.5 BMI z-score increase from baseline for determination of a clinically significant abnormal weight gain in pediatric participants who were treated with psychotropic medications. Nonetheless, while these data do not suggest that sertraline has a sustained and clinically meaningful effect on weight gain in most youngsters, children treated with antidepressants, including sertraline, should have their weight and BMI monitored on a regular basis as part of routine clinical care.
Aside from the effect on weight gain, sertraline had no differential effect after 3 years of follow-up on other physical or psychological developmental outcomes when compared with participants taking other antidepressant medications and participants not taking any pharmacological treatment.
In addition, with the possible exception of weight gain, the MSM analyses support the conclusion that the physical, cognitive, and behavioral development of participants treated with sertraline is generally comparable with participants in the no pharmacological therapy group.
The present study had some limitations. Our study did not have balanced baseline characteristics between treatment groups due to lack of randomization. For instance, the sertraline group and the no pharmacological therapy group are not comparable in terms of disorder status, the severity of disease, and psychiatric history at baseline. Furthermore, there was no accounting for multiplicity. Thus, significant differences between treatment groups should be interpreted with caution. Our study did not assess the impact of imputation rules. The reason why missing interim dosing data was imputed as a 0 dose was that the data collection forms did not allow entry of “No treatment” for the forms collecting antidepressant use data. Thus, for missing antidepressant dosing data, there was no way to determine whether it was truly missing or if it indicated that no antidepressant was taken. The result was that we assumed a 0 dose for participants missing antidepressant dosing data.
The observation that the sertraline group at baseline reflects a more mentally ill study population is consistent with real-world clinical practice. Clinical practice guidelines for the treatment of depression and anxiety in children and adolescents recommend pharmacological therapy for participants with moderate-to-severe illness who do not respond to psychotherapy and for participants with more complicated depressions (Birmaher et al, 2007; Connolly and Bernstein, 2007).
Another important limitation is that the study was not designed to account for potential confounding of concomitant psychotropic medications. As SPRITES was intended to reflect sertraline use in real-world clinical practice, postbaseline psychiatric medications were not prohibited. However, psychiatric polypharmacy has become increasingly common and a major concern among practitioners, prescribers, and parents in recent years (Bhatara et al, 2004, Girand et al, 2020 Winterstein et al, 2017) and is associated with effects on weight and BMI (Maayan and Correll, 2011; Nguyen et al, 2018). Thus, the assessment of concomitant psychiatric medication use in this study was important, although limited by the fact that only prescription information was available for analysis.
It was not possible to distinguish between patients who took the medication and those who received a prescription but did not take the medication. Post hoc analyses showed that ∼20% of patients were prescribed concomitant psychiatric medication during the study and the proportion of patients prescribed concomitant psychotropic medications (i.e., stimulants, antipsychotics, additional antidepressants) during the same treatment interval when they were receiving sertraline was also relatively small (≤10%). Systematic differences in the change in standardized weight were observed only in the small subgroup of patients who received concomitant antipsychotic prescriptions compared with patients on sertraline alone. Antipsychotic-induced weight gain and increases in BMI in pediatric patients are common and well-characterized effects, and the increases observed in this subgroup of patients in SPRITES are consistent with previous reports (De Hert et al, 2011; Fraguas et al, 2008; Maayan and Correll, 2011).
Overall, descriptive post hoc analysis of concomitant psychotropic prescription data suggests that it is unlikely the statistically significant association of sertraline with a modest increase in standardized weight reported here is confounded by concomitant medication usage.
Conclusion
In summary, the results of the SPRITES study demonstrate that the overall growth and development of children and adolescents aged 6–16 years treated for up to 3 years with sertraline is consistent with normal developmental pathways.
Clinical Significance
Although only approved for the treatment of OCD in pediatric patients, sertraline, an SSRI, is used off-label to treat various psychiatric conditions. Furthermore, SSRIs comprise a significant proportion of antidepressants prescribed for pediatric depression treatment. In contrast to short-term effectiveness, the long-term impact of sertraline use on physical, cognitive, and emotional development has not been systematically explored in the context of benefits and tolerability in children and adolescents. Given the dearth of the published literature and multiple methodological weaknesses with the available evidence, this study was designed to obtain safety information for patients with long-term sertraline use. Results of the current study show that the physical, cognitive, and behavioral development of participants treated with sertraline was consistent with normal development.
Footnotes
Acknowledgments
We thank all the investigators and coordinators who took part in this study; the 941 participants in SPRITES; the Pfizer Medical, Worldwide Safety and Regulatory employees: Cynthia DeLuise, Tanya Russell, Omar Ahmed, Sarah Dubrava, Lisa Falato, Nancy Sherman, and Lisa Ludwig. Joann Munting was an employee of ExecuPharm, who was a paid contractor to Pfizer in the management of this study. John March, John Curry, Mary Creed, Kristy Vaughan, Sara Taylor, Jennifer Murphy, and Eliza Sgherza are (in some cases, were previously) employees of Duke Clinical Research Institute (DCRI), which received financial support in the management of this study. We also thank Rekha Raghuram, from Viatris, Bengaluru, India, for her contribution in medical editorial review of the article.
Authors' Contributions
All the authors confirm that they were part of this study and have played significant role from conceptualization of the study to the article preparation. Authorship for this study is considered following the ICMJE and COPE guidelines of authorship. All the authors approved the final version of the article along with the author order as presented in the article. F.K. participated in the design of the study. S.B., F.K., S.R., P.C., J.O., W.B., S.N.C., and Y.L. were involved in scientific, logistical, and operational decisions, drafting of the study statistical analysis plan, result interpretation, and took part in article writing. K.M. took part in drafting the article.
Disclosures
This study was sponsored by Pfizer. W.B., F.K., P.C., and S.R. are full-time employees and stock shareholders of Pfizer. At the time of study conduct, J.O. was a full-time employee and stock shareholder of Pfizer. S.N.C., S.B., and Y.L. are employees of Duke University/Duke Clinical Research Institute. K.M. is full-time employee and stock shareholder of Viatris.
Supplementary Material
Supplementary Appendix Figure SA1
Supplementary Appendix Figure SA2
Supplementary Appendix Figure SA3
Supplementary Appendix Figure SA4
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Table SA4
Supplementary Appendix Table SA5
Supplementary Appendix Table SA6
Supplementary Appendix Table SA7
Supplementary Appendix Table SA8
Supplementary Appendix Table SA9
Supplementary Appendix Table SA10
Supplementary Appendix Table SA11
Supplementary Appendix Table SA12
Supplementary Appendix Table SA13
Supplementary Appendix Table SA14
Supplementary Appendix Table SA15
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.