
Abstract
Objective:
To investigate the relationship between plasma aripiprazole (ARI) and its metabolite dehydroaripiprazole (DARI) concentrations and prolactin (PRL) levels in Chinese children and adolescents.
Methods:
This was a retrospective cross-sectional study and the data were collected at Beijing HuiLongGuan Hospital, a Beijing City owned psychiatric hospital, between January 1 and December 31, 2021. Fifty-two child and adolescent inpatients (17 males, 35 females) aged 13–18 years and received ARI regardless of diagnosis were included. The steady-state ARI and DARI plasma concentrations were measured using high-performance liquid chromatography-tandem mass spectrometry. The serum PRL levels were measured by chemiluminescence immunoassay.
Results:
The plasma concentrations of ARI, DARI, and the total of ARI and DARI were negatively correlated with serum PRL levels in female children and adolescents. Approximately 15% of child and adolescent inpatients treated with ARI exhibited subnormal PRL serum levels.
Conclusions:
The results suggest that in addition to regularly monitoring PRL levels, therapeutic drug monitoring for ARI and its main metabolite DARI can help to mitigate the adverse medical consequences associated with PRL reduction. Thus, clinicians should consider the ARI-induced reduction of PRL levels when prescribing ARI to child and adolescent patients, particularly among females.
Introduction
Aripiprazole (ARI) is one of the most widely prescribed atypical antipsychotic drugs for children and adolescents. ARI is used to treat schizophrenia, bipolar disorders, Tourette's syndrome, behavior impairments associated with autism or intellectual disability, attention-deficit/hyperactivity disorder, and other psychiatric disorders. The main advantage of ARI is its good safety profile, with a low potential for adverse effects (Kerwin et al, 2007).
However, recent studies suggest that the adverse effects of ARI are more important in children and adolescents than in adults, particularly weight gain, extrapyramidal effects, metabolic effects, and drowsiness, even though its adverse effects may be less important than those of other atypical antipsychotics (Coustals et al, 2021; Palanca-Maresca et al, 2017; Pozzi et al, 2019; Pringsheim et al, 2017). Therefore, its benefit–risk ratio for children and adolescents should be assessed accurately.
ARI is a partial agonist of dopamine D2 receptors and serotonin 5-HT1A receptors, and a partial antagonist of serotonin 5-HT2A receptors (Shapiro et al, 2003; Uzun et al, 2005). Furthermore, ARI is regarded as a dopamine system stabilizer and it is metabolized by CYP2D6 and CYP3A4. Moreover, ARI undergoes N-dealkylation, hydroxylation, and dehydrogenation, yielding its active metabolite, dehydroaripiprazole (DARI). DARI has pharmacological properties similar to its parent compound with a plasma concentration that is ∼45% of ARI at a steady state (Gupta and Masand, 2004).
According to the Arbeitsgemeinschaft für Neuropsychopharmakologie und Pharmakopsychiatrie (AGNP) consensus guideline, ARI is recommended for therapeutic drug monitoring (TDM) at a recommendation level of two, which means a moderate recommendation. The recommended therapeutic reference ranges for ARI and ARI+DARI are 100–350 ng/mL and 150–500 ng/mL, respectively. The laboratory alert concentration is 1000 ng/mL (Hiemke et al, 2018).
Prolactin (PRL) is a hormone primarily secreted by the lactotroph cells of the anterior pituitary gland stimulated by the inhibitory effect of hypothalamic dopamine (Ben-Jonathan and Hnasko, 2001). Elevated PRL levels comprise common adverse effects of conventional and several other atypical antipsychotics (Besnard et al, 2014; Crespo-Facorro et al, 2017). ARI is a partial dopamine agonist consistently reported to decrease PRL secretion levels. Several studies have reported that combination therapy using ARI can reduce PRL levels in antipsychotic-induced hyperprolactinemia (Chen et al, 2015; Li et al, 2013; Raghuthaman et al, 2015; Zhao et al, 2015).
Other studies show that switching from risperidone to ARI decreases serum PRL levels and improves sexual function in patients with schizophrenia (Chen et al, 2011; Yoon et al, 2016). Reduced PRL levels are associated with reduced sperm quality, erectile dysfunction, hypoandrogenism, a relative degree of infertility in males, and the failure to lactate after pregnancy in females (Gonzales et al, 1989; Safer et al, 2013; Turkington, 1972). In addition, low PRL is associated with immune dysfunction (Fomicheva et al, 2004; Luca, 1997).
Despite these findings, there is limited research on the association between ARI and its metabolite pharmacokinetics and decreased PRL levels in children and adolescents who received ARI treatment. Therefore, this study aims to investigate the relationship between plasma ARI and DARI concentrations and PRL levels in Chinese youth.
Materials and Methods
Participants
This was a retrospective cross-sectional study and the data were collected at Beijing HuiLongGuan Hospital, a Beijing City owned psychiatric hospital, between January 1 and December 31, 2021. Fifty-two child and adolescent inpatients (17 males, 35 females) aged 13–18 years and received ARI regardless of diagnosis were included. The inpatients were all stable and receiving a fixed dose of ARI (5–30 mg/day) orally for at least 1 month. TDM for ARI and measurement of serum PRL levels were included in their routine clinical blood tests according to the physician's orders.
The daily doses were determined by the physician who was treating the patients. This study used patient medical records to obtain clinical information including age, gender, weight, daily dose, the date of last dose adjustment, the time of the last drug intake, the date of blood sampling, psychiatric diagnosis, and combined use of drugs. Patients who received sustained-release ARI were excluded from the study. Furthermore, patients with known physical disorders, such as pituitary disorders and primary hypothyroidism, which may affect serum PRL levels, were excluded.
The study was approved by the review board of Beijing Hui-Long-Guan Hospital. Moreover, written informed consent was not required for the TDM analysis as the determination of plasma concentrations forms part of the clinical routine of the blood test.
Blood sampling
Two blood samples were drawn on the same day, one for TDM of ARI and the other for serum PRL levels measurement and other blood biochemical tests. They were drawn in the morning under fasting conditions generally between 7 and 8 a.m., ∼24 hours after the last dose of ARI. One blood sample was immediately centrifuged for 10 minutes at 3000 g at 4°C. The plasma samples were collected and stored at −20°C until analysis for determination of ARI and DARI, which was completed within 5 days. The other one was subjected to biochemical analysis.
Determination of the plasma concentrations of ARI and DARI
The steady-state ARI and DARI plasma concentrations were measured by high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS/MS). The plasma sample (100 μL) was added to 300 μL of d8-ARI internal standard solution (50 ng/mL in acetonitrile), vortex mixed for 30 seconds, centrifuged at 18620 g for 10 minutes, and then 150 μL of supernatant was injected into the HPLC-MS/MS system. The HPLC analysis was carried out on the LC20A system (Shimadzu, Japan).
Chromatographic separation was performed using a phenyl–hexyl column (Phenomenex, 50 × 4.6 mm, 2.6 μm). A guard column was placed before the analytical column. A binary mobile phase consisting of a mixture of 5 mM ammonium formate and 0.05% formic acid in water (A) and 0.05% formic acid in methanol (B) was used at a flow rate of 0.8 mL/min. The column temperature was 40°C, and the injection volume was 2 μL. The gradient elution was performed according to the following program: 20%–90% mobile phase B from 0 to 0.9 minutes, 90% mobile phase B from 0.9 to 2.0 minutes, and 20% mobile phase B from 2.0 to 3.0 minutes.
The total running time of the analysis was 3.0 minutes. The MS/MS experiments were conducted on a SciexTriple Quad 4500 system (Applied Biosystems, Foster City, CA). All measurements were conducted with a mass spectrometer in positive electrospray ionization mode. The multiple reaction monitoring transitions (Q1/Q3) were 448.2/285.1 for ARI, 446.2/285.1 for DARI, and 456.2/293.1 for ARI-d8. The collision energy was 37 V for ARI, 35 V for DARI, and 40 V for ARI-d8. The declustering potential, entrance potential, and collision exit potential for ARI, DARI, and d8-ARI were 140, 10, and 7 V, respectively.
Other parameters, such as collision gas, curtain gas, ion source gas 1, and ion source gas 2, were 8, 35, 50, and 50 psi, respectively. The dwell time was 10 ms, and the ion spray voltage and temperature were 5500 V and 500°C, respectively. The standard curves of ARI and DARI were linear in the range of 20–1000 ng/mL and 20–1000 ng/mL, respectively.
By adding analytes to blank plasma, four quality control samples (QCs) at four concentrations were prepared: the lower, low, middle, and high limit of quantification with concentrations of 20, 50, 250, and 750 ng/mL for ARI, and 20, 50, 250, and 750 ng/mL for DARI. The intraday/interday precision and accuracy were estimated by analyzing six replicate samples at four different QC concentrations on 3 separate days. The precision and accuracy values of all intraday/interday precision determinations were <±5%. The lower limits of quantification for ARI and DARI were 20 ng/mL. The detection limits of ARI and DARI were 1.2 and 4.9 pg/mL, respectively. The average recovery rates of ARI and DARI were 96% and 92%, respectively.
Determining serum PRL levels
The serum PRL levels were measured in the hospital laboratory by chemiluminescence immunoassay (Beijing Leadman Biotechnology Co Ltd, Beijing, China) using an automatic biochemistry analyzer AU2700 (Olympus, Japan).
Statistical analyses
All statistical analyses were performed using SPSS 20.0. Kolmogorov–Smirnov test to analyze the normality. Descriptive statistics were presented as the mean ± standard deviation (SD) for continuous variables and the rate for discrete variables. Group comparisons on demographic and clinical variables used the χ 2 tests for categorical variables and analysis of variance (ANOVA) for continuous variables. Spearman's rank order correlation analysis was used to assess the correlation between the serum PRL levels and CARI, CDARI, and CARI+CDARI. Modified Bonferroni's method was used to correct possible errors during multiple tests.
Furthermore, multiple regression analysis (i.e., stepwise regression model) was performed to assess the association of serum PRL levels and CARI and CDARI after controlling for confounding factors, including age, gender, weight, dose, and duration of ARI. The significance level was set to p < 0.05.
Results
Demographic and clinical characteristics
Table 1 gives the demographic and clinical characteristics of the participants. A total of 52 child and adolescent inpatients under TDM for ARI were included in this study. There were no significant differences in age, body mass index (BMI), the daily ARI dose, CARI, and CDARI, CARI+CDARI, serum PRL levels, diagnosis, and comedication between males and females (all p > 0.05). The number of patients with CARI below, within, and above the AGNP-recommended concentration range was 6, 40, and 6, respectively. The number of patients with CARI+CDARI below, within, and above the AGNP-recommended concentration range was 7, 41, and 4, respectively.
Demographic and Clinical Characteristics of Participants
ARI, aripiprazole; BMI, body mass index; CARI, concentrations of aripiprazole; CDARI, concentrations of dehydroaripiprazole; DARI, dehydroaripiprazole; F, female; M, male; PRL, prolactin.
None of the patients had CARI or CARI+CDARI above the AGNP-recommended laboratory alert concentrations. The daily ARI dose was positively correlated with CARI (r = 0.658, confidence interval [CI] 95% [0.465–0.844], p < 0.001), CDARI (r = 0.618, CI 95% [0.395–0.821], p < 0.001), and CARI+CDARI (r = 0.664, CI 95% [0.458–0.854], p < 0.001) for all participants, respectively (Fig. 1).

The positive correlations between the daily ARI dose and CARI
There were eight inpatients (three males, five females) with subnormal PRL serum levels, none of whom exhibited any symptoms of subnormal PRL at the time of enrollment in this study. Table 2 gives the differences in demographic and clinical characteristics between inpatients with subnormal PRL levels and those with normal PRL levels. The rate of subnormal PRL serum levels (<63.6 mIU/L in females and <42.4 mIU/L in males) was 17.6% and 14.3% of the male and female children and adolescents among inpatients treated with ARI. Thus, no significant gender difference was found (p > 0.05).
Comparison in Demographic and Clinical Characteristics Between Subnormal Prolactin (PRL) Group and Normal PRL Group
ARI, aripiprazole; BMI, body mass index; CARI, concentrations of aripiprazole; CDARI, concentrations of dehydroaripiprazole; DARI, dehydroaripiprazole; F, female; M, male; PRL, prolactin.
Based on the daily dose of ARI, all subjects were divided into a low-dose group (<10 mg) and a high-dose group (>10 mg). No significant differences were found in gender, age, BMI, PRL, and the PRL subnormal rates in these two groups (all p > 0.05). In addition, the daily dose (7.9 ± 2.3 mg vs. 18.5 ± 3.9 mg), CARI (167.7 ± 152.5 ng/mL vs. 274.5 ± 94.4 ng/mL), CDARI (49.0 ± 41.7 ng/mL vs. 90.3 ± 51.8 ng/mL), and CARI+CDARI (216.8 ± 192.3 ng/mL vs. 364.9 ± 137.9 ng/mL) were significantly higher in the high-dose group than in the low-dose group (all p < 0.05). No significant correlation was found between the daily dose of ARI and the PRL levels, either in the combined group or in the two independent groups (all p > 0.05).
Relationship of steady-state plasma concentrations of ARI and DARI and serum PRL levels in youth
There were significant negative correlations between the serum PRL levels and CARI (r = −0.443, CI 95% [−0.679 to −0.123], p = 0.008) or CDARI (r = −0.432, [−0.672 to −0.109], p = 0.011) or CARI+CDARI (r = −0.460, [−0.691 to −0.144], p = 0.006) in females (Fig. 2). Furthermore, multiple regression analysis revealed that the serum PRL levels were still negatively correlated with CARI (β = −0.406, t = −2.590, p = 0.014) or C DARI (β = −0.470, t = −3.091, p = 0.004) after controlling for age, weight, duration of ARI, diagnosis, and comedication in females. In contrast, no such correlations were found between the serum PRL levels and CARI or CDARI, or CARI+CDARI in males (all p > 0.05).
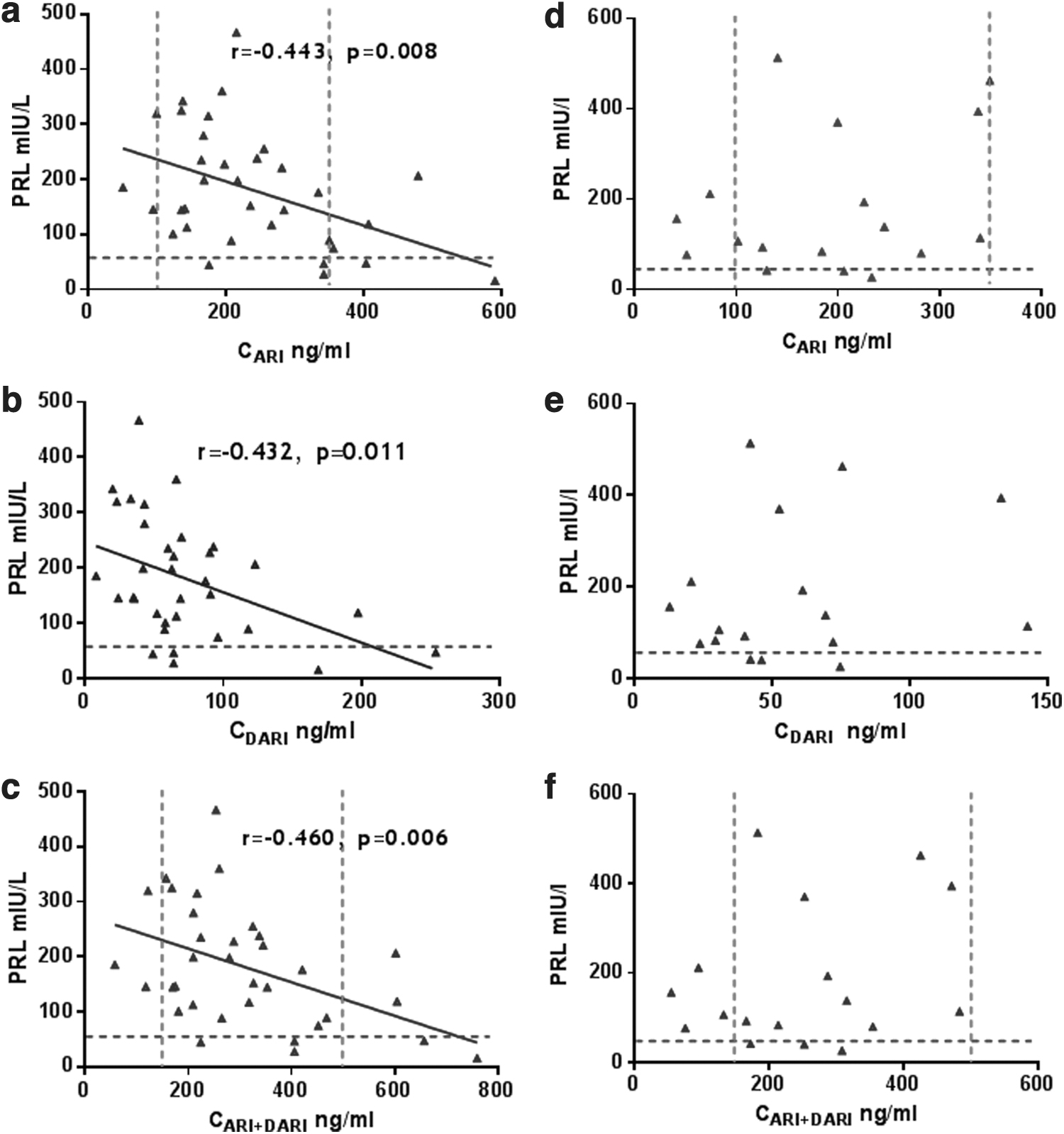
The negative correlations between the serum PRL levels and CARI
Discussion
According to current literature, this is the first study to investigate the relationship between the plasma concentrations of ARI and DARI as well as serum PRL levels in children and adolescents treated with ARI in China.
This study found that the plasma concentrations of ARI and DARI were negatively correlated with serum PRL levels in female children and adolescents treated with ARI in China. The results are similar to a recent study by Tasaki et al (2021a), who showed that plasma PRL levels were inversely correlated with the plasma concentrations of ARI and the active moiety (ARI+DARI) in male and female patients with schizophrenia treated with ARI in Japan. Furthermore, Tasaki et al (2021b) found a negative correlation between PRL levels and the ARI daily dose among 83 male schizophrenia outpatients receiving ARI.
ARI has a unique pharmacological profile as it is a dopamine D2 and serotonin 5-HT1A receptor partial agonist and 5-HT2A receptor antagonist (Uzun et al, 2005). Thus, the D2 partial agonist properties of ARI are likely to attribute to the reduction of serum PRL levels. Previous studies reported that ARI treatment is associated with lower serum PRL levels than other antipsychotic treatments (Crespo-Facorro et al, 2017). ARI combination therapy may lower serum PRL levels, regardless of antipsychotic monopharmacy or polypharmacy, which is independent of dose (Sugai et al, 2020).
Collectively, these studies suggest that patients treated with ARI may exhibit lower PRL levels. In contrast, Sogawa et al (2016) investigated the PRL serum levels in 25 psychiatric patients who were prescribed ARI and found no significant correlation between the PRL levels and the dose of ARI in patients (Sogawa et al, 2016).
This study also found that ∼15% of child and adolescent inpatients treated with ARI exhibited subnormal PRL serum levels. However, the rate of subnormal PRL serum levels in this study was lower than the results from previous studies. For example, Safer et al (2013) reviewed the extent of serum PRL level reduction during ARI treatment in children and adolescents. The researchers found that 60% of children treated with ARI exhibited subnormal PRL serum levels in contrast to 8% of unmedicated participants. Furthermore, the rate of PRL subnormality in response to ARI was 30%–32% and 2%–3%, respectively, in adolescents and adults (Safer et al, 2013).
Sogawa et al (2016) also investigated ARI-related hypoprolactinemia in adult psychiatric patients at a daily dose of 10.8 mg and found a 44% incidence of hypoprolactinemia (Sogawa et al, 2016). Tasaki et al (2021a) reported that 79% and 33% of male and female patients, respectively, had hypoprolactinemia in a sample comprising adult patients with schizophrenia treated with ARI at a daily dose of 10.6 mg for males and 12.4 mg for females. Moreover, Findling et al (2008b) reported a 34% and 26% incidence of subnormal PRL levels in the 10 mg and 30 mg dose groups, respectively, in adolescent patients with schizophrenia treated with ARI for 6 weeks.
Another study by Findling et al (2009b) reported a 25.3% and 39.3% incidence of subnormal PRL levels in the 10 mg and 30 mg dose groups, respectively, in children and adolescent patients with bipolar disorder treated with ARI for 4 weeks. The lower rate of subnormal PRL serum levels in this study may be related to the different diagnoses of the patients recruited, comedication, as well as the dose and duration of ARI treatment. ARI-induced reduction of PRL serum levels became more prominent with increasing doses of ARI and with an increased treatment duration (Safer et al, 2013). Therefore, further studies should be conducted to control these influencing factors.
In this study, the daily dose of ARI ranged from 5 to 20 mg with a mean value of 13.8 mg, the mean values for CARI and CARI+DARI were 228.7 ± 128.9 ng/mL and 297.6 ± 171.8 ng/mL, respectively. About 75% of inpatients had CARI and CARI+DARI within the AGNP-recommended therapeutic reference range. The CARI, CDARI, and CARI+DARI correlated with daily dose of ARI. These results are consistent with previous TDM studies of ARI in children and adolescents (Findling et al, 2009a; Findling et al, 2008a).
Furthermore, a recent study reported a preliminary therapeutic window of 105.9–375.3 ng/mL for ARI in children and adolescents (Egberts et al, 2020). All these studies suggest that the therapeutic reference ranges for ARI in children and adolescents are similar to that established in adults.
This study had several limitations. First, this is a retrospective cross-sectional study and the PRL level of patients before ARI treatment was not available. Therefore, the extent to which ARI treatment reduces serum PRL levels and the incidence of subnormal PRL levels associated with ARI treatment could not be adequately evaluated. Second, the effect of pubertal status on PRL was not considered as the pubertal status of all subjects was not accurately measured in this study. Third, combination medication, particularly for different antipsychotics, has a significant effect on patients' serum PRL levels, but this confounding factor was not considered in this study due to the small sample size.
In future studies, more subjects will be recruited to study the effects of combined antipsychotics. Fourth, no correlation was found between the serum PRL levels and CARI or CDARI in males. Furthermore, this finding should be considered with caution as a small sample size was used. Thus, further study is warranted to evaluate this preliminary result.
Conclusions
In conclusion, this study found that higher plasma concentrations of ARI and DARI were associated with lower serum PRL levels in female children and adolescents treated with ARI. Furthermore, ∼15% of the child and adolescent inpatients treated with ARI exhibited subnormal PRL serum levels. TDM of ARI and its main metabolite DARI and regularly monitoring PRL levels may help to reduce the adverse medical consequences associated with the reduction of PRL. Furthermore, this monitoring can enhance individualized treatment for patients.
Clinical Significance
This study demonstrated that clinicians should consider the ARI-induced reduction of PRL levels when prescribing ARI to patients who are children and adolescents, particularly females.
Footnotes
Acknowledgments
We thank all participants and all coauthors in the study.
Authors' Contributions
F.Y. and H.A. were responsible for the study design, article, preparation, and providing the funding for the study. B.M., W.Z., and Y.Y. were responsible for drug assays. H.F. was responsible for statistical analysis. All authors have contributed to and have approved the final article.
Disclosures
No competing financial interests exist.