
Abstract
Objectives:
Knowledge is limited regarding the adverse effects of therapeutic glucocorticoids on pediatric mental health outcomes. Glucocorticoid-induced psychosis (GIP) is a rare but severe side effect of high-dose glucocorticoid therapy in children and adolescents. This study identified reported pediatric cases of GIP, based on DSM-5 criteria, and defined its presentation, treatments, and outcomes.
Methods:
A systematic review was completed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, including pediatric patients with incident psychosis following glucocorticoid treatment. Patient demographics, clinical presentation, interventions, outcomes, and long-term management were extracted from individual cases.
Results:
Of 1131 articles screened, 28 reports were included, comprising of 31 patients. The mean age was 13 years, and 61% of patients were male. The most common medical illnesses requiring administration of high dose glucocorticoids were asthma (23%) and acute lymphoblastic leukemia (23%). The most common glucocorticoid used was prednisone (35%), and most patients (91%) received doses greater than or equal to 40 mg/day of prednisone. The range of time to symptom onset was 1 day to 7 months. Hallucinations alone (45%) were the most reported feature of GIP. Glucocorticoids were discontinued in 52% of cases, reduced in dosage in 32%, and 81% of affected patients were prescribed psychotropic medications. Long-term management plans and prophylactic psychotropic use were not mentioned in 52% of cases. Symptoms resolved in 90% of patients, and the majority (71%) had no recurrence of psychiatric symptoms.
Conclusions:
GIP can generally be managed by tapering the causative agent with adjunctive second-generation antipsychotics if psychotic symptoms persist. All patients in this review had complete resolution or improvement of their psychotic symptoms; however, there is likely reporting bias due to the expected underreporting of negative outcomes. Managing clinicians must take a circumspect approach when prescribing high-dose glucocorticoids to minimize the risk of serious but preventable side effects.
Introduction
Glucocorticoids are some of the most widely used medications in the world (Yasir et al., 2022). The immunosuppressive effects of glucocorticoids are not only useful in the acute setting but also in the treatment of chronic inflammatory and autoimmune conditions (Cain and Cidlowski, 2017; Yasir et al., 2022). Although clinically significant, these medications are associated with a myriad of adverse effects, including infection, osteoporosis, myopathy, and adrenal suppression (Yasir et al., 2022). The somatic side effects of these powerful anti-inflammatory mediators have been extensively studied and documented; nevertheless, the pathophysiology of glucocorticoid-induced neuropsychiatric events is still poorly understood (Dubovsky et al., 2012).
Therapeutic glucocorticoids were first used in the management of rheumatoid arthritis in 1948, and by the 1950s, there were already several case reports of psychiatric disturbances reported in the literature (Cain and Cidlowski, 2017; Clark et al., 1952). However, the exact mechanism of these neuropsychiatric adverse events has not been established, perhaps due to the complexity and interrelationships of these mechanisms (Dubovsky et al., 2012). For example, serotonergic, noradrenergic, and dopaminergic systems play an integral role in the neuropathology of psychiatric disorders, and there have been well-established relationships between the hypothalamus-pituitary-adrenal (HPA) axis and the aforementioned systems (Bao and Swaab, 2018). There are also proven interactions between the HPA axis and other neuropeptides, monoamines, glutamate, and GABA, which further impact mood and cognition (Bao and Swaab, 2018).
In addition, high doses of glucocorticoids have also been linked to structural changes, such as a decrease in hippocampal volume and brain atrophy (Ciriaco et al., 2013). A clinical example of this relationship is exhibited by Cushing's Syndrome, a condition of glucocorticoid excess, which can manifest as depression, mania, anxiety, and psychosis (Pivonello et al., 2015). Thus, although the exact mechanism is not yet elucidated, cognitive and behavioral changes are generally acknowledged consequences of abnormalities of the HPA axis and steroid excess (Varghese and Brown, 2001).
The total incidence of glucocorticoid-induced neuropsychiatric events reported ranges from 2% to 60%, primarily due to the broad range and vague definitions of symptoms (Dubovsky et al., 2012). Glucocorticoids are linked to neuropsychiatric events ranging from mild irritability to anxiety, delirium, psychosis, and even suicidality; nevertheless, most of our understanding comes from case reports (Warrington and Bostwick, 2006). The term steroid psychosis is used frequently as a label for a diverse group of cognitive, behavioral, and affective syndromes, even if patients do not fit the technical criteria for psychosis (Warrington and Bostwick, 2006). However, this is not due to a lack of a clear definition for true steroid psychosis.
Glucocorticoid-induced psychosis (GIP) is classified under Substance/Medication-Induced Psychotic Disorders in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) (American Psychiatric Association, 2013). Glucocorticoids, specifically dexamethasone, are mentioned as a known cause of GIP (American Psychiatric Association, 2013). Based on the current criteria, the patient must manifest delusions and/or hallucinations during or soon after exposure to glucocorticoids (American Psychiatric Association, 2013). These symptoms must not better be explained by another psychotic or medical condition or other medications/substances and must not occur exclusively during an episode of delirium (American Psychiatric Association, 2013).
A review of GIP in literature was published in 2021, focusing on the pharmacological interventions used in reported cases (Huynh and Reinert, 2021). In their search, they found the use of the aforementioned term steroid psychosis and also steroid-induced psychosis in case reports of other psychiatric disorders that did not meet the DSM-5 criteria of GIP (Huynh and Reinert, 2021). Apart from tapering and discontinuing the causative glucocorticoid, the psychiatric management of GIP varied greatly but all 13 cases included in the study were resolved after a few weeks (Huynh and Reinert, 2021). Most of the inflammatory conditions included were chronic; however, there was no mention of a management plan for future flares or prophylactic antipsychotic use before glucocorticoid treatment (Huynh and Reinert, 2021).
In addition, patients under the age of 18 were excluded from the 2021 systematic review (Huynh and Reinert, 2021). Although rare, pediatric GIP can occur; however, there is currently no well-defined rate of incidence reported (Bag et al., 2012). Apart from a brief review of cases in a study in 2018, there have been no recent trials or systematic reviews of GIP in a pediatric population (Hodgins et al., 2018). Therefore, a comprehensive literature search of GIP in children and adolescents is needed to serve as a reference point and summary of reported cases and potentially identify any other forms of literature available.
This study will aim to identify reported pediatric cases of true GIP, according to DSM-5 criteria, and to provide a better understanding of the clinical presentation of GIP in children and adolescents. It hopes to provide valuable insight into the treatments and outcomes of psychosis in this population. In addition, this study will report any long-term management plans related to GIP implemented in children with chronic inflammatory conditions. Ultimately, this review hopes to act as an important step toward formulating a rational treatment pathway for this rare but severe side effect.
Methods
Protocol and registration
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Supplementary Data S1) (Page et al., 2021). The protocol for this review is registered in the PROSPERO online database (University of York, Centre for Reviews and Dissemination; Registration number: CRD42022311901) (Supplementary Data S2).
Search strategy and information sources
P.F.M. developed a search strategy, combining terms for GIP and children and adolescents (Supplementary Data S3) and systematically searched electronic databases, including Scopus, Medline, Embase, PsycINFO, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews on April 24, 2022.
Eligibility criteria
Studies that met the following criteria were included: (1) patients 5–18 years old, (2) use of oral, intravenous, or inhaled glucocorticoids, (3) any credited source (e.g., case reports, case series, letters to the editor, literature reviews, and so on) that described the patient's presentation, and (4) patients presenting with psychosis after glucocorticoid use (as described and diagnosed by authors of the reports), as per the current DSM-5 criteria (Fig. 1). Children under the age of five were excluded since psychosis cannot be confidently diagnosed in this population (Garralda, 2016).

Simplified DSM-5 diagnostic criteria for Substance/Medication-Induced Psychotic Disorder, modified for GIP. DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th Edition; GIP, glucocorticoid-induced psychosis.
Study selection
Using EndNote20, P.F.M. screened references after manually removing duplicates. P.F.M. initially reviewed titles and abstracts, removing those that clearly did not meet the full inclusion criteria. P.F.M. and J.B. then independently evaluated the remaining full-text articles and excluded those that did not meet the inclusion criteria. P.F.M. also conducted a reference search of all included studies. Any disagreements were discussed with M.S.C.
Extraction of cases
P.F.M. extracted information from articles using an excel template. P.F.M. extracted (1) patient demographics (i.e., patient age and sex) and study characteristics (i.e., year of publication), (2) medical illness requiring glucocorticoids, (3) glucocorticoid used (i.e., type, dose, route of administration), (4) psychiatric course of illness (i.e., presence and duration of psychotic symptoms), (5) clinical interventions (i.e., changes in glucocorticoid management of medical illness, psychotropic medications), and (6) outcome and long-term management used.
Critical appraisal of studies
Due to the subjective reporting in case studies and case series, these forms of literature are at the bottom of the hierarchy of evidence (Murad et al., 2016). Consequently, a quality assessment tool was not needed in this systematic review.
Case analysis
Frequencies and percentages were used for categorical variables and means and range for continuous variables. Time to symptom onset was reported as a range due to the inconsistencies and approximate reporting of this information across the literature. Glucocorticoid dose equivalency was estimated using a Steroid Conversion Calculator (Steroid Conversion Calculator: Pediatric Oncall, 2022). In cases where weight and height were not reported but the dosage was only given in mg/(kg·day) or mg/(m2·day), an online calculator was used to estimate the weight and body surface area based on age (Average Height to Weight Chart: Babies to Teenagers, 2017).
Results
Study characteristics
A PRISMA flow diagram of study selection is outlined in Figure 2. A total of 1131 records were identified from six databases. The records were screened for duplicates, and 268 duplicates were removed manually. A total of 784 records were then excluded based on titles and abstracts, and 79 records were sought for retrieval. Of the remaining records, 51 were excluded. Of the excluded articles, 11 did not confirm psychosis, 10 reported psychosis due to another cause, 12 cases were over the age of 18, eight were not in English, 7 were abstracts only, and 3 described delirium. Through reference searching, five reports were retrieved, but only one met the eligibility criteria. A total of 28 studies met the inclusion criteria, comprising of 31 cases, which include 20 case reports, 4 case series, 3 letters to the editor, and 1 case report written as a clinical quiz.
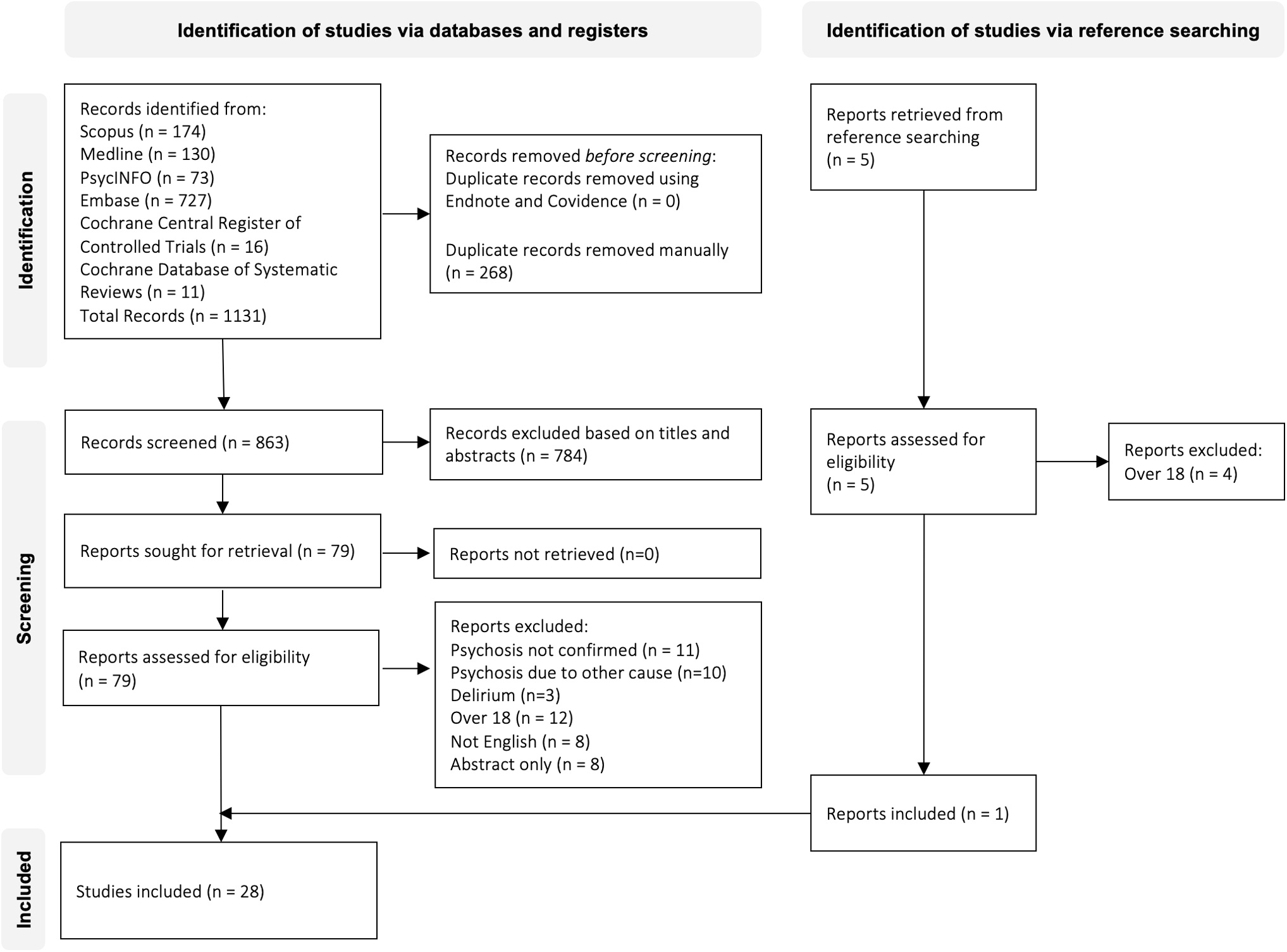
PRISMA flow diagram of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Patient demographics and clinical presentation
Details of patients' psychiatric presentations are available in Table 1. Of the 31 patients, the mean age was 13 years old with a range of 5–18 (Table 2). A total of 16 (61%) patients were males, and 12 (39%) were females (Table 2). The most common medical illnesses that required the administration of high dose glucocorticoids were asthma (7 [23%]), acute lymphoblastic leukemia (7 [23%]), Crohn's disease (4 [13%]), nephrotic syndrome (4 [13%]), and ulcerative colitis (2 [7%]) (Table 2). Other indications reported once (3%) include bimaxillary osteotomy, dermatomyositis, discoid lupus erythematosus, Hodgkin's lymphoma, systemic lupus erythematosus, mumps orchitis, and toxic epidermal necrolysis (Table 2).
Summary of the Glucocorticoid-Induced Psychosis Cases
Prednisone dose equivalency calculated using the Pediatric Oncall Steroid Conversion Calculator (Steroid Conversion Calculator: Pediatric Oncall, 2022).
Assuming 1 g for “high dose” glucocorticoids.
Assuming weight and height based on age and sex (Average Height to Weight Chart: Babies to Teenagers, 2017).
—, Prednisone dose equivalency not known or not reported.
ACTH, adrenocorticotropic hormone; ALL, acute lymphoblastic leukemia; bid, twice daily; BSA, body surface area; CPZ, Chlorpromazine; ECT; electroconvulsive therapy; EPS, extrapyramidal symptoms; F, female; GC, glucocorticoid; ICS, inhaled corticosteroid; IM, intramuscular; IV, intravenous; M, male; mane, in the morning; nocte, at night; PO, orally; PRN, as required; q6h, every 6 hours; qad, every other day; qid, four times daily; tds, three times daily; tx, treatment.
Characteristics of Patients with Glucocorticoid-Induced Psychosis (n = 31)
The most common glucocorticoid used was prednisone alone (11 [35%]), followed by combination glucocorticoid therapy (7 [23%]), methylprednisolone (4 [13%]), prednisolone (3 [10%]), dexamethasone (4 [13%]), and beclomethasone dipropionate (2 [6%]) (Table 2). Most glucocorticoids were administered orally (17 [55%]) or in combination (7 [23%]) (Table 2). Intravenous glucocorticoids alone were administered to 5 (16%) patients, and 2 (6%) patients received inhaled glucocorticoids (Table 2). Most patients (28 [91%]) received doses greater than or equal to 40 mg/day of prednisone, while 1 (3%) patient received a dose <40 mg/day of prednisone, and 2 (6%) patient's dose equivalency is unknown (Table 2).
The range of time to symptom onset was 1 day to 4 months, but of the 31 patients, 15 (48%) presented with psychosis <1 week following pulse glucocorticoid therapy, 13 (42%) presented between 1 week and 1 month, and 3 (10%) presented 1 month after continued glucocorticoid treatments (Table 3). The most reported sign of psychosis was hallucinations alone (14 [45%]), followed by both hallucinations and delusions (8 [26%]) and delusions alone (9 [29%]) (Table 3).
Clinical Presentation and Interventions of Patients with Glucocorticoid-Induced Psychosis (n = 31)
Clinical interventions
All 31 patients were hospitalized in some capacity as they required both medical and psychiatric stabilization. Glucocorticoids were discontinued in 16 (52%) patients and reduced in 10 (32%) (Table 3). A total of three (10%) patients had no change in their glucocorticoid management, and two (6%) cases did not state if the glucocorticoids were stopped or continued (Table 3). Only six (19%) cases did not use any psychotropic medications in the management of GIP (Table 3). Most patients received combination therapy (10 [32%]), followed by monotherapy with risperidone (5 [16%]), chlorpromazine (3 [10%]), quetiapine (2 [7%]), diazepam (2 [7%]), sertraline (1 [3%]), and olanzapine (1 [3%]) (Table 3). Only one (3%) case mentioned the use of psychotropics but did not name the medications used (Table 3).
Long-term management plans and prophylactic use of psychotropics were not mentioned in 16 (52%) cases, but 10 (32%) used psychotropic medications, 3 (10%) modified the medical management of the condition requiring glucocorticoids, and 1 (3%) patient received family and individual therapy in addition to psychotropics (Table 3). Of the 31 GIP cases, 28 (90%) resolved completely while 3 (10%) improved (Table 3). There was a recurrence of psychiatric symptoms in seven (22%) patients (Table 3). Two (7%) patients were lost to follow-up (Table 3).
Discussion
This systematic review summarizes the currently available published literature on clear DSM-5 classifiable GIP in children and adolescents (Table 1). The review of GIP in a pediatric population published in 2018 composed of 15 cases, and in comparison, this systematic review was able to identify 31 cases due to the comprehensive search strategy outlined in Supplementary Data S3 (Hodgins et al., 2018). The small sample size of patients met the inclusion criteria of this review and the likelihood that cases with less clear-cut diagnostic features of GIP potentially limits the generalizability of the findings; however, the study provides well-needed insight into this rare side effect.
A recent protocol for managing GIP in adults is glucocorticoid tapering to <40 mg/day, as the first step, plus an atypical antipsychotic and lithium (Zagaria, 2016). The Boston Collaborative Drug Surveillance Program found that 4.6% of 718 hospitalized adult patients receiving >40 mg/day of prednisone presented with psychiatric symptoms (The Boston Collaborative Drug Surveillance Program, 1972). Most patients in this systematic review received a prednisone equivalent dose of 40 mg/day or higher, with only 1 out of the 31 cases receiving a dose of 25 mg/day (Table 2). This suggests a dose-dependent relationship in GIP manifestations and that doses under 25 mg/day are less likely to cause GIP in children and adolescents. However, many cases did not report glucocorticoid doses in appropriate units for a pediatric population (Table 1). Consequently, dose-dependent assumptions are difficult to make, considering a dose of 40 mg/day is distributed very differently in a 5-year old compared to a 17-year old (Batchelor and Marriott, 2015).
The time to symptom onset ranged from 1 day to 4 months; however, 48% of patients presented with psychosis <1 week following glucocorticoid therapy (Table 3). Although variable, the onset of psychotic symptoms aligned with the notion that GIP is more common in patients receiving pulse glucocorticoids. In addition, patients who had a more prolonged time to symptom onset were receiving continuous treatment with high dose glucocorticoids. Every patient also manifested other psychiatric symptoms, such as depression, catatonia, aggression, anxiety, regression, and even suicidality, as described in Table 1. The impact of glucocorticoids on mood and cognition, as exhibited by the diversity in the psychiatric presentations in this study, is consistent with the proven interactions between the HPA axis and serotonergic, noradrenergic, and dopaminergic systems (Bao and Swaab, 2018). While it is beyond the scope of this study to examine all neuropsychiatric side effects of glucocorticoids, it is important to note that the mood and behavioral symptoms can still be debilitating in the absence of frank psychosis.
All but three patients had a change in their glucocorticoid regime, but the three that did not were given prophylactic and concomitant risperidone with further glucocorticoid treatment. Nine other cases also used psychotropic medications and modified the glucocorticoid dose, while three opted to modify the medical management of the condition requiring glucocorticoids. Long-term management plans were not mentioned in 16 (52%) cases, even though 13 of the 16 patients had chronic conditions.
The absence of a management plan in this cohort is worrying since it is likely that these patients would require high dose glucocorticoids for treatment of future flares. In addition, three patients in this study had suicide attempts, and one patient was detained under the mental health act (Beshay and Pumariega, 1998; Doherty et al., 1991; Fleming and Flood, 2005; Kramer and Cottingham, 1999). These cases highlight the severe consequences of GIP and the need for a management plan. Studies have shown that management plans, such as the personalized Asthma Action Plan, can improve the patient's quality of life and increase their knowledge and confidence about their lifelong condition (Goronfolah et al., 2019). In the case of GIP in an asthmatic, for example, a section can be added to the asthma action plan by the treating physician to include a warning of GIP as an adverse event following glucocorticoid use and to alert clinicians to consider a reduction in the dose or the use of psychotropic medications to manage GIP.
A possible GIP treatment pathway has been outlined based on the 31 cases included in this review (Fig. 3). Depending on the medical illness, patients presenting with hallucinations and/or delusions during or post high-dose glucocorticoid treatment should initially have their glucocorticoid dose tapered and/or discontinued if possible, after a full psychiatric assessment. If psychotic symptoms persist, second-generation antipsychotics (SGAs), like risperidone, can be used due to their favorable side effect profile (Briles et al., 2012). The Australian Clinical Guidelines for Early Psychosis also recommend SGAs in substance-related psychotic disorders (Early Psychosis Guidelines Writing Group and EPPIC National Support Program, 2016). In cases where glucocorticoids cannot be tapered and/or discontinued due to the severity of the patient's inflammatory condition, SGAs can be used as part of the patient's management plan for future flares.

Potential treatment pathway for GIP in children and adolescents. When possible, clinicians should taper and discontinue the causative agent. If psychotic symptoms persist, a SGA can be used. In cases where glucocorticoids cannot be tapered and/or discontinued due to the severity of the patient's inflammatory condition, SGAs can be used prophylactically and concomitantly. GIP, glucocorticoid-induced psychosis; SGA, second-generation antipsychotic.
In contrast, the pharmacological management of GIP in adults consists mainly of haloperidol, followed by risperidone (Huynh and Reinert, 2021). Consequently, longitudinal studies are needed to establish more reliable methods for patient management and predict at-risk pediatric patients. While it is beyond the scope of this review to identify potential risk factors for GIP, it should be noted that none of the patients included had a prior history of psychotic illness.
Limitations
As with any systematic review, there is the risk of unintentionally omitting relevant literature. In addition, the inconsistencies in reporting GIP and the misuse of the term steroid psychosis further complicated this search. To combat the issue, very comprehensive search terms were used in this systematic review, as outlined in Supplementary Data S3. This study focused on only GIP, but corticosteroids and steroids were included in the search terms to ensure that literature incorrectly referring to glucocorticoids was included. In addition, only articles available in English were included, which could lead to a potential loss of relevant data.
Several limitations also prevent a clearer understanding of GIP in children and adolescents. The currently available literature consists almost entirely of case reports and case series, and although case reports provide valuable information regarding rare conditions, they are on the lower end of the quality scale, ranked as 4c for case series and 4d for case studies (Aromataris and Munn, 2020). Pediatric patients have a smaller volume of distribution, lower bioavailability, and a faster metabolism compared to adults; thus, pediatric dosing is better represented as mg/(kg·day) or mg/(m2·day) (Batchelor and Marriott, 2015). However, very few of the included cases reported doses with appropriate units or provided the body weights or body surface area of patients (Table 1). Consequently, a limitation of this study is the inconsistent reporting of dosage, body weights, and body surface area in the individual case reports, which are critical for accurate drug dose adjustments in children. In addition, the inconsistencies in reporting made it difficult to determine the range of time to symptom from the very first glucocorticoid dose, exact time frame of resolution, and the follow-up time of each patient.
Although this systematic review reported 31 cases of GIP with the age range of 5–18, it should be noted that the literature search did yield 2 cases of GIP in much younger children, aged 2 and 4 (Alsalamah and Alsahali, 2021; Ingram and Hagemann, 2003). However, in both cases, the children were too young for the hallucinations to be confirmed (Alsalamah and Alsahali, 2021; Ingram and Hagemann, 2003). Hallucinations in very young children have been known to be part of their normal development and may not always be confidently linked to a psychotic state in this population (Edelsohn, 2006). Night terrors, illusions, or sensory misrepresentations might be misinterpreted as hallucinations, complicating the firm diagnosis of GIP in very young children (Garralda, 2016). Younger children are vulnerable to glucocorticoid induced neuropsychiatric side effects; however, since case reports are lower quality evidence, we could not confidently ascertain if these young children were experiencing GIP. The currently available literature on GIP on a very young population is currently very sparse, and more studies are needed for this under-represented population.
A significant concern is also publication bias, as clinicians may be less likely to report cases with poor outcomes (Nissen and Wynn, 2014). Every patient in this study had resolution or improvement in their psychotic symptoms, suggesting a positive overall outcome of GIP; however, it is possible that cases that did not improve or culminated in completed suicide attempts would not be published by the treating clinicians. Furthermore, a cause-effect relationship cannot be established from an uncontrolled observation, making it hard to generalize information from a case report (Nissen and Wynn, 2014). Randomized control trials (RCTs) are needed to determine the frequency of GIP, as well as potential risk factors. However, since RCTs of rare and life-threatening conditions are practically difficult, especially in vulnerable populations such as children and adolescents, case reports can provide valuable information in these instances (Nissen and Wynn, 2014).
Conclusion
GIP is a rare but severe side effect of high dose glucocorticoids in children and adolescents. As evidenced by this small number of patient cases, GIP can generally be managed by tapering the causative agent with adjunctive SGAs if psychotic symptoms persist. Although the patients in this review all had complete resolution or improvement in their psychotic symptoms, there is likely reporting bias due to the expected underreporting of negative outcomes. Managing clinicians must take a circumspect approach in prescribing high doses of glucocorticoids, to minimize the risk of serious but preventable side effects.
Clinical Significance
Glucocorticoids are associated with a myriad of adverse effects, and although rare, GIP can significantly impact the lives of affected individuals. Children and adolescents are particularly vulnerable to glucocorticoid induced neuropsychiatric side effects; however, psychosis can be difficult to diagnose in this population. Moreover, the currently available literature on GIP in children and adolescents is sparse and consists mostly of case reports and case series. In this study, we present a comprehensive systematic review of the literature, highlighting 31 patients with confirmed GIP as per the DSM-5 criteria, and summarizing the clinical presentations and interventions. In addition, we outline a potential treatment pathway for GIP based on the 31 cases. Ultimately, we hope to provide clinicians with some insight into recognizing and managing this severe side effect in children and adolescents.
Footnotes
Authors’ Contributions
P.F.M.: conceptualization (lead); methodology (lead); writing—original draft (lead); formal analysis (lead); writing—review and editing (equal). J.B.: methodology (supporting); writing—original draft (supporting); writing—review and editing (equal). M.S.C.: conceptualization (supporting); methodology (supporting); writing—original draft (supporting); writing—review and editing (equal).
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.