
Abstract
Objectives:
Childhood mental illness is an ongoing public health crisis which is accompanied by an increase in antidepressant (i.e., serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors) use in children. Recent evidence highlighting the cultural differences in the utilization, efficacy, and tolerability of antidepressants in children underscores the need for diverse samples in studies examining antidepressant use. Furthermore, the American Psychological Association in recent years has emphasized the importance of including participants from diverse backgrounds in research studies, including investigations of medication efficacy. The present study, therefore, examined the demographic composition of samples used and reported in antidepressant efficacy and tolerability studies with children and adolescents experiencing anxiety and/or depression in the last decade.
Methods:
A systematic literature review utilizing two databases was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. In line with the extant literature, antidepressants were operationalized as Sertraline, Duloxetine, Escitalopram, Fluoxetine, and Fluvoxamine.
Results:
Out of the 11 articles included in this review, 71% reported having a primarily adolescent sample (i.e., over 50% of the sample was 12 years or older). In addition, all studies omitted any transgender, genderqueer, or gender-nonconforming demographics, and one study omitted all racial demographic information. While 64% of studies only partially reported racial demographic information, 36% of studies omitted ethnicity demographics altogether.
Conclusions:
The present study addresses a gap in the literature by supporting a lack of diversity in studies examining antidepressant use in children and adolescents. Furthermore, it underscores the importance of future studies using a more diverse and representative sample. Limitations of the present study included limited generalizability and the lack of independent and blind reviewer process. Possible explanations for the lack of inclusion and suggestions on how to address these disparities are discussed.
Introduction
Childhood mental health
The youth mental health crisis in the United States is a public health concern, with ∼7.7 million children between the ages of 5 and 17 meeting the criteria for at least one mental health disorder in the last year (American Psychiatric Association, 2013). These rapidly increasing mental health concerns are associated with a notable increase in the use of psychotropic medications in children and adolescents (Garfield et al., 2015). Affective disorders, such as anxiety (i.e., feelings of uncontrollable worry, fear, and hyperarousal) and depression (i.e., feelings of sadness, loss of interest and pleasure in activities, disruption in sleep and appetite), are a particular concern among this population. Specifically, rates of anxiety and depression have increased by 27% and 24% from 2016 to 2020, respectively. Approximately 5.6 million children (9.2%) were diagnosed with anxiety and 2.4 million (4.0%) with depression in 2020 (Lebrun-Harris et al., 2022).
In addition, recent literature, including a meta-analysis by Racine et al. (2021), has demonstrated that the COVID-19 pandemic has exacerbated rates of anxiety and depression in youth (age ≤18 years). Specifically, before COVID-19, ∼12.9% of youth experienced symptoms of depression and 11.6% experienced symptoms of generalized anxiety, and after the first year of the pandemic, these rates increased to 25.2% and 20.5%, respectively (Racine et al., 2021).
The rapid increase in rates of childhood anxiety and depression is particularly concerning given the detrimental outcomes associated with these disorders. Specifically, it has been established that childhood onset of anxiety and depression is predictive of a poorer prognosis and is often accompanied by more severe and chronic symptoms. In addition, depression and anxiety can persist throughout the lifetime, with lifetime prevalence rates of 20% (Dwyer and Bloch, 2019) and 34% (Bandelow and Michaelis, 2015), respectively. Childhood anxiety and depression are widespread, pervasive, and debilitating, which underscores the importance of investigating selective serotonin reuptake inhibitor (SSRI) use within this population.
Cultural differences in anxiety and depression
Distinct differences in the incidence rates of anxiety and depression exist across genders. Before adolescence, the incidence of these disorders between boys and girls is similar; however, the onset of anxiety and depression peak during adolescence (i.e., postpuberty), and girls are at a significantly greater risk of developing anxiety and/or depression (American Academy of Child and Adolescent Psychiatry, 2020; Van Droogenbroeck et al., 2018). This trend extends through adulthood, as women have double the lifetime rates of major depressive disorder (MDD) and most anxiety disorders (e.g., generalized anxiety disorder [GAD], panic disorder, and specific phobias) compared to men (Brody et al., 2018; McLean et al., 2011; Skarl, 2015).
In addition, epidemiological studies reveal that transgender and gender-nonconforming youth appear to experience anxiety and depression at higher rates compared to their cisgender peers (Chodzen et al., 2019), and this increased occurrence is associated with stigma and discrimination experienced by gender minorities (Puckett et al., 2020).
Differences in presentation and rates of anxiety and depression across race and ethnicity have also been documented; however, these differences have primarily been examined among adult populations. The research examining anxiety and depression prevalence in youth across race and ethnicity is limited, and findings are inconsistent (McLaughlin et al., 2007; Parodi et al., 2022). There are, however, long-standing concerns regarding the underdiagnosis of anxiety and depression in youth ethnic and racial minorities, as cultural factors that should inform diagnoses are often not considered (e.g., differences in symptom presentation and levels of stigma) (Marques et al., 2015; Varela and Hensley-Maloney, 2009). For example, evidence from epidemiological research supports an elevated risk for anxiety disorders in Hispanic youth relative to non-Hispanic whites and indicates that anxiety may be differentially related to parental strategies and family dynamics (Georgiades et al., 2018; Varela and Hensley-Maloney, 2009). Other factors associated with cross-cultural differences in anxiety and/or depression include collectivism and social strategies (Enrique Varela et al., 2004), uninvolved parenting, racial discrimination, and criminal victimization (Assari et al., 2017; Simons et al., 2002).
Pediatric psychotropics
Due to the identification and increased attention to childhood mental health disorders in the United States, the use of psychotropic medications in children and adolescents has magnified. Data from the National Health Interview Survey (2019) indicated that 8.4% of children ages 6–17 used psychotropics to treat their mental and behavioral concerns in 2019, compared to 7.4% in 2012 (Howie et al., 2015; Zablotsky and Terlizzi, 2020). The increase in psychotropic use may also be related to the need-to-access gap in mental health services for youth, as the mental health provider workforce is unable to meet the demand for evidence-based interventions (Schleider et al., 2020). Notable differences among sex, race, and ethnicity were evident, with a higher percentage of males (9.8%) using medication compared to females (7.0%) (Zablotsky and Terlizzi, 2020). Use of medication was highest for non-Hispanic white children (11.4%), followed by non-Hispanic black children (5.6%) and Hispanic children (4.7%) (Zablotsky and Terlizzi, 2020).
There are also notable differences across age groups in the utilization of psychotropics, with older females having a higher percentage (6.3%) than younger females (4.0%), but no differences emerged by age group for males (Zablotsky and Terlizzi, 2020). Furthermore, 6.2% of children ages 9–11 were prescribed medication for their mental health compared to 10.9% of ages 12–17 (Zablotsky and Terlizzi, 2020). Differences across sex shift when examining the utilization of psychotropics in adolescents, particularly across antidepressants (Jonas et al., 2013). Among those aged 12–19, females were more likely than males to report the use of antidepressants in the past month (4.2% and 2.2%, respectively) (Locher et al., 2017).
As the need for pharmaceutical interventions for childhood mental health disorders rapidly increases, pediatric practitioners must make challenging decisions regarding which medications to prescribe. The evidence for the use of psychiatric medications in children, however, is not as well established relative to that of adult psychiatry (Dwyer and Bloch, 2019). Prescribing to young children is particularly challenging, as the majority of psychotropic prescribing is “off-label,” meaning that the medication has not been tested and approved by the Food and Drug Administration (FDA) for use in this age group (Garfield et al., 2015). Among these, commonly prescribed psychotropic medications include SSRIs and serotonin-norepinephrine reuptake inhibitors (SNRIs), which are most frequently used to treat anxiety and depression (Jonas et al., 2013).
Antidepressants (SSRIs and SNRIs)
Antidepressants are the first line of defense when treating childhood depression and anxiety, despite the lack of consistent results demonstrating the overall efficacy of these medications (Boaden et al., 2020). For example, in the context of major or severe depression, a meta-analysis evaluating 34 clinical trials for the efficacy and tolerability of antidepressants in children and adolescents found that fluoxetine was the most tolerable antidepressant and the only one that was significantly more effective than placebo (Cipriani et al., 2016). Several antidepressants (primarily SSRIs and SNRIs) have been approved by the FDA for pediatric use (i.e., ages ranging from 6 to 12 and older) for GAD, MDD, and bipolar depression (Table 1).
Food and Drug Administration Approved Antidepressants for Children
FDA, Food and Drug Administration; GAD, generalized anxiety disorder; MDD, major depressive disorder; OCD, obsessive-compulsive disorder; SNRI, serotonin-norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
Prescribing antidepressants off-label is a common and accepted practice in the medical field, and subsequently, children may be prescribed antidepressants at younger ages and for disorders that differ from those approved by the FDA (American Academy of Child and Adolescent Psychiatry, 2020; The American Academy of Child and Adolescent Psychiatry, 2018). Off-label antidepressants often prescribed to children include sertraline (Zoloft™), fluoxetine (Prozac™), fluvoxamine (Luvox™), paroxetine (Paxil™), and venlafaxine ER (Effexor XR™) (Assari et al., 2017; Locher et al., 2017).
Cultural differences in antidepressant efficacy and utilization
Similar to the cultural differences observed in the presentation and prevalence of anxiety and depression, cultural differences in antidepressant efficacy and utilization have been documented in the literature. For example, Chinese patients with depression were found to require lower dosages of an antidepressant (i.e., Sertraline) to achieve clinical efficacy compared to white patients (Chen et al., 2009; Ng et al., 2006). In a study with black and white Americans, Murphy et al. (2013) also found group differences across medication responses. Specifically, they observed a lower effect of antidepressant treatment among black Americans, which persisted despite controlling for primary predictors (i.e., socioeconomic and baseline clinical factors) of racial differences (Murphy et al., 2013). Findings indicated that genetic African ancestry predicted poorer treatment response across models beyond that predicted by socioeconomic and baseline clinical factors and revealed an additional influence of genetic ancestry on the remaining variability (Murphy et al., 2013).
Cultural differences, such as ethnicity and race, have also been associated with the metabolism and disposition of medications (i.e., pharmacokinetics) and the interactions of those medications with therapeutic targets (i.e., pharmacodynamics). As noted by Chen et al. (2009, p. 283), “Genes controlling the expression of drug-metabolizing enzymes as well as the function of the brain are highly polymorphic, and the patterns and distribution of these polymorphisms are typically divergent across ethnic groups,” therefore impacting vulnerability to psychological disorders and drug response. Furthermore, research has also demonstrated differences across ethnic, racial, and gender groups regarding the utilization of antidepressants. Research indicates that people of color and other underrepresented groups typically have poorer access to mental health care, utilize their health care at a lower rate, are less likely to be prescribed and to fill prescriptions for newer antidepressants, and are less likely to receive nonpharmacological treatment relative to white Americans (Lesser et al., 2010).
Despite the equal or greater need for psychiatry and psychological interventions, research also indicates that barriers to health care access also impact the underutilization of antidepressants by refugees, first-generation immigrants, and non-English speaking populations (Derr, 2016; Taipale et al., 2021). In addition, wide racial and ethnic differences in the utilization of antidepressants specifically by adolescents also exist. In a representative sample of U.S. adolescents, researchers found that non-Hispanic white adolescents were more than twice as likely as Hispanic adolescents, and over five times as likely as non-Hispanic black adolescents, to use antidepressants (Kirby et al., 2010). Further examination through decomposition analysis indicated that racial and ethnic differences in characteristics such as household income, parental education, health insurance, and source of care explained between one-half and two-thirds of the gap in antidepressant use between Hispanics and non-Hispanic whites, but none of the gap between whites and blacks (Kirby et al., 2010).
Additional factors associated with differences in antidepressant utilization include contextual variables (e.g., economics, availability, and accessibility of services), patient variables (e.g., differences in prevalence or manifestation of the disorder, cultural beliefs, and attitudes, preferential use of alternative or informal services, health literacy, and adherence), and provider variables (e.g., referral bias and patient–provider communication) (Stewart et al., 2012). Furthermore, antidepressant utilization in children and adolescents is also associated with racial and ethnic differences in parental perceptions about the risks and benefits of antidepressants and their expectations of providers (Stevens et al., 2009). Findings by Steven and colleagues (2009) revealed that black parents had less favorable views of antidepressants compared to other parents.
Underrepresentation of culturally diverse groups in research
The underutilization of antidepressants by diverse groups is likely associated with the underrepresentation of these groups in research studies. Research samples have historically excluded marginalized groups and people of color (Roberts et al., 2020). The explanation for the exclusion of diverse populations is multifaceted. The use of convenient sampling in psychological research has often resulted in sampling from Western, educated, industrialized, rich, and democratic (WEIRD) populations (Henrich et al., 2010; Rad et al., 2018). Moreover, theories and practices of Western mental health and psychological research have been elevated, while that of other historically marginalized groups have been devalued (Settles et al., 2020).
Exclusionary practices maintained by sampling biases and a lack of multiculturally informed theories have culminated in the wide underrepresentation of diverse groups (e.g., racial, ethnic, sexual, and gender minorities) in psychological research and consequently impact the validity of psychiatric and psychological research findings and promote inequality, health disparities, and underutilization of services across marginalized groups (Boaden et al., 2020; Monahan et al., 2022; Nalven et al., 2021). To address these disparities and allow for critical reviewing, guidelines such as those shared by the American Psychological Association (2020) and American Psychological Association (2019) suggest reporting the characteristics of the sample as specifically as possible, highlighting characteristics that may impact the interpretation of findings. Major demographic characteristics that should be reported include age, sex, ethnicity, race, nationality, level of education, socioeconomic status, immigrant status, disability status, sexual orientation, gender identity, and language preference.
Present review
The current mental health crisis and the increased use of antidepressants in children and adolescents require further evaluation of the efficacy and tolerability of these psychotropics. When evaluating antidepressant efficacy and tolerability, age must be considered, because antidepressants are often prescribed off-label to younger children. Furthermore, it is important to consider gender, race, and ethnicity as there appear to be disparities across groups regarding the efficacy, tolerability, and rate of use of antidepressants. Thus, the present systematic review aimed to identify and summarize the literature examining the demographic composition and diversity of samples used and reported in antidepressant efficacy and tolerability studies among children and adolescents being treated for depression and anxiety.
Methods
Search and retrieval
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a systematic review of the literature was conducted to examine the demographic composition of children and adolescent samples used in antidepressant efficacy and tolerability studies in the last decade (Page et al., 2021). PRISMA guidelines are designed to facilitate a broad search of databases using specific keywords and search terms, screening articles based on title, conducting an abstract review, conducting a full-text review, and identifying all remaining articles that meet the final inclusionary criteria. Given the availability of medications in the extant literature, antidepressants were operationalized as Sertraline, Duloxetine, Escitalopram, Fluoxetine, and Fluvoxamine.
The literature search was completed in September 2022. Two reviewers (E.R. and A.B.) identified the articles for final inclusion, while one reviewer (E.R.) extracted and compiled the pertinent information into two tables (Tables 2 and 3). A second reviewer (A.B.) reviewed the extracted information for accuracy. All researchers involved in search and data retrieval were trained according to study protocols. A combination of the following key terms was searched within the bibliographic databases PubMed and PsycINFO: Children, and SSRI, and Efficacy study, and Treatment, and Antidepressants, and Sertraline or Duloxetine, or Escitalopram, or Fluoxetine, or Fluvoxamine.
Summary of Included Articles
GAD, generalized anxiety disorder; MDD, major depressive disorder; NIMH, National Institute of Mental Health; SAD, separation anxiety disorder; SNRI, serotonin-norepinephrine reuptake inhibitor; SOP, social phobia; SSRI, selective serotonin reuptake inhibitor.
Summary of Included Articles: Demographics
The distribution across locations was not reported.
Study did not report disaggregated data based on age (e.g., children vs. adolescent).
Eligibility criteria
Studies were included in the systematic review if the following criteria were met: The study examined the efficacy or tolerability of at least one antidepressant (SSRI) among anxiety and depression in both children and adolescent samples. The sample included children (ages <12) and did not include adults (ages >19) populations. The study was originally published in English. The study used an original or secondary dataset. The study was conducted in the United States. The study was published in a peer reviewed journal between January 2011 and September 2022.
Exclusionary criteria
Articles were excluded if the sample did not include children (ages <12; n = 0), only included adolescents (ages 12–18), or included adults (ages >19).
Studies conducted outside the United States were excluded.
Studies conducted in the United States, but that also included other countries of origin, were excluded.
Meta-analyses, systematic reviews, protocols for future research, and case studies (n = 1) were excluded.
Data extraction
After screening all titles and abstracts and conducting a full-text review, a total of (n = 11) articles were identified for inclusion by two reviewers (Fig. 1). These 11 articles were reviewed, and information relevant to study goals was extracted by one reviewer and checked for accuracy by a second reviewer. The data extracted were compiled into two tables (Tables 2 and 3). The following information was extracted from each article: sample size, sample demographics (e.g., age, sex, race, ethnicity, geographic location), disorders under evaluation, antidepressant use, study design/method, and group differences. The current study did not require a quality review of the articles included or an assessment of risk of bias because the objective of this study was not related to the study findings. However, information concerning two quality indicators was extracted: effect sizes and whether the study reported a power analysis to help inform future research.
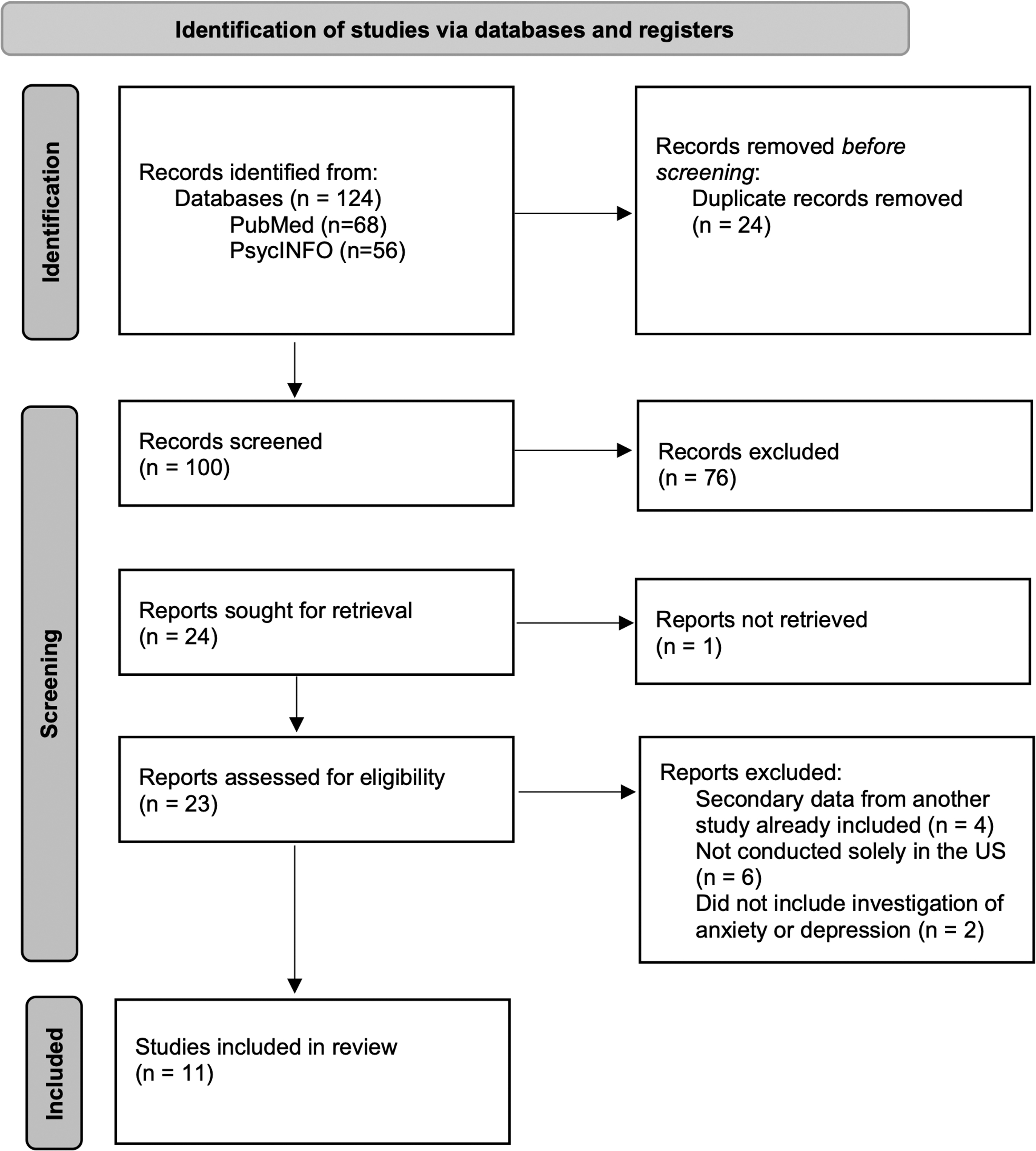
Flow diagram according to the PRISMA guidelines. This flow diagram has been modeled after: Page et al. (2021). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Results
Search results
A total of 124 articles were located using the search terms in PsycInfo and PubMed.
After duplicate articles were removed, the search resulted in (n = 100) unique articles. These articles underwent an abstract review, which yielded 24 articles that underwent a full text review. The full text review resulted in 11 articles that met inclusionary criteria and were included in the current systematic review.
Summary of included articles
The studies included in this review were published between the years of 2011 and 2020. Thirty-six percent of the articles included in this review did not report effect sizes for their findings, while 91% did not report statistical power and within-group differences among racial, ethnic, and gender groups. Of the 11 studies, the majority (73%) examined the use of antidepressants in relation to depression (e.g., MDD, severe mood dysregulation), and the remaining 27% examined antidepressants in relation to anxiety (e.g., GAD, social phobia, separation anxiety disorder, selective mutism). Fluoxetine was the most common antidepressant studied among children and adolescents. While 64% of studies examined fluoxetine alone, one study compared Fluoxetine to Sertraline, Paroxetine, Citalopram, Escitalopram, and Venlafaxine (SNRI). In addition, Citalopram (n = 1), Duloxetine (n = 1), and Sertraline (n = 1) were each examined individually.
Furthermore, the study designs and methodology varied across studies. Forty-five percent of studies utilized a randomized placebo-controlled design, 18% utilized a randomized, double-blind, placebo-controlled design, 18% used a retrospective cohort study design. Out of the remaining two studies, one was a long-term follow-up study examining outcomes, and the other was a relapse prevention clinical trial. The sample sizes ranged from 5 to 36,842 (mean = 3301). The total sample for all studies combined was 39,614. The majority (46%) of the studies had a sample between 100 and 500 individuals, 18% reported a sample >500, and 36% of the studies reported a sample size <100.
Summary of demographic findings: age
Participant age ranged from 5 to 18 years, with the average age ranging from 9 to 14 across studies. The majority (73%) of the studies reported an average age between 11 and 14. One study reported an average age of 9, one study reported an average age of 14, and another study did not report mean age. All studies included both children (ages <12) and adolescents (ages 12–18). Thirty-six percent of the studies did not report the distribution of the sample in relation to child and adolescent groups; however, out of those seven studies reporting the distribution, 71% reported having a primarily adolescent sample (i.e., over 50% of the sample was 12 years or older) and 43% reported having ∼80% of their sample to be ages 12 and older. Notably, the search did not yield any studies with child only samples.
Summary of demographic findings: gender
All the studies included in this review reported the distribution of binary male and female sex/gender, with the overall range being 32%–80% female. Eighty-two percent of the studies reported nearly equal numbers of males and females (ranging from 44% to 59% female). Notably, one study had a smaller sample of females (32%), and one study with a small sample had a majority female sample (N = 5, 80% female). None of the studies reported on any transgender, genderqueer, or gender-nonconforming demographics.
Summary of demographic findings: race and ethnicity
For the purpose of this review, studies reporting the distribution of at least three racial groups were considered to have fully reported racial demographics, while those reporting on only one to two races and having at least 10% of their sample unaccounted for were considered to have partially reported racial demographics. One study omitted all racial demographic information, while 64% partially reported racial demographics. Of those studies with only partial reporting, three studies reported White/Caucasian and Black/African American distribution (27%), two reported either the percentage of Black/African American (9%) or the percentage of White/Caucasian (9%), and one simply described the sample as majority white (9%). Only four studies (36%) fully reported on racial demographics. While all four studies reported on the White/Caucasian, Black/African/African American distribution, only a portion reported the following groups: Asian/East Asian (27%), Multiracial (27%), American Indian/Native American/Alaskan Native (18%), Other/Unknown (9%). Notably, one of the studies (9%) grouped Asian and American Indian together; therefore, there was no way to disaggregate these data and examine these groups separately.
All studies that reported racial demographics reported having a majority White/Caucasian sample (>50%), except for one study which only reported having 16% African American and did not account for the remaining 84% of the sample. The percentage of white participants ranged from 58% to 82%. Black/African American/African was the second most common racial category endorsed, which ranged from 6% to 24%. While 45% of studies had 7%–21% of their sample unaccounted for in terms of racial demographics, one study had 84% of their sample unaccounted for. Only 27% of studies accounted for the racial demographics of nearly their entire sample. Regarding ethnicity, while 64% of the studies reported what portion of their sample identified as Hispanic/Latinx, 36% of studies omitted ethnicity demographics altogether. Among the studies that reported ethnic distribution, Hispanic/Latinx accounted for 0.7%–30% of the sample.
Discussion
The purpose of the present review was to examine the demographic composition of childhood samples used in antidepressant efficacy and tolerability studies in the last decade. Specifically, this review evaluated studies investigating the use of antidepressants (e.g., SSRIs and SNRIs) for the treatment of depression and anxiety in children and adolescents. Although a quality review of the studies was not necessary for the purpose of this review, it is important to note the lack of reporting of effect sizes (i.e., 36% did not report an effect size) and power (i.e., 91% did not report calculating power). These omissions are concerning as these studies were investigating group differences related to medication usage, and the effect size is crucial in interpreting results and should be addressed by future studies.
Furthermore, the demographic composition of samples used in antidepressant efficacy and tolerability studies with children and adolescents revealed that although all studies reported having at least some percentage of their sample to be 11 years of age or younger, most studies nevertheless utilized a majority adolescent sample. This is a noteworthy finding because antidepressants are approved for use with younger children (i.e., as young as six) and are also often used off-label with young children (American Academy of Child and Adolescent Psychiatry, 2020; Garfield et al., 2015). Due to the high volume of antidepressants being prescribed to children (age < 12), it is imperative that antidepressant efficacy and tolerability studies include young children in their samples and compare findings across age groups.
Regarding gender and sex, all of the reviewed studies reported the distribution of their sample based on binary terms (i.e., male and female), and no studies reported on the inclusion of transgender, genderqueer, or gender-nonconforming participants. This omission is highly concerning, especially considering that as of 2017, 2% of high school students identified as transgender (Johns et al., 2019), 9% identified as lesbian, gay, or bisexual (LGB) (UCLA School of Law, 2020), and one in four LGBTQ youth identified as outside of the gender binary (The Trevor Project, 2019). Furthermore, relative to cisgender youth, transgender and gender-nonconforming youth are at a higher risk for anxiety, depression, and suicide, which underscores the importance of including this population in studies that investigate common treatments for these mental health difficulties (Reisner et al., 2015).
While most studies (91%) reported at least some portion of the race and ethnicity distribution of their sample, one study did not report any information regarding race or ethnicity. In addition, of the studies that reported race and ethnicity demographics, many only reported on limited racial groups (e.g., white or African American). The racial categorizations used in some of the articles were noteworthy for using seemingly arbitrary grouping categories such as “Asian and American Indian.” Furthermore, studies also demonstrated bias by operationalizing racial labels which do not appear to be representative of the groups included, such as one study using “African” when including Black/African American groups and most studies utilizing “Asian” without differentiating between Pacific Islander, East Asian, Asian American, or other notable within group differences. In addition, 6 (67%) out of the 9 articles which reported racial demographic information had a portion of their sample unaccounted for.
As evident by the results of this review, groups other than the dominant race (i.e., white) were often grouped together as “other” or omitted altogether. Most of the studies did not have samples that were representative of the U.S. population of children or of the populations that are significantly affected by the disorders treated by antidepressants. In addition, there was a lack of inclusion of immigrants, non-English speaking populations, and refugees in antidepressant efficacy studies, which is concerning given the high rates of distress reported by these populations. Given these exclusions, the findings from this study may not be generalizable to the general population of children and adolescents.
The present findings are indicative of a lack of diversity in studies examining the efficacy and tolerability of antidepressants in youths or at best are indicative of an oversight when gathering and reporting demographic data. The aforementioned disparities found in anxiety and depression presentation and prevalence across cultural groups dictate the need for inclusive samples that can benefit from the use of these medications. Moreover, to address the disparities in the prescription and utilization of antidepressants across cultural groups, evaluations of these medications must include diverse samples.
Although an explanation for the lack of diversity and/or reporting is outside the scope of this review, it is worth noting some of the possible explanations for why these studies may not have had representative and inclusive samples. Although young children are also prescribed antidepressants both on and off-label, their lack of inclusion in studies relative to that of adolescents may be related to the lack of FDA approval for the use of these medications with younger children. The lack of inclusion may also be related to the limited knowledge base surrounding the efficacy and tolerability of antidepressants in children and the limited understanding of developmental effects (Dwyer and Bloch, 2019). These limitations may prevent studies from being approved by the institutional review boards, and even if approved, parents may be hesitant to consent to a study using these medications.
Although speculative, people of color may display more hesitancy and concern regarding scientific and pharmacological studies compared to their white counterparts and may be related to historical discrimination and lack of equity seen in psychiatric and psychological studies in the United States (Xia et al., 2016). In addition, the well-documented disparities in the access and utilization of health care are also critically important to medication use in youth from racially and culturally diverse backgrounds, as this limits their access to research participation in antidepressant efficacy studies. Despite the researchers' intentions to utilize nonbiased sampling, their samples are representative of the populations who have the most access to care (i.e., white, middle to high socioeconomic class, English speaking) (Lesser et al., 2010). The lack of racial and ethnic diversity in study samples may also be related to the same cultural factors involved in the lack of utilization of antidepressants among these populations (e.g., parental perceptions, education level, cultural and religious beliefs, and referral bias).
Furthermore, it is important to consider the difference between the lack of representation in the studies included in this review and the lack or inappropriate reporting of the sample characteristics of these samples. While some studies may have successfully recruited a representative sample, we are unable to assess their sample due to the lack of reporting of demographic characteristics or due to the biased grouping of categorically different groups. Possible explanations for limited, committed, or biased reporting may be associated with the lack of consistent demographic measures used across studies. As researchers create their measures and develop the methods for their studies, they may inadvertently omit categories for racial, ethnic, gender, sexuality, and other dimensions of identity. Consequently, individuals who may choose to identify as “other” may not have had the ability to report their specific identity, or if they provided qualitative data, it may not have been quantified in a meaningful way.
Future directions
Future studies would benefit from addressing the current gap in the literature regarding antidepressant efficacy and tolerability across cultural groups. Studies must also strive to calculate and report statistical power and effect size to facilitate the interpretation and understanding of the magnitude of their findings. The current review demonstrates a lack of diversity regarding age, sex/gender, race, and ethnicity with respect to children and adolescents. A critical finding is that many of the studies did not report racial and ethnic demographics, and none of the studies reported the inclusion of nonbinary and transgender youth. Future studies should address cultural factors that are often related to underrepresented individuals' hesitancy to engage in and/or trust research. In addition, community-based participatory research must be conducted to properly represent these historically underrepresented and marginalized groups. Future research should also include more sensitive measures of gender, race, and ethnicity, to properly report the spectrum of diversity found in these samples, and between- and within-group differences based on ethnic, racial, and gender groups should also be explored.
At a minimum, in the United States, it is important to report age, gender, race, ethnicity, sexual orientation, disability status, immigration status, and socioeconomic status in commonly accepted terms (e.g., census categories). Furthermore, when reporting these characteristics, it is important to note if there was no representation from a certain demographic group, rather than omitting it altogether (e.g., documenting that 0% of the sample was Native American, rather than not listing this category). Future studies would benefit from resources such as the Publication Manual (seventh edition) of the American Psychological Association (2020), which provides guidelines for appropriate reporting of demographic information.
The American Psychological Association (2020) guidelines urge researchers to be specific, focus on relevant characteristics, and acknowledge relevant differences (American Psychological Association, 2020). For example, when reporting age, the exact ages or age ranges of participants should be provided, instead of broad categories such as “adolescents” or “under 18.” In addition, it is important to provide the mean and median of age groups. In terms of gender and sex, use descriptors such as “cisgender” or “assigned sex” to capture the diversity of the sample. When reporting race and ethnicity, being specific may mean identifying the specific nations or regions of the participants (e.g., Chinese American, Dominican) compared to more generalized origin (e.g., Asian American, Latinx).
Although the focus of this review is not on psychopathology, it is worth noting that the majority of the studies that met inclusionary criteria investigated the efficacy or tolerability of antidepressants in the context of a MDD diagnosis. The lack of diversity of presenting concerns is troublesome, as antidepressants are commonly used off-label to treat other psychiatric disorders such as anxiety, which is the second most common mental health disorder identified and treated in children (second only to attention-deficit/hyperactivity disorder) (Lebrun-Harris et al., 2022). Future studies should address this gap in the literature and explore antidepressant efficacy and tolerability for diverse presenting concerns.
Limitations
The current review provided relevant information regarding sample characteristics of childhood studies assessing the efficacy and tolerability of antidepressants; however, there are also important limitations to take into consideration. First, the review only extended to the last 10 years and excluded several studies conducted internationally (e.g., Australia, Canada, Brazil, Germany, Mexico, Spain), as well as studies that primarily assessed antidepressant use with disorders other than anxiety and depression (e.g., Autism, Obsessive Compulsive Disorder). The exclusionary criterion of this review limits its generalizability to international research or to research related to other mental health difficulties. Future reviews in this subject should conduct larger reviews assessing a wider range of related disorders, as well as larger, more diverse child and adolescent populations.
The current review used two different databases (PsycInfo and PubMed) and screened all peer-reviewed, published articles in both of those databases; however, it is probable that studies were unintentionally excluded because they were not present in the two databases used. Furthermore, since this review only included published articles, there is a possibility of publication bias, which was not addressed through statistical analysis. In addition, only the data found in full-text articles were assessed in this study. Therefore, future reviews should address publication bias by including nonpublished studies (e.g., dissertations), as well as contacting authors to gather additional demographic information that may have been attained during the original study but was not reported. Moreover, this systematic review was conducted by two reviewers; however, the reviewers did not work independently, and the reviewing process was not blind. In turn, the current review process may have impacted the reliability of the screening process and data extraction. Future studies could benefit from having multiple independent reviewers and a blind review process.
Conclusions
Despite the increased rate of antidepressants in children and adolescents, and the common practice of prescribing SSRIs/SNRIs off-label for the treatment of anxiety and depression, this review revealed a general lack of studies reporting on the efficacy and tolerability of these medications in children. Furthermore, this review revealed the lack of gender and race diversity represented in the literature regarding antidepressant use with children and adolescents. Future research is warranted to better understand and address the cultural disparities found in the utilization, efficacy, and tolerability of antidepressants in children and adolescents, and this research must include diverse samples that are representative of the populations using and needing these medications.
Clinical Significance
To effectively address the increasing rates of anxiety and depression among children and adolescents from diverse backgrounds, antidepressant efficacy and tolerability studies must include representative samples in regard to age, gender, sexuality, race, ethnicity, and other pertinent demographic factors.
Footnotes
Authors' Contributions
E.R.: Conceptualization (lead), Methodology (lead), Formal analysis (lead), Data curation (equal), Writing—Original draft preparation (equal), Visualization (equal). A.B.: Formal analysis (supporting), Data curation (equal), Writing—Original draft preparation (equal), Visualization (equal). L.W.: Conceptualization (supporting), Visualization (equal), Writing—Review and Editing (lead), Supervision (lead).
Disclosures
No competing financial interests exist.