
Abstract
Objective:
To conduct a pilot study to examine topiramate for the treatment of weight gain associated with olanzapine in manic adolescents with bipolar disorder.
Methods:
We conducted a 12-week double-blind randomized placebo-controlled pilot study of topiramate (300–400 mg/day) versus placebo in manic youth (ages 10–18 years) with bipolar disorder who were treated with olanzapine (10–20 mg/day). The primary outcome measure was gender- and weight-normed change in body mass index (BMI z-score).
Results:
Thirty manic adolescents were treated with olanzapine and were randomized to either topiramate (n = 16) or placebo (n = 14). There was a significantly greater increase in BMI z-scores in the placebo group (0.28 standard deviations [SDs]) compared with the topiramate group (0.10 SDs) when analyzed by longitudinal regression (p = 0.049). The placebo group had greater increases in raw BMI and weight (2.25 kg/m2 and 6.9 kg, respectively) compared with the topiramate (0.99 kg/m2 and 2.9 kg) group (p = 0.011 for BMI, p = 0.016 for weight). The most common adverse events in the topiramate group were headache (n = 7, 44%), gastrointestinal upset (n = 3, 19%), and muscle stiffness (n = 3, 19%).
Conclusions:
Topiramate may minimize the weight gain associated with olanzapine treatment in adolescents with bipolar disorder. Moreover, topiramate in combination with olanzapine was well tolerated. Larger studies that are adequately powered are necessary to determine the efficacy of topiramate for second-generation antipsychotic-related weight gain.
Trial Registration:
Introduction
Second-generation antipsychotics (SGAs) are effective for the treatment of manic episodes in youth with bipolar disorder (DelBello et al. 2006a, 2006b; Correll et al. 2010). Although treatment with SGAs often leads to considerable symptom improvement, it is very commonly associated with substantial weight gain in children and adolescents (Kowatch and DelBello 2005; Correll and Carlson 2006; Correll 2007; Fraguas et al. 2008; Correll et al. 2009; Moreno et al. 2010; De Hert et al. 2011; Eapen and John 2011).
Results of open-label and double-blind placebo-controlled studies suggest that olanzapine is effective for the treatment of manic adolescents with bipolar disorder (Frazier et al. 2001; Tohen et al. 2005; DelBello et al. 2006b); however, among SGAs, olanzapine appears to be associated with the greatest weight gain (Tohen et al. 2005; Correll and Carlson 2006; Fleischhaker et al. 2007, 2008; Correll et al. 2009). Prior open-label and double-blind studies suggest that adolescents treated with olanzapine for 3–4 weeks exhibit significant weight gain that ranges from 3 to 6 kg (Frazier et al. 2001; Tohen et al. 2005; DelBello et al. 2006a).
Adjunctive interventions aimed at reducing olanzapine-associated weight gain in adolescents would make olanzapine a more acceptable treatment option for this population (Correll and Carlson 2006). In addition, minimizing olanzapine-associated weight gain may also decrease the risk of metabolic syndrome, type 2 diabetes, and cardiovascular morbidity (Correll et al. 2009; Eapen and John 2011), as well as, further social withdrawal and stigmatization (Martinez-Ortega et al. 2013).
Topiramate is an antiepileptic medication, reduces weight in adolescents (Fox et al. 2015), and is effective for treating binge eating disorder in adults in double-blind studies (McElroy et al. 2007). Moreover, in contrast to studies of adults (Kushner et al. 2006), topiramate may be effective, and well tolerated, for the treatment of mania in youth with bipolar disorder (DelBello et al. 2002, 2005; Barzman et al. 2004).
Specifically, although in a double-blind placebo-controlled study of 56 manic/mixed youth (6–17 years old) comparing topiramate (n = 29) with placebo (n = 27) the reduction in mean Young Mania Rating Scale (YMRS) score from baseline to final visit using the Last Observation Carried Forward was not significantly different between the topiramate group (−9.7 ± 9.65) and the placebo group (−4.7 ± 9.79, p = 0.152) and the mean total YMRS score reduction with topiramate at day 28 was not statistically significant compared with placebo (−11.7 ± 8.90 vs. −5.6 ± 10.38, p = 0.064), there was a numerically greater reduction in manic symptoms in the topiramate group compared with the placebo group (DelBello et al. 2005).
Findings from several open-label (Kim et al. 2006) and double-blind (Ko et al. 2005; Nickel et al. 2005; Wang et al. 2020) studies as well as meta-analyses (Maayan et al. 2010; Fiedorowicz et al. 2012; Mohmood et al. 2013) suggest that topiramate is effective for reducing and preventing weight gain associated with SGAs in adults (Ko et al. 2005; Nickel et al. 2005; Kim et al. 2006; Maayan et al. 2010; Fiedorowicz et al. 2012; Mohmood et al. 2013; Wang et al. 2020). However, there are few studies examining the impact of topiramate in youth treated with SGAs (Rezaei et al. 2010; Shapiro et al. 2016; Jumaili et al. 2022) and even fewer studies in youth with bipolar disorder treated with SGAs (Tramontina et al. 2007; Wozniak et al. 2009; Arman and Haghshenas 2022).
Specifically, there are two open-label studies (Tramontina et al. 2007; Wozniak et al. 2009), a single-blind randomized study (Mahmoudi-Gharaei et al. 2012) and a double-blind placebo-controlled study (Arman and Haghshenas 2022) examining topiramate for SGA-related weight gain in youth with bipolar disorder. Specifically, Wozniak et al. conducted a study of two concurrent open-label 8-week trials of olanzapine monotherapy (n = 17) or topiramate augmentation of olanzapine (n = 23) in youth with bipolar disorder. Patients assigned to the olanzapine and topiramate trial experienced statistically significantly less weight gain than those patients in the olanzapine monotherapy trial (2.5 vs. 5.1 kg) (Wozniak et al. 2009).
Although this study provides preliminary data to support the use of topiramate for olanzapine-associated weight gain, this was an open-label study and the average dose of topiramate was low (average daily dose at endpoint was 70.5 ± 30.5 mg/day). More recently, a double-blind placebo-controlled study examined topiramate as an adjunctive treatment to aripiprazole for the prevention of weight gain and metabolic alterations in youth with bipolar disorder (Arman and Haghshenas 2022). Although there were no significant group differences in anthropometric parameters overtime, there was a significant increase in anthropomorphic measures in the placebo group, but not in the topiramate group.
Limitations of this study include the small sample size, not analyzing data from participants who dropped out of the study, and using a very low dose of topiramate (average dose of 53.5 ± 27.6 mg/day). With these considerations in mind, we conducted a 12-week double-blind placebo-controlled pilot study of the efficacy and tolerability of topiramate in combination with olanzapine for the prevention of weight gain in manic youth with bipolar disorder. We hypothesized that topiramate would be more effective than placebo as adjunctive treatment for the prevention of weight gain and changes in other metabolic measures. Moreover, we hypothesized that topiramate would be well tolerated.
Methods
The study was approved by the University of Cincinnati and the Cincinnati Children's Hospital Medical Center Institutional Review Boards. All study participants provided written assent and had a legal guardian who provided written informed consent before any study-related procedures were performed. Patients were recruited for study participation from 2007 to 2010.
Participants
Youth (ages 10–18 years) with a manic or mixed episode of bipolar I disorder were recruited from the inpatient units and outpatient clinics at the University of Cincinnati and Cincinnati Children's Hospital Medical Center. All potential participants were evaluated using the Washington University in St. Louis Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U KSADS), which was administered by trained interviewers with established symptom and diagnostic reliability (κ > 0.9) and reviewed by a child and adolescent psychiatrist (M.P.D., L.R.P.D.) (Geller et al. 2001). Youth and their primary caregivers were interviewed separately and their responses were combined to ascertain diagnoses. Demographic information was obtained by interviewing the patients and their primary caregivers.
Participants were included in the study if they had a diagnosis of bipolar I disorder, current episode manic or mixed, according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revised (DSM-IV-TR) criteria and as determined by WASH-U KSADS interview. In addition, to be included in this study, patients were required to have a baseline YMRS score of at least 16, and a body mass index (BMI) ≥75th percentile (Young et al. 1978; Fristad et al. 1992).
Patients were excluded by having a substance use disorder (other than nicotine or caffeine) within the previous 3 months; an unstable medical or neurological illness; a history of intolerance or hypersensitivity to topiramate or olanzapine; history of olanzapine or topiramate nonresponse; treatment with an injectable depot neuroleptic within less than one dosing interval between depot neuroleptic injections and baseline; or treatment with concurrent mood stabilizers, anticonvulsants, benzodiazepines, psychostimulants, or antidepressants.
Patients judged to be at risk for suicide (defined as having active suicidal ideation, intent or plan, or a serious suicide attempt within 30 days or a baseline Children's Depression Rating Scale (CDRS) suicide item >3) were excluded from study participation (Poznanski et al. 1979). Patients were outpatients or inpatients, and discharge from the hospital to outpatient treatment was permitted during the study at the discretion of the inpatient attending psychiatrists.
Study medication
After it was determined that all study criteria were met, participants were randomized to topiramate or placebo. Randomization was stratified by gender and the presence of psychotic features. All participants and their caregivers, as well as study staff who performed efficacy and tolerability ratings, were blinded to treatment assignment. All participants received olanzapine starting at 5–10 mg, with flexible titration based on antimanic efficacy to a maximum dose of 20 mg by day 21. In addition, participants also received either topiramate or matched placebo. Topiramate (or matched placebo) was initiated at 25 mg bid and titrated over 4 weeks to a dose of 100 mg bid. Further titration to a maximum dose of 200 mg bid by week 6 was permitted as tolerated.
Efficacy assessments
The primary efficacy measure, defined a priori, was the change over the 12-week course of the study in gender- and age-normalized BMI in the modified intent-to-treat sample (all subjects who were randomized took at least one dose of study medication, and were assessed at least once after taking their first dose of study medication). Secondary outcome measures included change in vitals (weight, heart rate, blood pressure, and BMI) as well as change in fasting triglycerides, cholesterol, high-density lipoprotein, low-density lipoprotein, glucose, and insulin levels from baseline to endpoint. Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) was calculated as follows: fasting insulin (microU/L) × fasting glucose (nmol/L)/22.5.
Symptom rating scales
Symptom rating scales included change over the 12-week course of the study in the YMRS, CDRS-Revised (CDRS-R), and the Clinical Global Impressions–Bipolar Disorder Version Severity for overall illness (CGI-BP-S overall) (Poznanski et al. 1979; National Institute of Mental Health 1985; Fristad et al. 1992).
Tolerability assessments
Tolerability evaluations included assessments of adverse events (AEs). AEs were recorded by asking patients and primary caregivers open-ended questions about potential side effects. Extrapyramidal symptoms (EPSs) were assessed at baseline and endpoint using the Simpson–Angus, Barnes Akathisia, and Abnormal Involuntary Movement scales (Simpson and Angus 1970; AIMS 1976; Barnes 1989). In addition, the Behavior Rating Inventory Executive Function (BRIEF) measure was utilized to measure executive functioning at baseline and endpoint (Gioia et al. 2000).
Statistical analyses
Statistical analyses were performed using Statistical Analysis System (SAS), version 9.4 (SAS Institute, Cary, NC). Before study initiation, we estimated that a sample of 15 patients per study group would be able to detect large effect sizes (d = 1.06 with power = 0.8 at α = 0.05, two-tailed) (Cohen 1988). However, we conducted this study as a pilot feasibility study to determine recruitment and study completion rates during a fixed time period and to provide a preliminary estimate of effect size.
Longitudinal mixed-effects regression models, estimated with PROC MIXED, were conducted to evaluate changes over time in BMI z-score, BMI, weight, and symptom ratings. Our prior experience with similar studies suggested that profiles of change over time may exhibit some curvature, with more rapid change in the early weeks of the study, so we compared models (using the sample-size corrected version of Akaike's Information Criterion [AICc]) using the square root of days since randomization as the time scale to models that were linear in days since randomization.
AICc was also used to select a preferred covariance structure for the random effects (i.e., whether to include subject-specific random intercepts and/or slopes, and if both, whether they should be allowed to be correlated vs. independent), and residual correlation pattern (compound symmetric vs. spatial autoregressive).
T-tests were used to examine change from baseline to endpoint in laboratory measures. Rates of AEs were compared between groups using Fisher's exact test. All statistical tests were two-tailed, α = 0.05.
Results
Patient characteristics
Thirty-one patients were initially consented and were eligible for study participation, however, a patient withdrew consent before randomization (Fig. 1). The remaining 30 eligible manic youth were randomized to treatment with olanzapine and placebo (n = 14) or olanzapine and topiramate (n = 16). There were no statistically significant differences in demographic or clinical characteristics between the treatment groups at baseline (Table 1). Age at onset of bipolar disorder was defined as the age at which a DSM-IV-TR manic episode first occurred and was determined using the WASH-U KSADS.
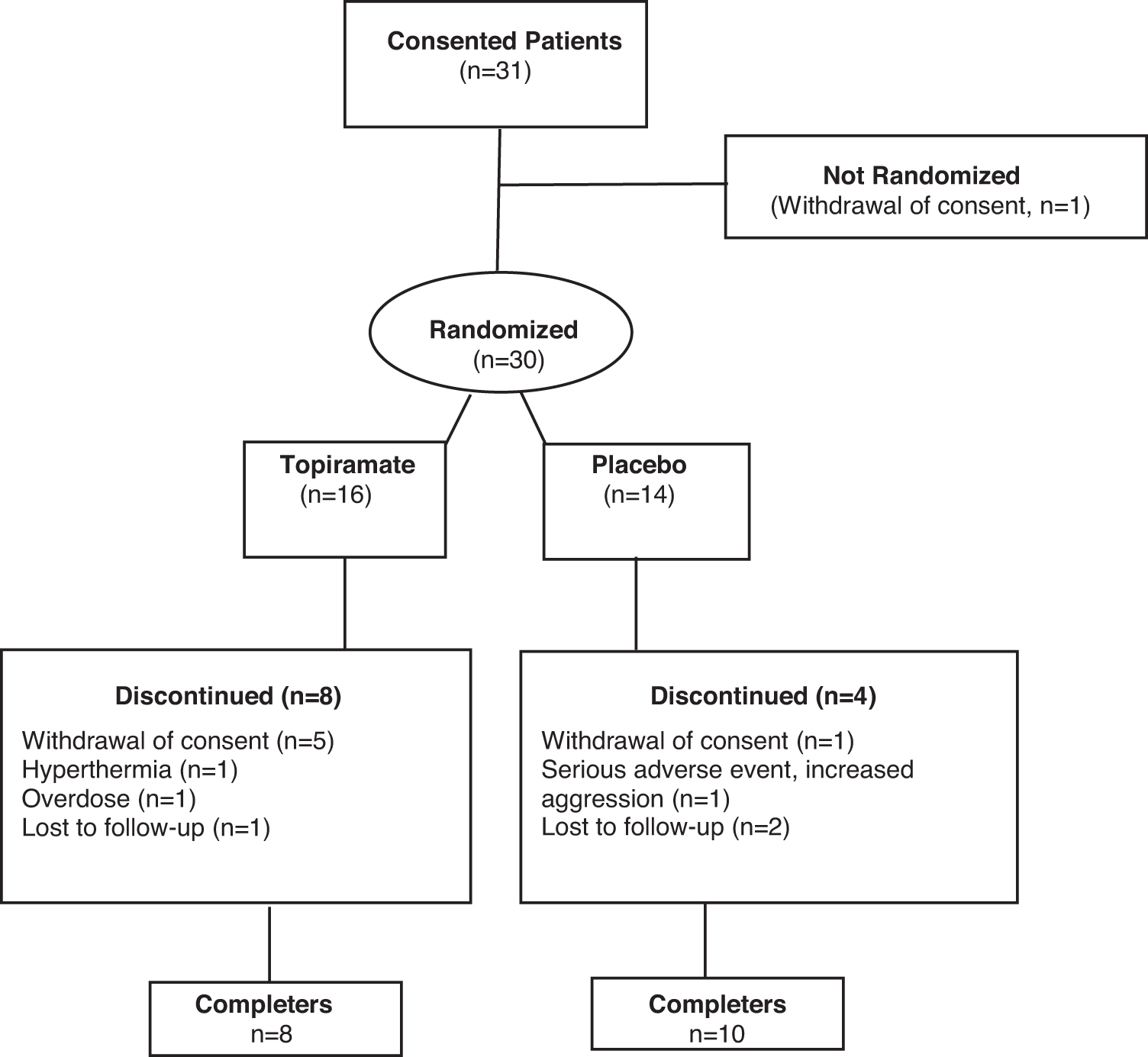
Flow chart of study participants.
Demographic and Clinical Variables of Bipolar Adolescents (n = 30) with Mixed or Manic Episode Bipolar Disorder by Treatment Group
ADHD, attention-deficit/hyperactivity disorder; OLZ, olanzapine; SD, standard deviation; TPM, topiramate.
Eight patients in the placebo group and seven patients in the topiramate group were inpatients at the time they were randomized. There were no statistically significant differences in baseline or change in rating scale scores between patients enrolled as inpatients compared with those enrolled as outpatients (smallest p ≥ 0.40).
Patient disposition
Within the topiramate group, the mean (standard deviation [SD]) dose at endpoint for olanzapine was 11.4 (3.3) mg/day and topiramate dose was 146.7 (67.4) mg twice per day. Within the placebo group, the mean (SD) dose at endpoint for olanzapine was 12.1 (3.1) mg/day, and placebo was 175.0 (42.7) mg twice per day.
Although there were fewer patients (n = 4, 29%) in placebo group than in the topiramate group (n = 8, 50%) who discontinued study participation before day 84, this difference was not statistically significant (Fisher's exact test, p = 0.28). In the topiramate group, reasons for premature discontinuation included withdrawal of consent (n = 5 at baseline, days 21, 35, 56, and 70), lost to follow-up (n = 1 on day 14), and hyperthermia (n = 1 on day 70, and suicide attempt (n = 1 on day 56). Reasons for premature discontinuation in the placebo group included withdrawal of consent (n = 1 on day 23), lost to follow-up (n = 2 on days 21 and 28), and increased aggression (n = 1 on day 56).
Primary efficacy measures
Model comparison using AICc led us to adopt a regression model that was linear in the square root of days since randomization, with subject-specific random intercepts but not subject-specific slopes, and with a spatial-autoregressive structure for the residual covariance matrix. The group-by-time interaction term from this model was statistically significant (p = 0.049), suggesting a modestly greater rate of gain in normalized BMI in the placebo group. BMI z-scores in the placebo group were estimated to increase by 0.28 SDs, compared with an increase of 0.10 SD in the topiramate group.
Mixed-model regression estimates of raw (not adjusted by gender and age for normal growth) gains in BMI and weight were also greater in the placebo (2.25 kg/m2 and 6.9 kg) than in the topiramate (0.99 kg/m2 and 2.9 kg) group (p = 0.011 for BMI, p = 0.016 for weight). The effect sizes for change in weight and BMI were 0.83 and 0.56, respectively.
Figure 2 shows weekly means and 95% confidence intervals (CIs) for BMI z-score in both groups (these were estimated from a standard repeated-measures analysis of variance model for categorical time points; the a priori analysis model used parametric regression functions of the exact days of assessment). Also shown are the means and CIs for the BMI z-score for each subject's last available observation (“endpoint”). Simple change scores from baseline to this value were analyzed as a secondary analysis for BMI z-score and other outcomes. In general, the observed endpoint means tended to be very close to the 12-week means estimated by the selected regression model, though with wider CIs (as the model-based estimates use all available observations, yielding greater precision).

Mean and 95% CI BMI z-score in youth with bipolar disorder treated with olanzapine and topiramate versus olanzapine and placebo, estimated from a standard repeated-measures ANOVA model for categorical time points. Also shown are the means and CIs for the BMI z-score for each subject's last available observation (“endpoint”). ANOVA, analysis of variance; BMI, body mass index; CI, confidence interval.
Secondary efficacy measures
Metabolic parameters
There was no statistically significant between-group or within-group differences in change from baseline to endpoint in the metabolic laboratory measures (Table 2). There was no statistically significant between-group difference in change from baseline to endpoint in HOMA-IR, although HOMA-IR decreased in the topiramate group (mean = −0.01, SD = 2.02) and increased in the placebo group (mean = 1.24, SD = 2.28) (mean difference of change = −1.25 [95% CI: −3.04 to 0.53], t = −1.45, p = 0.16).
Change in Metabolic Variables at Baseline and Endpoint by Treatment Group
Baseline to endpoint change.
CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein; OLZ, olanzapine; TPM, topiramate.
Symptom rating scales
There was no statistically significant difference between treatment groups in change in YMRS scores (difference of regression slopes = −1.02 [95% CI: −6.52 to 4.47], p = 0.71). There were statistically significant within-group decreases in YMRS scores from baseline to endpoint within each treatment group; the topiramate group decreased from mean (SD) of 25.6 (5.4) to 12.1 (9.7), p < 0.0001, whereas the placebo group mean decreased from 27.7 (4.4) to 10.0 (5.7), p < 0.0001.
There was no statistically significant difference between treatment groups in change in CDRS-R scores (difference of regression slopes = −1.07 [95% CI: −10.03 to 7.90], p = 0.82). There were statistically significant within-group decreases in CDRS-R scores from baseline to endpoint in each treatment group; the topiramate group decreased from mean (SD) of 42.4 (7.0) to 30.3 (13.0), p = 0.0013, whereas the placebo group decreased from mean (SD) of 42.9 (5.9) to 24.5 (9.1), p < 0.0001.
There was no statistically significant difference between treatment groups in change in overall CGI-BP-S scores (difference of regression slopes = −0.13 [95% CI: −0.87 to 0.61], p = 0.73). There were statistically significant within-group decreases in each treatment group; the topiramate group decreased from mean (SD) of 4.9 (0.3) to 3.0 (1.5), p < 0.0001, whereas the placebo group decreased from mean (SD) of 5.1 (0.5) to 2.7 (1.1), p < 0.0001.
Tolerability
Common (>10% in either treatment group) treatment-emergent AEs are listed in Table 3. There were three serious AEs during this study: increased aggression (n = 1, placebo), malignant hyperthermia (n = 1, topiramate) (Strawn et al. 2008), and a suicide attempt (n = 1, topiramate). There were no statistically significant between-group differences in change from baseline to endpoint in heart rate, blood pressure, serum laboratory values, EPS ratings, or BRIEF subscale scores.
Common Treatment-Emergent (>10% in Either Treatment Group) Adverse Events
Note: Values are indicated as n (%).
Discussion
To our knowledge, this is the first double-blind placebo-controlled study examining the effects of topiramate on olanzapine-related weight gain in youth with bipolar disorder. Although both treatment groups exhibited an increase in BMI z-scores, BMI, and weight, topiramate as adjunctive treatment to olanzapine resulted in less of an increase in BMI z-score, BMI, and weight than olanzapine alone. Our pilot findings are consistent with several prior studies that report topiramate may be effective for decreasing SGA-related weight gain. In addition, although the mean dose of topiramate used in this study was higher than prior studies, we found that topiramate in combination with olanzapine was well tolerated.
It is important to note, however, that a patient who was treated with topiramate and olanzapine experienced severe hyperthermia. There have been several case reports of hyperthermia associated with topiramate (Strawn et al. 2008), and patients who are treated with topiramate should limit their exposure to extended periods of high temperatures. In general, prior studies suggest topiramate is well tolerated. Renal calculi have been reported in 1.5% of patients taking topiramate. Reduced appetite, slow and dulled thinking, as well as decreased cognition are also commonly reported side effects. Moreover, cognitive slowing may be related to the rate of dose titration (Jones 1998).
The exact mechanism for the effect of topiramate on mitigating SGA-related weight gain remains unknown. However, it is possible that topiramate exerts its effects by enhancing impulse control and reducing craving. Indeed, topiramate has been effective for reducing alcohol and drug craving (Zullino et al. 2002; Johnson et al. 2003; Kampman et al. 2004) and symptoms of binge eating disorders (McElroy et al. 2007). Topiramate may have similar effects on craving of food, thus, leading to decreased appetite. It has been hypothesized that this effect may be related to increased efficacy of gamma-aminobutyric acid activation in leptin-responsive neurons that ultimately lowers appetite (Stanley 2012).
There were no treatment group differences in metabolic parameters. However, HOMA-IR increased in the olanzapine group, but not in the topiramate group, suggesting that topiramate may mitigate the increase in insulin resistance observed with olanzapine. Studies of longer duration are necessary to further examine the metabolic impact of topiramate in youth treated with SGAs.
Our pilot study results indicate topiramate may be effective for reducing the weight gain associated with olanzapine treatment in youth with bipolar mania. Targeting SGA-induced weight gain may lead to better medication adherence, and ultimately lower rates of relapse, and better outcome. Moreover, topiramate was well tolerated and did not interfere with the effectiveness of olanzapine in reducing manic symptoms associated with bipolar disorder in adolescents.
Both treatment groups exhibited significant improvement in manic and depressive symptoms as well as overall functioning. Prior studies suggest that topiramate may be effective for treating mania in youth (Barzman et al. 2004; DelBello et al. 2005). Moreover, prior studies suggest that topiramate added to aripiprazole reduced manic symptom in youth with bipolar disorder compared with aripiprazole alone. In contrast, consistent with other studies of olanzapine and topiramate (Wozniak et al. 2009), we did not find greater reduction in manic symptoms when topiramate was added to olanzapine in manic youth. Although direct comparison studies of SGAs are needed, perhaps olanzapine monotherapy is more effective for mania than aripiprazole monotherapy.
Conclusions
There are several limitations of this study that should be considered when interpreting our results. First, the sample size in this pilot study only allowed for power to detect large between-group effect sizes. The small sample size at study endpoint further limited our ability to detect group differences. Second, although half our patients were recruited from inpatient psychiatric units, few of our patients had psychotic symptoms and patients with co-occurring substance use disorders were excluded. Therefore, our findings may not be generalizable to patients with more severe illness. Finally, our study used topiramate in conjunction with olanzapine. Whether topiramate is effective and well tolerated in combination with other SGAs remains unknown.
Despite these limitations, our findings support the use of topiramate to minimize olanzapine-related weight gain in manic youth with bipolar disorder. However, a larger well-powered study to determine the efficacy of topiramate for the prevention and treatment of SGA-related weight gain is needed.
Footnotes
Authors' Contributions
M.P.D. contributed to conceptualization (lead), methodology (lead), writing (colead), and analysis. K.M.B. was involved in methodology (supporting) and writing (colead). T.B. carried out methodology (supporting), analysis (supporting), review, and editing. L.R.P.D. was in charge of methodology (colead), analysis (supporting), review, and editing. J.S. took charge of methodology (equal), reviewing and editing (equal), and conceptualization (equal). C.M.A. carried out methodology (equal), reviewing, and editing (equal). J.W. was in charge of methodology (equal), writing (equal), reviewing and editing (equal), and analysis (lead).
Disclosures
In addition to the financial support provided by Eli Lilly to conduct this study, the authors have the following financial disclosures: Dr. DelBello has received research support from the National Institute of Health, the Patient-Centered Outcomes Research Institute (PCORI), AbbVie, Alkermes, Eli Lilly, Janssen, Johnson and Johnson, Lundbeck, Myriad, Novartis, Otsuka, Pfizer, Sage, Shire, Sunovion, Supernus, and Vanda, and has provided consultation or advisory board services for Alkermes, Allergan, Assurex, CMEology, Janssen, Johnson and Johnson, Lundbeck, Myriad, Neuronetics, Otsuka, Pfizer, and Sage.
Dr. Strawn has received research support from the Yung Family Foundation, the National Institutes of Health (NIMH/NIEHS), the National Center for Advancing Translational Sciences, the Patient-Centered Outcomes Research Institute (PCORI), and AbbVie. He has received material support from Myriad Health and royalties from three texts (Springer).
Dr. Strawn serves as an author for UpToDate and an associate editor for Current Psychiatry and has provided consultation to the FDA, Cereval, and IntraCellular Therapeutics. Dr. Patino has received research support from Eli Lilly, Pfizer, Otsuka, Novartis, Lundbeck, Sunovion, AbbVie, Martek, and Shire. Dr. Adler has received research support from Janssen, Sage, and SyneuRx, and serves on the speaker's bureau for Otsuka and Janssen. Dr. Welge, Dr. Bruns, and Mr. Bloom have no relevant financial relationships to disclose.