
Abstract
Background:
Treatment of obsessive-compulsive disorder (OCD) in children and adolescents frequently involves cognitive behavioral therapy (CBT), selective serotonin reuptake inhibitors (SSRIs), or their combination. However, how adding CBT to SSRIs affects the trajectory and magnitude of improvement has not been evaluated meta-analytically.
Methods:
We performed a meta-analysis using weekly data from prospective randomized parallel group trials of CBT and SSRIs in pediatric patients with OCD. Response was modeled for the change in the Child Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) using a Bayesian hierarchical model over 12 weeks.
Results:
Fourteen studies included pharmacotherapy arms, 4 studies included combined pharmacotherapy and psychotherapy, and 10 studies included a placebo or control arm. The studies included 1146 patients (mean age 12.7 ± 1.3 years, mean 42.1% female). In the logarithmic model of response, statistically significant differences in treatment effects for CBT+SSRI and SSRI monotherapy were observed compared with placebo (SSRI β = −3.59, credible interval [95% CrI]: −4.13 to −3.02, p < 0.001; SSRI+CBT β = −4.07, 95% CrI: −5.05 to −3.04, p < 0.001). Adding CBT to an SSRI produced numerically (but not statistically significantly) greater improvement over 12 weeks. Greater improvement was observed in studies with more boys (p < 0.001), younger patients (p < 0.001), and in studies with greater baseline symptom severity (p < 0.001).
Conclusions:
In children and adolescents with OCD, compared with placebo, both SSRIs and SSRI+CBT produced early and sustained improvement over 12 weeks, although the improvement was also related to sample characteristics. Longer term studies are needed to determine when the additive benefit of CBT emerges relative to SSRI monotherapy.
Introduction
Treatment of obsessive-compulsive disorder (OCD) in children and adolescents generally involves selective serotonin reuptake inhibitors (SSRIs) (Geller et al., 2003; Geller et al., 2001; Keller et al., 2001; Pediatric OCD Treatment Study [POTS] Team, 2004), cognitive behavioral therapy (CBT) (POTS Team, 2004), or a combination of the two (Franklin et al., 2011; POTS, 2004; Storch et al., 2013). Multiple SSRIs, including sertraline (POTS, 2004), fluvoxamine (Riddle et al., 2001), fluoxetine (Geller et al., 2001), and sertraline (POTS Team, 2004; Storch et al., 2013) have demonstrated efficacy in prospective randomized controlled trials.
Similarly, CBT has generally been superior to waitlist control conditions in children and adolescents, and both SSRIs and CBT produce similar improvements in OCD (Uhre et al., 2020). However, treatment response varies substantially in children and adolescents with OCD regardless of whether they are treated with SSRIs, other medication classes (e.g., tricyclic antidepressants) (Varigonda et al., 2016), or the combination of CBT+SSRIs.
In the POTS, a randomized controlled trial of youth aged 7–17 years (N = 112) with OCD that randomized patients to CBT, sertraline, CBT+sertraline, or pill placebo (POTS Team, 2004), youth with less severe OCD and less functional impairment as well as those with more insight, fewer comorbid externalizing symptoms, and less family accommodation had greater improvement regardless of whether treatment was an SSRI, CBT, or the combination (Garcia et al., 2010).
In addition, youth with OCD with a family history of OCD had a sixfold decrease in the efficacy of CBT monotherapy compared with the improvement seen in youth without a family history of OCD, potentially related to more family support being needed for exposure-related components of CBT compared with pharmacotherapy (Garcia et al., 2010). The heterogeneity of response in pediatric OCD has led to piecemeal recommendations regarding treatment, including guidance to begin treatment with CBT or CBT+medication or, in the case of those with a family history of OCD, offering CBT with medication as opposed to monotherapy (Garcia et al., 2010).
However, other data from the Nordic Long-term OCD Treatment Study revealed that improvement is more related to clinical and family characteristics (Torp et al., 2015) rather than to pharmacotherapy or pharmacotherapy+CBT (Jensen et al., 2020). Systematic reviews of response to CBT in pediatric patients with OCD suggest that response is related to a family history of OCD and tics (Turner et al., 2018). Importantly, substantial differences in the design of individual trials and the patient populations involved in these trials drive variation in response. These factors complicate our understanding of the trajectory of response to CBT+SSRI compared with SSRI monotherapy.
Only one meta-analysis has examined the response trajectory in pediatric OCD (Varigonda et al., 2016). In this meta-analysis of nine trials (801 children and adolescents), the greatest benefit of SSRI treatment emerged early, and the response was logarithmic (Varigonda et al., 2016). In addition, the tricyclic antidepressant clomipramine produced greater benefits than SSRIs, whereas SSRI dose was not associated with response. However, this meta-analysis did not examine the combined effect of CBT with pharmacotherapy, nor was it able to compare the response to SSRI+CBT versus SSRI monotherapy.
Understanding differences in the trajectory of improvement across treatments (or their combination) can now be accomplished with Bayesian hierarchical models (BHMs) (Stimpfl et al., 2021; Strawn et al., 2022). BHMs integrate multilevel information (e.g., individual patient, treatment, and comorbidity) to estimate the change in symptoms or probability of improvement at each hierarchy level, with submodels within the hierarchy combined with the observed data to account for uncertainty (McGlothlin and Viele, 2018).
BHMs allow observed variability to be separated to identify random differences versus true differences in treatment outcomes (McGlothlin and Viele, 2018). For example, applying a BHM to studies of OCD that use different SSRIs with or without CBT allows us to examine the influence of the disorder (e.g., treatment combination) and patient characteristics (e.g., baseline severity) on response while controlling for the influence of other factors. Thus, BHMs allow us to determine treatment effects relative to the information from all available studies (McGlothlin and Viele, 2018).
With these considerations in mind, we examined the magnitude and trajectory of response to SSRI or SSRI+CBT using BHMs in prospective treatment studies of children and adolescents with OCD. We hypothesized that SSRI+CBT would produce greater improvement in symptoms (and response) compared with SSRI monotherapy and that the additional benefit of CBT would emerge later than the improvement associated with SSRI treatment, given general response patterns in meta-analyses of children and adolescents with depressive and anxiety disorders (Strawn et al., 2022).
Methods
Literature search
We conducted a literature search with the PubMed database from inception to October 13, 2022, using the following terms: (“Obsessive-Compulsive Disorder”[Mesh] Disorder OR Obsessive Compulsive Disorder OR Obsessive-Compulsive Disorders OR Obsessive-Compulsive Neuroses AND (randomized controlled trial[Publication Type] OR (randomized[Title/Abstract] AND controlled[Title/Abstract] AND trial[Title/Abstract])) AND (pediatr* OR youth* OR adolescen* OR child*). The results of the search were then manually limited to randomized trials.
The references of all eligible trials were searched for additional clinical trials. In addition, we searched the annual meeting abstracts from the American Academy of Child and Adolescent Psychiatry, The American College of Neuropsychopharmacology, and the Anxiety & Depression Association of America from 2021 to 2023 for additional trials.
Inclusion criteria
Studies were included if they were prospective, randomized, and parallel-group trials that evaluated the efficacy of SSRI or SSRI+CBT (either group or individual) in the treatment of OCD and used the Children's Yale-Brown Obsessive-Compulsive Scale (CY-BOCS), a validated rating scale to measure the severity and frequency of obsessive-compulsive symptoms (Goodman et al., 1989; Storch et al., 2006).
Clinical trials were excluded if they met any of the following criteria: included adults (age >18 years), utilized a cross-over design, did not study an SSRI or an SSRI+CBT combination, were not randomized, included a Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV; American Psychiatric Association, 1994) or DSM-5 (American Psychiatric Association, 2013) disorder that confounded the assessment of obsessive-compulsive symptoms or treatment response (i.e., autism spectrum disorders, depressive disorders, and attention-deficit/hyperactivity disorder) or included <5 patients per treatment group.
Data extraction
The literature search and data extraction were conducted independently by two investigators (J.M.H. and E.M.M.) and reviewed independently by a physician investigator (J.R.S.) (Fig. 1). Study data and characteristics (e.g., year of study publication, patient sample size, age, percentage female, OCD severity before treatment, OCD severity after treatment, medication or psychotherapy employed, treatment duration, and number of sites) were extracted from primary articles, Supplementary Data, and/or review articles into a database (Microsoft Excel).
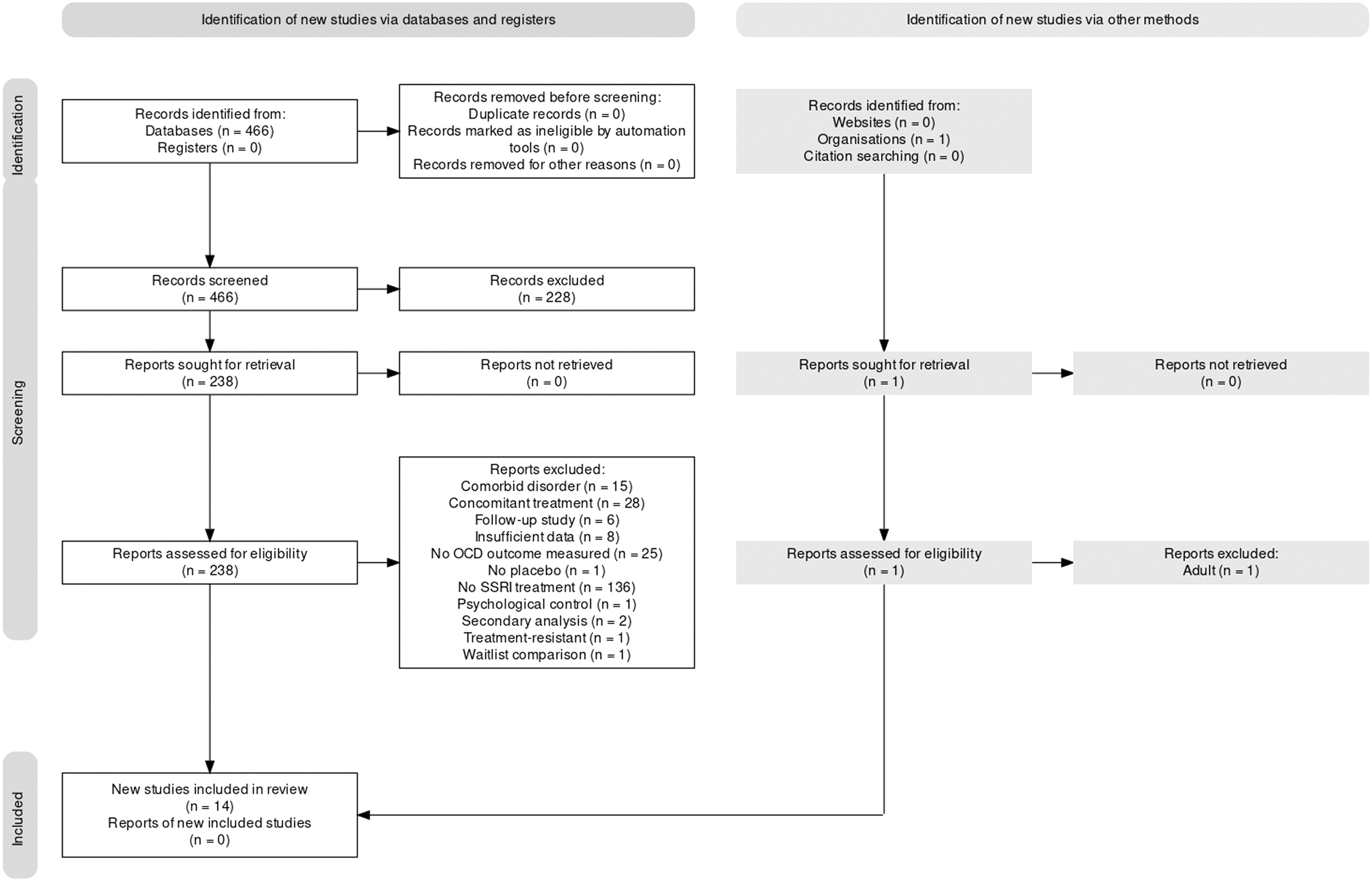
Systematic review inclusion and exclusion flow chart.
Statistical methods
The primary outcome for these analyses was the change in CY-BOCS total score from baseline to endpoint. A set of logarithmic trend treatment response models was developed. The relative treatment effects were modeled using a Bayesian inferential approach with parameters estimated using Hamiltonian Monte Carlo (HMC) simulation.
Change in OCD symptom severity was evaluated as a function of time, with average patient age, gender, and baseline severity in each study examined as covariates, using both aggregate logarithmic trajectory models and BHMs with the individual (study level) logarithmic trajectories to capture unobserved heterogeneity across studies. Posterior estimates were obtained from HMC simulations as previously described (Mills and Strawn, 2020; Stimpfl et al., 2021; Suresh et al., 2020).
For comparison of placebo, SSRI monotherapy, and SSRI+CBT combined therapy response by week, posterior distributions of the weekly difference in means were obtained from a time indicator random effects BHM. Differences in means, credible intervals, and so forth were determined from the posterior HMC samples. The logarithmic trajectory BHM was specified as
where
where
Statistical heterogeneity was quantified with standard measures: the Q statistic (i.e., weighted sum of squared differences between individual study effects and the pooled effect across trials) and I 2 (i.e., heterogeneity-related variance rather than variance attributed to sampling error). To further and more comprehensively assess heterogeneity, we examined (1) individual trend models, (2) time indicator random effects specifications, and (3) the robustness of each response model to alternative functional forms.
Analyses were conducted in Julia (version: 1.7.2) (Bezanson et al., 2017). The BHMs were each estimated using 5000 iterations of the No U-Turn HMC sampler in Turing.jl (Ge et al., 2018). For all analyses, Bayesian posterior tail-area equivalents of a frequentist p-value for evidence against the null hypothesis (H 0) were determined and considered statistically significant at the p < 0.05 level. Means are represented ± their standard deviations, and precision is expressed as credible intervals (95% CrIs).
Results
Characteristic of studies
Seventeen studies included pharmacotherapy arms, 7 studies included combined pharmacotherapy and psychotherapy (one used the same sample and this sample counted as 1 study for the purposes of comparing pharmacotherapy vs. psychotherapy studies), and 10 studies included a placebo or control arm (Table 1).
Characteristics of Included Studies
All studies included an SSRI arm and either a placebo or SSRI+CBT arm.
CBT, cognitive behavioral therapy; CY-BOCS, Children's Yale-Brown Obsessive Compulsive Scale; SSRI, selective serotonin reuptake inhibitor.
SSRI—compared with SSRI+CBT—studies had more patients in each treatment arm but were similar in female percentage (SSRI vs. placebo p = 0.754, SSRI vs. SSRI+CBT p = 0.817, SSRI+CBT vs. placebo p = 0.503), age (SSRI vs. placebo p = 0.784, SSRI vs. SSRI+CBT p = 0.943, SSRI+CBT vs. placebo p = 0.877), and baseline CY-BOCS severity score (SSRI vs. placebo p = 0.527, SSRI vs. SSRI+CBT p = 0.657, SSRI+CBT vs. placebo p = 0.390). In one study (Asbahr et al., 2005), because of discordance in reporting of CY-BOCS scores between a table and the graph, CY-BOCS scores were scaled based on Table 1, and one study that reported only baseline and 13-week outcomes was excluded.
Heterogeneity across studies
Heterogeneity measures across studies were as follows: Q = 15.88 (p = 0.256), I 2 = 18.15, τ 2 <0.001. For studies involving CBT or CBT+SSRI, Q = 11.29 (p = 0.080), I 2 = 46.83, τ 2 <0.001, whereas for studies involving SSRI monotherapy, Q = 56.09 (p < 0.001), I2 = 91.09, τ 2 <0.001.
Time course of treatment response compared with placebo
The best fitting model for antidepressant treatment response was a linear-logarithmic model (log. trend coefficients:  . Both SSRI and SSRI+CBT-related improvement in anxiety symptoms compared with placebo emerged early. Statistically significant standardized SSRI-placebo differences and SSRI+CBT-placebo differences emerged early in treatment (Fig. 2). However, we did not observe statistically significant differences between SSRI monotherapy and SSRI+CBT (Fig. 2) in either the magnitude of response or in the trajectory of response (Fig. 2).
. Both SSRI and SSRI+CBT-related improvement in anxiety symptoms compared with placebo emerged early. Statistically significant standardized SSRI-placebo differences and SSRI+CBT-placebo differences emerged early in treatment (Fig. 2). However, we did not observe statistically significant differences between SSRI monotherapy and SSRI+CBT (Fig. 2) in either the magnitude of response or in the trajectory of response (Fig. 2).
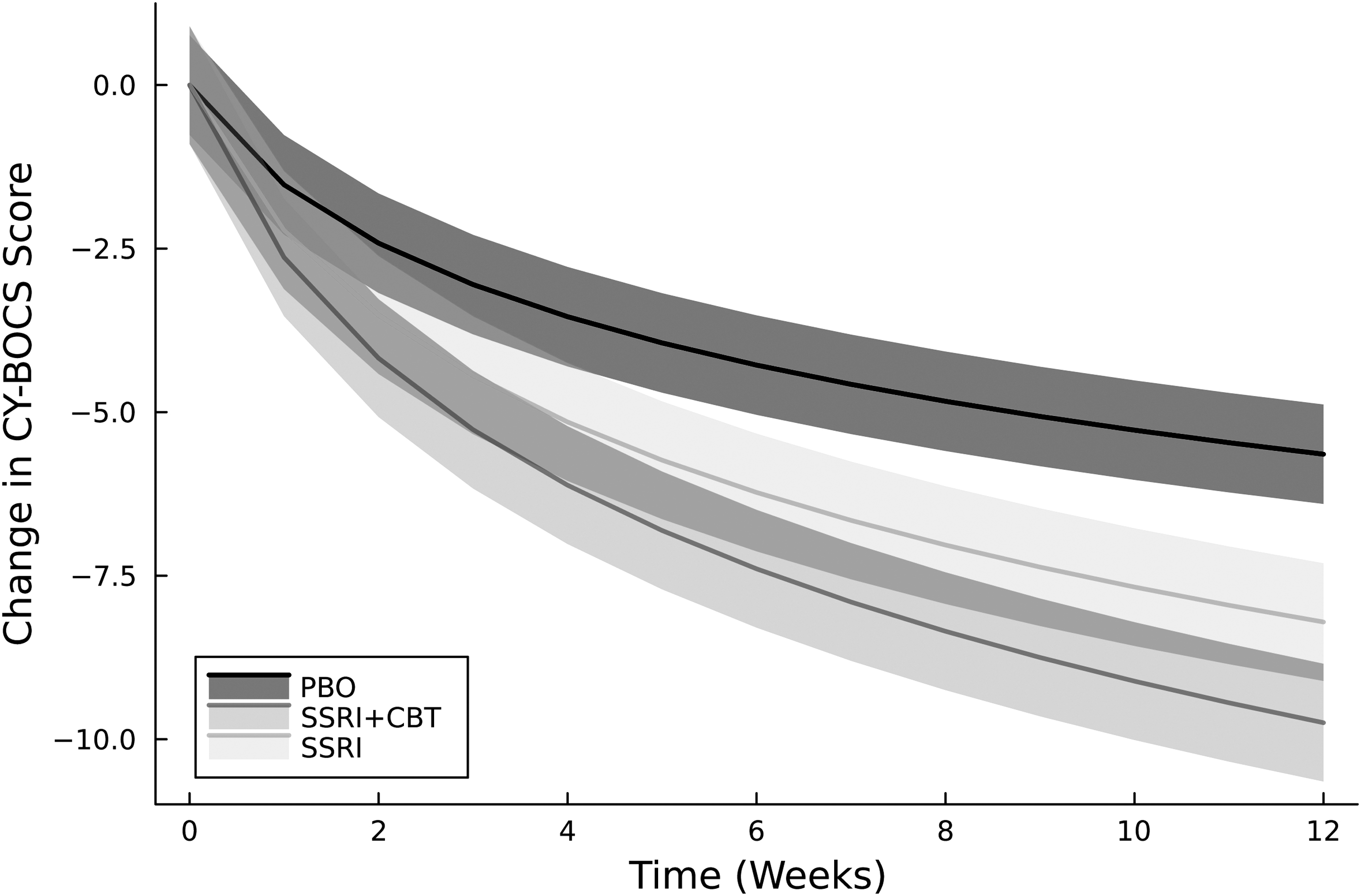
Improvement trajectory in children and adolescents with OCD. Improvement was logarithmic across all treatments and placebo. Solid lines represent the improvement in CY-BOCS score for patients receiving placebo, SSRI (SSRI), and SSRI+CBT. Shaded regions represent 95% credible intervals. CBT, cognitive behavioral therapy; CY-BOCS, Child Yale-Brown Obsessive-Compulsive Scale; OCD, obsessive-compulsive disorder; PBO, placebo; SSRI, selective serotonin reuptake inhibitor.
Predictors of response to CBT+SSRI and SSRI monotherapy
Across treatment groups, older patients had less improvement (β = 0.72 ± 0.06, 95% CrI: 0.605–0.832, 95% highest probability density interval [HPDI]: 0.604–0.832, p < 0.001) than younger patients. In addition, girls had less improvement than boys (β = 0.056 ± 0.01, 95% CrI: 0.04–0.071, 95% HPDI: 0.041–0.072, p < 0.001). Finally, patients with more severe symptoms at baseline had greater improvement (β = −0.085 ± 0.02, 95% CrI: −0.12 to −0.052, 95% HPDI: −0.118 to −0.051, p < 0.001).
Discussion
We have confirmed, meta-analytically, that SSRI+CBT and SSRI monotherapy are superior to placebo in youth with OCD and that treatment response is logarithmic: the greatest improvement occurs early during treatment. However, we did not observe the superiority of adding CBT to SSRI monotherapy, despite a numerically greater magnitude and rate of improvement for patients receiving CBT+SSRI. Several aspects of our findings warrant additional discussion and are directly relevant to the treatment of youth with OCD.
One question raised by the current results is why SSRI+CBT did not add value to SSRI alone, particularly when in several past randomized controlled trials, SSRI+CBT outperformed medication alone (Ivarsson et al., 2015; Romanelli et al., 2014; Woody and Szechtman, 2005), and in some cases, CBT alone outperformed medication (Ivarsson et al., 2015; Romanelli et al., 2014; Storch et al., 2013)? Our somewhat surprising finding regarding SSRI+CBT deserves some interpretation and discussion, given that a previous meta-analysis of pediatric OCD treatment has shown the effect size for CBT (d = 1.45) is considerably larger than that for SSRIs (d = 0.48) (Watson and Rees, 2008).
We hypothesize that the CBT for OCD used in the early trials included in the current meta-analysis suffered a similar fate to early CBT in trials of child anxiety disorders generally (Skarphedinsson et al., 2015). As in OCD, well-controlled studies also established CBT as the recommended first-line psychosocial treatment for child non-OCD anxiety disorders, largely due to CBT's superiority over waitlist control conditions (Higa-McMillan et al., 2016). But CBT for non-OCD pediatric anxiety disorders has not consistently outperformed active control conditions, and an emerging line of research suggests that in some cases, variation in response may relate to the underuse of the most active component of anxiety treatment protocols, namely, exposure (Ale et al., 2015; Whiteside et al., 2020).
Most manuals used in these trials spend initial sessions on less efficacious CBT components such as relaxation and cognitive restructuring, delaying the introduction of exposures of sufficient intensity and perhaps compromising treatment response (Peris et al., 2015).
Similarly, almost every pediatric OCD trial included in this meta-analysis used the same first-generation 14-session CBT manual, which prescribes psychoeducation, cognitive modification, and treatment planning for the first four sessions, with graduated exposures starting, in earnest, in session 5 (March and Mulle, 1998). Practically speaking, this means that a child in a CBT+med arm of a trial has been receiving the active ingredient of SSRI treatment (the medication itself) for fully a month before receiving the active ingredient of CBT (exposure). By extension, this also means that, at 12 weeks, the child has had at most seven sessions devoted to exposures. They have also not completed the full 14 sessions of the treatment manual.
Another important consideration in the outcomes of CBT for pediatric OCD is family accommodation and homework compliance (Freeman et al., 2018). Exposures—once they are actually introduced into CBT sessions—can only be expected to work if they are then practiced in ecologically valid settings—namely, the home and community settings where the child actually lives (Abramowitz et al., 2002; Park et al., 2014). But who is responsible for ensuring homework happens? To believe that already anxious children are likely to cajole themselves to complete exposure homework of sufficient frequency and intensity seems developmentally inconsiderate: Parents must be trained as exposure cotherapists.
And yet the early manual almost universally used in the OCD trials of this meta-analysis engages the child in individual sessions with little in the way of regular parental involvement beyond end-of-session check-ins (March and Muelle, 1998). More recent research has shown that augmenting treatment with family-based sessions specifically designed to discourage parental accommodation of anxious avoidance outperforms individual CBT and that decreasing family accommodation predicts symptom reduction and enhances treatment outcomes (Merlo et al., 2009; O'Connor et al., 2023; Peris et al., 2017; Piacentini et al., 2011)
Numerous studies and meta-analyses support the efficacy of SSRIs or CBT monotherapy in pediatric OCD (Geller et al., 2003; Varigonda et al., 2016). Given that improvement is likely with both CBT+SSRI compared with SSRI monotherapy, guidelines recommend CBT alone or CBT in combination with SSRIs as a first-line treatment for OCD in pediatric patients (Bloch and Storch, 2015; Geller and March, 2012); however, these results suggest that SSRI monotherapy might be considered—based on efficacy—among the first-line interventions.
Understanding the differences in improvement trajectory for OCD patients is important when considering treatment options. The varying clinical presentations and responses to the treatment of OCD underscore the need to individualize treatment (Bartz and Hollander, 2006). Historically, guidelines recommend a one-size-fits-all approach to treatment. For example, guidelines and expert opinions recommend CBT or CBT+SSRI (Bloch and Storch, 2015; Geller and March, 2012) but fall short in terms of helping clinicians identify which patient may benefit most from which treatment, which SSRI should be considered, or how the SSRI should be dosed.
In addition, these guidelines tell clinicians little about the trajectory of improvement, which is critically important for patients and their families. In the current meta-analysis, we examined response differences through 12 weeks of treatment; however, fully capturing the advantage of CBT may require longer, particularly in individuals with more severe symptoms (Adam et al., 2022). Thus, these findings, which reveal a numerical advantage of CBT+SSRI at 12 weeks, could conceal the true advantage of adding CBT to SSRIs, which may become apparent over the subsequent several weeks.
In this meta-analysis, regardless of whether CBT+SSRI or SSRI monotherapy is used, girls and older patients tended to improve less than boys and younger patients. These effects were present in both treatments raising the possibility that an intrinsic aspect of OCD subtends this reduced response. For clinicians, this suggests that additional strategies may be needed for these groups, including increased family involvement (Peris et al., 2017), strategies to target family dysfunction (Peris et al., 2019), alternative approaches to dosing SSRIs (Ramsey et al., 2020; Strawn et al., 2021), or perhaps more frequent therapy sessions (i.e., greater therapist contact) (McGuire et al., 2015).
Currently, CBT monotherapy and CBT+SSRI are first-line treatments for OCD (Geller and March, 2012), yet some patients may not engage in therapy or may lack access to experienced therapists (Piacentini et al., 2021). With exposure-based CBT, the most effective form of CBT for these patients, the dearth of access to high-quality practitioners and lack of competency standards have contributed to a gap in treatment for many youth with OCD. Ultimately, having more data on when patients can be expected to improve during their treatment course allows clinicians to better tailor a regimen compatible with their individual patients.
For example, in depressed adolescents treated with interpersonal psychotherapy for adolescents, increasing the frequency of therapy sessions or adding fluoxetine early (i.e., week 4) rather than later (i.e., week 8) conferred statistically and clinically significant advantages (Gunlicks-Stoessel et al., 2019).
Despite this being one of the few meta-analyses to examine SSRIs and SSRI+CBT in children and adolescents with OCD, there are several limitations. First, with regard to heterogeneity, BHMs allow us to control for observed variability; however, unobserved factors may still influence the response (McGlothlin and Viele, 2018). Second, baseline OCD severity differs across studies, which may lead to patients with milder baseline symptoms having less improvement. Similarly, comorbidity differs across studies and may differentially affect response to either pharmacotherapy, CBT (Højgaard et al., 2018), or their combination. Third, SSRI dose may have a modest correlation with blood concentrations in children and adolescents for reasons such as pharmacogenetics and differences in metabolism (Sakolsky et al., 2011; Strawn et al., 2019).
Fourth, there is variability in how CBT, particularly exposure-based therapy, is practiced. In fact, not all clinicians fully leverage exposure-based therapy, although this type of CBT is most associated with positive outcomes in OCD patients (Kircanski and Peris, 2015). Fifth, we did not preregister this meta-analysis, nor was the Cochrane Risk of Bias tool applied. However, recent systematic examinations of response to SSRIs and CBT in pediatric patients with OCD have assessed risk of bias in these studies (Uhre et al., 2020). Sixth, some studies may have had significant site effects, which were not captured in our analyses. However, in the largest trial in which site effects were reported—POTS—we extracted the CY-BOCS scores from a model that controlled for site.
As another potential limitation of this study, we focused on comparing CBT+SSRI and SSRI monotherapy for several reasons. There are already multiple meta-analyses of CBT compared with waitlist conditions, and we sought to include trials with a placebo comparison arm to not bias the medication component of treatment. The control group in CBT trials—frequently waitlist—is very different from a placebo group which may raise issues related to participant/family blinding. An additional control group in the analysis (i.e., waitlist) substantially increases the unobserved heterogeneity, which complicates analysis and interpretation.
Conclusions
In this meta-analysis, SSRI+CBT and SSRI monotherapy were superior to placebo in youth with OCD, and the greatest improvement occurred early during treatment. However, our results do not suggest the superiority of adding CBT to SSRI monotherapy, despite a numerically greater magnitude and rate of improvement for patients receiving CBT+SSRI. In the current meta-analysis, we examined response over 12 weeks of treatment; however, fully capturing the advantage of CBT may require longer. Moreover, these results have implications for how CBT is implemented. In most of the trials included in the present meta-analysis, the same first-generation 14-session manualized CBT was used. This manual prescribes psychoeducation, cognitive modification, and treatment planning for the first four sessions, with graduated exposures starting, in earnest, in session 5 (March and Mulle, 1998). In essence, this may have delayed and reduced the time during which patients could benefit from the key ingredient of CBT—exposure.
Clinical Significance
Guidelines for treating OCD in children and adolescents recommend CBT monotherapy as the initial treatment (Geller and March, 2012). Furthermore, a meta-analysis suggested that CBT and SSRIs produce similar improvements in youth with OCD (Uhre et al., 2020). However, in the interest of balance, we point out that expert reaction to this meta-analysis raised methodological concerns, particularly with regard to the grouping of CBT trials (e.g., group CBT, internet-based CBT) and the qualitative assessment of bias in CBT trials (Storch et al., 2020). Thus, although our results suggest that the combination of SSRI+CBT and SSRI monotherapy may produce similar improvements, the decision to utilize any treatment (or combination) is necessarily based on myriad clinically important factors.
Accordingly, clinicians may consider other factors beyond differences in efficacy when selecting from evidence-based treatments, including patient and family preference (Lewin et al., 2014), comorbidity patterns (McGuire et al., 2015), and perhaps pharmacogenetic factors that influence response (Ramsey et al., 2020).
Footnotes
Authors' Contributions
J.R.S. contributed to conceptualization, methodology, data acquisition and data curation, interpretation, writing—original draft, writing—editing, and review; K.K.D. carried out conceptualization, interpretation, writing—original draft, writing—editing, and review; E.M.M. was involved in data acquisition and data curation, writing—original draft, writing—editing, and review; J.M.H. was in charge of data acquisition, writing—editing, and review; J.A.M. took charge of conceptualization, methodology, analysis, interpretation, data visualization, writing—original draft, and writing—editing, and review; V.S. was in charge of methodology, analysis, interpretation, data visualization, writing—editing, and review.
Disclosures
J.R.S. has received research support from AbbVie, PCORI, and the National Institutes of Health. He has provided consultation to Cerevel, Intracellular Therapeutics Otsuka and the FDA. He receives royalties from Springer Publishing and UpToDate and received material support from Myriad. He has also received honoraria from Medscape Live, Neuroscience Education Institute, the American Academy of Pediatrics, and the American Academy of Child and Adolescent Psychiatry. J.A.M. receives support from the Yung Family Foundation.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.