
Abstract
Objective:
Pediatric anxiety disorders are associated with increased stimulus-driven attention (SDA), the involuntary capture of attention by salient stimuli. Increased SDA is linked to increased activity in the right ventrolateral prefrontal cortex (rVLPFC), especially in the portion corresponding to the ventral attention network (VAN). In this study, we present a small clinical trial using a novel attention training program designed to treat pediatric anxiety by decreasing SDA and activity in the rVLPFC.
Methods:
Children ages 8–12 with anxiety disorders (n = 18) participated in eight sessions of attention training over a 4-week period. At baseline and after completing training, participants completed clinical anxiety measures and a battery of cognitive tasks designed to measure three different aspects of attention: SDA, goal-oriented attention, and threat bias. A subset of participants (n = 12) underwent baseline and post-training neuroimaging while engaged in an SDA task. Brain analyses focused on activity within the rVLPFC.
Results:
Parent (p < 0.001)-, child (p < 0.002)-, and clinician-rated (p < 0.02) anxiety improved significantly over the course of training. Training significantly altered SDA [F(1,92) = 8.88, corrected p-value (p cor) < 0.012, uncorrected p-value (p uncor) < 0.004]. Anxiety improvement correlated with improvements in goal-directed attention [r(10) = 0.60, p cor < 0.12 p uncor < 0.04]. Within an area of the rVLPFC corresponding to the cingulo-opercular network (CON), there was a main effect of training [F(1,20) = 6.75, p cor < 0.16, p uncor < 0.02], with decreasing signal across training. There was a significant interaction between training and anxiety on this region's activity [F(1,20) = 9.48, p cor < 0.048, p uncor < 0.006]. Post hoc testing revealed that post-training activity within this CON area correlated with residual anxiety [r(10) = 0.68, p < 0.02].
Conclusions:
SDA and rVLPFC neural activity may be novel therapeutic targets in pediatric anxiety. After undergoing a training paradigm aimed at modifying this aspect of attention and its underlying neural circuitry, patients showed lower anxiety, changes in SDA and goal-oriented attention, and decreased activity in the CON portion of the rVLPFC.
Introduction
Pediatric anxiety disorders are common (Kessler et al., 2005) and correlate with psychological, medical, and functional impairment (Bitsko et al., 2018). Available treatments benefit many, but patients often experience residual symptoms (Peris et al., 2021). New treatments are needed that target the underlying cognitive and neural bases of pediatric anxiety. In this study, we describe a novel treatment designed to modify attention-related cognitive and neural targets in a pediatric group with anxiety disorders.
Attention is a central cognitive process with direct relevance to anxiety disorders. An expansive literature highlights elevated attention toward threatening stimuli (“threat bias” or TB) in anxiety disorders. The extent of TB correlates with symptom severity across pediatric anxiety disorders (Abend et al., 2018). A cognitive training program, attention bias modification (ABM), has targeted TB in numerous clinical trials of pediatric anxiety disorders (Lazarov and Bar-Haim, 2021). Evidence suggests that ABM decreases anxiety symptoms by reducing TB (Amir et al., 2011); however, effect sizes are modest (Linetzky et al., 2015; Mogoase et al., 2014). We hypothesize that cognitive training approaches could be improved by targeting additional, abberant facets of attention, including error sensitivity, emotional regulation, top-down control, and stimulus-driven attention (SDA) (Sylvester et al., 2012).
Emerging literature suggests that pediatric anxiety disorders are associated with a generalized increase in SDA, the involuntary capture of attention by all salient stimuli, regardless of emotional valence (Eysenck et al., 2007; Sylvester et al., 2012). SDA to suddenly appearing, salient stimuli includes a rapid orientation of attention toward the location of the stimulus (“initial orienting”) followed shortly thereafter (∼500 mseconds) by impaired attention at the location of the stimulus onset (“inhibition of return”) (Klein, 2000). Increased initial orienting of SDA (Corbetta et al., 2008) may partly explain other attention-related alterations in anxiety disorders, including TB (Sylvester et al., 2016). Both pediatric (Perino et al., 2021b) and adult (Pacheco-Unguetti et al., 2010) samples with heightened anxiety have been shown to have greater involuntary capture of attention by irrelevant salient stimuli, with differential effects at short and longer cue-target delays (Perino et al., 2021b).
Right ventrolateral prefrontal cortex (rVLPFC) activity may be a key neural marker and measurable treatment target in pediatric anxiety disorders. In children with anxiety disorders, elevated rVLPFC activity is associated with altered processing of emotional stimuli (McClure et al., 2007; Strawn et al., 2012), increased TB (Britton et al., 2012), and increased SDA (Perino et al., 2021b). The VLPFC connects multiple attention networks (Uddin et al., 2019) implicated in anxiety disorders (Sylvester et al., 2012). It includes portions of the ventral attention network (VAN), responsible for SDA (Corbetta and Shulman, 2002), and the cingulo-opercular network (CON), which underlies the maintenance of goal-oriented behavior (Dosenbach et al., 2007).
Based on the literature highlighting the rVLPFC's role in pediatric anxiety, in a recent study of pediatric anxiety using an SDA functional magnetic resonance imaging (fMRI) task, we focused a priori analyses on the rVLPFC. A VAN area within the rVLPFC showed the strongest relationship between neural activation and anxiety, but we also detected relationships between anxiety and activity within the CON and frontoparietal network areas. CON/VAN interactions are vital to the adaptive control of attention, balancing top-down attention to current task goals with appropriately responding to unexpected stimuli (Corbetta et al., 2008). We have found that CON/VAN resting-state connectivity is disrupted in anxiety disorders and may account for the link between altered SDA and anxiety (Perino et al., 2021a).
In the current study, we present a small, open, pilot clinical trial of n = 18 youth ages 8–12 years with current anxiety disorders who completed a novel cognitive training program. The training was designed to improve anxiety symptoms by reducing SDA and attention-related rVLPFC activity. Participants completed eight biweekly 30-minute training sessions, during which they had to maintain attention at a particular location while ignoring salient distractors appearing at unpredictable locations and intervals. Subjects underwent baseline and post-training clinical interviews, cognitive tasks, and a functional neuroimaging SDA task. Trial design, along with primary and secondary anxiety outcome measures, was preregistered (Clinicaltrials.gov, ID No. NCT03790696). We hypothesized that training would decrease symptoms of anxiety by reducing SDA.
Based on our previous findings, we predicted differential effects across cue-target delay conditions (Perino et al., 2021b). We also hypothesized that training would reduce neural activity evoked by unexpected stimuli within the rVLPFC. Our results provide initial data on a novel treatment for pediatric anxiety disorders.
Materials and Methods
Participants
We recruited participants ages 8–12 years with anxiety disorders from primary care clinics and elementary schools in the St. Louis, Missouri region. Informed consent was obtained from parents and all participants also signed assent forms. All procedures in this study were approved by the Washington University School of Medicine Institutional Review Board.
Parents were initially screened using the Screen for Child Anxiety Related Emotional Disorders (SCARED; Birmaher et al., 1999) and Mood and Feelings Questionnaire (MFQ; Messer et al., 1995). Participants were invited to participate who (1) scored above threshold for separation anxiety disorder (SAD), generalized anxiety disorder (GAD), and/or social phobia (SP) and (2) their parent reported anxiety as a primary concern. An in-person, baseline evaluation session included a semistructured clinical interview using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (Kaufman et al., 2016) for DSM-5 psychiatric diagnoses. We included participants meeting criteria for current GAD, SAD, and/or SP. Participants with comorbid depression were included if anxiety was the primary parent concern. Participants on stable selective serotonin reuptake inhibitor (SSRI) medication doses were included.
Exclusion criteria included the following: active suicidality, a primary concern of depression, any non-SSRI medication use, diagnosis of attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder, pervasive developmental disorder, intellectual disability, schizophrenia, or any medical disorders.
Of 41 children screened, 28 met the eligibility criteria. Ineligibility reasons included autism diagnosis, primary depression diagnosis, active suicidality, and lack of significant anxiety. Seven eligible, screened participants did not participate further due to elective withdrawal before baseline experimental visit (2), scheduling conflicts (1), or nonresponse (4). Of the 21 consented participants, 2 were excluded for not meeting specified anxiety disorder at baseline assessment and 1 dropped out for COVID infection. Eighteen subjects completed baseline and post-training anxiety data, but one subject only completed three training sessions. The 17 remaining participants completed baseline through post-training behavioral sessions, with 1 participant stopping post-training behavioral session early because of being unable to complete the eye tracking task.
Twelve participants also completed baseline and post-training neuroimaging sessions, with the other five excluded from neuroimaging sessions due to metal dental braces (4) or excessive motion (1; insufficient blood-oxygen-level-dependent [BOLD] runs with >150 motion-free frames). Enrolled participants were randomized between two cognitive training task versions. There were no significant differences in age, gender, anxiety diagnosis, pretreatment anxiety, or any other baseline measures of interest in participants who did versus those who did not complete neuroimaging (Table 1; p > 0.05 for all).
Patient Demographics of Behavioral Sample and Subset of Participants Who Completed All Scanning Sessions
There were no significant differences (p > 0.05) in any baseline measures including baseline anxiety (as measured by SCARED—parent report).
GAD, generalized anxiety disorder; SCARED, Screen for Child Anxiety Related Emotional Disorders.
Measures
Anxiety measures included parent- and patient-reported SCARED (Birmaher et al., 1999) and clinician-administered (Pediatric Anxiety Rating Scale [PARS]; Riddle et al., 2002) scales. Additional self-reported scales measured mood [MFQ and Children's Depression Inventory (Kovacs, 1985)], attention [Conners' Parent Rating Scale (Conners et al., 1998)], and problematic emotions and behaviors [Child Behavior Checklist parent report (Achenbach, 1999)]. We obtained PARS/SCARED during screening, baseline, and post-training behavioral sessions. SCARED was obtained weekly during training sessions 2, 4, 6, and 8. Change in SCARED from baseline to the last measurement (post-training or last available survey) was predefined as a primary study outcome measure since it was obtained most often (Clinicaltrials.gov, ID No. NCT03790696). Change in PARS from baseline to post-training was a predefined secondary outcome measure.
Study approach
There were two baseline sessions. The behavioral session included a diagnostic psychiatric interview, clinical measures, and computerized attention tasks. The neuroimaging visit included structural and functional magnetic resonance imaging scans. Participants subsequently completed eight twice-weekly cognitive training sessions and weekly anxiety self-reports. Participants underwent post-training behavioral and neuroimaging sessions (full schematic in Supplementary Fig. S1).
Attention tasks
Participants completed three computerized tasks measuring aspects of attention during the baseline and post-training behavioral sessions (Fig. 1A–C).
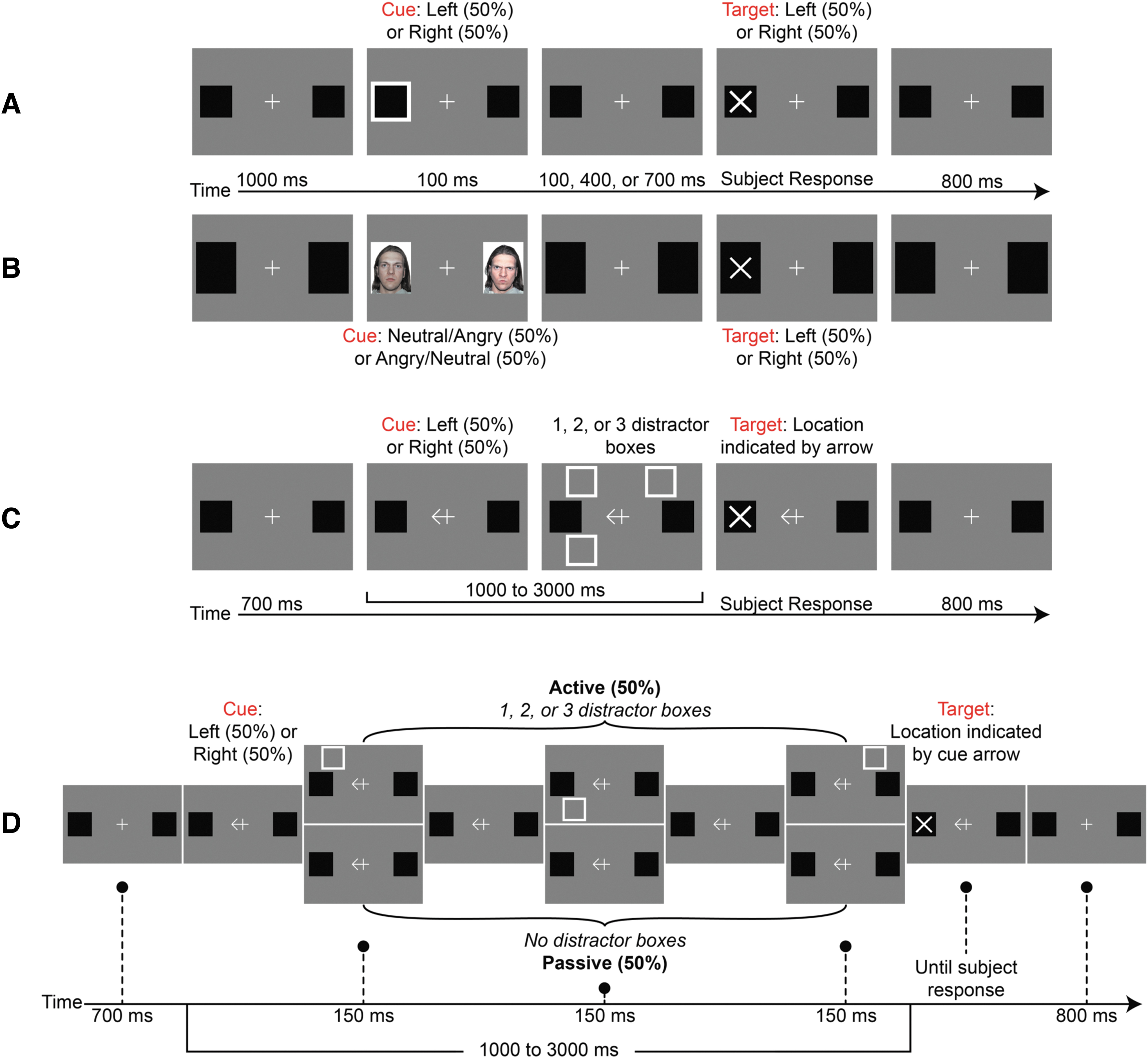
Behavioral tasks used to measure various aspects of attention and attention training task. Participants completed three behavioral tasks at baseline and post-training behavioral sessions
We measured SDA using an adapted Posner cueing paradigm (Fig. 1A) (Posner and Cohen, 1984). Each trial began with a central fixation cross for 1000 mseconds. Next, a “box” cue appeared on the left or right side of the screen for 100 mseconds. After a variable cue-target onset delay (200, 500, or 800 mseconds), a target “X” appeared at the cued (valid trials) or uncued (invalid trials) location. Target location was randomized equally between the left and right sides, unrelated to the preceding cue. Participants pressed a button indicating which side on the screen the target appeared. Trials ended with an 800 mseconds blank screen. Cue-target delay and valid/invalid trial conditions were counterbalanced in a pseudorandomized order. SDA is operationalized as reaction time (RT) for invalid trials minus RT for valid trials.
The second attention task used a modified dot probe paradigm (MacLeod et al., 1986) to measure TB (Fig. 1B). Trial structure was identical to the SDA task except for the cues, an “angry” face stimulus and a “neutral” face stimulus, which appeared simultaneously on opposite sides of the screen. We quantified TB as the difference of RTs to neutral minus RTs angry trials (positive scores indicate attention bias toward the angry face).
A third task assessed goal-directed attention in the face of distractors (Fig. 1C). A 700 mseconds fixation period was followed by a central “arrow” cue pointing to the eventual target location (left or right side) with 100% accuracy. The cue remained on screen throughout the trial. Following a randomly variable cue-target delay of 1000–3000 mseconds, a target “X” appeared at the cued location. Participants pressed a button indicating the side of the screen on which the target appeared. During some trials, 1–3 distractor boxes appeared one at a time for 150 mseconds each during the cue-target delay. Distractors never appeared at potential target locations. Subject RTs were compared from baseline to post-training sessions to quantify directed attention improvements.
Cognitive training task
Following baseline sessions, participants completed our novel cognitive training protocol (Fig. 1D). The training task was designed to encourage directed attention and reduce SDA, the tendency of irrelevant stimuli to capture attention. We utilized a task requiring participants to hold their attention at a cued location during a variable delay. The training task was identical to the goal-directed attention task, except that a subset of participants (n = 10) were randomly assigned to a task version where 1–3 distractor boxes appeared, sequentially, at random screen locations for 150 mseconds (active condition). Distractors did not predict and were never presented at the target location. For the remaining participants (n = 8), no distractors appeared (passive condition). The presence of distractors did not impact key outcomes (Supplementary Fig. S2); primary analyses are presented collapsed across both conditions. Participants underwent eight twice-weekly 45-minute training sessions.
Each attention task included 240 total trials split into 5 equal blocks of 48 trials. Each cognitive training task session included 242 trials split into 5 blocks of 48 or 49 trials. See Supplementary Methods section in the Supplementary Data.
Clinical trial information
Study data were collected as a registered clinical trial (Clinicaltrials.gov, NCT03790696). Of note, only 18 of the 21 consented participants completed the study (n = 2 did not meet diagnostic anxiety criteria, n = 1 due to active COVID infection). Participants were randomized to active and sham training. However, since there were no differences in anxiety change (primary clinical outcome) between active and sham treatment groups (Supplementary Fig. S2), we combined data from both arms for subsequent analyses.
Neuroimaging session protocols
Imaging parameters
We obtained and preprocessed fMRI images identically to previously published methods (Perino et al., 2021b). See details in the Supplementary Methods section in the Supplementary Data.
fMRI task design
Participants completed an fMRI attention task during each neuroimaging session. Similar to our behavioral tasks, this task involved cues appearing on either side of the screen, followed by a variable cue-target delay and eventually asked participants to respond to the target. The cue was a square box in the “box” condition, most similar to the SDA behavioral task. We focused on this condition in the main text. Briefly, a fixation cross appeared first and remained on the screen throughout each trial. Next, the cue appeared for 150 mseconds on the left or right side of the screen. After a variable cue-target onset delay (200, 500, or 800 mseconds), a target “arrow” appeared. Participants indicated via button press if the arrow was pointing upward or downward.
Targets appeared with equal probability on the cued (valid) or uncued (invalid) side of the screen with valid/invalid trials counterbalanced and other variables (cue-target delay, target side) pseudorandomized within each five-trial block. Each block included five trials over about 18 seconds in total, separated by a variable 18–33 repetition time (TR) fixation period. Each run contained 8 blocks of trials, lasting 5.808 minutes with 484 frames (TR = 720 mseconds). Participants completed 160 total trials over 4 runs, 40 of each cue-type condition. We included all trials in the final analysis regardless of accuracy. Other conditions are described in Supplementary Data.
fMRI task analysis
We modeled regressors for BOLD response to each trial block using a block design and convolved each regressor with a standard hemodynamic response function (Boynton et al., 1996). For each participant, we ran a general linear model on BOLD activity with regressors for each cue-type condition (box, angry, neutral, angry+neutral) as well as baseline and linear run trends. We ran this model at each surface vertex and then extracted parameter estimates from eight functional areas within the rVLPFC (Gordon et al., 2016). As discussed in the introduction, functional areas were selected a priori for their role in anxiety disorders and association with anxiety-related attention changes in our prior study (Perino et al., 2021b). In the Results section below, we analyze functional neuroimaging analyses from box cue trials based as in our own prior work. Analysis including all conditions is presented in Supplementary Data.
Statistical analyses
All comparisons between two groups were performed using paired or between-subjects Student's t-tests. Any individual with a median RT >2 standard deviations outside the group mean on that task was removed from analysis before statistical testing. We correlated relationships between anxiety measures and behavioral task performance using the Pearson correlation coefficient. Omnibus analysis of variance (ANOVA) for the SDA task was a 2 × 3 ANOVA measuring time (baseline vs. post-training) and cue-target delay (200 mseconds vs. 500 mseconds vs. 800 mseconds) as main effects. The dependent variable was the mean validity effect (invalid − valid cue RTs) in each condition.
Our a priori hypotheses included looking at changes in the validity effect for each delay condition separately. We also calculate a composite measure of SDA (validity effect at 200 mseconds − [validity effect at 500 mseconds + validity effect at 800 mseconds]) combining the initial cueing effect with subsequent inhibition of return (Klein, 2000). We modeled group-level effects of training and anxiety on attention-related activation during our fMRI task using a linear mixed-effects model (Kuznetsova et al., 2017), implemented via R statistical software version 3.6.3 (R Core Team, 2021). We performed Bonferroni correction on p-values within each category of a priori analyses (Omnibus ANOVAs, correlations with anxiety, neuroimaging testing). We present corrected p-values (p cor) and uncorrected p-values (p uncor) for all applicable analyses.
Results
Anxiety changes with cognitive training
We observed a significant decrease in anxiety as measured by our primary outcome of SCARED—parent version from baseline to last measurement [mean (95% confidence interval, CI): −22.44 (−16.96 to −27.92), t(17) = 8.63, p < 0.001; Fig. 2]. In addition, all secondary anxiety measures significantly decreased across training: SCARED-child report [mean (95% CI): −10.39 (−4.85 to −15.92), t(17) = 3.96, p < 0.002], and the clinician-rated PARS severity score [mean (95% CI): −3.71 (−0.70 to −6.73), t(13) = 2.26, p < 0.02].
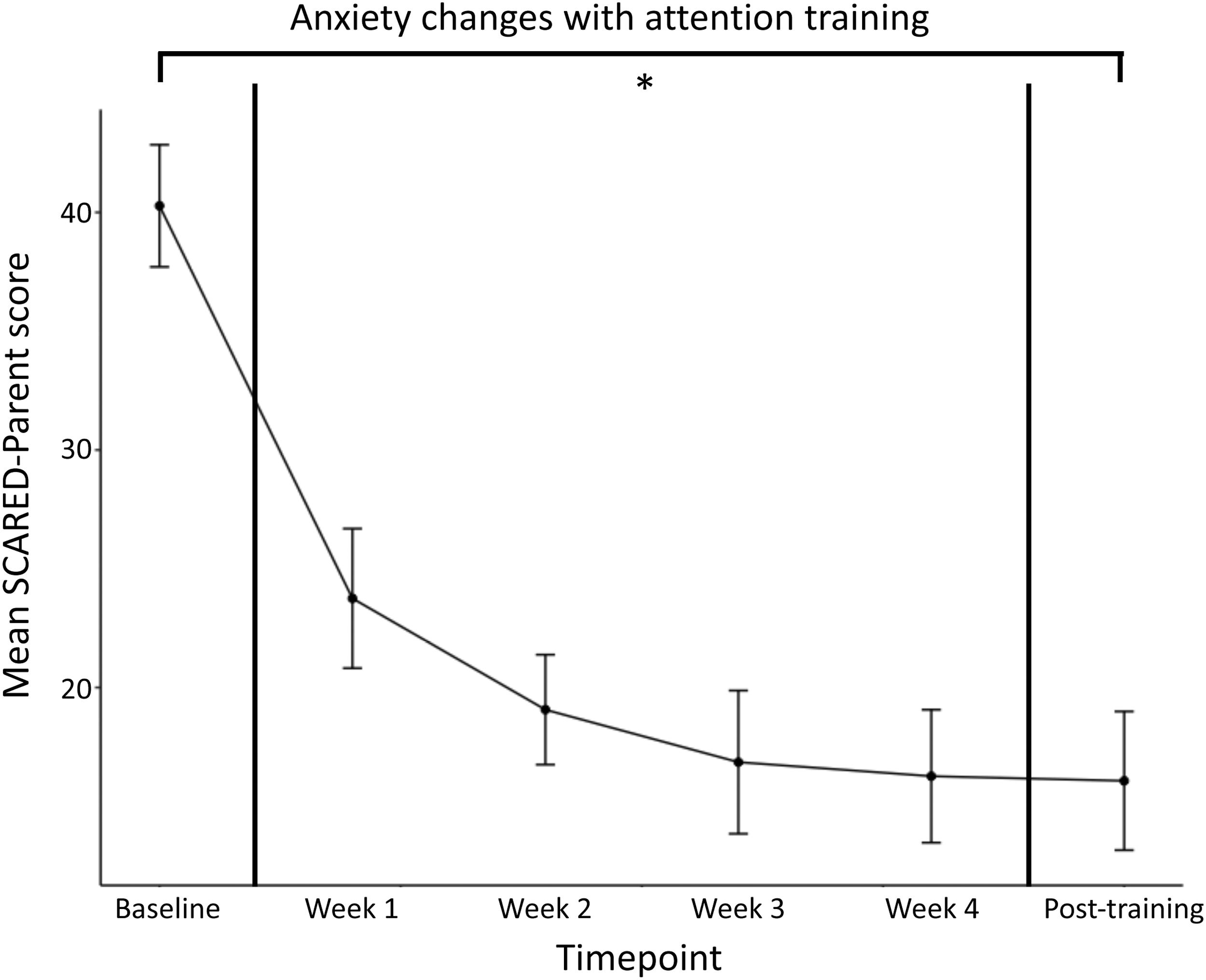
Anxiety decreases over the course of attention training. Anxiety (y-axis) as measured by the Screen for Child Anxiety, Parent version (SCARED-Parent) plotted across all time points (x-axis). Anxiety decreased significantly from baseline to final measurement [t(17) = 8.63, p < 0.001], the primary clinical outcome in this study. *p < 0.05. SCARED, Screen for Child Anxiety Related Emotional Disorders.
Training impacts on attention
An omnibus ANOVA characterizing SDA showed significant main effects of training [F(1,92) = 8.88, p cor < 0.012, p uncor < 0.004] and cue-target delay [F(1,92) = 26.70, p cor < 3 × 10−5, p uncor < 1 × 10−5). Post hoc testing showed increased attention toward the cued versus uncued location after training [mean change (95% CI): 21.42 mseconds (9.70 to 33.13 mseconds), t[3.90(15), p < 0.002]; Fig. 3A). The omnibus ANOVA characterizing goal-directed attention showed a significant main effect of training [F(1,164) = 19.75, p cor < 0.0003, p uncor < 0.0001], such that participant RTs were faster after training compared with baseline (Fig. 3B). There were no significant changes in TB across training (Fig. 3C).
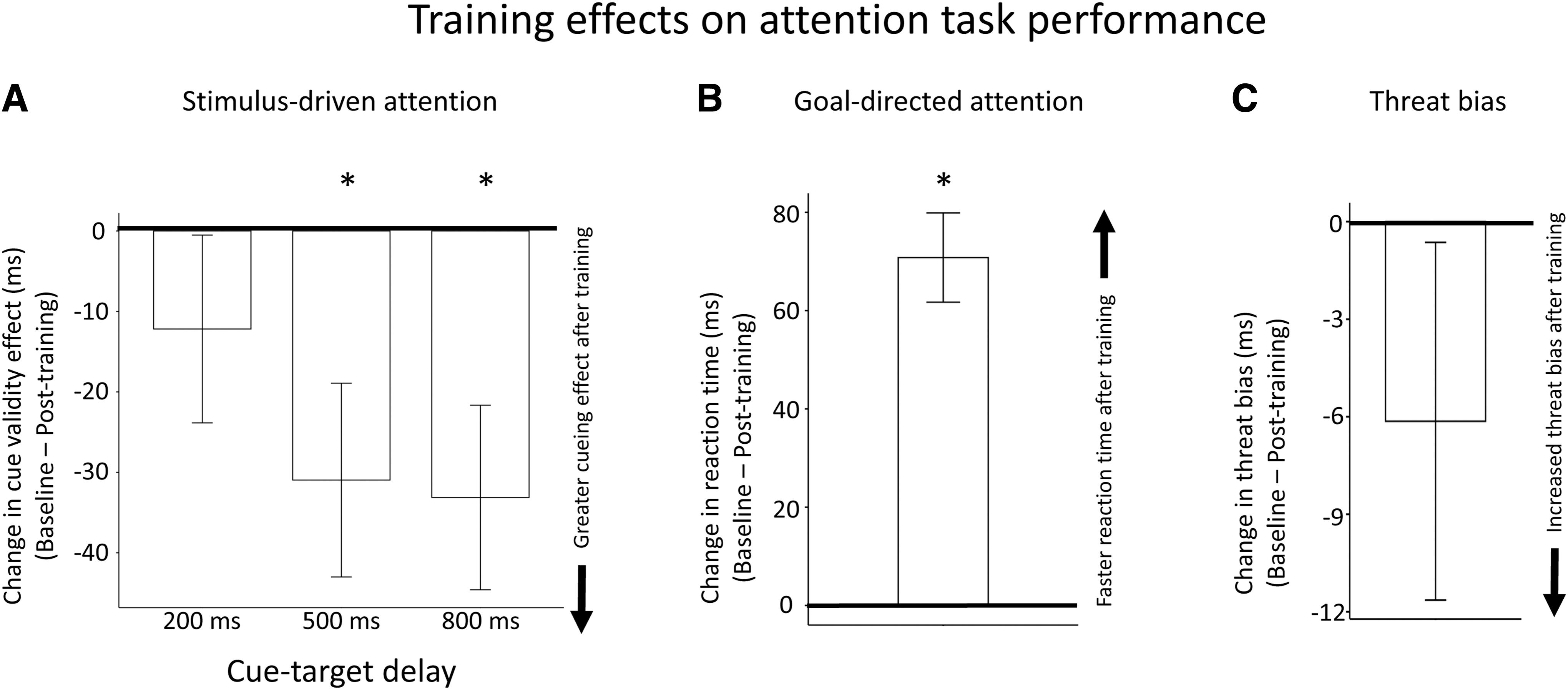
Following training, participants show changes in stimulus-driven and goal-directed attention, but not threat bias. All changes reported as baseline minus post-training.
Given the known impact of cue-target delay on SDA [i.e., orienting toward cues at short delays, followed by impaired attention at the cued location at longer delays (Klein, 2000)], we followed the main effect of training in the SDA task with a series of post hoc tests examining each cue-target delay separately (Supplementary Fig. S3). As expected, at baseline, participants responded faster to targets at the cued location with a 200 mseconds delay [t(17) = 3.09, p < 0.007], and faster at uncued locations at the 500 mseconds [t(17) = 2.23, p < 0.04] and 800 mseconds [t(17) = 4.08, p < 0.001] delays. After training, responses remained faster at the cued location with 200 mseconds delay [t(15) = 3.42, p < 0.004].
At the longer cue-target (500/800 mseconds) delays, however, there were no longer any cueing effect post-training, that is, there was an abolishment of inhibition of return (both p > 0.05). This loss of inhibition of return was also reflected in significant changes in the validity effect (valid trial RT − invalid trial RT) across training in 500 and 800 mseconds cue-target delay conditions [500 mseconds: t(15) = 2.57, p < 0.03; 800 mseconds: t(15) = 2.89, p < 0.02; Fig. 3A].
Training effects on selected neural regions of interest
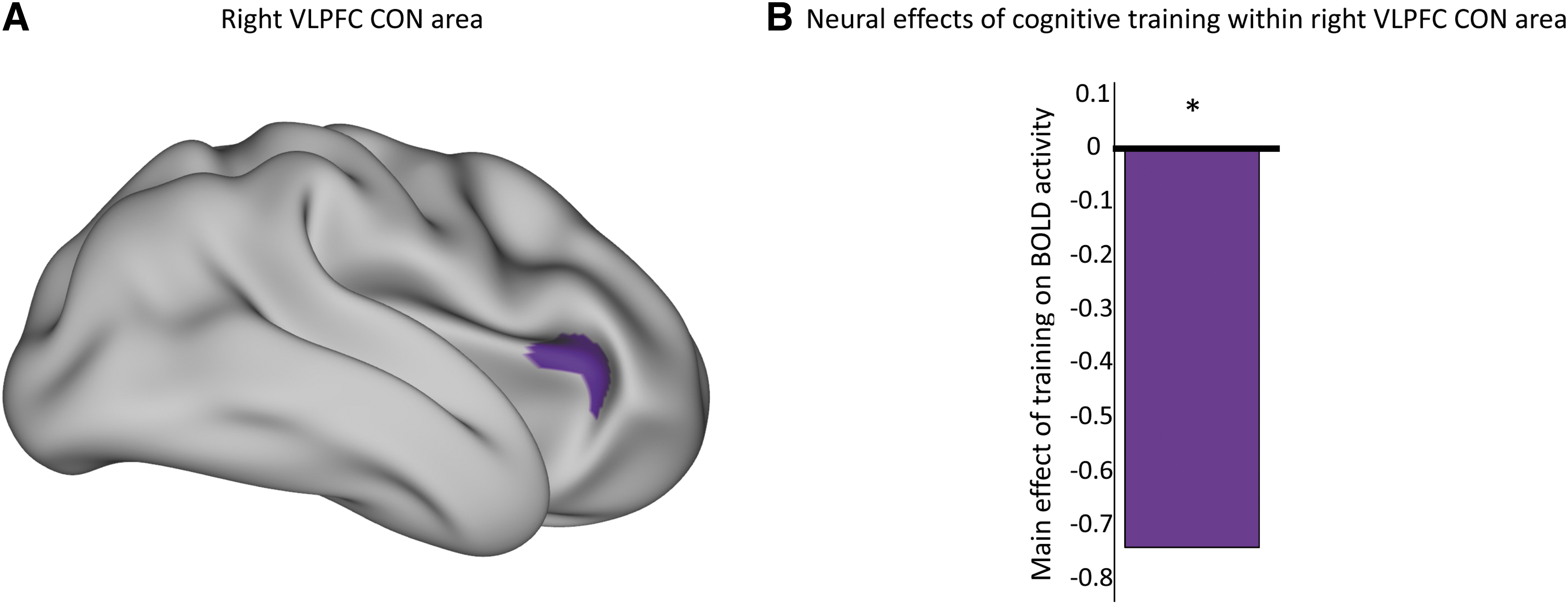
We examined the impact of training on BOLD activity in a priori selected regions within the rVLPFC based on our prior work (Perino et al., 2021b) and a substantial literature indicating that pediatric anxiety is associated with increased activity in this anatomical location (Supplementary Fig. S4A) (McClure et al., 2007; Strawn et al., 2012; Sylvester et al., 2012). To parallel the training task, analyses focused on fMRI blocks that included the box cue. Among the a priori rVLPFC regions-of-interest, there was decreased activity in an area belonging to the CON [F(1,20) = 6.75, p cor < 0.16, p uncor < 0.02] (Fig. 4 and Supplementary Fig. S4B).
Relationships between target engagement and changes in anxiety
We tested the relationships between individual training-related changes in attention and anxiety. In the goal-directed attention task, decreases in participant RT correlated with decreases in anxiety [r(10) = 0.60, p cor < 0.12, p uncor < 0.04; Fig. 5A]. In the TB task, increases in TB correlated with anxiety decreases [r(14) = −0.51, p cor < 0.15, p uncor < 0.05].
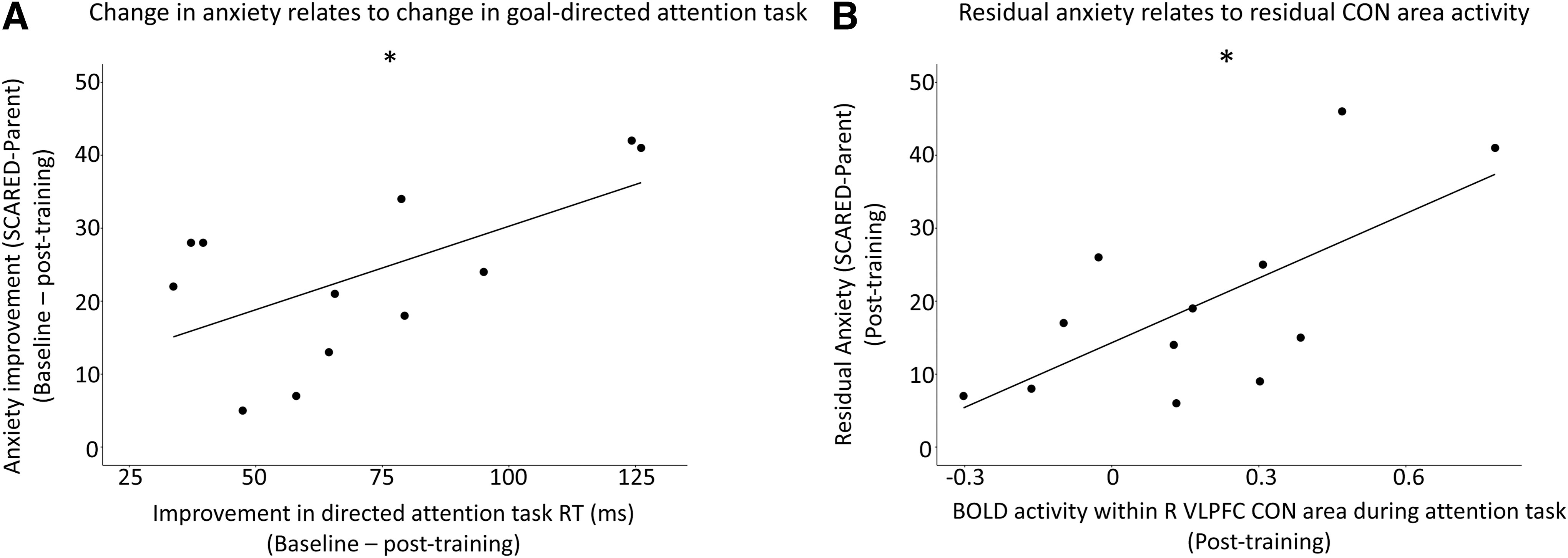
Links between anxiety, behavior, and neural activation over the course of cognitive training.
Finally, we related changes in the SDA (box cue) condition of our fMRI task to changes in anxiety. Activity in the CON parcel identified above showed a significant interactive effect between anxiety and training [F(1,20) = 9.48, p cor < 0.048, p uncor < 0.006]. Post hoc testing within this region showed no correlation between baseline (pretraining) activity and anxiety, but a positive correlation in post-training activity and anxiety [r(10) = 0.68, p < 0.02; Fig. 5B].
Discussion
In this pilot clinical trial, a novel cognitive training program reduced anxiety in conjunction with changes in attention and neural activity. We observed alterations of SDA and increases in goal-directed attention after training. In an fMRI attention task, activity within the CON portion of the VLPFC decreased after training. Individual differences in training-related attention changes correlated with treatment response, and individual post-training rVLPFC CON area BOLD activity was related to residual anxiety.
This program targeted pediatric anxiety with attention training, reducing anxiety by all predefined primary and secondary measures (Clinicaltrials.gov, ID No. NCT03790696). Depression symptoms also decreased significantly, although baseline symptoms were below clinical thresholds in all but one participant (Supplementary Fig. S5). The training task was designed to reduce SDA toward irrelevant stimuli while encouraging top-down, goal-oriented attention. Behavioral changes from baseline to post-training suggest that this attention training achieves both goals.
Prior work suggests that anxiety disorders are associated with increased SDA toward suddenly appearing stimuli. SDA includes rapid, initial orienting toward suddenly stimuli shortly after they appear (e.g., <200 mseconds) followed by impaired attention at the cued location at longer durations (e.g., >500 mseconds). This latter phenomenon is called “inhibition of return” and may prevent individuals from getting their attention stuck at a particular location during, for example, search Klein (2000). Here we found a main effect of training on SDA, such that attention, averaged over all cue-target durations, was better at the cued location after training. Post hoc tests, however, revealed that improved attention at the cued location was entirely driven by the longer 2 cue-target delays (500 and 800 mseconds). Thus, the main impact of training appeared to be abolishment of the inhibition of return phase of SDA.
Altogether, these data suggest that our attention training protocol reduced the impact of the stimulus-driven cue, especially at longer cue-target delays. An alternative explanation is that participants voluntarily paid more attention to cues after training, sustaining attention at the cued location until target appearance.
We also observed significantly improved goal-directed attention after training, indexed by faster RTs. While this improvement in attention could be explained by a general practice effect, individual differences in RT changes in the goal-directed attention task related to anxiety changes (Fig. 5B), supporting the specific relationship of goal-directed attention changes to clinical benefit. Our attention training paradigm had no effect on TB. Thus, the training task seems to have reduced anxiety by reducing SDA, increasing goal-directed attention, or the combination.
The training program also decreased evoked activity in the rVLPFC CON area during an SDA task. Residual task-evoked activity in this region was related to residual (post-training) anxiety, supporting the interpretation that downregulation of this activity underlies successful anxiety treatment. The CON is involved in executive functions and demonstrates transient activity increases following salient stimuli and errors (Dosenbach et al., 2007). Alterations in CON activity have consistently been linked to psychiatric illnesses in meta-analyses, with CON regions thought to be overactive in anxiety disorders (Cocchi et al., 2012; Liao et al., 2010; McTeague et al., 2017). In our prior work, resting-state functional CON/VAN connectivity was linked to both SDA and anxiety severity in children with and without anxiety disorders (Perino et al., 2021a). Thus, the literature is consistent with our current observations that reducing CON activity supports anxiety reduction.
Contrary to our hypothesis, we did not detect decreased activity in the rVLPFC VAN area following training. Possible explanations include the following: (1) the training program induces greater changes in executive function networks (i.e., the CON) compared with attention networks (i.e, the VAN), (2) we lacked sufficient power in this pilot study to detect VAN activity changes, and (3) the brain area in which we detected training-related activity decreases actually corresponds to what has been called the VAN in some prior work despite its label as CON in our network scheme (Gordon et al., 2016). To adjudicate this last possibility, further work is needed to link activity elicited by classic attention paradigms (Corbetta and Shulman, 2002; Corbetta et al., 2008) to modern, resting-state-based network classification schemes (Gordon et al., 2016; Power et al., 2011; Yeo et al., 2011).
An important limitation of the present study is the lack of a control group, preventing exclusion of unrelated factors contributing to anxiety reductions. This concern is partially mitigated by the findings that individual differences in SDA and goal-directed attention changes were related to individual differences in anxiety improvement, but future work should incorporate a control arm. This is a small, pilot clinical trial with 18 patients, 12 of whom completed neuroimaging. This sample size provides limited power to detect subtle changes. We present uncorrected statistical results in this exploratory analysis to generate hypotheses for more stringent testing in larger studies. The presence of significant results in this limited sample supports expanded clinical trials based on this paradigm.
Conclusions
In this pilot clinical trial, a novel cognitive training intervention reduced pediatric anxiety, altered SDA, increased goal-directed attention, and reduced activity in an rVLPFC CON area. Individual differences in attention and neural changes were associated with differences in anxiety improvement. This training paradigm was designed to reduce SDA. Its success supports the hypothesis that SDA is a suitable treatment target in pediatric anxiety disorders (Lazarov and Bar-Haim, 2021; Meyer et al., 2020; Waters et al., 2015). Future work with larger samples and control subjects is required to further explore this promising treatment approach.
Clinical Significance
Pediatric anxiety disorders may be associated with increased involuntary capture of attention by salient stimuli coupled with increased activity in brain regions underlying this process. Patient anxiety significantly improved after receiving cognitive training designed to reduce this involuntary attention capture and associated neural activity. Anxiety improvements related to changes in attention and attention-relevant neural circuitry.
Footnotes
Authors' Contributions
A.T.D.: conceptualization, formal analysis, writing—original draft, and visualization. M.J.M.: data curation, software, and visualization. J.C.H.: methodology and investigation. M.G.: visualization. M.M.: methodology and investigation. Q.Y.: methodology and software. M.T.P.: validation and writing—review and editing. J.L.L.: writing—review and editing and supervision. D.M.B.: writing—review and editing and supervision. D.S.P.: conceptualization, writing—review and editing, supervision, and funding acquisition. C.M.S.: conceptualization, methodology, resources, supervision, writing—review and editing, and funding acquisition.
Disclosures
No competing financial interests noted by any authors.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.