
Abstract
Objectives:
This study aimed to examine the association between abnormal readings of metabolic parameters detected during second-generation antipsychotic (SGA) treatment and the likelihood of receiving subsequent adverse drug event interventions.
Methods:
This was a nested case–control study conducted on patients 1–17 years of age with at least two prescriptions of SGAs between January 2010 and January 2019 using TriNetX EMR data. Following an incident density sampling procedure, patients who received the SGA metabolic adverse event intervention (mAEI) (case) were matched with three nonrecipients (controls). The abnormal readings of metabolic parameters within 30 days before the initiation of mAIEs were further identified. These metabolic parameters include body mass index (BMI) and laboratory parameters such as cholesterol, high-density lipoprotein, low-density lipoprotein, triglycerides, blood glucose, HbA1c, thyroid hormones, liver enzymes, and prolactin. The association of abnormal metabolic parameters with subsequent mAEIs was assessed using a conditional logistic regression model, after adjusting for demographic and other clinical risk factors.
Results:
One thousand eight hundred eighty-four children and adolescents met the inclusion criteria and were prescribed SGA mAEIs. The most common types of mAEIs prescribed were weight management pharmacotherapy (40.6%), switching from a high or medium metabolic risk profile SGA to a low-risk one (30.9%), nonpharmacological treatment (25.4%), and switching from SGA polytherapy to monotherapy (11.7%). The conditional logistic regression analysis on matched mAEI recipients and nonrecipients showed that patients with an abnormal BMI had 43% higher odds of receiving mAEI (odds ratio [95% confidence interval]: 1.43 [1.13–1.79]). However, the presence of an abnormal laboratory reading was not associated with the initiation of mAEIs.
Conclusions:
The prescribing of mAEIs were associated with the presence of obesity, but not with abnormal readings of other metabolic parameters, suggesting that additional data are needed to clarify the long-term implication of SGA metabolic adverse events other than weight gain and to inform the appropriate timing for interventions.
Background
A diverse array of side effects has been associated with second-generation antipsychotics (SGAs) (Carli et al., 2021; Libowitz and Nurmi, 2021; McIntyre and Jerrell, 2008; Pillinger et al., 2020). Other than antipsychotics-induced weight gain (AIWG) (Dayabandara et al., 2017), SGAs can disrupt glucose metabolism, induce dyslipidemia (Chaggar et al., 2011; Grajales et al., 2019), and cause asymptomatic elevation of liver enzymes (Atasoy et al., 2007), thyroid function disturbance (Vedal et al., 2018), and prolactin elevation (AACAP, 2011).
Due to concerns about SGA-associated side effects, the American Academy of Child and Adolescent Psychiatry (AACAP) practice parameter for the use of atypical antipsychotic medications in children and adolescents and the Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) recommend baseline and periodic monitoring of body mass index (BMI), blood glucose, and lipid profile (high-density lipoprotein [HDL], low-density lipoprotein [LDL], total cholesterol, and triglycerides) (AACAP, 2011). In addition, the CAMSEA guidelines also recommend monitoring for prolactin (baseline, annually, or with clinical symptoms), thyroid-stimulating hormones (TSH; baseline and annually only for quetiapine) and liver enzymes (baseline, semiannually, and annually) (Pringsheim et al., 2011).
In addition to the monitoring recommendation, CAMSEA also recommends management strategies for SGA-associated side effects (Ho et al., 2011). These interventions include nonpharmacological interventions such as behavioral counseling and lifestyle modifications, and pharmacological interventions that include adding a weight neutralizing agent, switching to a lower metabolic risk profile SGA, avoiding multitherapy, and tapering off SGA dose if feasible (Dayabhandara et al., 2017; Ho et al., 2011).
However, the guidelines do not provide a clear guidance on when these SGA adverse effect mitigating interventions should be initiated. A study by Morrato et al. (2009) found that the presence of abnormal metabolic parameters in adults on SGAs were not consistently associated with the selection of an SGA with lower metabolic risk. The association of the presence of abnormal metabolic parameters and the SGA metabolic adverse event interventions (mAEIs) in children and adolescents has not been examined.
The objective of our study was to characterize the mAEIs implemented during SGA treatment in children and adolescents and to examine the association of mAEIs (outcome) with the presence of abnormal metabolic parameters (exposure) using a national electronic medical records (EMR) database.
Methods
Data source
This study was conducted using the TriNetX EMR database from January 1, 2009, till January 31, 2019. This database includes 60 million patients from 50 large healthcare organizations in the United States. The health care organizations include a mixture of hospitals, primary care, and specialist providers and contribute data from insured and uninsured patients alike. The database records patient information such as detailed patient demographics, diagnoses, procedural information, vital signs, and laboratory test results. Medication list entries include their RxNorm codes and start dates. The database may include multiple data points, making it a rich source for longitudinal analyses. The database is de-identified in accordance with the Health Insurance Portability and Accountability Act and has been used widely in published literature (Firl et al., 2021; Freedman et al., 2021; Harrison et al., 2021 ; Harrison et al., 2020; Mukherjee et al., 2021; Sultan et al., 2021; Taquet et al., 2021).
Study population
Individuals who were 1–17 years of age and had at least two prescription orders of SGAs were identified from the TriNetX EMR database. The SGAs included were aripiprazole, asenapine, brexpiprazole, cariprazine, clozapine, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine, risperidone, and ziprasidone. To minimize the potential confounding effect of chronic SGA treatment, we used a new-user design. We defined the index SGA as the first SGA prescription patients received after a 6-month period without an SGA prescription order. Patients were excluded if they had <30-day SGA exposure or if they received a diagnosis of dyslipidemia, diabetes, or eating disorder at SGA initiation.
Because many SGA recipients were obese before SGA initiation, abnormal BMI detected during SGA treatment may simply be the continuation of baseline weight status. To understand how the weight status change could affect the downstream regimen adjustment, a subcohort, including patients who were not affected by obesity (n = 607) before SGA initiation, was also constructed. A child was defined as “not affected by obesity” if their body mass index-for-age (or BMI-for-age) percentile is <95%.
Study design
As presented in Figure 1, a nested case–control design was employed to assess the association of the presence of abnormal metabolic monitoring results with the receipt of mAEIs after controlling for other clinical and demographic factors.

Nested case–control (1:3 match) study design.
Cases
The mAEI recipients were defined as patients who received the first mAEI beyond 30 days after SGA initiation. The mAEIs included both nonpharmacotherapy treatments and pharmacotherapies. The nonpharmacotherapy comprised dietary interventions, obesity counseling, and psychotherapy. Pharmacological interventions consisted of weight management pharmacotherapy and SGA regimen adjustment, including switching from a high or medium metabolic profile SGA to a low metabolic risk profile SGA or switching from SGA polytherapy to monotherapy. SGAs such as aripiprazole, asenapine, lurasidone, and ziprasidone are considered having low metabolic risk (Carli et al., 2021; Pillinger et al., 2020). Thus, our definition of switching included switching from any other SGA to these four low-risk SGAs. Detailed diagnosis, procedural, and medication RX-Norm codes used to identify mAEIs are described in Supplementary Appendix Table SA1.
Case–control matching
The date of mAEI initiation was defined as the “event date.” Each mAEI recipient was matched at a 1:3 ratio with individuals who had not received an intervention by the case event date, using an incidence density sampling procedure (Grandits, 2010; Richarson, 2004). The incidence sampling procedure allows cases to serve as potential controls for other cases and to be matched based on their SGA follow-up duration, thus eliminating potential immortal time bias. For each matched case–control set, the event date of the case was assigned to the controls.
Observation period
Factors associated with the initiation of mAEIs were observed within a 30-day window before the event date.
Main risk factor
The main risk factor of interest was the presence of abnormal metabolic parameters within the 30-day observation period. According to the AACAP and CAMESA guidelines, the metabolic parameters considered were BMI and laboratory measures, including blood glucose, HbA1c, HDL cholesterol, LDL cholesterol, total cholesterol, triglycerides, liver enzymes, prolactin, and thyroid hormones. BMI was considered an independent measure, and all laboratory parameters were grouped under the measure “Labs.” Both measures (BMI and Labs) were categorized as normal, abnormal, or absent. Abnormal BMI was defined as ≥95 percentile of age- and gender-adjusted BMI values according to the CDC weight chart. Laboratory results were flagged as abnormal or normal according to standard pediatric guidelines (ADA, 2022; Mayo Clinic Laboratories, 2022; NHLBI, 2012; Whitelock et al., 2010). Detailed threshold cutoff values for normal and abnormal BMI and Labs are presented in Supplementary Appendix Tables SA2 and SA3.
Other potential risk factors
Other potential risk factors identified during the 30-day observation period were age, gender, race, SGAs used, use of multiple SGAs, mental disorder diagnoses including attention-deficit/hyperactivity disorder (ADHD), mood and depressive disorders, anxiety disorders, psychotic disorders, and schizophrenia, other mental health disorders, and comedications including antidepressants, psychostimulants, and α-2 agonists, mood stabilizers and anticonvulsants, benzodiazepines and other anxiolytics, and other psychotropic medications.
These factors were selected because literature has reported that gender, race, age group, and preexisting conditions are risk factors associated with SGA use and some of these risk factors can contribute to changes in treatment strategies such as antipsychotic switching or discontinuation (Fulone et al., 2021; Stroup and Gray, 2018). Age and gender could also modify the risk of some adverse drug events (ADEs) (e.g., QT prolongation) associated with SGAs (He et al., 2022). Mental health comorbidities may be associated with the degree of weight gain associated with SGAs (Doane et al., 2022). It has also been shown that concurrent use of SGAs with other psychotropic medication drug classes is associated with a higher risk for SGA-associated metabolic adverse effects (Burcu et al., 2017; Zhang et al., 2021).
Statistical analysis
Paired t-test was conducted to compare continuous variables and Cochran-Mantel-Hansel test was conducted to compare categorical variables between matched cases and controls. A conditional logistic regression model was fitted to determine the association between the presence of abnormal BMI or laboratory values and the initiation of mAEIs after controlling for other potential risk factors.
The study was approved by the institution review board of the University of Houston. All analysis was done using SAS 9.4 (NC).
Results
Incidence and subtypes of mAEIs
The cohort identification schematic is presented in Figure 2. There were 1884 patients who met inclusion criteria and received an mAEI at least 30 days after SGA initiation, of which 607 (32%) had a baseline BMI <95 percentile. The median time to mAEIs from SGA initiation was 64 (interquartile range: 44–98) days. The cohort characteristics are presented in the Supplementary Appendix Table SA4.
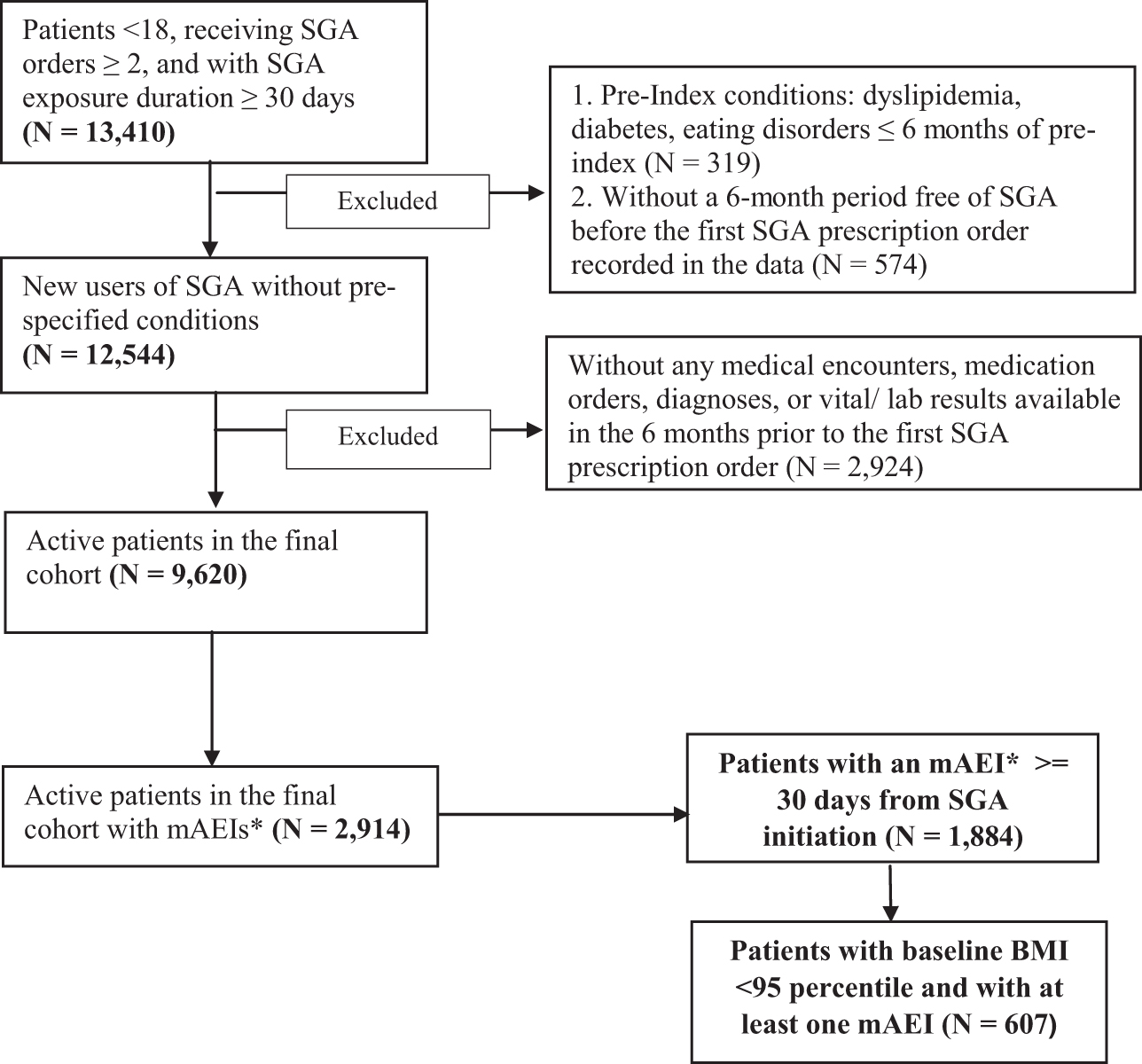
Schematic diagram for the identification of study cohort. *mAEI, SGA metabolic adverse event intervention. SGA, second-generation antipsychotic.
Table 1 presents the types of SGA mAEIs prescribed. In the full cohort, 40.55% of those initiated mAEIs were prescribed weight management pharmacotherapy, followed by switching from a high or medium metabolic profile SGA to a low metabolic profile (as described earlier) SGA (30.89%), adding nonpharmacotherapy treatment (25.37%), and switching from SGA polytherapy to monotherapy (11.73%). Among those prescribed weight management pharmacotherapy, 74% received adjuvant metformin. While in the subcohort of patients who were not affected by obesity, nonpharmacotherapy treatments (32.12%) were the second most common choice of MAEIs, following weight management pharmacotherapy (36.57%). The third most commonly prescribed mAEI was switching from high- or medium-risk profile SGAs to low-risk profile SGAs (27.18%).
Subtypes of Second-Generation Antipsychotic Metabolic Adverse Drug Event Interventions (Second-Generation Antipsychotic Metabolic Adverse Event Interventions)
Obesity counseling: obesity counseling identified through specific procedural (CPT) codes.
Weight management counseling diagnosis: dietary management and counseling identified through ICD diagnosis code Z71.3 (ICD-10 code).
BMI, body mass index; mAEI, metabolic adverse event intervention; SGA, second-generation antipsychotic.
Incidence and subtypes of SGA ADE monitoring
There were 1882 out of 1884 mAEI patients in the full cohort and 606 out of 607 mAEI patients in the subcohort were successfully matched with controls at a 1:3 ratio. Table 2 presents the monitoring frequency of SGA metabolic parameters in the matched event and control groups. During the 30-day period before the event date, less than half of the patients (41.92%) in the full cohort had BMI monitoring and only a fraction of patients (17.43%) had laboratory monitoring for SGA-associated ADEs. The most monitored laboratory parameters were liver enzymes (8.98%), followed by blood glucose (4.25%) and cholesterol (3.40%). Other metabolic parameters such as HbA1c, TSH, and prolactin were only monitored in a few patients.
Body Mass Index and Lab Monitoring Frequency
BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein; mAEI, metabolic adverse event intervention; SGA, second-generation antipsychotic; TSH, thyroid-stimulating hormones.
In the nonobese subcohort (BMI <95 percentile), almost two-thirds of the patients had BMI monitoring (72.28%) and only 13.70% of patients had any kind of laboratory monitoring. Among the laboratory parameters monitored, the most frequent were alanine aminotransferase (ALT) liver enzymes (6.27%), followed by blood glucose (3.47%) and cholesterol (3.14%).
Characteristics of matched cases and controls
The distribution for the main and other potential risk factors associated with mAIEs for the full cohort is presented in Table 3. The mAEI recipients had significantly higher BMI and laboratory monitoring rates compared with the matched controls (BMI: 41.92% vs. 21.19%, p < 0.001 and Labs: 17.43% vs. 12.9%, p < 0.001). The proportion of patients with abnormal BMI and laboratory reading was also significantly higher among the mAEI group (BMIabnormal: 10.52% vs. 4.04%; p < 0.001 and Lababnormal: 5.79% vs. 4.64%; p < 0.001) than that in the controls. Of children identified with abnormal Labs, 89.90% had elevated liver enzymes. The mean dysregulated Lab value for ALT liver enzyme was 72 U/L, which is 16–26 U/L points (34.7%–46.43%) above the threshold value. The mAIEs recipients also had higher usage of multiple SGAs (12.75% vs. 5.01%; p < 0.001), higher usage of psychotropic comedications such as antidepressants (30.02% vs. 20.84%; p < 0.001), psychostimulants and α-2 agonists (33.95% vs. 26.24%; p < 0.001), mood stabilizers and anticonvulsants (11.42% vs. 7.32%; p < 0.001), benzodiazepines, and other anxiolytics (8.71% vs. 6.25%; p = 0.003), and had more psychiatric comorbidities, including ADHD (36.93% vs. 23.33%; p < 0.001), mood and depressive orders (42.51% vs. 27.02%; p < 0.001), anxiety disorders (25.29% vs. 17.24%; p < 0.001), psychosis, and schizophrenia (6.32% vs. 3.38%; p < 0.001).
Distribution of Risk Factors Between Matched Metabolic Adverse Event Intervention Recipients and Nonrecipients in the Full Cohort
ADHD, attention-deficit/hyperactivity disorder; ALT, alanine aminotransferase; AST, aspartate transaminase; BMI, body mass index; CMH, Cochran-Mantel-Hansel; mAEI, metabolic adverse event intervention; PIs, Pacific Islanders; NAs, native Americans; SGA, second-generation antipsychotic.
The distribution for the main and other potential risk factors associated with mAIEs for the subcohort is presented in Table 4 Unlike the full cohort, statistically significant differences between mAEI recipients and matched controls were not observed in BMI monitoring rate. The proportion of patients who had abnormal BMI and Labs was also not statistically different between mAEI group (BMIabnormal: 6.11% vs. 4.46%; p = 0.1301 and Labsabnormal 3.96% vs. 3.91%; p = 0.5260) and matched non-mAEI group.
Distribution of Risk Factors Between Matched Metabolic Adverse Event Intervention Recipients and Nonrecipients in the Subcohort of Patients Not Affected by Obesity at Second-Generation Antipsychotic Initiation
ADHD, attention-deficit/hyperactivity disorder; ALT, alanine aminotransferase; AST, aspartate transaminase; BMI, body mass index; CMH, Cochran-Mantel-Hansel; mAEI, metabolic adverse event intervention; PIs, Pacific Islanders; NAs, native Americans; SGA, second-generation antipsychotic.
The association of BMI and lab monitoring results with the likelihood of receiving SGA mAEIs
The estimates for the risk factors associated with the likelihood of receiving SGA mAIEs from the conditional logistic regression analysis are presented in Table 5. In the full cohort, compared to patients with normal BMI, those with abnormal BMI had 40% higher odds of receiving mAEIs (odds ratio, OR [95% confidence interval, CI]: BMIabnormal vs. normal: 1.43 [1.13–1.79]), and those with absent BMI had 51% lower odds of receiving mAEIs (OR [95% CI]: BMIabsent vs. normal: 0.49 [0.43–0.57]).
Conditional Logistic Regression Results
p < 0.05-significant.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index; CI, confidence interval; NAs, native Americans; OR, odds ratio; PIs, Pacific Islanders; SGA, second-generation antipsychotic.
Having abnormal laboratory readings was not associated with the likelihood of receiving mAEIs (OR [95% CI]: Lababnormal vs. normal: 1.09 [0.81–1.47]). Other factors associated with the likelihood of receiving mAEIs included receiving SGAs associated with moderate metabolic risk (risperidone and quetiapine), multiple SGAs (≥2 different SGAs at index), mood stabilizers, and anticonvulsants and diagnosis of comorbid conditions such as ADHD, mood and depressive disorders, psychotic disorders, and schizophrenia, during the 30-day period before the event date.
The results of conditional logistic regression analysis on the subcohort of patients who were nonobese at the baseline (BMI <95 percentile) showed that having weight increase (BMI ≥95 percentile) or abnormal labs during SGA treatment was not associated with higher odds of receiving mAEIs compared to without (OR [95% CI]: BMIabnormal vs. normal: 1.13 [0.74–1.73] and Labsabnormal vs. normal: 1.30 [0.73–2.32]) (Table 5).
Discussion
The purpose of the study was to evaluate any association between abnormal metabolic parameters and the likelihood of receiving mAEIs. The principal finding of this study is that, as expected, abnormal BMI is an important factor associated with the initiation of mAEIs. Patients with an abnormal BMI value had 40% higher odds of receiving any interventions for SGA-induced metabolic adverse effects (mAEIs) within 30 days. AIWG is the most important adverse metabolic effect of SGAs, and it is evident in more than 80% of children during the first few months of SGA therapy (Dayabandara et al., 2017). AIWG can also impact the pathway of glucose dysregulation or cause lipid abnormalities and metabolic syndrome (Chaggar et al., 2011; Dayabandara et al., 2017; Grajales et al., 2019; Libowitz and Nurmi, 2021).
However, our findings also showed that a statistically significant association was not seen for the abnormal reading of other metabolic parameters and subsequent mAEIs. The descriptive statistics showed that although blood glucose and cholesterol were among the most commonly monitored metabolic parameters for pediatric SGA recipients, abnormal readings for these two parameters were rare. The most common abnormal reading for laboratory tests found in our study was liver enzymes. It is known that SGAs commonly cause asymptomatic elevation of liver enzymes such as ALT (Atasoy et al., 2007). Earlier literature has also shown that ∼20% of patients on SGAs have significantly higher elevated liver enzymes (Meiyanti et al., 2022), thus corroborating our findings.
In a prospective study conducted by Erdogan et al. (2008), it was found that 52.5% of children had clinically nonsignificant elevation of liver enzymes with risperidone usage. The elevation of liver enzymes was associated with the type of SGA use (more prone to increase with olanzapine and clozapine), duration of therapy, and combination of SGAs with psychotropic medications (Gonzalez-Heydrich et al., 2003; Meiyanti et al., 2022). LFT are recommended by CAMSEA guidelines in Canada; however, in the United States, there is no consensus for the treatment of abnormal liver function tests (ALT/aspartate transaminase), and not recommended by guidelines that explain the lack of association between elevated laboratory parameters and SGA mAEIs.
In addition, the findings of the subgroup analysis showed that, for patients with abnormal BMI, physicians might not consider mAIEs when the abnormality was newly detected. In the subgroup analysis on patients who were not affected by obesity before SGA initiation, a significant association between abnormal BMI during SGA treatment and subsequent mAIEs was not detected. The finding is different from the results of the main analysis, implying that there might be competing priorities, such as the effectiveness of the treatment, making prescribers decide not to intervene in the ADE immediately.
Another interesting finding is that patients had 50% lower odds of receiving mAEIs when BMI was not monitored compared to those who had a normal BMI measure during SGA treatment. This could be because having any BMI measure may imply that patients had a follow-up visit in which some other changes in the patient's condition have led to the decision to prescribe an mAEI. There might also be a possibility that patients who did not have BMI measurements were likely to have clinicians who did not consider evaluating and managing AIWG. It is important to point out that some mAEIs, such as switching from SGA polypharmacy to monotherapy and prescribing a comedication with weight loss potential, may not necessarily be due to the concern on SGA-associated metabolic side effects. It could be a regimen adjustment due to the improvement of patients' psychiatric symptoms.
Among those who received the mAEIs, the descriptive statistics showed that the selection of interventions for metabolic side effects was mostly evidence based and guideline concordant. For instance, metformin has the most evidence of efficacy among the different interventions to counter AIWG (De Hert et al., 2011). Our results showed metformin was the most prescribed pharmacological mAEIs. The IMPACT Trial showed that switching to a lower risk SGA is as effective as adding metformin (Correll et al., 2020). Our findings revealed that switching to a lower risk SGA was the next commonly prescribed mAEIs. Nonpharmacological strategies like behavioral interventions are often used as frontline therapy for AIWG (Dayabhandara et al., 2017). This was corroborated in our study that patients in the subcohort who were not affected by obesity at the baseline used more nonpharmacotherapy compared to the full cohort.
This large national retrospective study is critically important because, to our knowledge, it is the first to evaluate the association of metabolic risk factors and receiving subsequent SGA mAEIs in children and adolescents. Our previous research has found that the SGA metabolic monitoring recommendation has been modestly followed. The findings of this study suggest that some monitoring recommendations, especially the laboratory monitoring for cholesterol and blood glucose, should be reconsidered, given the low risk of having abnormalities in the population and its limited impact on subsequent interventions.
Our study likely has several limitations. One inherent limitation is that prescriptions in an EMR database are tracked by medication orders/lists, not prescriptions filled at the pharmacy. There can be some misclassification of exposure if the patients were not filling or taking the prescriptions. Another limitation is that due to data unavailability, we were not able to capture certain ADE management strategies, such as dose reduction. In addition, the metabolic parameters captured could be both fasting and nonfasting due to incomplete fasting designation in the EMR dataset. However, perhaps the greatest limitation would be the lack of SGA effectiveness measure, which has prevented us from understanding how physicians made clinical decisions by weighing the risks and benefits of SGAs.
Conclusions
The prescribing of SGA metabolic ADE interventions was associated with the detection of abnormal BMI during the SGA treatment, but was not associated with abnormal Lab readings, which predominantly comprised abnormal liver function tests. The findings suggest that additional data are needed to clarify the long-term implication of SGA metabolic adverse events other than weight gain and to inform the appropriate timing for ADE interventions.
Clinical Significance
The findings of this EMR-based research on children and adolescents prescribed SGAs showed that having an abnormal BMI measure during SGA treatment was associated with a higher chance of receiving interventions for metabolic ADEs. However, a similar association was not found between abnormal lab results detected during the monitoring of SGA-associated metabolic ADEs and the ADE interventions. The findings indicate that more data is needed to help clinicians understand the long-term implications of abnormalities other than weight gain detected during SGA metabolic monitoring and to inform appropriate timing for the ADE intervention in children and adolescents.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Table SA4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.