
Abstract
Introduction:
Major depressive disorder (MDD) is a primary risk factor for suicide, which is one of the leading causes of death among adolescents worldwide. Understanding the heterogeneity of suicidality in adolescents with MDD is critical for suicide prevention and intervention discovery. Quantitative electroencephalography (EEG) is a promising tool to address the knowledge gaps related to the neurophysiological characteristics of depression and suicidality. This study sought to examine resting-state EEG coherence differences in adolescents with MDD and suicidal ideation (SI)/behaviors (SB) and healthy controls (HC) to assess the utility of coherence as a biomarker of suicide.
Methods:
Twenty-six adolescents with MDD who were hospitalized for suicidality and 30 HC were recruited. The clinical sample was divided into SI (n = 9) and SB (n = 19) subgroups. Eyes closed resting-state EEG were recorded, and coherence was calculated. Depression severity and suicidality were assessed with the Children's Depression Rating Scale Revised and the Columbia Suicide Severity Rating Scale, respectively.
Results:
There were intrahemispheric differences in the right hemisphere across multiple electrode pairs. Delta, alpha, and beta coherence were higher in the SB group over the right prefrontofrontal and left parietooccipital electrode pairs, while alpha coherence was higher in the HC group over the right centroparietal electrode pair. There were no significant differences between HC and SI groups in any electrode pair.
Conclusions:
Patients with recent SB showed increased coherence in right frontal regions compared with patients with SI, suggesting altered cognitive states between those with SB and SI. These findings may have implications for suicide prevention in adolescents and could serve as useful biomarkers in clinical settings, but larger studies are needed to confirm the results.
Introduction
One in seven children between the ages of 10 and 19 have a mental disorder. Worldwide, depression and anxiety are the leading contributors of functional impairment among adolescents (WHO, 2022). Major depressive disorder (MDD) is a primary risk factor for suicide, which is the fourth leading cause of death for those between 15 and 19 years of age globally, and the second leading cause of death for people between 10 and 14 years of age in the United States (Angst, 1999; CDC, 2020; WHO, 2022). Understanding the heterogeneity of suicidality in adolescents with MDD is critical for suicide prevention efforts and intervention discovery (Khan, 1987). A myriad of factors likely contribute to this heterogeneity, from including social determinants like sex and race of health, to cognitive functioning, and affective states (Esposito et al., 2003; Miranda-Mendizabal et al., 2019; Rudd, 2006; Xiao and Lindsey, 2021). There is ongoing work in parsing the heterogeneity of suicide using clinical measures, neuroimaging data, and genotyping (Buch and Liston, 2021; Ginley and Bagge, 2017). However, there is a paucity of knowledge and data to guide these efforts.
Quantitative electroencephalography (qEEG) is a promising tool to address the knowledge gaps related to the neurophysiological characteristics of depression and suicidality. qEEG has shown early potential as a diagnostic biomarker in MDD, but sample sizes have not been large enough to evaluate its utility in differentiating variations of MDD, including those with predominant anxiety, irritability, or anhedonia (Olbrich and Arns, 2013; Widge et al., 2019). Resting-state qEEG offers easily translatable clinical utility since it is a baseline neurophysiology measure that is accessible in clinical practice. One of these neurophysiological measures is coherence, the similarity of the signal between two electroencephalography (EEG) electrodes, which assesses intra and interhemispheric functional connectivity across the frequency spectrums. Coherence can also be considered as an indicator of neural efficiency where lower coherence is indicative of better neuronal performance since a smaller amount and more localized cortical activity is required for the given task (Achard and Bullmore, 2007; Bowyer, 2016).
Coherence assessed with EEG may have a role as an accessible index of cognitive effects of adverse environments and states across various neurological and psychiatric disorders (Marshall et al., 2008; Murias et al., 2007; Rodinskaia et al., 2022). Careful considerations about the neurobiology of the disorders and how they map onto symptoms must be considered when using coherence as a biomarker.
Within the context of suicide, coherence measures may guide efforts to understand the heterogeneity of suicidality that is more accessible to patients and health care providers. Prior functional Magnetic Resonance Imaging literature suggests that there are functional connectivity differences between suicidal and nonsuicidal depressed populations (Schmaal et al., 2020). These differences have also been identified in depressed young populations with suicide attempts, where attempters were observed to have reduced connectivity between prefrontal and parietal regions compared with depressed youth without suicide attempts and controls (Cao et al., 2021). EEG coherence maybe a more accessible and scalable method for examining connectivity differences to assess suicide risk in busy clinical environments. However, there are only few studies that looked at EEG coherence in suicidal teens. In a study of teens at risk of suicide, Jeong et al. (2021) found various changes in both intra and interhemispheric coherence decreased during a working memory task in teens that attended a 6-week aerobic exercise course compared with controls.
This study investigated the resting-state EEG coherence differences in adolescents with MDD and suicidal ideation (SI), suicidal behaviors (SB), and healthy controls (HC) to assess the utility of coherence as a biomarker of suicide. We hypothesized that there would be intrahemispheric and interhemispheric coherence differences between depressed adolescents with SB compared with those with SI only and HC. In line with previous findings, we specifically hypothesized that there would be left intrahemispheric differences in prefrontoparietal coherence between patients with SB and others.
Materials and Methods
Participants
Thirty adolescents admitted to an inpatient psychiatry unit with SI and SB as determined by the Columbia Suicide Severity Rating Scale (C-SSRS) and thirty with no prior psychiatric diagnoses were recruited. All patients were diagnosed with MDD using the children's Mini International Neuropsychiatric Interview (MINI-KID) conducted by a trained physician (Sheehan et al., 2010). Depression severity was measured using the Children's Depression Rating Scale Revised (CDRS-R). Anxiety was measured using the Pediatric Anxiety Rating Scale (PARS). The CDRS-R, C-SSRS, and PARS are clinician assessment rating scales that show good interval consistency and validity in the adolescent population (Mayes et al., 2010; Posner et al., 2011; The Research Units on Pediatric Psychopharmacology Anxiety Study Group, 2002). Three patients and two controls dropped out of the study before completing EEG recordings. The inpatient group was further divided into two subgroups, those with SI (n = 9) or SB (n = 17) based on the C-SSRS assessment. Analysis of Covariance (ANCOVA) models were used to test if intra- and interhemispheric coherence differed among the groups controlled for age and sex.
Bonferroni correction was used for post hoc comparisons. Patients were allowed to be on psychotropic mediations, except for stimulants, which were held on the day of EEG assessments. The study was approved by the institution's Review Board (IRB: 18-003340), all research activity was conducted according to the Declaration of Helsinki and Good Clinical Practice and Human Subjects Protection guidelines.
EEG processing
Resting-state EEG was recorded in two interleaved 3-minute eyes-closed and eye-open periods using the MagStim-EGI Hydrocel 64 channel saline-based system at 1000 Hz sampling rate. Data were processed in EEGLab version 2022.1, using MATLAB version 2020a (Delorme and Makeig, 2004). The eyes-closed sessions were then combined for coherence analysis. Data were then offline filtered with a bandpass filter of 0.1–70 Hz with a 60 Hz notch filter, then divided into 10-second-long epochs. Epochs that contained large artifacts of amplitudes greater than 100 μVs were automatically rejected using the TBT toolbox (Ben-Shachar, 2018).
Coherence calculations
The coherence analysis was performed using a proprietary semiautomatic tool we have created that can calculate the power spectral density (PSD) and coherence measures for each individual in the study. This tool enables users to review and verify EEG segments before calculating the PSD and coherence measures. By default, the tool analyzes segments that are 2 seconds long and automatically detects segments with eye movement using data from six EEG channels that have been filtered for clinical review. To ensure accuracy, the EEG data for each participant was reviewed in a semiautomated process that involved both clinician review and automated removal of segments containing artifacts. Once the review process was complete, the PSD and coherence were calculated for EEG channels, Fp1-F7, F7-T7, T7-P7, P7-O1, Fp2-F8, F8-T8, T8-P8, P8-O2, Fp1-F3, F3-C3, C3-P3, P3-O1, Fp2-F4, F4-C4, C4-P4, P4-O2, Fz-Cz, and Pz-Cz at the Delta (0.5–4 Hz), Theta (4–8 Hz), Alpha (8–12 Hz), and Beta (12–20 Hz) frequency bands.
EEG coherence is a measure of connectivity that reflects the consistency of the phase relationship between two surface EEG signals. It is calculated in the frequency domain and is normalized to represent the functional coupling between signals at any given frequency. To calculate coherence between two time-domain signals x and y, we first compute the autocorrelation and cross-correlation of the signals to obtain the PSD of x and y, and the Cross-PSD, respectively, as a function of frequency. Coherence is then calculated by taking the square of the absolute value of the cross-spectral density divided by the product of the individual power spectra of the two signals, demonstrated in the formula
See Supplementary Data for further details of calculations above.
Results
Table 1 shows the demographics, the average CDRS-R, C-SSRS, and PARS scores and the medication use at EEG recording. Seven out of 9 in the SI group, and 14 out of the SB group were on antidepressants at the time of EEG recording. The type of antidepressants used and comorbid diagnoses is as determined by MINI KID described in Table 2.
Age, Sex, Children's Depression Rating Scale Revised and Columbia-Suicide Severity Rating Scale Scores of the Sample
ANOVA, Analysis of Variance; CDRS-R, Children's Depression Rating Scale-Revised; C-SSRS, Columbia Suicide Severity Rating Scale; HC, healthy control; NA, not applicable; PARS, Pediatric Anxiety Rating Scale; SB, suicidal behavior; SD, standard deviation; SI, suicidal ideation.
Comorbid Diagnoses and Medication Use in the Clinical Samples
ADHD, attention-deficit/hyperactivity disorder; GAD, generalized anxiety disorder; SAD, social anxiety disorder; PTSD, posttraumatic stress disorder; SNRI, selective norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; SB, suicidal behavior; SI, suicidal ideation.
There were no participant group effects in left intrahemispheric frontoparietal coherence as this pair (F3-P3) was above significance level (p > 0.05). This was the opposite of what had been hypothesized. Instead, we found extensive intrahemispheric differences in the right hemisphere, in prefrontofrontal (Fp2-F4), centroparietal (C4, P4), temporoparietal (T8-P8) electrode pairs, as well as the left parietooccipital (P7-O1) electrode pair. Table 3 shows the ANCOVA results in each frequency band where there was a significant effect of the participant group. Table 4 shows the results of Bonferroni corrected post hoc comparisons conducted.
Analysis of Covariance Results of Electroencephalography Coherence Across Suicidal Behavior, Suicidal Ideation, and Healthy Controls with Age and Sex as Covariates
Denotes statistical significance.
Bonferroni Corrected Post Hoc Comparisons Across Suicidal Behavior, Suicidal Ideation, and Healthy Control Groups
Denotes statistical significance.
HC, healthy control; SB, suicidal behavior; SI, suicidal ideation.
Delta, alpha, and beta coherence over the right prefrontofrontal electrode pair (Fp2-F4), and delta coherence over the left parietooccipital electrode pair (P7-01) were higher in the SB group compared with the SI group. Alpha coherence over the right centroparietal electrode pair (C4-P4) was higher in the HC group compared with the SB group. The group effect observed in the beta band of this pair rose above the significance level when corrected for multiple comparisons. Similarly, theta, alpha, and beta coherence over the right temporoparietal electrode pair (T8-P8) was higher in the HC group compared with the SB group. A significant effect of sex in the theta coherence over this region was also observed. A pairwise comparison showed that males (mean = 0.879, standard deviation [SD] = 0.054) had higher coherence at this electrode pair compared with females (mean = 0.820, SD = 0.088), (mean difference = 0.066, standard error = 0.026, p = 0.014). There were no significant differences observed between the HC and SI groups in any electrode pair. Electrode pairs with significant coherence differences are demonstrated in Figure 1.
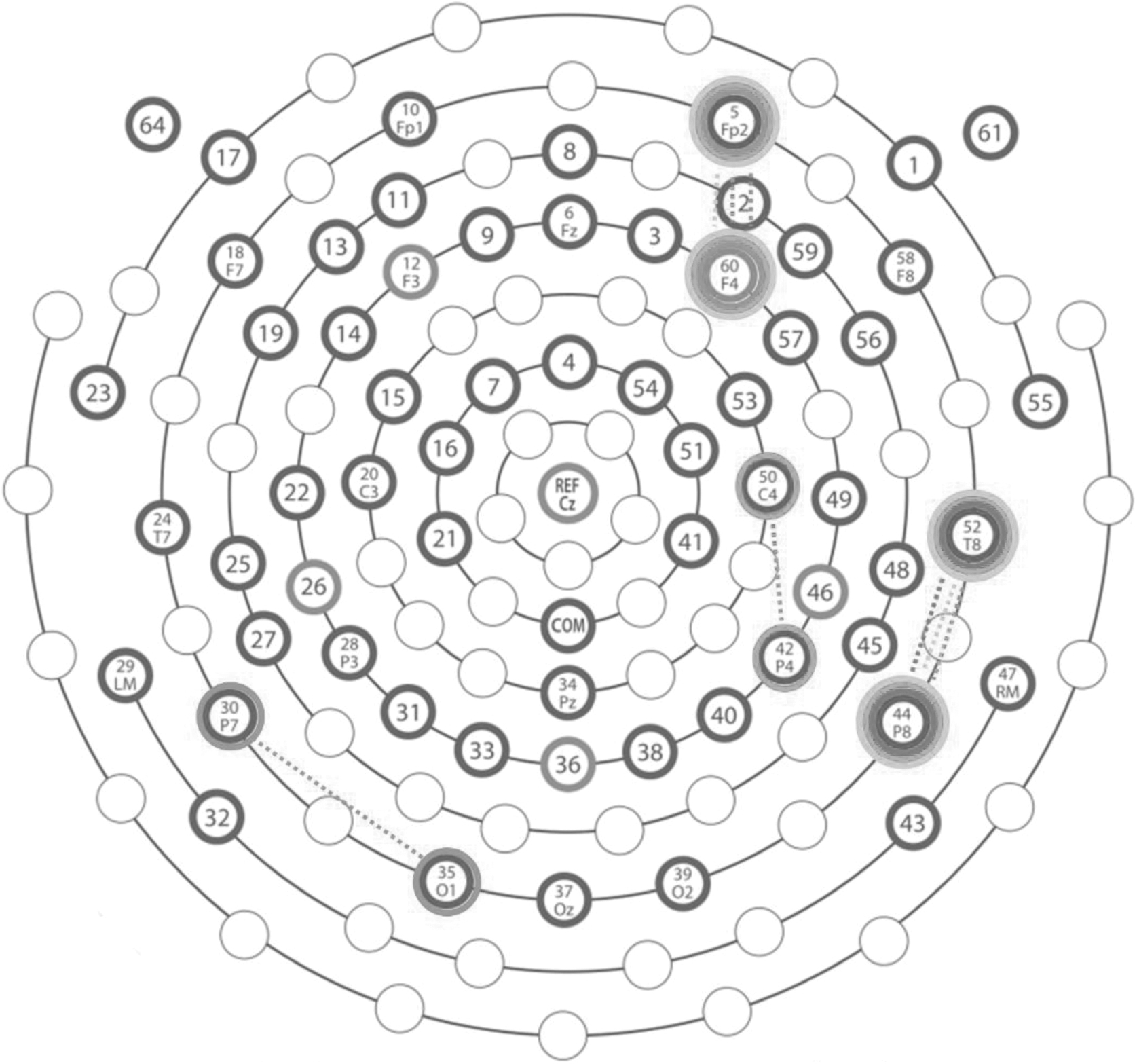
Electrode pairs with significant coherence differences across Delta, Theta, Alpha, and Beta bands. Frequency bands are denoted from darkest to lightest as Delta, Theta, Alpha and Beta respectively.
As expected, depression and anxiety severity were significantly higher in both the SB and SI groups compared with the control group (statistics reported in Table 1). Depression symptom severity, suicidality severity in the last 2 weeks before study participation, and anxiety severity (assessed with CDRS-R, C-SSRS, and PARS, respectively) did not differ between SB and SI groups (p > 0.05).
Discussion
Contrary to our hypothesis, we found no frontal intrahemispheric coherence differences in the left hemisphere between the groups. In addition, no interhemispheric coherence differences were identified. However, we found robust prefrontofrontal and temporoparietal intrahemispheric coherence differences in the right hemisphere. Overall, HC showed higher coherence values, followed by patients with SB and patients with SI at each significant difference.
Frontal differences in coherence
Right intrahemispheric prefrontal coherence between the Fp2 and F4 electrodes differed between the SB and SI groups. Given that these groups were comparable in depression and suicidality severity, it is possible that the increased coherence of the SB group is indicative of SB. This is a promising finding that marks increased coherence as a potential predictor of suicide risk. Due to the limited spatial resolution of EEG, it is difficult to ascribe these findings to specific cortical regions and cognitive or affective systems that may underlie SB. However, this finding is in line with the previously observed Default Mode Network differences found in similar populations (Cao et al., 2021; Ho et al., 2021; Zhang et al., 2016). In addition, it is coherent with previous findings of increased right hemispheric activity in adolescent with SB measured by qEEG (Park et al., 2019). While alpha asymmetry is a widely studied qEEG measure of this kind, we have found that the difference was across a broad range of frequencies, from delta to beta range. Hence, it is likely that this is indicative of a generalized reduced neural efficiency and connectivity of the right hemisphere in the SB group.
Interestingly, there was no theta coherence difference observed in this electrode pair. Previously, Lee et al. (2017) demonstrated that theta band power correlates with SI. The SI and SB groups had comparable C-SSRS scores, which may be reflected as similar levels of theta coherence. It is possible that other frequency bands may distinguish between SI and SB.
The current literature on suicide and coherence is sparse, and future work should further investigate the predictive power of this measure in clinical settings. Given the urgent need for suicide prevention, right frontal coherence should be considered as a biomarker for suicidality in depressed adolescents. qEEG biomarkers are also proposed to be response predictors for neuromodulation treatments, and the area observed to have higher coherence is a treatment target for accelerated neuromodulation treatments (Watts et al., 2022). Future work should examine if frontal EEG coherence can also be investigated as a prognostic biomarker of rapid neuromodulation interventions for suicidality.
Temporoparietal differences in coherence
Right intrahemispheric temporoparietal coherence between the T8 and P8 electrodes differed between the HC and SB groups. Previous work by our group did not find significant coherence differences in this electrode pair when comparing depressed adolescents with HC (McVoy et al., 2022). In this previous study only 12% of the depressed sample suffered from SI. The observation of coherence differences in the T8-P8 pair may mean that temporoparietal coherence is more linked to suicidality than depression.
Centroparietal and parietooccipital coherence differences
We have also found higher centroparietal alpha coherence in the SB group compared with the HC group on the right hemisphere. While beta band also showed an effect, the significance disappeared after correcting for multiple comparisons. Because of the spatial resolution limitations of EEG, it is difficult to discern if this centroparietal coherence is indicative of a separate cerebral function regarding SB, or if it is a part of the robust coherence differences in the temporoparietal electrode pair.
Another study found left parietooccipital coherence differences in the P3-O1 pair between depressed adolescents and controls (McVoy et al., 2019). Here we found a delta band difference between the SI and SB groups at the P7-O1 pair. This coherence measure should also be considered as a differentiator of SB and SI in the future.
Lack of observed differences in SI group and sex effect on temporoparietal theta coherence
We did not observe any coherence differences between the HC and SI groups. One possible explanation is that the neural correlates of SB are stronger than ideations only since they indicate impacts on the circuitries of inhibition and impulsivity. Alternatively, it may be that the relationship between HC, those with SI and with SB is not linear. Coherence may be higher in healthy individuals compared with the depressed group with SI, but may increase again among those who escalate ideations to behaviors due to underlying cognitive deficits. Coherence has been demonstrated as an indicator of cognitive compensatory mechanisms in difficult tasks among teens at risk for suicide (Jeong et al., 2021). Another explanation is the limitation of the smaller sample size of the SI group. We may not have had enough participants to identify the coherence differences of SI only.
We also observed an effect of sex solely in the right temporoparietal theta band coherence. This deserves further investigation, as we had a sample of mostly females, and sex-based qEEG differences have been reported in depressed populations (Orgo et al., 2016).
Limitations
Although anxiety severity was examined as a potential confounder, the present study is limited by a small sample size and the particularly small sample size for the group of adolescents with SI, which limits our ability to detect potential smaller differences between the groups and test for the confounding factors such as the presence of anxiety disorders, and attention-deficit/hyperactivity disorder. In addition, we do not have a control group of patients with MDD, but no SI. Due to the suicide severity and inpatient status of the patients, most were on psychotropic medications, and majority of these patients had medication changes in the past 6 weeks, which may alter EEG measures.
Conclusions
Patients with SB had increased delta, alpha, and beta band coherence on the right prefrontal and frontal electrode pair compared with patients with SI. They also had lower coherence at the theta, alpha, and beta bands of the right temporal and parietal electrode pair compared with HC. These results may suggest altered default mode network and inhibitory mechanisms in patients with recent SB as compared with patients with SI. These coherence measures may be useful biomarkers of SB in clinical populations and aid suicide prevention in adolescents. For example, cortical areas with decreased coherence can serve as target sites for investigational neuromodulation interventions to improve outcomes. Given the paucity of information in this area, further research is needed to replicate the results in larger sample sizes. Future studies should utilize change in coherence as a measure of target engagement for various brain stimulation modalities.
Clinical Significance
EEG coherence may be a prognostic biomarker for suicide risk in adolescents with MDD. Adolescents with SB showed higher right frontal coherence compared with adolescents with ideations. Further research is required to confirm the clinical utility of abnormal coherence. If confirmed, coherence may be an accessible and low-cost biomarker to enhance suicide prevention and intervention.
Footnotes
Acknowledgments
The sources of funding for this study had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article, and in the decision to publish the results.
Authors' Contributions
D.D.C. and P.E.C. conceptualized and designed the study. D.D.C., P.E.C., and C.O. performed data collection and assessments. D.D.C., C.O., and S.C. developed the EEG data processing and analyses. C.O. constructed the initial draft of the article. D.D.C., C.O., S.C., M.M., and P.E.C. edited and assisted with revising the following versions of the article. The final version of the article has been read and approved by all authors.
Disclaimer
The content of this publication is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosures
P.E.C. has received research grant support from Mayo Foundation for Education and Research, Neuronetics, Inc.; NeoSync, Inc.; NSF, NIMH, and Pfizer, Inc. He has received grant-in-kind (equipment support for research studies) from Assurex; MagVenture, Inc; and Neuronetics, Inc. He has served as a consultant for Engrail Therapeutics, Myriad Neuroscience, Procter & Gamble, and Sunovion. The other authors have no disclosures or potential conflicts of interest.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.