
Abstract
Background:
Similar outcomes and remission rates have been found for the treatment of depression in adults in primary and psychiatric care settings. However, comparatively little is known about how pediatric depression is managed across different settings. This study aims to address this gap by comparing depression treatment in pediatric and psychiatric settings. We hypothesized that pediatric care settings would be more likely to treat individuals with lower depression severity and would select pharmacotherapy less frequently as a treatment option.
Methods:
Patients (n = 3498) were screened for depression at a children's hospital from May 2017 to May 2022 as part of the VitalSign6 project, a web-based application for depression management. The two-item patient health questionnaire (PHQ) was used for screening, and the data set contains patient-reported measures and provider-reported diagnoses and treatment selections at each clinic visit. Patients with nine-item PHQ (PHQ-9) scores ≥10 at baseline were included in the analysis to compare diagnosis and treatment recommendations between pediatric and psychiatric settings.
Results:
Among the 1323 patients who screened positive for depression, those in psychiatric settings had higher PHQ-9 scores (15.9 ± 5.0 vs. 12.1 ± 5.5; p < 0.0001). Patients with PHQ-9 ≥ 10 in psychiatric settings were more likely to be diagnosed with major depressive disorder (60.6% vs. 24.7%, p < 0.0001) and receive pharmacotherapy (54.8% vs. 6.6%) than those in pediatric settings. Pediatric setting patients were more likely to receive nonpharmacological treatment alone (36.3% vs. 4.3%) or an outside referral (27.7% vs. 5.7%). Remission rates did not significantly differ between the two settings.
Conclusions:
Youth in psychiatric settings are more likely to screen positive for depression and to have greater depression severity than those in pediatric settings. Both settings provide treatment recommendations for moderate-to-severe depression, but treatment types vary substantially. Yet, remission rates remain similar. Further research is needed to understand the nuances of treatment differences and their implications.
Introduction
Adolescent depression is a critical public health problem, with ∼20% of adolescents having a history of lifetime depression (Shorey et al., 2022). Depression in adolescents often goes unrecognized and untreated, leading to adverse outcomes such as suicidal behaviors or attempts (Wilkinson et al., 2011). Adolescents and their families are often reluctant to seek help from mental health professionals or do not have access to mental health care (Gould et al., 2004; Radez et al., 2021); thus, pediatricians and primary care providers are often the first places where symptoms of depression in youth may be identified.
Pediatric treatment guidelines recommend assessing for and treating depression in primary care settings (Zuckerbrot et al., 2018) and seeking help from mental health providers if the patient fails to improve (Cheung et al., 2018). Previous studies have examined the treatment of adolescent depression in primary care (Asarnow et al., 2005; Rushton et al., 2002; Stafford et al., 2020; Stein et al., 2006; Wells et al., 2012) and collaborative care models (Costello et al., 2021; Rapp et al., 2017; Richardson et al., 2014), but none have compared the diagnosis and treatment of depression in pediatrics versus psychiatric settings.
Previous research on adult populations found similarities in how depression is treated in primary care and psychiatric care settings. For example, the landmark STAR*D trial found that depression severity was similar in psychiatric and primary care settings (Gaynes et al., 2007) and that remission and response rates of depressed patients were also similar when identical care was provided (Gaynes et al., 2008). An observational study comparing depression treatment in psychiatric versus primary care settings also found similar rates of improvement in symptom severity and functioning (Simon et al., 2001).
Overall, these findings reinforce the proposition that, for the treatment of depression, primary care settings can be a good alternative to specialized care among adults. Extrapolating from the findings among the adult population, pediatric care guidelines recommend the provision of psychiatric care within primary care settings. However, existing literature provides little evidence that the findings from the adult population also hold true in the pediatric population. Given this shortage of evidence, it is currently unknown how treatment for depression in adolescents differs between pediatric and psychiatric care settings.
To begin addressing this gap in the literature, our study compared the outpatient psychiatric care provided in pediatric and psychiatric settings at a large urban pediatric medical center. The practices utilized a measurement-based care (MBC) application called VitalSign6 (Trivedi et al., 2019), a web-based software for screening patients for depression using the patient health questionnaire (PHQ). For patients with positive screenings, the program further assigns additional scales. During follow-up visits, it aids providers in monitoring symptoms and treatment planning based on MBC principles, which have demonstrated efficacy in depression treatment (Siniscalchi et al., 2020; Wang et al., 2022).
In this report, we leveraged the granular psychiatric care data available through VitalSign6 and compared the two types of care settings in the following respects: (1) the prevalence and sociodemographic features of patients who screened positive for depression, (2) the diagnosis received and the psychiatric treatment provided for those with moderate or greater depression, and (3) remission rates for those with moderate-to-severe depression severity.
Given the distinctive characteristics of depression in adolescents and considering the attitudes of both providers and families toward psychiatric diagnosis and treatment, we hypothesized that providers in pediatric settings would be more likely to treat individuals with lower depression severity and to select pharmacotherapy less frequently as a treatment option than providers in psychiatric settings.
Materials and Methods
This report is based on deidentified data obtained from 3498 patients who received treatment at a large urban children's hospital between May 2017 and May 2022 as a part of the VitalSign6 program evaluation project. The rationale, design, and implementation process of the VitalSign6 project have been detailed elsewhere (Trivedi et al., 2019). In brief, VitalSign6 is a point-of-care web-based application used to implement MBC practices. For each patient, the clinical staff created a profile in the application that included demographic information along with patient data from self-report clinical scales (completed on tablets or handheld devices) and providers' diagnostic assessment and treatment recommendations after a review of the patient self-report data and clinical evaluation.
The application was designed to assist with clinical decision making based on symptom severity, as well as symptom changes during treatment; data from VitalSign6 were integrated into the electronic health records of the clinical sites. Only data from this web-based application were analyzed for this report. The UT Southwestern Medical Center Institutional Review Board approved this study with a waiver of the need to obtain informed consent from individual patients.
Patients and clinical sites
Children and adolescents treated in various clinical settings at the children's hospital were included in this report. Psychiatric settings included the psychiatry outpatient clinic, foster care psychiatric services, substance use disorders program, and psychiatric day treatment program; nonpsychiatric settings included the cardiology clinic, solid organ transplant clinic, foster care clinic, and primary care clinics. Participating providers were physicians (psychiatrists and pediatricians), therapists, advanced nurse practitioners, and physician assistants.
Clinical measures
All clinical sites administered the two-item PHQ (PHQ-2) self-report screen for depression. This scale rates mood and anhedonia each with a 0–3 score for a total score range of 0–6. Those who scored >2 for PHQ-2 completed the PHQ-9 for further evaluation of depressive symptoms, as well as the generalized anxiety disorder (GAD-7) scale (Kroenke et al., 2003; Spitzer et al., 2006). The PHQ-9 is a nine-item self-report measure that evaluates the nine symptom domains for the Diagnostic and Statistical Manual 5th Edition (DSM-5; American Psychiatric Association 2013) major depressive episode (Kroenke et al., 2001).
Each PHQ-9 item is scored from 0–3, for a total score range of 0–27; scores of 0–4, 5–9, 10–14, 15–19, and 20–27 are considered minimal, mild, moderate, severe, and very severe symptom severity, respectively. Each GAD-7 item is scored from 0–3, giving a total score range of 0–21, with higher scores indicating worse symptoms (Hughes et al., 2021; Spitzer et al., 2006).
For patients who screened positive, clinicians were encouraged to conduct a DSM-5-based diagnostic interview by using a DSM-5-based checklist for major depressive disorder (MDD) within the VitalSign6 application. After the clinical interview, the application enabled providers to enter the depressive diagnoses (if applicable), which included MDD, persistent depressive disorder, unspecified depressive disorder, and adjustment disorder with depressed mood. Other psychiatric diagnoses included other psychiatric diagnoses (e.g., anxiety disorder, bipolar, attention-deficit/hyperactivity disorder), no psychiatric disorders, and unable to confirm (presence of or specific) psychiatric diagnosis.
Treatment selection
After the diagnostic assessment, providers were prompted to select one or more MBC tactics, including (1) MBC pharmacotherapy—an antidepressant medication is started after the initial diagnosis (the application provided an algorithm to assist with initial dose selection and follow-up visit dose adjustments based on clinical measures and self-report measures for side effects and adherence to medication regimen); (2) rescreen—symptom surveillance by the provider with plans to screen at future visits; (3) nonpharmacological treatment—this option includes monitoring of symptoms and incorporation of nonpharmacological treatment options such as individual or group psychotherapy, exercise, or behavioral activation; (4) refused treatment; (5) external referral—such as transfer of care to another provider within the clinical site or referral to psychiatry; and (6) no further follow-up is indicated.
Follow-up visits for those initiating depression treatment were recommended every 4 weeks but occurred based on the provider's preference and the patient's availability. Following depression treatment guidelines from the American Academy of Pediatrics and the American Psychiatric Association (Gelenberg et al., 2010; Zuckerbrot et al., 2018), the VitalSign6 algorithm suggested the options of starting either pharmacotherapy or evidence-based psychotherapy for those with PHQ-9 > 10. During subsequent follow-up visits, the algorithm provided recommendations regarding medication dosing changes if applicable. Remission was defined as having PHQ-9 < 5.
Statistical analysis
Data on continuous baseline characteristics were summarized as means with standard deviations and compared using Student's t-tests or one-way analysis of variance tests. Categorical variables were summarized as frequencies and percentages and were compared using chi-square tests. p-Values <0.05 were judged as statistically significant. When providers did not answer the diagnosis or treatment selection questions, we classified these missing variables “unknown/missing”; no imputations for missing data were conducted, as lack of entering decisions for these variables is a relevant outcome for these comparisons. All analyses were done using SAS 9.4 (SAS, Inc., Cary, NC).
Results
A total of 3498 children and adolescent patients were screened using VitalSign6 in the above-mentioned clinics. The sample was predominantly female (61.4%), White (58.6%), and non-Hispanic (63.1%). The mean age was 14.7 ± 2.1 years. Of the total sample, 1715 (49%) patients were screened in psychiatric settings and 1783 (51%) were screened in pediatric settings. There were significant differences in demographic characteristics between psychiatric and pediatric settings. Specifically, psychiatric settings had a higher frequency of female and White patients than pediatric settings, whereas the pediatric settings had a higher percentage of Hispanic patients than psychiatric settings (Table 1).
Baseline Characteristics of the Total Sample
N = 469 missing for race.
N = 102 had unknown ethnicity.
PHQ-2 screening
Of the total sample, 1323 (37.8%) patients had a positive screen for depression (Fig. 1). Within psychiatric settings, 50.7% (n = 870) of patients screened positive for depressive disorders, whereas 25.4% (n = 453) of patients in pediatric settings screened positive (χ 2 = 238.35, p < 0.0001). Patients who screened positive for depression had characteristics similar to those of the overall sample by treatment setting (Table 2). The mean age for those with a positive screen was 14.3 ± 1.9 years, with no statistical difference in age based on settings.
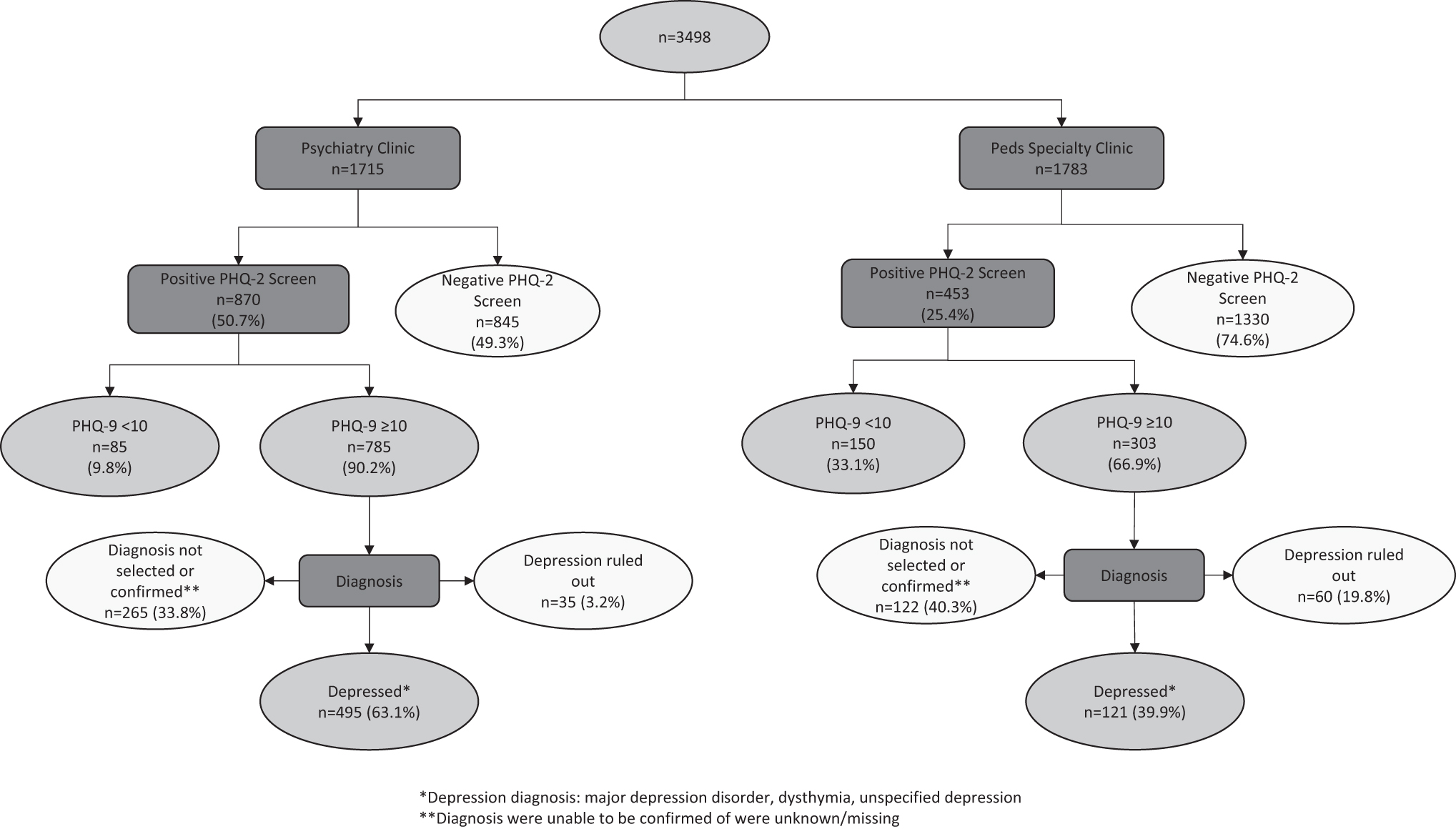
Flow of patients in psychiatric and pediatric settings. PHQ, patient health questionnaire.
Baseline Characteristics of PHQ-2 Screen-Positive Patients at Psychiatric and Pediatric Settings
All 1323 patients were given a PHQ-9, clinically assessed, and diagnosed by a provider.
Not all 1323 PHQ-2 screen-positive patients submitted demographic data for each category (per row).
PHQ-9 0–5: no depression, PHQ-9 6–9: mild depression, PHQ-9 10–14: moderate depression, PHQ-9 15–19: moderately severe depression, PHQ-9 20+: severe depression.
GAD-7, generalized anxiety disorder 7-item;
PHQ-9 scores
All patients who screened positive on the PHQ-2 were administered the PHQ-9 and GAD-7 as detailed above. The mean PHQ-9 score of those who screened positive was 14.6 ± 5.5 and the mean GAD-7 score was 11.8 ± 5.6. In the patients treated in the psychiatric settings, the mean PHQ-9 and GAD-7 scores were statistically higher than the patients treated in pediatric settings (PHQ-9: 15.9 ± 5.0 vs.12.1 ± 5.5, t = 12.69, p < 0.0001; GAD-7: 12.8 ± 5.2 vs. 10.0 ± 5.8, t = 8.52, p < 0.0001 for psychiatric vs. pediatric patients, respectively). Of the 870 patients who completed PHQ-9 in psychiatric settings, 90.3% (n = 785) had moderate/severe depression severity (total PHQ-9 ≥ 10), whereas in the pediatric settings, 66.9% (n = 303) of patients had moderate-to-severe depression severity.
Patients diagnosed with depression
All patients who screened positive and completed a PHQ-9 scale were clinically evaluated by a provider. Among 1088 youth scoring in the moderate or greater range (≥10) on the PHQ-9 (785 in psychiatric settings and 303 in pediatric settings), 551 (47.0%) were diagnosed with MDD; youth seen in psychiatric settings were more likely to be diagnosed with MDD than those in pediatric settings (60.6% vs. 24.7%; p = <0.0001; Table 3). In pediatric settings, 40.3% did not have a diagnosis (12.5% unable to confirm and 27.7% unknown/missing), whereas in psychiatric settings, 33.8% of patients did not have a diagnosis (all unknown/missing).
Diagnosis and Treatment Selection for Patients with a PHQ-9 ≥ 10
Excluded patients with an unknown diagnosis.
Supplementary Table S1 provides a breakdown of diagnoses based on PHQ-9 depression severity groups. For those with PHQ-9 score ≥15 (severe depression), 60.2% of patients in psychiatric settings were diagnosed with MDD, whereas only 35.9% of patients in pediatric settings were diagnosed with MDD. Of interest, over half of those seen in a psychiatric setting with a PHQ-9 score <10 received a depression diagnosis (MDD, dysthymia, or unspecified depressive disorder); this likely reflects that patients seen in these settings may have already been in treatment for depression and their scores may reflect improvement in symptoms.
Treatment selection
In psychiatric settings, of the 785 youth scoring in the moderate/severe depression range, 357 patients (45.5%) received combination treatment (MBC pharmacotherapy plus a nonpharmacological treatment option), 73 patients (9.3%) received only MBC pharmacological treatment, and 45 patients (5.7%) were referred to outside care. Only 34 patients (4.3%) received nonpharmacological only treatment options in psychiatric settings. In pediatric settings, 36.3% (n = 110) of patients in the moderate-to-severe range for depression severity received nonpharmacological treatments.
Only 11 patients (3.6%) had pharmacological treatment and 9 patients (3.0%) received combination treatment. The outside referral rate was 27.7% (n = 84) in pediatric settings. Around 30% of patients with moderate-to-severe depression had missing or unknown treatment data (33.2% in psychiatric settings and 24.4% in pediatric settings).
For those with PHQ-9 score ≥15, 54.5% of patients in psychiatric setting received pharmacological treatment, either alone or in combination with psychotherapy, whereas in pediatric settings, only 11.7% of patients with PHQ-9 ≥ 15 received pharmacological treatment (alone or combination), 26.9% of patients were referred to outside care, and 37.9% were provided nonpharmacological treatment. Just over 50% of youth scoring in the mild depression range in a psychiatric setting received pharmacological treatment (alone or in combination); as noted above, these patients may have already been in depression treatment at the time of screening into the VitalSign6 application. Supplementary Table S1 provides a breakdown of treatments based on PHQ-9 depression severity groups.
Remission rates
Among patients with moderate-to-severe depression, we examined remission rates for patients who had been enrolled for at least 4 months and who completed at least one follow-up visit. Of the 1088 patients with moderate-to-severe depression, 1045 had been enrolled for at least 4 months (764 in psychiatric clinics and 281 in pediatric clinics). In psychiatric settings, 42.3% (323/764) received at least one follow-up visit within 4 months, whereas only 21.4% (60/281) of patients in pediatric settings received a follow-up visit (p < 0.0001). For the patients who participated in 4 months of follow-ups with at least one follow-up visit, remission rates were not significantly different between psychiatric and pediatric settings (28.4% vs. 19.2%, respectively; χ 2 = 0.99, p = 0.32) (Fig. 2).
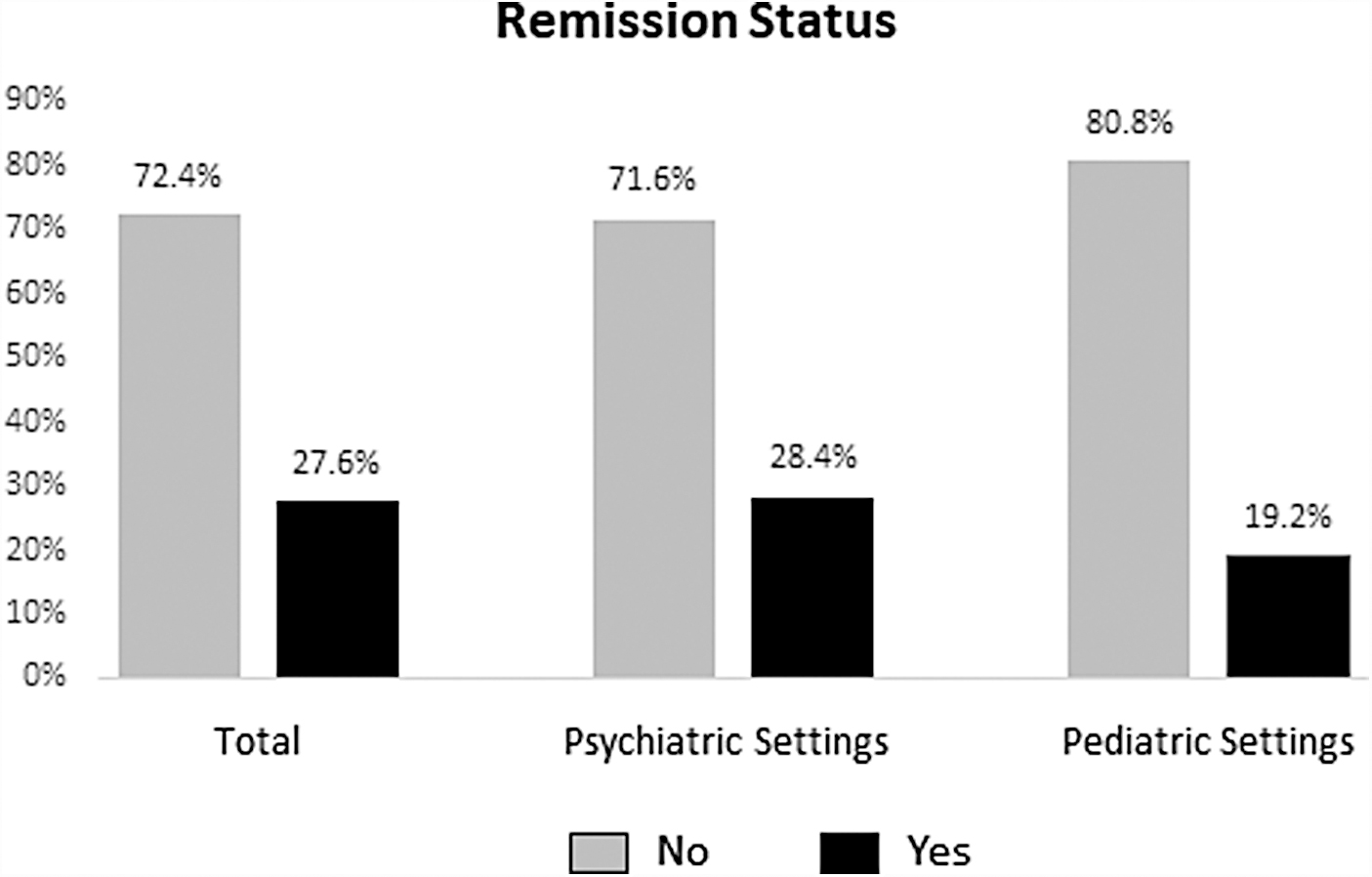
Remission outcomes of patients with ≥1 follow-up visits and 4 months enrollment. Remission = PHQ <5.
Discussion
This research examined youth screened for depression in psychiatric and pediatric treatment settings in a large urban children's hospital. Significant demographic differences were noted between the patients at the two treatment settings in this sample, with more White patients and females in the psychiatric settings and more Hispanic patients in the pediatric settings. Previous research has similarly shown that historically marginalized populations are less likely to receive psychiatric care than White patients (Kataoka et al., 2002), and are less likely to receive outpatient psychiatric care and prescriptions for psychiatric medication (Cook et al., 2013; Rodgers et al., 2022). Reluctance to seek professional help, perceived biases in the medical system, or socioeconomical factors such as lack of insurance may be barriers to seeking mental health treatment (Rickwood et al., 2007). Our results highlight the need for further understanding determinants of access in these populations.
The current sample has a higher frequency of PHQ-2 positive patients (total sample, 37.8%; 50.7% in psychiatric settings and 25.4% in non-psychiatric settings) compared to other VitalSign6 cohorts, which had 17%–18.4% PHQ-2 positive patients, primarily in community primary care settings (Jha et al., 2019; Wang et al., 2022). PHQ-2-positive patients, primarily in community primary care settings. This finding can be possibly explained by the treatment setting, a tertiary medical center treating patients with chronic medical or psychiatric problems as opposed to community care settings. Among patients with positive PHQ-2, those receiving care in psychiatric settings had significantly higher depression and anxiety total scores and were more likely to score in the moderate-to-severe range of depression than those receiving care in pediatric settings. These findings do not align with the literature in adult populations, as adult patients treated in nonpsychiatric settings had similar depression severity compared with those treated in psychiatric settings (Gaynes et al., 2007; Simon et al., 2001).
The variation in depression severity among adolescents in pediatric and psychiatric settings may be attributed, in part, to the treatment recommendations made by pediatric providers before data collection for this study. For instance, Radovic et al. (2014) conducted a study that examined how adolescent depression is treated in primary care settings. The study found that primary care providers were more likely to refer adolescents with severe depression to child psychiatry services than those with moderate depression. This discrepancy in the referral process may result in a higher likelihood of adolescents with severe depression being treated in psychiatric facilities, potentially contributing to the observed differences in depression severity between the two settings. Owing to the nature of the data collected by VitalSign6, we are unable to assess how often patients presenting to psychiatric care settings for treatment were referred by primary care physicians. Further study is needed to determine whether these differences are present in broader treatment settings.
In our sample, patients in psychiatric settings had higher rates of receiving a diagnosis of MDD than those in pediatric settings. Yet, although there were fewer depression diagnoses in the pediatric settings, in both settings, the majority of patients were given some type of treatment recommendation for their depressive symptoms. Patients in psychiatric settings were more likely to receive pharmacological treatment, with most receiving combination treatment (pharmacological combined with psychotherapy) compared with pediatric settings, where only 6.6% of patients received either pharmacological or combination treatment. Even with access to decision-aid tools such as VitalSign6, patients in pediatric settings were often referred out for further psychiatric care or to receive nonpharmacological treatment. Several of the pediatric settings had access to in-house psychotherapy personnel, and it is possible that this access led to increased rates of psychotherapy referrals. In addition, overall depression severity was lower in the pediatric settings, which may have led to increased rates of nonpharmacological treatments.
It is also possible that pediatric providers in our sample did not feel comfortable recommending pharmacotherapy for depression in the pediatric setting or did not have sufficient ongoing follow-up visits for medical appointments to recommend treating the depression in that setting. Regardless of the explanation, the substantial disparity in pharmacotherapy rates (54.8% in psychiatric vs. 6.6% pediatric) suggests disparate treatment and may impact on adolescents who are treated in psychiatric settings versus those treated in pediatric settings, and it unknown whether these differences in treatment are unique to our settings or found in the broader medical community. However, it is important to point out that patients in psychiatric and pediatric settings had similar rates of receiving any type of depression treatment recommendation (64.8% and 70.6%, respectively); simply the type of treatment was different, with psychiatric settings more likely to recommend depression medications and pediatric settings more likely to recommend nonpharmacological treatment or referral to outside mental health care. Furthermore, among those with follow-up visits, remission rates were similar between those in psychiatric and pediatric settings.
Attrition was very high, with only 36.6% of those with moderate-to-severe depression having a follow-up visit. Follow-up visits were more common in the psychiatric setting than in the pediatric setting, which may be due to reduced need for medical follow-up visits in the specific medical clinics, particularly given that the majority with depression were referred to external mental health providers.
In health systems in which it is implemented, MBC plays a crucial role in the detection and diagnosis of depression. However, when it comes to the treatment phase, various barriers impacting patients, parents, or providers can lead to discrepancies in treatment modalities. To address this, MBC tools may include enhanced support for pharmacotherapy, particularly during the early phases of treatment selection. For instance, in cases in whom pharmacotherapy is necessary, but pediatricians are reticent to manage the care themselves, incorporation of pharmacotherapy support could enhance the medication management. This approach can be particularly supportive in collaborative care models where primary care providers receive assistance from psychiatric specialists. Coupling assistance from child psychiatry specialists and using measurement-based support for implementation of treatment recommendations for depression in primary care may be an avenue for improving treatment disparities.
This study has some limitations. The naturalistic and observational design of this study does not allow us to infer causality. Another limitation is that providers were encouraged to use a DSM-5-based diagnostic interview and were provided a checklist to facilitate diagnostic assessment; however, the existing data set does not allow us to assess provider compliance with these recommendations. In addition, the sample is from a large urban hospital, therefore, generalizability to other community treatment settings might be limited. Tertiary medical centers often receive referrals for medically or psychiatrically complicated patients, therefore, psychiatric and medical comorbidities are likely to be more prevalent in these samples than in community-based clinical samples. Another limitation is the high attrition rate of the sample. Future research can shed light on barriers at the patient, provider, or system levels and can help in understanding the effect of other covariates surrounding provider engagement and patient barriers.
Conclusions
Depressive disorders in the pediatric population remain a prevalent diagnosis in both psychiatric and pediatric settings. This study found differences in treatment recommendations for moderate-to-severe depression in pediatric and psychiatric settings, particularly lower rates of antidepressant prescription rates in pediatric settings. MBC is an important tool for detecting and diagnosing depression, yet addressing the disparities in treatment modalities is essential. Enhancing MBC with additional support for pharmacotherapy during early phases of treatment selection, coupled with the integration of collaborative care models, holds the potential to improve the treatment disparities in adolescent depression, especially in the pediatric settings. Further research is needed to understand the nuances of treatment differences and their implications.
Clinical Significance
This study showed differences in treatment recommendations for moderate-to-severe depression between pediatric and psychiatric providers, particularly lower rates of pharmacotherapy use in pediatric settings. Measurement-based care is an important tool for detecting and diagnosing depression, yet disparities in treatment between treatment settings were found even with the support of a measurement-based care decision tool. Augmentation of measurement-based care by providing additional support for pharmacotherapy use during the initial stages of treatment may ameliorate these treatment discrepancies and promote treatment more in line with guidelines for the treatment of depression in pediatric care contexts.
Footnotes
Acknowledgments
The authors thank the patients, clinics, and CRDC staff and colleagues who made this project possible.
Authors' Contributions
G.J.E. contributed to conceptualization (equal), investigation (equal), methodology (lead), and writing—original draft preparation (lead). A.M. was involved in data curation (lead), formal analysis (lead), visualization (lead), and writing—review and editing (equal). J.S.E. carried out conceptualization (supporting), writing—original draft preparation (support), and writing—review and editing (equal). K.Y. took charge of writing—original draft preparation (equal).
M.K.J. took charge of writing—review and editing (equal). G.J.E. carried out investigation (equal), supervision (equal), and writing—review and editing (equal). T.L.M. carried out conceptualization (supporting) and writing—review and editing (equal). M.H.T. was in charge of conceptualization (equal), resources (lead), supervision (equal), funding acquisition (lead), and writing—review and editing (equal).
Data Availability
Data from the VitalSign6 project are not publicly available due to provider and patient confidentiality.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the various funding organizations. The intellectual property of VitalSign6 belongs to the University of Texas Southwestern Medical Center (principal investigator, M.H.T.).
Disclosures
G.J.E. has received research support from the American Foundation for Suicide Prevention (AFSP), Janssen Pharmaceuticals, Janssen Research & Development, National Institutes of Health (NIH), Patient-Centered Outcomes Research Institute (PCORI), and the State of Texas; and consulting fees from Lundbeck and Neuronetics.
M.K.J. has received contract research grants from Acadia Pharmaceuticals, Neurocrine Bioscience, Navitor/Supernus, and Janssen Research & Development; educational grant to serve as section editor of the Psychiatry & Behavioral Health Learning Network; consultant fees from Eleusis Therapeutics US, Inc., Janssen Global Services, Janssen Scientific Affairs, Worldwide Clinical Trials/Eliem and Inversargo, Boehringer Ingelhein, and Guidepoint Global; and honoraria from North American Center for Continuing Medical Education, Medscape/WebMD, Clinical Care Options, and Global Medical Education.
M.H.T. has served as a consultant or advisor for Acadia Pharmaceuticals, Inc., Akili Interactive, Alkermes, Inc. (Pub Steering Comm-ALKS5461), Allergan Sales LLC, Alto Neuroscience, Inc., Applied Clinical Intelligence, LLC, Axome Therapeutics, Boehringer Ingelheim, Engage Health Media, Gh Research, GreenLight VitalSign6, Inc., Heading Health, Inc., Health Care Global Village, Janssen–Cilag. SA, Janssen Research and Development, LLC, Janssen Research and Development, LLC (panel for study design for MDD relapse), Janssen–ORBIT, Legion Health, Jazz Pharmaceuticals, Lundbeck Research U.S.A, Medscape, LLC, Merck Sharp & Dohme Corp., Mind Medicine (MindMed) Inc., Myriad Neuroscience, Neurocrine Biosciences Inc, Navitor, Pharmaceuticals, Inc., Noema Pharma AG, Orexo US Inc., Otsuka Pharmaceutical Development & Commercialization, Inc., Otsuka America Pharmaceutical, Inc. (MDD expert), Pax Neuroscience, Perception Neuroscience Holdings, Inc., Pharmerit International, LP, Policy Analysis Inc., Sage, Therapeutics, Rexahn Pharmaceuticals, Inc., Sage Therapeutics, Signant Health, SK Life Science, Inc., Takeda Development Center Americas, Inc., The Baldwin Group, Inc., and Titan Pharmaceuticals, Inc.
M.H.T. also received editorial compensation from Oxford University Press. E.R.A., A.M., K.Y., J.S.E., and T.L.M. have no conflicts to disclose.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.