
Abstract
Background:
Risperidone and, to a lesser extent, paliperidone are metabolized by CYP2D6; however, there are limited data related to variation in CYP2D6 phenotypes and the tolerability of these medications in children and adolescents. Furthermore, the impact of CYP2D6 on the association of risperidone and paliperidone with hyperprolactinemia in youth is not well understood.
Methods:
A retrospective chart review was performed in psychiatrically hospitalized children and adolescents prescribed risperidone (n = 263, age = 3–18 years, mean age = 13 ± 3 years, 49% female) or paliperidone (n = 124, age = 5–18 years, mean age = 15 ± 2 years, 44% female) who had CYP2D6 genotyping performed as part of routine care. CYP2D6 phenotypes were determined based on Clinical Pharmacogenetics Implementation Consortium guidelines and CYP2D6 inhibitors causing phenoconversion. Adverse effects were obtained from a review of the electronic health record, and patients were selected, in part, to enrich non-normal metabolizers.
Results:
Among risperidone-treated patients, 45% experienced an adverse effect, whereas 36% of paliperidone-treated patients experienced adverse effects. Discontinuation of risperidone due to lack of efficacy was more frequent in the CYP2D6 normal metabolizers and ultrarapid metabolizers compared with intermediate metabolizers (IMs) and phenoconverted poor metabolizers (pPMs) (54.5% vs. 32.7%, p < 0.001). Discontinuation due to weight gain was more common among risperidone- than paliperidone-treated patients (17% vs. 7%, p = 0.011). Among those taking paliperidone, CYP2D6 was associated with discontinuation due to side effects (p = 0.008), and youth with slower CYP2D6 metabolism (i.e., pPMs and IMs) were more likely to discontinue. Hyperprolactinemia was found in 10% of paliperidone-treated patients and 5% of risperidone-treated patients, and slower CYP2D6 metabolizers required higher risperidone doses to cause hyperprolactinemia (p = 0.011).
Conclusions:
CYP2D6 phenotype is associated with discontinuation of risperidone due to lack of efficacy and the dose of risperidone that induced hyperprolactinemia, as well as discontinuation of paliperidone due to adverse effects. Future studies should evaluate exposure-response and toxicity relationships in risperidone- and paliperidone-treated youth.
Introduction
The atypical antipsychotic medication risperidone is commonly used in pediatric patients and is approved by the Food and Drug Administration for the acute treatment of schizophrenia in adolescents aged 13–17 years, bipolar I disorder in children and adolescents, and irritability associated with autism spectrum disorder in youth aged 5–16 years (CDER FDA, 2009). Beyond this, risperidone is commonly prescribed to treat myriad psychiatric disorders in children and adolescents. In addition, its active metabolite, 9-hydroxyrisperidone, also known as paliperidone, is commonly prescribed to pediatric patients with affective and psychotic-spectrum disorders.
Risperidone is primarily metabolized to 9-hydroxyrisperidone by the highly polymorphic hepatic enzyme CYP2D6 (De Leon et al., 2010). Polymorphisms in CYP2D6 correspond with differences in the activity level of the enzyme, with poor metabolizers (PMs) having no CYP2D6 activity, intermediate metabolizers (IMs) having low activity, normal metabolizers (NMs) having normal activity, and ultrarapid metabolizers (UMs) having elevated activity.
Notably, the Dutch Pharmacogenetics Working Group guideline for risperidone recommends CYP2D6 PMs receive a reduced dose or use an alternative drug, whereas they recommend titrating to the maximum dose for the active metabolite for CYP2D6 UMs (PharmGKB, 2020). After administration, the majority of paliperidone is excreted unchanged in the urine; CYP2D6 plays a very small part in the metabolism of paliperidone (De Leon et al., 2010).
Risperidone and paliperidone are associated with numerous adverse effects in youth, including sedation, weight gain, hyperprolactinemia, sexual side effects, dyslipidemia, impaired glucose metabolism, drug-induced Parkinsonism, and akathisia, as well as headaches, nausea, and vomiting (Calarge et al., 2009; Cohen et al., 2012; De Hert et al., 2011; Koch et al., 2023; Krøigaard et al., 2022; Laita et al., 2008; Roke et al., 2009; Safer, 2004). These have generally been difficult to predict, although several studies suggest dose- and exposure-related effects.
For example, Kloosterboer and colleagues (Kloosterboer et al., 2021) found that higher risperidone and 9-hydroxyrisperidone concentrations predict increases in body mass index (BMI) z-scores in risperidone-treated children and adolescents. In addition, in this study, based on the relationship between exposure and response/tolerability, they recommended that for risperidone-treated patients, monitoring plasma concentrations of risperidone and 9-hydroxyrisperidone may help avoid side effects.
Their study suggests that optimal concentrations depend on the age of the child, duration of treatment, and concomitant medication with attention-deficit/hyperactivity disorder (ADHD) drugs. They suggest that for a 10-year-old child, receiving risperidone for 3 months without ADHD comedication 15–25 μg/L would be the theoretical therapeutic range to achieve treatment outcomes of a BMI z-score <1 and Aberrant Behavior Checklist irritability score <11 (Kloosterboer et al., 2021).
In the context of using therapeutic drug monitoring, CYP2D6 genotyping could still be helpful in predicting the starting dose, optimal sampling time, and could be incorporated into the pharmacokinetic model used for suggesting dose adjustments. However, although therapeutic drug monitoring is being evaluated for impact on clinical outcomes (Hermans et al., 2022), it is not current standard practice in risperidone-treated youth. Therefore, using CYP2D6 phenotypes, when available, to predict tolerability and efficacy of risperidone may be of great benefit.
CYP2D6 metabolizer status is associated with risperidone-related side effects in adults, but few studies have evaluated risperidone and paliperidone pharmacogenetics in children and adolescents. Pediatric CYP2D6 PMs and IMs taking risperidone are more likely to experience adverse effects compared with NMs (Rossow et al., 2020). However, it is still unclear whether PMs switching from risperidone to paliperidone decreases the risk of adverse effects, in addition to whether these side effects are common and result in treatment discontinuation or switching to another antipsychotic (Biswas et al., 2022).
In this study, we retrospectively analyzed data from risperidone and paliperidone-treated children and adolescents to determine if CYP2D6 phenotypes are associated with side effects, specifically hyperprolactinemia and weight gain. We hypothesized that CYP2D6 PMs are at an increased risk for risperidone-related side effects because of their inability to convert risperidone into its active metabolite. We also hypothesized that there would be no difference in the risk for side effects among different CYP2D6 metabolizers with paliperidone because the influence of CYP2D6 on paliperidone metabolism is much less than risperidone (De Leon et al., 2010).
Methods
Study design
Data for this study were obtained from electronic health record (EHR) at Cincinnati Children's Hospital Medical Center (CCHMC) from January 1, 2010 to December 31, 2021. Pediatric patients (≤18 years) who were prescribed oral risperidone, oral paliperidone, or intramuscular paliperidone had clinical notes regarding their medication course in their chart, which included adverse effects and tolerability, at least three medication administrations, and underwent pharmacogenetic testing for CYP2D6 as part of routine care were included in this study. This study was approved by the institutional review board at our institution and was deemed exempt in accordance with applicable regulations and institutional policy.
Patients were excluded if the CYP2D6 metabolizer status was undefined or ambiguous (e.g., *1/*4 with a duplication present). Owing to the small sample size, patients receiving tricyclic antidepressants were excluded. Patients with a history of traumatic brain injury (e.g., ICD-10 S06), substance abuse, intellectual disability (e.g., ICD-10 F78: Other intellectual disabilities), organ transplant, or congenital brain abnormality (e.g., ICD-10 Q07: Other congenital malformations of nervous system) were excluded to minimize variability contributed by these conditions, and in the case of organ transplant, to avoid discordance with genotyping and liver enzyme activity. Those with thyroid-stimulating hormone levels >5.5 mU/L were excluded to rule out thyroid disease as a cause of symptoms.
CYP2D6 genotyping
Patient DNA was obtained through blood samples or buccal swabs, which were collected during inpatient hospitalization as part of routine clinical care. CYP2D6 genotyping was performed at the CCHMC Genetics and Genomics Diagnostic Laboratory and included: *2, *2A, *3, *4, *5, *6, *9, *14, *15, *17, *19, *29, *40, *41, and duplications. A *1 allele was inferred if the tested variant alleles were absent. The test methodology, interpretation, and tested alleles changed over the study period, from a TaqMan low-density array with long-range PCR to the Agena VeriDose assay with CYP2D6 copy number variation (CNV) assay (Ramsey et al., 2023). CYP2D6 alleles were extracted from the EHR, and phenotypes were determined using Clinical Pharmacogenetics Implementation Consortium guidelines (Caudle et al., 2020).
When a patient was prescribed a strong CYP2D6 inhibitor concurrently with risperidone or paliperidone (e.g., fluoxetine and paroxetine), the patient was considered phenoconverted to a poor metabolizer (pPM) (Cicali et al., 2021). Moderate inhibitors were not considered due to the variability of inhibition observed with CYP2D6 moderate inhibitors (Cicali et al., 2021).
Data collection
Data extracted from the EHR included patient demographics (e.g., sex, age, race, and ethnicity), diagnoses, weight, height, CYP2D6 pharmacogenetic results, route of administration, maximum daily dose, days treated, concomitant medications, and reason for discontinuation. Clinical notes were reviewed for the presence of risperidone- or paliperidone-related side effects, including weight gain, hyperprolactinemia, drooling, sedation, extrapyramidal symptoms, headaches, nausea/vomiting, and any other side effect attributed to risperidone or paliperidone.
The presence of side effects was verified by a board-certified child and adolescent psychiatrist (S.E.V.). The medication was considered ineffective if the patient discontinued the medication, and the clinical note indicated the reason was because it was ineffective. Data for this study were collected and managed using Research Electronic Data Capture tools hosted at CCHMC (Harris et al., 2009).
Statistical analysis
Changes in BMI were calculated by subtracting the BMI nearest to the time of starting the medication from the BMI nearest the time of data collection or discontinuation of the medication. GraphPad Prism (version 9.5.0) was used to calculate Fisher's exact tests comparing the frequency of hyperprolactinemia in risperidone- versus paliperidone-treated patients, ANOVA test for trend for p-values associating phenoconverted CYP2D6 with BMI change, and chi-square test for trend p-values associating phenoconverted CYP2D6 with the incidence of side effects and inefficacy. R (version 4.2.2) and R Studio (version 2022.12.0) were used to perform linear and logistic regression analyses.
Results
A total of 263 patients were treated with risperidone (Table 1), and 124 patients were treated with paliperidone (Table 2), 79 of whom overlapped between both cohorts. We observed an equal distribution between males and females in both medication cohorts, and the race and ethnicity of each cohort reflects the general catchment area of our hospital. Seven IMs, eight NMs, and one UM were concomitantly taking a strong CYP2D6 inhibitor with risperidone, phenoconverting them to pPMs (Cicali et al., 2021). Among those taking paliperidone, 12 IMs and 11 NMs were concurrently taking a strong CYP2D6 inhibitor, phenoconverting them to pPMs. The phenoconverted CYP2D6 metabolizer status was not associated with the maximum dose of risperidone or paliperidone (p > 0.6).
Demographic and Clinical Characteristics of Risperidone-Treated Patients
DMDD, disruptive mood dysregulation disorder; SD, standard deviation.
Demographic and Clinical Characteristics of Paliperidone-Treated Patients
DMDD, disruptive mood dysregulation disorder; IM, intramuscular; NA, not applicable; SD, standard deviation.
Among risperidone-treated patients, 45% of patients (n = 119) experienced a side effect, among whom 30% (n = 79) discontinued risperidone, and 41% of patients (n = 108) discontinued the medication due to inefficacy (Table 3). The most frequent side effects were weight gain (n = 44, 16.7%) and extrapyramidal symptoms (n = 24, 9.1%). Headaches (n = 7) and nausea/vomiting (n = 5) attributed to risperidone treatment were observed infrequently and were not analyzed further.
Risperidone-Related Side Effects
BMI, body mass index; NA, not applicable due to small sample size; SD, standard deviation.
Chi-square test for trend.
ANOVA test for trend.
Side effects that were more common with higher body weight-adjusted doses of risperidone were BMI change (p = 0.0003), extrapyramidal symptoms (p = 0.00003), and hyperprolactinemia (p = 0.038); however, discontinuation due to weight gain (p = 0.9) was not. Discontinuation due to any side effect was not associated with CYP2D6 metabolizer status (p = 0.9), nor were extrapyramidal symptoms (p = 0.43), discontinuation due to weight gain (p = 0.9), and BMI change (p = 0.24).
Among paliperidone-treated patients, 36% (n = 45) experienced a side effect, among whom 24% (n = 30) discontinued paliperidone, and 15% (n = 19) discontinued due to inefficacy (Table 4). The most frequent side effects were extrapyramidal symptoms (n = 12, 9.7%) and hyperprolactinemia (n = 12, 9.7%). Headaches (n = 2) and nausea/vomiting (n = 1) attributed to paliperidone treatment were observed infrequently and not analyzed further.
Paliperidone-Related Side Effects
BMI, body mass index; NA, not applicable due to small sample size; SD, standard deviation.
Chi-square test for trend.
ANOVA test for trend.
Side effects that were more common with higher body weight-adjusted doses of paliperidone were BMI change (p = 0.0002) and discontinuation due to weight gain (p = 0.015 in a generalized linear model accounting for the route of administration and phenoconverted CYP2D6; Supplementary Table S1), whereas extrapyramidal symptoms (p = 0.9) and hyperprolactinemia (p = 0.8) were not. Discontinuation due to any paliperidone-related side effect were significantly different between CYP2D6 phenotypes (p = 0.008), and were associated with the route of administration of paliperidone (27.3% with oral administration vs. 12% with intramuscular administration).
Discontinuation of risperidone due to lack of efficacy was more frequent in the CYP2D6 NMs and UMs than IMs and pPMs (p = 0.002; Table 3). Discontinuation due to lack of efficacy was also associated with a diagnosis of a bipolar disorder (p = 0.046), diagnosis of a depressive disorder (p = 0.049), and higher weight-adjusted doses of risperidone (p = 0.004). In a generalized linear model accounting for diagnosis of bipolar disorder (β = −0.153, p = 0.041), depression (β = −0.108, p = 0.11), and body weight-adjusted dose (β = 2.615, p = 0.013), phenoconverted CYP2D6 metabolizer status remained significantly associated with discontinuation of risperidone due to lack of efficacy (β = 0.092, p = 0.003; Supplementary Table S2).
Hyperprolactinemia was observed in 5% (n = 14) of the risperidone-treated patients, with 9% of NMs, 3% of pPMs, and 4% each of IMs and UMs (Table 3). Hyperprolactinemia was found in 9.7% (n = 12) of the paliperidone-treated patients, with 13% of phenoconverted pPMs, 14% of IMs, 3% of NMs, and none of the UMs (Table 4). Among risperidone-treated patients, the maximum body weight-adjusted dose in patients experiencing hyperprolactinemia was lower with increasing metabolism; slower metabolizers were receiving higher doses of risperidone that caused hyperprolactinemia (Fig. 1; p = 0.011, generalized linear model accounting for weight-adjusted dose, sex, and depression diagnosis; Supplementary Table S3). However, there was no association between CYP2D6 and hyperprolactinemia in paliperidone-treated patients (p = 0.074).
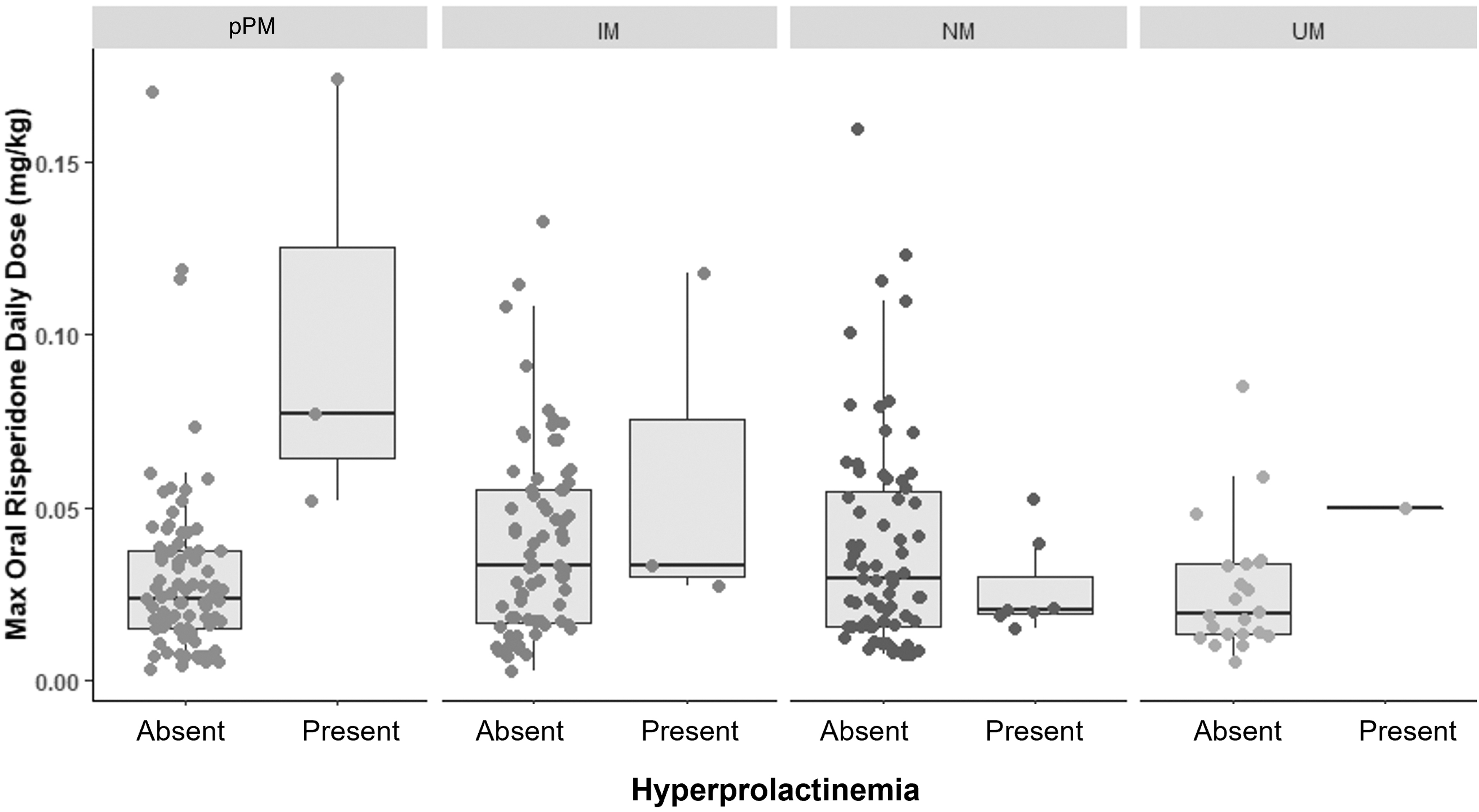
Hyperprolactinemia by CYP2D6 phenotype and dose. IM, intermediate metabolizer; NM, normal metabolizer; pPM, phenoconverted poor metabolizer; UM, ultrarapid metabolizer.
Discontinuation due to weight gain was significantly more common among the risperidone- than the paliperidone-treated patients (16.7% vs. 7.3%, p = 0.011, Fisher's exact test). CYP2D6 metabolizer status was associated with discontinuation due to weight gain in paliperidone-treated patients (p = 0.039; Table 4), with higher rates of discontinuation in slower metabolizers. This remained significant after adjusting for dose and route of administration (p = 0.045; Supplementary Table S1).
Discussion
In this retrospective study, we investigated the influence of pharmacogenetics on hyperprolactinemia, weight gain, extrapyramidal symptoms, and other side effects in risperidone- and paliperidone-treated youth. This study represents the largest examination of the role of pharmacogenetics on risperidone/paliperidone adverse effects to date. We found that after adjusting for the dose, CYP2D6 poor metabolizers were less likely to discontinue risperidone due to lack of efficacy but more likely to discontinue paliperidone due to weight gain. We also found that CYP2D6 poor metabolizers required higher doses of risperidone to cause hyperprolactinemia. The relationships between CYP2D6 metabolizer status, medication dose, and tolerability are closely intertwined and are discussed further hereunder.
The relationship between risperidone dose, CYP2D6 metabolism, and hyperprolactinemia has important clinical implications. It likely reflects the complex regulation of prolactin and the pharmacodynamic and pharmacokinetic effects of the medications. Pituitary prolactin secretion is negatively regulated by dopamine, such that decreasing dopamine unleashes pituitary lactotrophs, which secrete prolactin, from tonic dopaminergic inhibition (Strawn and Geracioti, 2023).
Furthermore, serotonin and dopamine have reciprocal roles in regulating prolactin secretion, with dopamine inhibiting prolactin release through stimulation of D2 receptors and serotonin promoting prolactin release through stimulation of 5HT2A receptors (Strawn and Stahl, 2023). Thus, although risperidone +9-hydroxyrisperidone exposure has been associated with hyperprolactinemia in youth, the combination of CYP2D6-driven pharmacokinetic variability and potential pharmacodynamic differences may contribute to differences in the risk of hyperprolactinemia (Correll et al., 2010; Correll et al., 2009; Solmi et al., 2020).
For example, CYP2D6 poor metabolizers may have greater risperidone to metabolite ratios and, therefore, differences in the ratio of D2 to 5-HT2A antagonism could contribute to differences in the risk of hyperprolactinemia. In a small study, Knegtering et al. found a stronger association between blood prolactin levels and paliperidone blood concentration compared with risperidone blood concentration after administration of risperidone (Knegtering et al., 2005).
Furthermore, our data do not address the temporal course of prolactin changes in risperidone-/paliperidone-treated children and adolescents, which initially increase rapidly, peak within 4–5 weeks, and then persist indefinitely in some youth (Koch et al., 2023). Whether patients who experience these sustained increases in prolactin are related to CYP2D6 remains to be determined (Troost et al., 2007).
We observed that discontinuation due to weight gain was more common among the risperidone- than the paliperidone-treated patients, but was unaffected by CYP2D6 metabolizer status or dose of risperidone. However, the CYP2D6 metabolizer status, route, and dose of paliperidone were associated with discontinuation due to weight gain. These findings underscore the complexity of weight gain as an adverse effect of second-generation antipsychotics.
Weight gain has been associated with multiple pharmacodynamic factors, including binding profiles at 5-HT2A, 5-HT2C, D3, H1, and M3 receptors (Roerig et al., 2012), and importantly, substantial binding at these receptors may occur at lower blood levels than those typically required for therapeutic efficacy, which is often—at least for psychotic and affective disorders—related to D2 occupancy. Furthermore, although risperidone and paliperidone differ in D2/5-HT2A profiles, they are similar in 5-HT2C, H1, and M3 receptor binding (Corena-McLeod, 2015) and may obscure the relative contribution of either moiety or the CYP2D6-related ratio of risperidone to paliperidone with weight gain.
Furthermore, clinical factors may dampen our ability to detect CYP2D6-related changes in risperidone-induced weight gain. For example, changes in appetite may be associated with the underlying disorder being treated, and during the age range being studied, there are age- and sex-related developmental shifts in weight and growth.
The relationship between increased hyperprolactinemia and extrapyramidal symptoms in patients receiving higher body weight-adjusted doses of risperidone raises the possibility that clinicians could identify patients or prescribing patterns that increase the risk of specific side effects. Such predictors are urgently needed, particularly for hyperprolactinemia, given that it is difficult to predict and, once present, requires complex management. However, unlike hyperprolactinemia, which has an inscrutable relationship to risperidone exposure in youth, our finding that higher weight-adjusted doses of risperidone are associated with an increased risk of extrapyramidal symptoms replicates prior studies in adults and pediatric patients (Kloosterboer et al., 2021; Knegtering et al., 2005; Troost et al., 2007).
The abstruse relationships between CYP2D6, risperidone, paliperidone, and tolerability likely relate to clinical features, prescribing patterns, and medication formulation. First, in terms of oral administration, risperidone dosing is more flexible, with doses ranging from 0.25 to 6 mg, whereas paliperidone doses are fixed at 1.5, 3, 6, and 9 mg with fewer dosing increments available. Thus, especially at the “lower” dosing range for the two medications, there is substantially more opportunity for fine dose adjustment with risperidone compared with paliperidone.
In addition, the distribution of risperidone-treated conditions differs from paliperidone-treated conditions, which introduces an additional source of variation that is compounded by the tendency of clinicians to use different dosing and titrations across these disorders.
These patients received CYP2D6 testing as part of routine clinical care, usually at the time of an inpatient admission to the psychiatry unit. The report is automatically uploaded to the results section of the electronic medical record (without notifying the provider) and includes dosing recommendations for risperidone but not paliperidone. If risperidone is ordered after the results are returned, an alert will indicate the patient's CYP2D6 status and notify the provider that recommendations for dosing risperidone are available in the result report.
For a CYP2D6 poor metabolizer, the report includes a recommendation for 50%–75% of the usual risperidone dose for the given indication, based on the difference in risperidone pharmacokinetics between PMs and NMs (Stingl et al. 2013), which is consistent with the Dutch Pharmacogenetic Working Group guideline for a 67% reduction of risperidone in CYP2D6 poor metabolizers (Beunk et al., 2023). However, the body-weight adjusted risperidone doses were similar across CYP2D6 metabolizer groups, both without accounting for phenoconversion and after accounting for phenoconversion.
This lack of difference could be due to a multitude of reasons, including differences in the primary indication for prescribing risperidone, lack of knowledge about the CYP2D6 result report recommendations being in the chart, or lack of confidence in the recommendations. With our finding of increased risk of discontinuation of paliperidone due to weight gain in CYP2D6 pPMs and IMs, one could consider dose reductions and/or slow titration in these patients.
Finally, although this is the largest examination of the role of pharmacogenetics on risperidone/paliperidone adverse effects to date, it has several important limitations. First, it is a retrospective study, and the population is clinically heterogeneous, with variable follow-up. Second, we lacked direct measures of risperidone and paliperidone concentrations in the blood, which raises the possibility that non-CYP2D6-related factors could influence exposure, including adherence. In this regard, adherence may also be related to side effects, further complicating our ability to elucidate these genotype-dose-tolerability relationships.
We also did not analyze whether concomitant medications influenced weight gain (e.g., metformin and methylphenidate). An additional limitation of our study is our inability to analyze the timing of discontinuation related to side effects due to significant variability in our sampling methods and inconsistencies in clinicians' documentation of discontinuation reasons, cross-titration, dose reduction, and others. Finally, the sample was racially and ethnically homogeneous and was conducted at a single site, which potentially limits the generalizability of these findings.
Conclusion
CYP2D6 phenotype is associated with clinically important outcomes in youth. Discontinuation of risperidone due to lack of efficacy was more common in faster metabolizers than slower metabolizers, however discontinuation of palipeidone due to adverse effects was more common among slower metabolizers compared to faster metabolizers. The dose of risperidone that induced hyperprolactinemia was higher in slower metabolizers compared to faster metabolizers. Prospective studies are needed to more thoroughly evaluate relationships between exposure, toxicity and efficacy.
Clinical Significance
These findings have important clinical implications. In the cohort of patients treated with risperidone and paliperidone, side effects were common, highlighting the need to assess and monitor side effects continually. In addition, these data raise the possibility that considering the CYP2D6 phenotype may inform the risk of hyperprolactinemia at a given dose in risperidone-treated patients. Clinicians should monitor weight-based dosing as risperidone is titrated to preemptively identify patients at greater risk of developing hyperprolactinemia, as well as other side effects, including weight gain and extrapyramidal symptoms.
Footnotes
Acknowledgment
The authors appreciate the help of Christina Horton in the design of the data collection instrument used in this study. The authors used Research Electronic Data Capture (REDCap) for chart review and thank the Center for Clinical and Translational Science and Training grant for supporting REDCap (UL1TR001425).
Authors' Contributions
Conceptualization, investigation, and writing by A.A.K. Investigation and writing by M.M.J. Conceptualization, data curation, and writing by E.A.P. Conceptualization, validation, and writing by S.E.V. Conceptualization and writing by J.R.S. Conceptualization, analysis, writing, visualization, and supervision by L.B.R.
Disclosures
Authors of this presentation disclose the following relationships: A.A.K., M.M.J., E.A.P., and S.E.V. have nothing to disclose. J.R.S.: Research support from AbbVie, PCORI, the National Institutes of Health and the Yung Family Foundation. He has provided consultation to Cerevel, Intracellular Therapeutics, and Otsuka. He receives royalties from Springer Publishing, Cambridge, and UpToDate, and material support from Myriad. He has also received honoraria from Medscape Live, Neuroscience Education Institute, the American Academy of Pediatrics, and the American Academy of Child and Adolescent Psychiatry. L.B.R.: Consultant: BTG Specialty Pharmaceuticals, Inc.; Support: BTG Specialty Pharmaceuticals, Inc.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.