
Abstract
Objective:
Attention-deficit/hyperactivity disorder (ADHD) treatment with stimulant products has been shown to be safe and effective; however, there are remaining concerns about their possible adverse effects on growth trajectories. We conducted a systematic review of the extant literature derived from ecologically valid databases and registries to assess the body of knowledge about the effects of stimulants on growth trajectories in naturalistic samples.
Methods:
Using PubMed and PsycINFO, we searched for articles published before February 8, 2023 that focused on growth findings associated with stimulant treatment in pediatric ADHD from comprehensive datasets derived from naturalistic population studies.
Results:
Of the 1070 articles initially identified, 12 met all inclusion criteria. Sample sizes ranged from 157 to 163,820 youths. Seven of 10 articles examining height found significant decreases in height associated with chronic stimulant treatment that normalized over time in 2 studies. Three articles found no significant association between stimulant treatment and height. No clear associations were identified between cumulative duration and dose of stimulant treatment and adult height. All articles examining weight and six of eight articles examining body mass index (BMI) found significant initial decreases that tended to normalize then increase over time. Longer duration of stimulant medication use was predominantly associated with significant weight and BMI reductions. The effects of stimulant dose on weight and BMI were mostly weak and clinically insignificant. Most studies found no significant association between age at start of stimulant treatment and change in height, weight, or BMI. Most studies did not find significant sex effects in relation to growth parameters.
Conclusions:
This review of ecologically informative samples revealed that the effects of stimulant treatment on growth trajectories are mainly small and transient. These effects seem to be clinically insignificant for most youth with ADHD who receive stimulant treatment from childhood onto adolescence and adulthood.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a prevalent and morbid neurobiological disorder estimated to affect 5% of children (Faraone et al., 2015). It is associated with high rates of many adverse functional outcomes including comorbid psychiatric disorders (Biederman et al., 2006), academic impairments (Barkley et al., 1991), accidents and injuries (Chen et al., 2017b), and car accidents (Thompson et al., 2007), among many others (Faraone et al., 2021).
While treatment for ADHD with stimulant products, such as methylphenidate (MPH) and amphetamine (AMPH), has been shown to be safe and effective (Boland et al., 2020; Faraone et al., 2006; Fredriksen et al., 2013), there are remaining concerns regarding their possible impact on growth trajectories (Charach et al., 2006; Faraone et al., 2008; MTA Cooperative Group, 2004; Poulton et al., 2013; Powell et al., 2015; Swanson et al., 2007; Zhang et al., 2010). To date, most of the literature on the subject has relied on selected samples (Banaschewski et al., 2018; Greenhill et al., 2020; Waxmonsky et al., 2022) and studies investigating the effects of particular stimulant products or compounds (Diez-Suarez et al., 2017; Zhang et al., 2010). Because these studies show small stimulant-associated decrements on growth trajectories, they have been interpreted by some authors as reassuring (Faraone et al., 2008; Harstad et al., 2014; Pliszka et al., 2006) and by others as concerning (Davallow Ghajar and DeBoer, 2020; Powell et al., 2015; Yackobovitch-Gavan et al., 2021). These differences create uncertainties about the seriousness of this problem and call for more research on this subject.
Examining growth trajectories in children treated with stimulants using comprehensive datasets derived from registries, cohorts, electronic medical records, or insurance claims is one method to overcome the limitations of studies derived from clinical trials, which are typically limited to one drug and apply exclusionary criteria to create samples that are not ecologically valid. The naturalistic datasets contain information on the full range of stimulants and patients with ADHD and, in turn, can provide comprehensive evidence on the potential effects of stimulants on growth trajectories.
Research on population-based datasets has greatly advanced medical knowledge for a wide range of conditions including macular degeneration, sickle cell disease, and pediatric cancer, among others (Brandl et al., 2019; Claster et al., 2013; Rice et al., 2015). These studies have allowed for the examination of the impact of therapies, regional rates of mortality, and average cost of specific treatments. Such information enables health care professionals and organizations to better understand current regional, nationwide, and international trends across a wide range of treatments and health care costs. Because these population-based databases are very large and linked to other health records and registries, they are distinctively poised to provide ecologically informative evidence on the impact of various diseases on the population. They also allow for the examination of the influence of treatment on these conditions. Compared with clinical trials, these studies can provide information on the full range of patients with ADHD, not only those meeting the many inclusion and exclusion criteria of clinical trials.
The main aim of this study was to conduct a systematic review of the literature from naturalistic databases to assess the effects of stimulant treatment on growth trajectories in stimulant-exposed children and adolescents. We hypothesized that the effects of stimulant exposure on growth trajectories would be minimal. To the best of our knowledge, this review of is one of the most comprehensive evaluations of this important topic.
Materials and Methods
Literature review
A literature search was performed using PubMed and PsycINFO. The following algorithm was used: (“attention deficit”[Title/Abstract] OR ADHD[Title/Abstract]) AND (height[Title/Abstract] OR weight[Title/Abstract] OR growth[Title/Abstract] OR “body mass index”[Title/Abstract] OR BMI[Title/Abstract]) AND (stimulant[Title/Abstract] OR methylphenidate[Title/Abstract] OR treatment[Title/Abstract] OR amphetamine[Title/Abstract] OR medication[Title/Abstract] OR psychostimulants[Title/Abstract]) AND (child*[Title/Abstract] OR youth[Title/Abstract] OR adolescent[Title/Abstract]). The search was limited to articles published before February 8, 2023. From the search results, we selected articles using the following criteria: (1) the study's focus was on growth findings associated with stimulant treatment in ADHD; (2) the sample size was 150 or greater; (3) the study relied on registry data, cohort data, electronic medical record data, or insurance claims data. We excluded articles not published in the English language, review articles, clinical trials, editorials, and commentaries.
Five authors (C.H.V., J.B., M.D., H.P., K.Y.W.) screened the articles for relevance and eligibility. Articles initially deemed eligible were cross-referenced for other relevant and potentially suitable articles that had been cited in their text. These cited articles were then screened according to the same inclusion and exclusion criteria.
Data extraction
The following variables were extracted from available studies: type of study, sample size, growth measurements examined, type of treatment, mean daily dose, and length of follow-up.
Results
Articles identified
As shown in Figure 1, our search resulted in 1070 articles (Table 1). After eliminating duplicate records, 837 unique articles were screened according to our inclusion/exclusion criteria. One hundred-six articles were identified as potentially relevant and carefully examined. Of the 106, 12 articles met all inclusion and exclusion criteria. Excluded were articles that either (1) did not focus on growth findings associated with stimulant treatment in ADHD (N = 39); (2) had a sample size of <150 (N = 15); (3) were review articles (N = 25); or (4) reported results of clinical trials (N = 15).
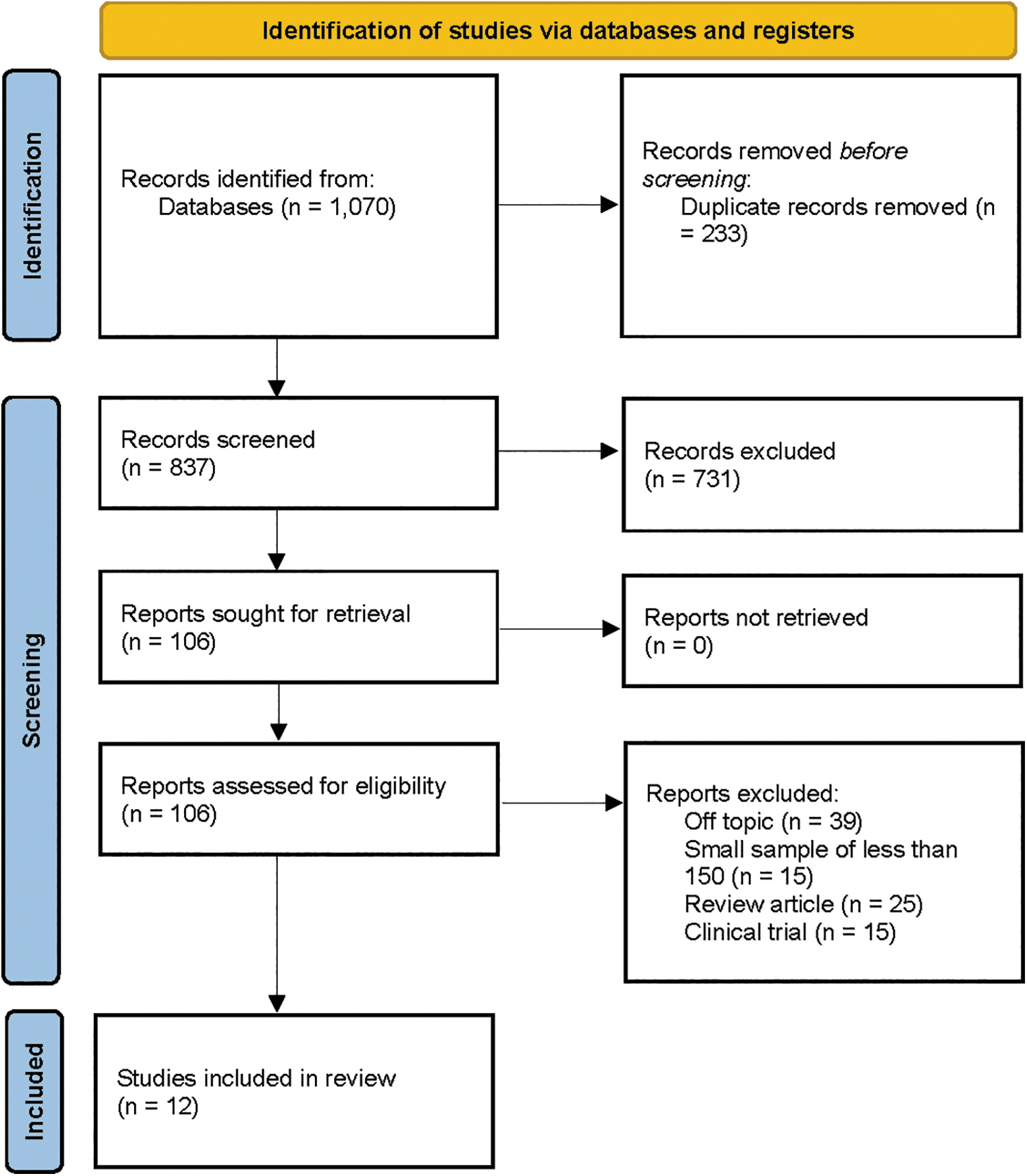
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Growth Findings Associated with Stimulant Treatment in Attention-Deficit/Hyperactivity Disorder Reported in Large-Scale Datasets Without Inclusion and Exclusion Criteria
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index; MEUs, MPH equivalent units; MPH, methylphenidate; SDS, standard deviation score.
Of the 12 included articles, 5 (42%) were derived from U.S. datasets (Biederman et al., 2023; Bowling et al., 2017; Davallow Ghajar and DeBoer, 2020; Harstad et al., 2014; Schwartz et al., 2014), while the other 7 (58%) were from Israel (Dubnov-Raz et al., 2011), Korea (Kim et al., 2014), Denmark (Powell et al., 2015), Spain (Diez-Suarez et al., 2017), the Netherlands (Lentferink et al., 2018), Thailand (Koonrungsesomboon and Koonrungsesomboon, 2020), and Turkey (Turan and Akay, 2020).
The sample sizes in these articles ranged from 157 to 163,820 youth with ADHD. Six studies examined only MPH treatment on growth parameters (Diez-Suarez et al., 2017; Dubnov-Raz et al., 2011; Kim et al., 2014; Koonrungsesomboon and Koonrungsesomboon, 2020; Lentferink et al., 2018; Turan and Akay, 2020), whereas the others examined the effect of all stimulant treatments (Biederman et al., 2023; Bowling et al., 2017; Davallow Ghajar and DeBoer, 2020; Harstad et al., 2014; Powell et al., 2015; Schwartz et al., 2014).
Effects of stimulants on height trajectories
Ten of the 12 articles included in this review examined height. Of these, seven found significant decreases in height z-scores in stimulant-treated youth with ADHD (Biederman et al., 2023; Davallow Ghajar and DeBoer, 2020; Diez-Suarez et al., 2017; Kim et al., 2014; Lentferink et al., 2018; Powell et al., 2015; Turan and Akay, 2020). These z-scores normalized over time in two of the studies (Davallow Ghajar and DeBoer, 2020; Kim et al., 2014). Three articles found no significant association between stimulant treatment and height trajectories (Dubnov-Raz et al., 2011; Harstad et al., 2014; Koonrungsesomboon and Koonrungsesomboon, 2020). One of these articles reported no significant difference in adult height (i.e., final height) between stimulant-treated and stimulant-naïve patients with ADHD (males: mean difference = 0.6 cm; females: mean difference = 0.2 cm) (Harstad et al., 2014).
As shown in Table 2A, two of six studies found that longer duration of stimulant treatment was associated with greater reductions in height z-scores (Davallow Ghajar and DeBoer, 2020; Kim et al., 2014), but these effects were transient in one study (Kim et al., 2014) [(A) in Table 2]. For example, Kim et al. (2014), reported that an 8-year-old boy of average height (z-score = 0) at the start of treatment would only be 0.43 cm less than the expected after 1 year of treatment (Kim et al., 2014). A third study found a positive association between duration of stimulant treatment changes in height z-scores (Koonrungsesomboon and Koonrungsesomboon, 2020). The remaining three studies found no significant association between duration of stimulant treatment and growth in height trajectories (Diez-Suarez et al., 2017; Harstad et al., 2014; Turan and Akay, 2020) [(A) in Table 2], with one reporting no correlation between cumulative duration of stimulant treatment and adult height (i.e., final height) (Harstad et al., 2014).
Effect of Cumulative Stimulant Use Duration on Changes in Growth Outcomes
Indicates significant result.
BMI, body mass index.
Although three of five studies found significant but weak associations between higher stimulant dose and greater reductions in height z-scores (Diez-Suarez et al., 2017; Lentferink et al., 2018; Powell et al., 2015), in one, higher dose did not predict final height (Diez-Suarez et al., 2017). The other two articles did not find a significant association between stimulant dose and reductions in height z-scores (Kim et al., 2014; Turan and Akay, 2020). Other articles found either a weak correlation (Diez-Suarez et al., 2017) or no correlation (Kim et al., 2014; Powell et al., 2015; Turan and Akay, 2020) between age at start of treatment and changes in height trajectories. Most articles did not find significant sex effects (Dubnov-Raz et al., 2011; Harstad et al., 2014; Kim et al., 2014; Powell et al., 2015; Turan and Akay, 2020), but of the four that did (Biederman et al., 2023; Diez-Suarez et al., 2017; Koonrungsesomboon and Koonrungsesomboon, 2020; Lentferink et al., 2018), three found that reductions in height z-scores were more pronounced in females than in males (Biederman et al., 2023; Diez-Suarez et al., 2017; Lentferink et al., 2018).
Effects of stimulants on weight trajectories
Six of the 12 articles included in this review examined stimulant-associated effects on weight trajectories. All six articles found significant decreases in weight z-scores (Biederman et al., 2023; Diez-Suarez et al., 2017; Kim et al., 2014; Koonrungsesomboon and Koonrungsesomboon, 2020; Powell et al., 2015; Turan and Akay, 2020). However, these decreases only lasted a short period of time before normalizing in four of them (Biederman et al., 2023; Kim et al., 2014; Koonrungsesomboon and Koonrungsesomboon, 2020; Powell et al., 2015).
As shown in Table 2B, two of four studies found that longer duration of stimulant medication use was associated with greater reductions in weight z-scores over time (Diez-Suarez et al., 2017; Kim et al., 2014) [(B) in Table 2], but in one study, they stabilized and subsequently increased after 1 year of treatment (Kim et al., 2014). For example, Kim et al. (2014), reported that an 8-year-old boy of average weight (z-score = 0) at the start of treatment would only be 0.67 kg less than the expected after 1 year of treatment (Kim et al., 2014). A third study found a positive association between longer duration of stimulant medication use and changes in weight z-scores over time (Koonrungsesomboon and Koonrungsesomboon, 2020), while a fourth study found no significant association (Turan and Akay, 2020) [(B) in Table 2].
An association between higher stimulant dose and greater reductions in weight z-scores was found in two articles (Diez-Suarez et al., 2017; Powell et al., 2015). However, the association was weak in one study (Diez-Suarez et al., 2017) and the sample size of those with high dosages was small in the other (Powell et al., 2015), limiting the accuracy of the calculation. An additional two articles found no association between dose and change in weight z-scores (Kim et al., 2014; Turan and Akay, 2020). Three out of four articles found no association between age at start of treatment and changes in weight trajectory (Diez-Suarez et al., 2017; Kim et al., 2014; Powell et al., 2015). In the one study that did, younger age at first treatment was associated with greater decline in weight z-scores and predicted final weight (Turan and Akay, 2020). Three articles did not find significant sex effects (Dubnov-Raz et al., 2011; Powell et al., 2015; Turan and Akay, 2020), but four did (Biederman et al., 2023; Diez-Suarez et al., 2017; Kim et al., 2014; Koonrungsesomboon and Koonrungsesomboon, 2020), with three finding that reductions in weight z-scores were more pronounced in females than in males (Biederman et al., 2023; Diez-Suarez et al., 2017; Kim et al., 2014).
Effects of stimulants on body mass index trajectories
Eight of the 12 articles included in this review examined stimulant-associated body mass index (BMI) trajectories. Of those, six articles found significant decreases in BMI z-scores among stimulant-treated youth with ADHD (Biederman et al., 2023; Bowling et al., 2017; Davallow Ghajar and DeBoer, 2020; Diez-Suarez et al., 2017; Lentferink et al., 2018; Schwartz et al., 2014), which were transient in four of the articles (Biederman et al., 2023; Bowling et al., 2017; Davallow Ghajar and DeBoer, 2020; Schwartz et al., 2014). In these studies, decreases in BMI trajectories mostly occurred during childhood with stabilization or increases during adolescence. One article did not find a significant association between stimulant treatment and BMI trajectory in the group as whole, but when stratified by children and adolescents, found a significant association in children only (Turan and Akay, 2020). An additional article found no significant association between stimulant treatment and BMI trajectory (Dubnov-Raz et al., 2011).
As shown in Table 2C, three of four studies found that longer duration of stimulant medication use was associated with greater reductions in BMI z-score trajectories (Davallow Ghajar and DeBoer, 2020, Diez-Suarez et al., 2017; Schwartz et al., 2014) [(C) in Table 2], with one study showing that BMI growth trajectory normalized and subsequently accelerated during adolescence (Schwartz et al., 2014). The fourth study found no significant association (Turan and Akay, 2020). Results for the effects of stimulant dose on BMI trajectories were weak, with two articles finding significant but weak correlations between dose and decreases in BMI z-scores (Diez-Suarez et al., 2017; Lentferink et al., 2018) and a third article finding no association (Turan and Akay, 2020).
Three of four studies found no significant association between age at start of stimulant treatment and change in BMI trajectory (Bowling et al., 2017; Diez-Suarez et al., 2017; Turan and Akay, 2020), and the one that did found that younger age at first stimulant use was associated with slower BMI growth trajectory in early childhood, with subsequent normalization followed by increases in adolescence (Schwartz et al., 2014). Additionally, three of five studies found no sex effects in relation to change in BMI growth trajectory (Dubnov-Raz et al., 2011; Lentferink et al., 2018; Turan and Akay, 2020). The two studies that did reported a stronger effect among females (Biederman et al., 2023; Diez-Suarez et al., 2017).
Discussion
Naturalistic growth trajectories in children exposed to stimulants were examined using data from ecologically valid, naturalistic datasets and registries. We found significant but small initial decreases in height (Δ z-score: −0.47 to −0.0017), weight (Δ z-score: −0.40 to −0.0271), and BMI (Δ z-score: −0.52 to −0.03) trajectories in children exposed to stimulants that tended to attenuate over time, with little evidence of enduring effects, even into adult life. The modest effects on growth trajectories observed in naturalistic samples are consistent with the literature from clinical trials (Faraone et al., 2008). In light of the morbidity associated with ADHD, the efficacy and protective effects of stimulant treatment, and the risks associated with not treating the disorder (Biederman et al., 2019; Faraone et al., 2021), these small decreases in growth trajectories from childhood to adolescence and adult years should aid clinicians and parents in assessing the risks versus benefits of stimulant treatment for children with ADHD.
Small decreases in height trajectories that are associated with stimulant treatment are likely to have negligible clinical significance for most children. However, these changes can differ on a case-by-case basis, which supports the clinical advice to monitor growth parameters in stimulant-treated youth for potential outliers (Carucci et al., 2021). On the other hand, the observed increases in weight and BMI trajectories in adolescence, particularly in females with ADHD, are consistent with emerging literature supporting clinical (Chen et al., 2019; Cortese et al., 2016; Muntaner-Mas et al., 2021) and genetic associations between ADHD and obesity (Chen et al., 2018; Chen et al., 2017a), which warrants close clinical attention.
Swanson et al. (2017) expressed concerns regarding height findings from the 16-year follow-up of the Multimodal Treatment of Attention Deficit Hyperactivity Disorder (MTA) study; however, their findings demonstrate a small average height z-score of only −0.226 at adult height for “consistently treated” participants with ADHD. Notably, the small height z-score indicates that “consistently treated” participants with ADHD, on average, were only marginally shorter than those of average height from whom z = 0.0 by definition (Swanson et al., 2017). Furthermore, a more recent analysis of MTA participants' growth trajectories emphasized that only small changes in height trajectory and increases in weight and BMI were associated with 16 years of “consistent” stimulant treatment among youth with ADHD (Greenhill et al., 2020).
Although Waxmonsky et al. (2020) and Carucci (2020) proposed the use of “drug holidays” to mitigate stimulant-associated adverse effects on growth trajectories, this recommendation should be followed with caution and reserved for the few cases demonstrating salient adverse effects on growth trajectories. There is limited data to support the proposed use of “drug holidays” (Waxmonsky et al., 2020), and prescribers should carefully consider the importance of weekends and holidays for success related to critical life functions (such as family, work, study, use of leisure time, and social life), which can be negatively affected by untreated ADHD. They should also consider if it is wise to have drug holidays for adolescents of driving age, given the association of ADHD with traffic accidents and the beneficial effects of stimulants on driving (Biederman et al., 2012; Biederman et al., 2007).
The mechanisms underlying growth deficits associated with ADHD are not understood. Some studies have found dysregulated growth trajectories in height and weight among children and adolescents with ADHD, irrespective of stimulant-treatment status (Faraone et al., 2012; Namimi-Halevi et al., 2023), which further supports the need to investigate potential factors underlying the association between ADHD, its treatment, and growth.
Our findings should be considered in light of some methodological limitations. Despite the beneficial, naturalistic characteristics of the identified samples, the available number of studies in this review was relatively small. However, because the available studies included samples from varied sources and geographic locations, our findings may generalize across clinical settings and geographical locations.
Conclusions
This systematic qualitative review examining the available literature about growth trajectories in stimulant-exposed children from ecologically informative naturalistic datasets suggests small, and largely transient, effects on growth trajectories over time in height, weight, and BMI. These reassuring findings extend previously reported findings derived from clinical trials suggesting the risks versus benefits analysis favors benefits when considering stimulant treatment for children with ADHD. Nevertheless, children with ADHD who are receiving stimulants should be monitored by their prescribers for growth deficits, and those with substantial decreases in height or increases in weight require close clinical attention.
Clinical Significance
This systematic review addresses lingering concerns regarding the possible adverse effects of stimulant medications on growth trajectories, revealing that any observed effects are generally small and transient. These findings hold clinical significance by offering reassurance to clinicians and parents as they navigate ADHD treatment decisions and contribute to the broader scientific discourse on the safety and efficacy of stimulant medications. Fortunately, growth is easily monitored, so should a large deviation in growth trajectory occur, it can be detected and addressed, as appropriate, by changing the dose or medication.
Footnotes
Acknowledgment
This work is published in honor of J.B. J.B. was a pioneer of child psychiatry and the founder of the field of pediatric psychopharmacology. He dedicated his career to examining the cause, diagnosis, and treatment of ADHD across the lifespan and was a fierce advocate for his patients and their families. J.B. mentored hundreds of people, both professionally and personally, and treated thousands of patients throughout his more than 40-year career at Massachusetts General Hospital. In addition to his exceptional competence as a psychopharmacologist, he was considered an empathetic physician beloved by all who knew him.
Authors' Contributions
C.H.V.: methodology, validation, formal analysis, writing—original draft, writing—reviewing and editing, visualization, project administration. J.B.: conceptualization, methodology, validation, formal analysis, writing—original draft, writing—reviewing and editing, visualization, supervision. M.D.: methodology, validation, formal analysis, writing—original draft, writing—reviewing and editing, visualization. H.O.: writing—review and editing, visualization. H.P.: methodology, validation. K.Y.W.: methodology, validation. J.W.: writing—review and editing, visualization, supervision. S.V.F.: conceptualization, writing—review and editing, supervision.
Disclosures
In 2023, J.B. received research support from the following sources: AACAP, Feinstein Institute for Medical Research, Genentech, Headspace, Inc., NIDA, Pfizer Pharmaceuticals, Roche TCRC, Inc., Sunovion Pharmaceuticals, Inc., Takeda/Shire Pharmaceuticals, Inc., Tris, and National Institutes of Health (NIH). J.B. and his program received royalties from a copyrighted rating scale used for ADHD diagnoses, paid by Biomarin, Bracket Global, Cogstate, Ingenix, Medavent Prophase, Shire/Takeda, Sunovion, and Theravance; these royalties were paid to the Department of Psychiatry at MGH. Through Partners Healthcare Innovation, J.B. had a partnership with MEMOTEXT to commercialize a digital health intervention to improve adherence in ADHD. Through MGH corporate licensing, J.B. held a U.S. Patent (No. 14/027,676) for a nonstimulant treatment for ADHD, a U.S. Patent (No. 10,245,271 B2) on a treatment of impaired cognitive flexibility, and a patent pending (No. 61/233,686) on a method to prevent stimulant abuse.
In 2022, J.B. received honoraria from UC Davis for Grand Rounds and the MGH Psychiatry Academy for tuition-funded CME courses. In 2021, J.B. received an honorarium for a scientific presentation from Multi-Health Systems, and a one-time consultation for Cowen Healthcare Investments. He received honoraria from AACAP, the American Psychiatric Nurses Association, BIAL—Portela & Ca. S.A. (Portugal), Medscape Education, and MGH Psychiatry Academy for tuition-funded CME courses. In 2020, J.B. received an honorarium for a scientific presentation from Tris and from the Institute of Integrated Sciences—INI (Brazil), and research support from the Food & Drug Administration. He received honoraria from Medlearning, Inc., NYU, and MGH Psychiatry Academy for tuition-funded CME courses.
J.W. receives research support from PCORI, Demarest Lloyd, Jr. Foundation, and the Baszucki Brain Research Fund. In the past, J.W. has received research support, consultation fees or speaker's fees from Eli Lilly, Janssen, Johnson and Johnson, McNeil, Merck/Schering-Plough, the National Institute of Mental Health (NIMH) of the NIH, Pfizer, and Shire. She is the author of the book, Is Your Child Bipolar published May 2008, Bantam Books. Her spouse receives royalties from UpToDate; consultation fees from Emalex, Noctrix, Disc Medicine, Avadel, HALEO, OrbiMed, and CVS; and research support from Merck, NeuroMetrix, American Regent, NIH, NIMH, the RLS Foundation, and the Baszucki Brain Research Fund. In the past, he has received honoraria, royalties, research support, consultation fees or speaker's fees from Otsuka, Cambridge University Press, Advance Medical, Arbor Pharmaceuticals, Axon Labs, Boehringer-Ingelheim, Cantor Colburn, Covance, Cephalon, Eli Lilly, FlexPharma, GlaxoSmithKline, Impax, Jazz Pharmaceuticals, King, Luitpold, Novartis, Neurogen, Novadel Pharma, Pfizer, Sanofi-Aventis, Sepracor, Sunovion, Takeda, UCB (Schwarz) Pharma, Wyeth, Xenoport, Zeo.
In the past year, S.V.F. received income, potential income, travel expenses continuing education support, and/or research support from Aardvark, Aardwolf, AIMH, Tris, Otsuka, Ironshore, Kanjo, Johnson & Johnson/Kenvue, KemPharm/Corium, Akili, Supernus, Atentiv, Noven, Sky Therapeutics, Axsome and Genomind. With his institution, he has U.S. patent US20130217707 A1 for the use of sodium-hydrogen exchange inhibitors in the treatment of ADHD. He also receives royalties from books published by Guilford Press: Straight Talk about Your Child's Mental Health, Oxford University Press: Schizophrenia: The Facts and Elsevier: ADHD: Non-Pharmacologic Interventions. He is Program Director of