
Abstract
Objectives:
Risperidone is commonly prescribed off-label in children and adolescents to manage disruptive behavior. This study aimed to investigate continued benefits of risperidone after at least 1 year of treatment and effects of discontinuation on physical health.
Methods:
Thirty-five youths (aged 6–18 years, intelligence quotient [IQ] >70) who were treated with risperidone for at least 1 year in regular clinical practice receiving outpatient care were randomly assigned to double-blind continuation of risperidone during 16 weeks or continuation for 2 weeks, gradual dose lowering over 6 weeks, and placebo for 8 weeks. Primary outcome was the total Disruptive Behavior (D-total) score of the parent-reported Nisonger Child Behavior Rating Form—Typical IQ (NCBRF-TIQ). Secondary outcome measures were the clinician-rated Clinical Global Impressions—Improvement scale (CGI-I), the parent, child, and teacher-rated Strengths and Difficulties Questionnaire (SDQ), the parent-rated Retrospective Modified Overt Aggression Scale (R-MOAS), and several health parameters (Udvalg for Kliniske Undersøgelser Side Effect Rating Scale [UKU-SERS], dyskinesia, akathisia, parkinsonism, body mass index (BMI), waist circumference, and laboratory outcomes). Mixed models for repeated measures were conducted for continuous outcomes and a chi-square test for the CGI-I.
Results:
Discontinuation of risperidone, as compared with continuation, was not associated with significant changes in parent-reported disruptive behaviors. However, discontinuation was related to significant deterioration in parent-rated verbal aggression, teacher-rated behavioral functioning, clinician-rated general functioning, and significant improvements in weight, BMI, waist circumference, and glucose, insulin, and prolactin levels. Although 56% of participants in the discontinuation group experienced relapse, causing premature withdrawal from the study, 44% was able to successfully discontinue risperidone.
Conclusion:
Discontinuation of risperidone was associated with deterioration on some, but not all behavioral measures according to this explorative study. Discontinuation was associated with important health gains. Despite long-term benefits of risperidone, attempts to withdraw risperidone should be undertaken in individual children. This is a crucial step in preventing harm and fostering health.
Introduction
Off-label prescription of risperidone in children and adolescents is common, mostly for the treatment of symptoms of irritability, aggression, or other disruptive behaviors and even attention-deficit/hyperactivity disorder (ADHD) or mood problems (Dinnissen et al., 2020; Rettew et al., 2015). Guidelines recommend prescription of risperidone for conduct problems after psychosocial therapy provided insufficient benefits (Gorman et al., 2015). In Europe, on-label pediatric prescription only constitutes the short-term treatment (up to 6 weeks) of persistent aggression in children with conduct disorder or mental retardation (European Medicines Agency, 2008).
However, risperidone is often being prescribed much longer than 6 weeks. A recent study reported that risperidone in children was prescribed for a period of 21 months on average, with a median of a little less than 12 months (Kloosterboer et al., 2018). We showed that 57.7% of children and adolescents largely recruited from outpatient clinics were still being treated with an antipsychotic prescribed for nonpsychotic target symptoms 3 years after initiation (Dinnissen et al., 2021). Male sex, age younger than 12 years, and presence of psychosis or autism spectrum disorders (ASD) and intellectual disabilities were identified as risk factor for higher duration of off-label antipsychotic treatment (Burcu et al., 2014; Kalverdijk et al., 2008; Kloosterboer et al., 2018).
Risperidone treatment is not without health hazards. It is associated with frequent occurrence of adverse effects, such as endocrine side effects (i.e., hyperprolactinemia), metabolic syndrome, weight gain, and diabetes, and also extrapyramidal symptoms and tardive dyskinesia, especially with longer duration of treatment (Bobo et al., 2013; Laita et al., 2007). Thus, substantial prevention of somatic complications can be achieved by minimizing unnecessary prescription of these medications.
Although the short-term efficacy of risperidone for irritability in ASD and disruptive behavior disorders has been studied quite extensively (Fung et al., 2016; Loy et al., 2017; Sochocky and Milin, 2013; van Schalkwyk et al., 2017), only few studies have targeted long-term efficacy and safety of risperidone in children and adolescents. In a naturalistic follow-up 21 months after initial entry into a placebo-controlled 8-week trial of risperidone for children and adolescents with ASD and severe irritability, on average, children who continued to be treated with risperidone scored better on behavioral and social measures, although their appetite and weight gain were higher than children who discontinued (Aman et al., 2015). Some studies into the long-term effectiveness of risperidone used a double-blind discontinuation design. For example, Reyes et al. (2006) studied risperidone treatment in 335 patients (5–17 years, intelligence quotient [IQ] >55) with disruptive behavior disorders.
Treatment in this study was divided into three phases: acute treatment (6 weeks of open-label risperidone), continuation treatment (6 weeks of single-blind risperidone), and maintenance (6 months of double-blind risperidone or placebo). During the maintenance phase, 52.9% of those who switched to placebo remained relapse-free for the following 6 months (as compared with 70.7% of those who continued on risperidone), suggesting that in many children and adolescents discontinuing risperidone does not lead to clinical relapse. A 1-year open-label extension of that study demonstrated continued treatment with risperidone was generally well tolerated and still had positive effects on disruptive behavior (Haas et al., 2008).
In a study of 32 children and adolescents with ASD, discontinuing risperidone after 24 weeks of treatment (8 weeks double-blind followed by 16 weeks open-label) led to rapid resurgence of aggression (five times as frequent as in continued treatment) (Research Units on Pediatric Psychopharmacology Autism Network, 2005). This implies that treatment for extended periods in this condition is often necessary in children with ASD. Troost et al. (2005) also conducted a placebo-controlled discontinuation trial of risperidone after 24 weeks of treatment, in 36 children with an ASD (5–17 years old) accompanied by severe tantrums, aggression, or self-injurious behavior. Continued treatment with risperidone was found to be superior to placebo in preventing relapse: this occurred in 3 of 12 patients (25%) continuing on risperidone versus 8 of 12 patients who had switched to placebo (66.7%).
Thus, these results indicate that many children with ASD and/or disruptive behavior benefit from risperidone in the long term, whereas in a portion risperidone may be discontinued without behavioral deterioration. Furthermore, discontinuation of risperidone has consistently been linked with considerable health gains such as reversal of weight gain and improvement on several other cardiometabolic outcomes, in both randomized (Research Units on Pediatric Psychopharmacology Autism Network, 2005; Reyes et al., 2006) and naturalistic studies (Aman et al., 2015; Calarge et al., 2014; Hulvershorn et al., 2017; Lindsay et al., 2004).
As previous randomized controlled studies have always been extension studies of clinical trials, the continued effectiveness of risperidone after long-term treatment in clinical practice still remains unclear. Ramerman et al. (2019) conducted a randomized, double-blind discontinuation study in a group of 25 children and adults with intellectual disabilities and challenging behaviors such as aggression, irritability, stereotypic behavior, or hyperactivity, who had been treated with risperidone in clinical practice for at least 1 year. In most individuals (82%), discontinuation was not associated with an increase in irritability compared with those continuing risperidone, whereas discontinuation was associated with beneficial effects on health parameters such as weight, waist circumference, body mass index (BMI), and prolactin and testosterone levels. No such placebo-controlled discontinuation studies have so far been conducted in children and adolescents without intellectual disabilities.
The primary objective of this study therefore, was to investigate the continued benefits of off-label risperidone for treatment of behavioral problems in children and adolescents without intellectual disability who had been on risperidone for at least 1 year. As secondary objectives, we investigated the effects of discontinuation on a range of behavioral measures and physical health parameters.
Methods
This study was a four-center randomized, double-blind, placebo-controlled discontinuation trial held over 16 weeks (Fig. 1), comparing the effects of continuation of risperidone to gradual tapering followed by complete discontinuation. If the clinical condition of a participant required the blind to be broken, further study participation ended. This study was approved by the Medical Ethical Committee of the University Medical Center Groningen (METc 2015/155) and was registered in The Netherlands National Trial Register (NTR5595).
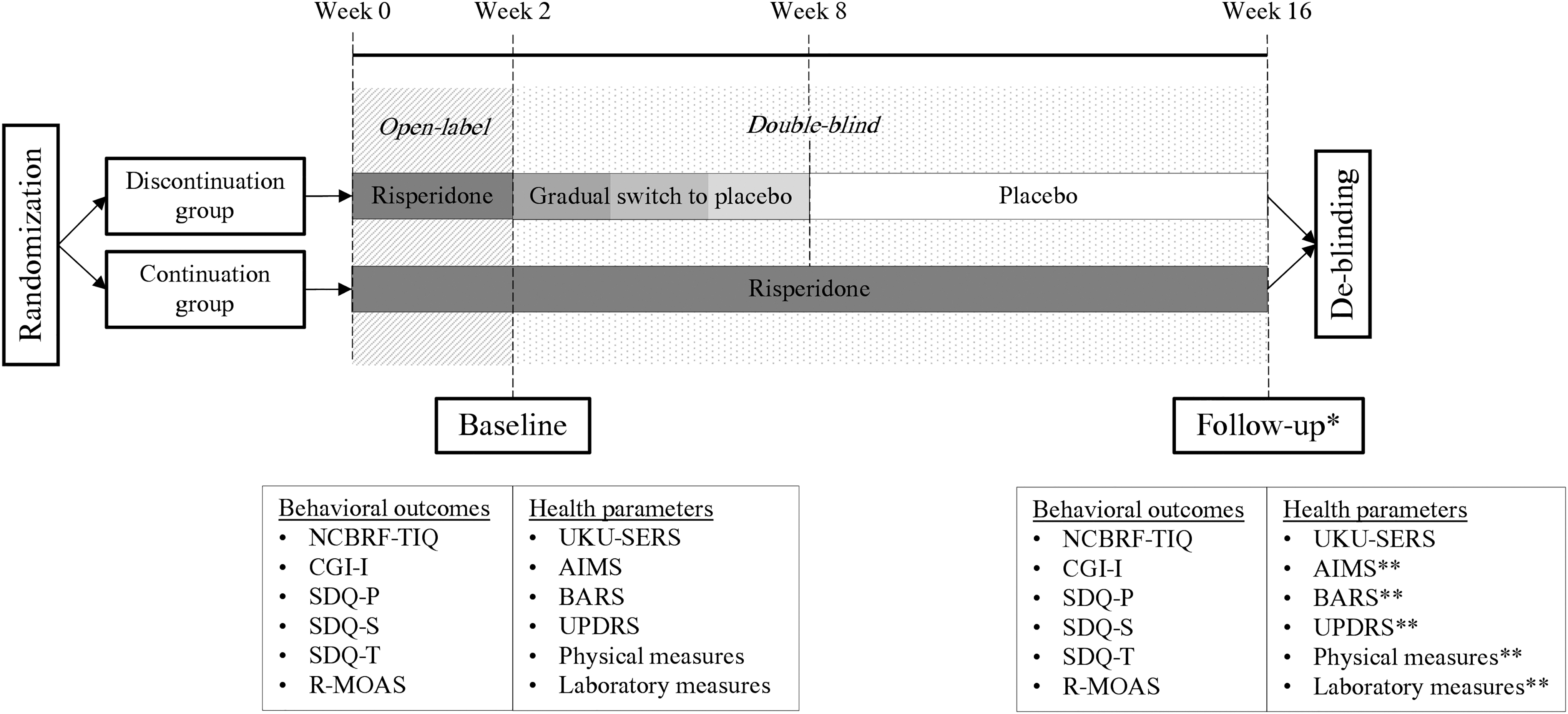
Study design of a randomized placebo-controlled discontinuation study of risperidone in children and adolescents. *If a participant prematurely stopped the study, follow-up measurements were done at dropout, before deblinding. **If a patient had already stopped taking the study medication at the time of the drop-out visit, this measure was omitted. AIMS, Abnormal Involuntary Movement Scale; BARS, Barnes Akathisia Scale; CGI-I, Clinical Global Impressions—Improvement scale; R-MOAS, Retrospective Modified Overt Aggression Scale; SDQ-P, parent-rated Strengths and Difficulties Questionnaire; SDQ-S, child-rated Strengths and Difficulties Questionnaire; SDQ-T, teacher-rated Strengths and Difficulties Questionnaire; UKU-SERS, Udvalg for Kliniske Undersøgelser Side Effects Rating Scale; UPDRS, unified Parkinson's disease rating scale.
Participants
We included children and adolescents between the ages of 6 and 18 years who had been treated with risperidone for at least 1 year at a maximum dose of 5 mg/day and had an IQ of 70 or higher (based on previous assessments or attending regular level education). Exclusion criteria were a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR; American Psychiatry Association, 2000) diagnosis of psychotic disorder, or if risperidone was primarily prescribed for the treatment of tics. Other psychiatric symptoms or diagnoses were not a reason for exclusion from this study. Participants were allowed to continue any comedication or psychosocial intervention they were being treated with before study initiation. If during the study changes in co-medication or psychosocial intervention were deemed essential by the clinician, these were allowed. Those participants could continue participating in the study and were included in the analyses. However, children who were planning to start a new psychosocial and/or any psychopharmacological therapy during the blinded period were encouraged to participate at a later time. Other reasons for exclusion included parents' inability to understand or comply with the protocol and any significant diseases that may have put the patient at risk or could influence the results of the study.
Participants were recruited from four Dutch organizations for child and adolescent psychiatry: Accare in the Northern, Karakter in the Eastern, GGZ Centraal in the Middle, and De Bascule in the Western parts of the Netherlands. Parents and children aged 12 years and older provided written informed consent. Children younger than 12 provided oral assent and if parents agreed to it, we also contacted children's primary teachers to obtain ratings.
Interventions
An overview of the study design is given in Figure 1. After obtaining informed consent, participants were randomized in a 1:1 ratio to either continued risperidone during 16 weeks, or to 2 weeks of their regular dose followed by gradual withdrawal to placebo over a 6-week period and 8 weeks of complete placebo. The dose reduction schedule was a function of dose at study entry, reduced by 25% each 2 weeks. Participants followed their regular schedule of taking medication. All study participants initially took their regular dosage of risperidone in the form of an oral solution of 1 mg/mL, which was dosed using a calibrated syringe. Participants then entered the double-blind phase and gradually switched to a second bottle of liquid in steps of 25% of their original dosage, which contained risperidone in the control group and placebo in the discontinuation group, identical in color, smell, and taste.
During the final 8 weeks, participants exclusively used the second bottle, and were therefore either fully discontinued or continued to take their original dose. To monitor adherence and prevent mistakes in administering the study medication, each participant received a personalized medication diary, specifying the daily amount of liquid to be taken from each bottle during participation. Each intake moment had to be checked off by the parent who administered the medication, any anomalies were noted in the diary.
Outcome measures
Outcome measures were collected at baseline, which took place right before starting the blinded phase and at 16 weeks (Fig. 1). If a participant prematurely stopped the study, measurements were done at dropout, after which deblinding took place. If patients had already stopped taking the study medication at the time of this visit, measurements were limited to rating behavioral outcome measures and the side-effect rating scale. Parent-rated measures were completed by both the primary parent (i.e., the parent who spends most time with the child) and if available a second parent. The score from the primary parent was used, but when missing it was replaced by ratings of the second parent. In addition, to investigate risperidone use after deblinding, parents were contacted by phone 6 months after the baseline assessment.
Behavioral outcomes
Disruptive problem behavior was the primary outcome measure as assessed by the total Disruptive Behavior (D-total) score of the parent-reported Nisonger Child Behavior Rating Form—Typical IQ (NCBRF-TIQ), calculated by adding the scores on the Conduct problems and the Oppositional behavior scale (Aman et al., 2008). This questionnaire measures the frequency of several disruptive behaviors over the past month.
Secondary behavioral outcome scales included the parent, child (11–17 years), and teacher-rated Strengths and Difficulties Questionnaire (SDQ), and the clinician-rated Clinical Global Impressions—Improvement scale (CGI-I). The SDQ is a widely used, brief screening questionnaire, aimed at identifying behavioral and emotional problems in children in the past 4 weeks. It contains five subscales; (1) Emotional symptoms, (2) Conduct problems, (3) Hyperactivity/inattention, (4) Peer relationship problems, and (5) Prosocial behavior (van Widenfelt et al., 2003). The CGI-I assesses how much the patient's symptoms have improved or worsened relative to baseline ranging from 1 = very much improved to 7 = very much worse (Guy, 1976b). Aggressive behavior was assessed by the parent-completed Retrospective Modified Overt Aggression Scale (R-MOAS), as adapted by Blader et al. (2009). Parents rate the frequency of 16 aggressive behaviors during the past week in 4 areas: verbal aggression; physical aggression toward others; aggression toward oneself; and destruction or hostile misuse of property.
Health parameters
The clinician-rated Udvalg for Kliniske Undersøgelser Side Effect Rating Scale (UKU-SERS-clin) includes 48 items measuring side effects on multiple domains in the past 3 days (Lingjaerde et al., 1987). It consists of subscales for psychic (e.g., concentration, memory, sleeping problems, and depression), neurological, autonomic, and other side effects (e.g., sexual side effects, headaches, rashes) that add up to a total score. Extrapyramidal side effects were additionally assessed with the Abnormal Involuntary Movement Scale (AIMS) (Guy, 1976a), The Barnes Akathisia Scale (BARS) (Barnes, 1989), and items 20, 21, 22, and 31 of the unified Parkinson's disease rating scale (UPDRS) (Fahn et al., 1987), as scored by the clinician.
Physical measures were performed by a trained study clinician and included length, weight, waist circumference, blood pressure, and pulse. Age-corrected body mass index (zBMI) was calculated, corrected for age based on Dutch reference values (Schonbeck et al., 2011). In addition, laboratory testing was carried out before each visit, including measurements of metabolism (fasting glucose, insulin, triglycerides, high-density lipoproteins [HDL], low-density lipoproteins [LDL], and total cholesterol), endocrine parameters (prolactin and testosterone), and thyroid function (TSH and T4).
Planned sample size
Previous studies of short-term risperidone in children and adolescents found effect sizes of 0.73–0.82 (Aman et al., 2002) on the NCBRF conduct scale in children with disruptive behavior disorders and subaverage IQ (35–84); large effect sizes (mean 0.9) on the NCBRF conduct scale in children with aggressive behavior (Pappadopulos et al., 2006; Snyder et al., 2002); and an effect size of 0.45 in children with ASD and disruptive behavioral symptoms (Shea et al., 2004). We therefore conservatively expected an effect size of 0.6 for this study.
Based on a repeated-measures t-test between 2 independent groups, with a power of 80% and an alpha of 0.05, we estimated that a sample size of 45 (90 total) in both the discontinuation and continuation group would be necessary to obtain an effect size of 0.6 (calculated with IBM SPSS SamplePower). The attrition rate from the total study was expected to be maximally 25%, resulting in a planned sample size at baseline of 60 participants in each group, that is, a total of 120 participants.
Randomization
Subjects were given a randomization number based on order of inclusion. The trial pharmacy dispensed study medication for either continued medication or gradual discontinuation according to a randomization list using block randomization of 4 to ensure even groups.
Statistical analysis
Mixed models for repeated measures were used to test the differences on continuous outcome measures between baseline and follow-up (16 weeks or study drop-out). Group (discontinuation or continuation) × time point (baseline and follow-up) was used as a fixed effect. An unstructured covariance matrix was used. Analyses were carried out on an intention-to-treat basis, meaning that in the case of study dropout, participants were included in the analyses using their ratings obtained at dropout. CGI-I ratings were dichotomized into worsened (much worse and very much worse) and not worsened (all other scores) and used in a chi-squared test to analyze differences between groups. The association between group and completion of the double-blind study period was tested using a chi-square test. Differences on baseline measures were tested by an independent t-test or a chi-squared test. Post hoc sensitivity analyses were conducted to assess the impact of baseline imbalances on behavioral outcome measures, by adding baseline scores as a covariate and fixed effect in the mixed models analyses. Analyses were performed using SPSS software version 26. The significance threshold for all analyses was a p-value of 0.05. Given the pilot nature of this study we did not correct for multiple testing. As a measure of effect size, we used Hedges' g. An effect size ∼0.20 is considered small, ∼0.50 medium, and >0.80 large.
Results
Flow of participants
The Consolidated Standards of Reporting Trials (CONSORT) diagram (Fig. 2) summarizes the flow of participants. Unfortunately, we encountered major recruitment difficulties and could not reach our planned sample size of n = 120. Of the 320 eligible patients, 35 were included in this study. Reasons for not participating included not wanting to discontinue risperidone because of fear of behavioral deterioration, wanting to discontinue immediately and therefore not wanting to be in the control group, not wanting the uncertainty of a double-blind study, feeling participation would be too much of a burden or time investment, and not wanting to switch to risperidone oral solution. In many cases, clinicians did not think patients were suitable owing to the nature of the problem behavior or contextual factors.

CONSORT flow diagram of participants in a randomized placebo-controlled discontinuation study of risperidone in children and adolescents. aNumbers of missing values and therefore numbers included in analyses varied across outcome measures and are reported in the results tables. Analyses were carried out on an intention-to-treat basis, meaning that participants who prematurely withdrew were included in the analyses using their ratings obtained at study dropout.
In the discontinuation group, 9 of 16 (56%) participants prematurely stopped the study, 4 of these stopped while only partially tapered and 5 after they had fully discontinued their medication. All the seven study participants from the discontinuation group who completed the study, remained off of risperidone even at the 6-month follow-up. In the continuation group, premature dropout was the case in 7 of 19 (37%) participants. The difference between both groups was not significant (Pearson χ 2 = 1.318, p = 0.251). However, the proportion of participants who prematurely stopped owing to behavioral deterioration was significantly higher in the discontinuation group (all 9 who dropped out; 100%) than in the continuation group (4 of 7 participants who dropped out; 57%; Pearson χ 2 = 4.75, p = 0.03). Other reasons for dropout in the continuation group were no longer being motivated to take the study medication (2 of 7 participants; 29%) and adverse effects, most likely owing to switching to the study medication which was an oral solution instead of tablets (1 of 7 participants; 14%). Participants in the discontinuation group dropped out on average 49.7 (standard deviation [SD] 19.54) days after the start of the double-blind phase, whereas in the continuation group this was after 29.7 (SD 18.6) days, which was not significantly different, likely because of the small sample size [t(13) = 1.98, p = 0.07]. One of the participants in the continuation group withdrew before starting the double-blind phase, and was therefore not included in the analyses.
Baseline characteristics
Table 1 describes the baseline characteristics of the discontinuation group and the continuation group. Groups did not differ on age, sex, total IQ, or risperidone dosage at study initiation. Dosing was in line with the Canadian guideline that recommends a daily dose of 0.5–1.5 mg/day for children with disruptive behavior problems (Gorman et al., 2015). None of the study participants were treated with anticholinergic medication. In the discontinuation group, there was a significantly higher percentage of treatment with melatonin (37.5% vs. 5.3% in the continuation group, χ 2 = 5.64, p = 0.018) and of children with a tic disorder (18.8% vs. 0% in the continuation group, χ 2 = 3.90, p = 0.048; note that risperidone was not prescribed for tics). In the continuation group, a significantly higher proportion of participants was diagnosed with ASD (94.7% vs. 68.8% in the discontinuation group, χ 2 = 4.13, p = 0.042).
Baseline Characteristics of Participants in a Randomized Placebo-Controlled Discontinuation Study of Long-Term (>1 Year) Risperidone Use in Children and Adolescents
p < 0.05.
DSM-IV-TR categorizations as derived from the medical records.
Tics were not allowed to be the primary reason for the risperidone treatment.
DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; IQ, intelligence quotient; NOS, not otherwise specified; SD, standard deviation.
With respect to the severity of baseline symptoms, participants in the discontinuation group scored significantly higher on the parent-rated SDQ subscales Conduct problems [t(31) = 3.29, p = 0.003] and Hyperactivity/inattention [t(31) = 2.22, p = 0.034], and the total SDQ score [t(31) = 3.11, p = 0.004], indicating more parent-reported problem behavior in this group at baseline. Child-reported total SDQ scores were also significantly higher in the discontinuation group [t(24) = 2.11, p = 0.045]. However, scores on the Nisonger D-total, R-MOAS, and other parent-rated SDQ subscales did not significantly differ between groups. Also, teacher-reported SDQ scores at baseline did not differ significantly between groups.
Behavioral outcomes
Table 2 provides results of the mixed-model analyses investigating group differences in change scores on the behavioral measures. To maintain conciseness, this table is limited to significant scores, in addition to total scores and the subscales that measure conduct problems. Full results are presented in Supplementary Table S1. The change score from baseline to follow-up on the parent-reported Nisonger D-total score, the primary outcome measure, did not differ between groups. All differences in parent-rated SDQ scores were nonsignificant as well. On the R-MOAS there was a significant increase in verbal aggression over time in the discontinuation group, as compared with the continuation group. Child-reported SDQ scores only revealed significant group differences in change scores on the prosocial scale, that is, children in the discontinuation group reported a decrease in prosocial behavior over time, whereas the continuation group on average scored higher at follow-up than at baseline.
Parent-, Child-, and Teacher-Reported Scores in Behavior in a Randomized Placebo-Controlled Discontinuation Study of Long-Term Risperidone Use (>1 Year) in Children and Adolescents
Table 2 reports all scales on which the change score differed significantly between the continuation and discontinuation group across 16 weeks, in addition to all total scores and scores on subscales focusing on conduct problems. Full results are given in Supplementary Table S1.
Difference (Δ) in mean change from baseline to follow-up between the discontinued and continued treatment groups, by mixed models for repeated measurements analysis.
Sensitivity analyses including the baseline score as a covariate, to control for baseline differences on this variable, did not alter the significance of our results. Table 2 therefore reports the results of the originally planned analyses without including baseline scores as a covariate.
p < 0.05.
CI, confidence interval; D-total, total Disruptive Behavior; R-MOAS, Retrospective Modified Overt Aggression Scale; SDQ, Strengths and Difficulties Questionnaire; SDQ-P, parent-rated Strengths and Difficulties Questionnaire; SDQ-S, child-rated Strengths and Difficulties Questionnaire; SDQ-T, teacher-rated Strengths and Difficulties Questionnaire.
Changes on the teacher-reported SDQ differed significantly between groups on the subscales for emotional problems, conduct problems, peer relationship problems, and on the total score, all indicating worse behavioral outcomes over time in the discontinuation group, as compared with the continuation group. Effect sizes were all in the large range (Table 2). To assess the impact of the baseline differences on the Conduct problems and Hyperactivity/inattention subscales and the total score on the parent-rated SDQ and the total score on the child-reported SDQ on effect estimates, we conducted sensitivity analyses including the baseline score as a covariate in the mixed models analyses. Results of the analyses remained robust. Table 2 therefore reports the results of our originally planned analyses without including baseline scores as a covariate.
As described in Table 3, clinician-rated CGI-I scores indicated a significantly worsened overall functioning at follow-up in 31.3% of the participants in the discontinuation group, compared with 6.7% in the continuation group.
Clinician-Rated Clinical Global Impressions Improvement Scale in a Randomized Placebo-Controlled Discontinuation Study of Long-Term (>1 Year) Risperidone Use in Children and Adolescents
p < 0.05.
CGI-I, Clinical Global Impressions—Improvement scale.
Health parameters
Table 4 reports group differences in changes over time on a number of health parameters, clinician-rated health problems, and laboratory measures. As compared with the control group, individuals who discontinued risperidone had a significant increase in dyskinesia (medium effect size) and a significant decrease in body weight, age-corrected BMI, and waist circumference (large effect sizes). Regarding laboratory measures, the discontinuation group showed a significant decrease in glucose, prolactin, and insulin levels (large effect sizes).
Changes in Health Parameters, Clinician-Rated Health Problems, and Laboratory Parameters in a Randomized Placebo-Controlled Discontinuation Study of Long-Term (>1 Year) Risperidone Use in Children and Adolescents
Difference (Δ) in mean change from baseline to follow-up between the discontinued and continued treatment groups across 16 weeks, by mixed models for repeated measurements analysis.
p < 0.05.
Continuation group: n = 14.
Clinician-rated health problems were measured with the UKU Side Effect Rating Scale.
p < 0.01.
This subscale includes a number of sexual side effects, headaches, and rashes.
AIMS, Abnormal Involuntary Movement Scale; BARS, Barnes Akathisia Scale; CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein; UKU-SERS, Udvalg for Kliniske Undersøgelser Side Effects Rating Scale; UPDRS, unified Parkinson's disease rating scale; zBMI, age-corrected body mass index.
Discussion
This randomized, placebo-controlled discontinuation study aimed to investigate the continued effectiveness of risperidone in children and adolescents beyond 1 year of treatment by comparing gradual discontinuation with placebo across 16 weeks. Although the target number of participants was unfortunately not obtained, some tentative, yet clinically relevant conclusions can be drawn from our results. As compared with continuing risperidone, discontinuation was not associated with significant changes on the primary outcome, measuring parent-rated behavioral problems. However, on a group level, discontinuation was associated with a significant and strong deterioration in parent-rated verbal aggression, child-rated prosocial behaviors, teacher-rated total behavioral problems and emotional, conduct, and peer relationship problems, and clinician-rated overall functioning. Conversely to this behavioral deterioration in multiple areas, discontinuation also led to strong improvements in weight, BMI, waist circumference, and glucose, insulin, and prolactin levels.
At the same time, some health-related measures worsened; significant increases in total clinician-rated health problems were observed in the discontinuation group, as compared with the continuation group, and specifically increased psychic (i.e., problems related to concentration, memory, and sleeping or depression), neurological, and other health problems (e.g., sexual side effects, headaches, rashes). An increase in dyskinesia was also reported in the discontinuation group, as observed by the clinician. These increases may indicate withdrawal effects, which would be expected especially regarding extrapyramidal symptoms.
Teachers reported significant deterioration in the discontinuation group over time as compared with the continuation group on several behavioral measures, whereas differences on parent- and child-reported scales were mostly nonsignificant. Teachers generally appear the most sensitive raters of medication effects on behavioral functioning (Schachter et al., 2001) and generally report a low placebo response (Antrop et al., 2002; Fageera et al., 2018).
Although tentative, findings of this study are consistent with previous studies, which found that discontinuation of risperidone in children and adolescents was associated with increases on measures of behavioral problems (Research Units on Pediatric Psychopharmacology Autism Network, 2005) and higher relapse rates (Reyes et al., 2006; Troost et al., 2005) than continuation of risperidone, whereas at the same time discontinuation was also associated with important health gains. Of interest, however, is that in all studies, including our study, a subgroup (44%) of patients were able to successfully discontinue risperidone and have not needed to restart risperidone for at least 20 weeks after discontinuation. This highlights the importance of regularly attempting to discontinue risperidone in clinical practice. Our study unfortunately did not have enough power to conduct analyses on predictors of the effects or feasibility of discontinuation.
This study should be interpreted in light of its strengths and limitations. To our knowledge, this study was the first to investigate long-term efficacy of risperidone in a group of children and adolescents who had been treated with risperidone for at least 1 year in regular clinical practice, all from an outpatient setting. The most obvious limitation is the low sample size, although we believe we still obtained meaningful results given the large effect sizes. In addition, there was a substantial amount of missing data on parent, child, and teacher-completed questionnaires, which may have been a source of bias in the results. Because of the explorative nature of this study, we did not correct for multiple testing, which increases the chance of false-positive findings, yet the effects were in the expected direction.
Furthermore, selection bias may have affected results and possibly compromised the external validity of the study; many patients did not want to discontinue treatment with risperidone and did thus not participate, whereas others wanted to start discontinuation right away and were therefore opposed to randomization. Despite these limitations, results of this study are in line with previous studies and highlight the feasibility and health benefits of discontinuation of risperidone after long-term treatment in a considerable proportion of patients.
Conclusions
In conclusion, this double-blind, placebo-controlled discontinuation study of risperidone after at least 1 year of treatment in children and adolescents without intellectual disabilities found increases in some measures of problem behavior associated with discontinuation. This suggests a beneficial effect of long-term treatment with risperidone. At the same time, discontinuation was associated with improvements on cardiometabolic outcomes and prolactin levels, indicating important health gains. About half of the participants who discontinued risperidone experienced relapse causing premature withdrawal from the study, but 44% were able to successfully discontinue risperidone. This is important, especially given the reluctance among clinicians, patients, and their parents to attempt discontinuation. Clinical practice could benefit greatly from larger studies looking into patient characteristics that could be predictive of successful discontinuation, such as psychiatric diagnosis, age or family context, or into the kind of support needed for patients and their parents to feel more confident in attempting discontinuation.
Clinical Significance
This double-blind, placebo-controlled discontinuation study suggests that discontinuation of risperidone after treatment for over 1 year is feasible in many, yet not all children. Discontinuation is not always associated with behavioral deterioration, and significant health gains may be obtained. This study highlights the importance of attempting at least temporary discontinuation of risperidone in children after long-term treatment, to monitor its harms and benefits as is recommended by clinical guidelines.
Footnotes
Disclosures
J.K.B. has been in the past 3 years a consultant to/member of advisory board of/and/or speaker for Janssen Cilag BV, Eli Lilly, Lundbeck, Takeda/Shire, Roche, Medice, and Servier. He is not an employee of any of these companies, and not a stock shareholder of any of these companies. He has no other financial or material support, including expert testimony, patents, and royalties. The other authors have no conflicts of interest relevant to this article to disclose.
Acknowledgments
The authors thank all participating organizations and trained study clinicians for their contributions to the recruitment and data collection for this study. Furthermore, this project would not have been possible without all participants and their parents. Preliminary results were presented at the ESCAP 19th International Congress 2022 in Maastricht, the Netherlands, June 20, 2022 (![]() ).
).
Authors' Contributions
A.D., B.J.H., Y.R., P.W.T., J.K.B., and P.J.H. contributed to conceptualization, methodology, and funding acquisition for this study. M.D. contributed to methodology and was in charge of database and software design, coordination of the study, project administration, data curation, statistical analysis, and writing the first draft, under supervision of and with review and editing by A.D. and P.J.H. M.B., J.H.M., A.M.V., and W.A.O. contributed to investigation and project administration. All authors approved the final article and agreed to be accountable for all aspects of the study.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.