
Abstract
Background:
Previous studies suggest that selective serotonin reuptake inhibitors (SSRIs) may increase the risk of suicide among children and youth, although the association between suicide risk and the combination of SSRIs with other medication such as stimulants in this population remains unclear. This study explored whether the combination of SSRIs with stimulants influenced suicide risk.
Methods:
A retrospective cohort study was conducted at a single children's hospital campus-based ambulatory psychiatric clinic between September 1, 2017, and September 30, 2020. Subjects were 6–21 years of age and prescribed either stimulants or stimulants and SSRIs only. The primary outcome was suicidal thoughts and behaviors (STB), defined by documented suicidal thoughts, plans, or behaviors. Firth logistic regression evaluated associations between medication class and STB.
Results:
Among 349 patients, the prevalence of STB was 5.7% (n = 20). In unadjusted model, patients prescribed SSRIs and stimulants had a 2.9-fold increase of STB compared to patients prescribed stimulants only, along with increasing age, male sex, and the diagnoses of anxiety and/or depression. In the final model adjusted for each of these factors, the observed association of medication regiment with STB was attenuated (odds ratio [OR]: 1.3, confidence interval [CI]: 0.3–4.9, p = 0.7). The magnitude of the adjusted association between depressive diagnosis and STB was notable (OR: 3.6, CI: 1.0–12.6, p = 0.049).
Conclusions:
Among patients followed in a children's hospital-based ambulatory psychiatric clinic, a combination medication regimen of SSRIs and stimulants after adjusting for genetic sex, age, anxiety diagnosis, and depression diagnosis, the observed association between STB and combination stimulant and SSRI treatment was attenuated. This finding suggests that other factors, including depression, may have contributed to the association between SSRI treatment and STB. Larger, prospective studies of the relationship between combination pharmacotherapy and suicide risk are warranted to guide clinical/pharmacological decision making and to better clarify these relationships.
Introduction
Suicide has ranked as the second leading cause of death in children and young adults, 10 to 24 years of age, in the United States since 2012 (CDC, 2022b). Previous studies have identified that adolescent males who are depressed and have previously attempted suicide are at greatest risk for suicide (Shaffer, 1988).
According to the Youth Risk Behavior Survey conducted by the Centers for Disease Control (CDC, 2022a), there has been a 25% increase since 2007 to 2017 in the number of high school students who report seriously considering a suicide attempt (Kann et al., 2018). Risk factors for suicide in the child and adolescent population include various psychiatric diagnoses (e.g., depression, anxiety, bipolar, posttraumatic stress disorder, substance use disorders, psychotic disorders), alcohol and drug abuse, family history of suicide, and identifying as lesbian, gay, bisexual, transgender, queer, and/or questioning (Beautrais, 2000; Brent et al., 1993; Dilillo et al., 2015; Greydanus and Calles, 2007).
Although some risk factors for suicidal thoughts and behaviors (STB) have been identified, the role of various medication in suicide risk is less clear. For example, in 2004, the Food and Drug Administration (FDA) began to require a boxed warning, the highest warning for safety, for STB on selective serotonin reuptake inhibitor (SSRI) medication. The warning states that SSRI use is associated with an increased risk for STB in children and adolescents. This warning was further extended to include young adults up to 24 years of age (Khan et al., 2003).
Subsequently, SSRI prescription rates by clinicians (i.e., pediatricians and family practice physicians) declined, while suicide completion increased in the pediatric population (Gibbons et al., 2007; Rushton et al., 2000). Since the boxed warnings were issued in 2004, results from pediatric studies have not provided clarity on the association between suicide risk and SSRI medication use (Khan et al., 2003). Given that untreated depressive and anxiety disorders are significant risk factors for suicide attempts and completions in the pediatric population (Brent et al., 1993), clinicians remain challenged by a boxed warning for SSRIs, the best available evidence-based medication for these disorders.
The relationship between suicide risk and the use of stimulants such as methylphenidate has also been of interest (McCarthy et al., 2009). Available studies have demonstrated an increased risk of suicide in association with untreated attention-deficit/hyperactivity disorder (ADHD) rather than with the use of methylphenidate (Man et al., 2017). Because stimulants and SSRIs are commonly used together to treat depressive and/or anxiety disorders co-occurring with ADHD, the primary objective of this study was to assess the prevalence of STB in pediatric patients prescribed stimulant medication, only to those prescribed a combination of stimulant and SSRI medication. We evaluated the adjusted association between STB and the combination SSRI and stimulant pharmacotherapy after consideration of other potentially contributory factors such as gender, age, and psychiatric diagnoses. We hypothesized that combination treatment with SSRIs and stimulants was associated with an increased prevalence of STB.
Methods
Study population
A retrospective cohort of pediatric patients was defined based on age and medication of interest from Johns Hopkins All Children's Hospital (JHACH) ambulatory psychiatric clinic from September 1, 2017, to September 30, 2020. Data analysts from the JHACH Clinical Research Data Acquisition Shared Resource queried the Cerner Electronic Health Record (EHR) database from September 1, 2017, to September 30, 2020, to identify clinic patients actively taking prescribed stimulants alone or in combination with SSRIs. Patients were confirmed to have a minimum of two documented visits at JHACH, at which either stimulant medication use or a combination of stimulant plus SSRI medication use was documented.
Medication applied in the stimulant search were methylphenidate derivatives (i.e., methylphenidate, dexmethylphenidate) and amphetamine derivatives (i.e., mixed amphetamine salts, amphetamine sulfate, dextroamphetamine, and lisdexamfetamine), while SSRI search terms included citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline. EHR manual review was used to validate data on medication administration and adherence, and to extract outcomes and covariate data. Patients younger than 6 years and older than 21 years were excluded from the study, as were patients prescribed psychiatric medication other than stimulants and SSRIs. The JHACH Institutional Review Board approved this study with a waiver of consent.
Outcomes
STB, the primary study outcome, were ascertained using EHR data. A dichotomous variable was created to indicate the documented presence of at least one suicidal thought, plan, or behavior (i.e., self-injurious behaviors with suicidal intent) on or after the first active clinical visit, defined as the first clinical encounter in which medication was documented and/or prescribed within the study time period. In keeping with the Columbia Suicide Severity Rating Scale (Interian et al., 2018), suicidal thoughts were defined as thoughts to harm oneself with the intention to kill oneself. Suicidal plans were defined as plans to harm oneself with the intention to kill oneself, and suicidal behavior was defined as actions taken toward oneself with the intention to kill oneself.
Assessment of medication regimen
The primary exposure of interest was medication regimen; a dichotomous variable was created to classify patients according to whether they were prescribed stimulants only or a combination of SSRIs and stimulants. Given that patients had multiple visits, exposure status was classified based on the first active clinical visit, as described above. Manual chart review was performed to minimize misclassification bias of the primary exposure. A list of SSRIs and stimulants included in the study is provided in Appendix Table A1.
Other parameters of interest
Parameters of interest included genetic sex (male/female), age in years at the first active clinical visit, psychiatric diagnosis (i.e., ADHD, anxiety, depression, other), family history of suicide, chronic medical conditions, concerns with sexual identity, and any prior suicide attempt. Charts were reviewed for documentation of chronic medical illnesses, including medical diagnosis for pulmonary diseases, allergies, migraines, dermatological conditions, pain conditions, malignancies, and cardiovascular diseases, as all these have demonstrated associations with STB in prior research. Given that some variables were collected only for new patients, an additional category was reported for pertinent variables to indicate patient data that were derived only from new patient psychiatric evaluations.
Statistical analyses
Continuous and categorical variables were summarized with medians and interquartile ranges (IQRs), as well as counts and percentages, respectively. The association between medication regimen and STB was evaluated with univariable and multivariable Firth logistic regression. This type of regression is a penalized likelihood method demonstrated to reduce bias in estimates from models exhibiting full or quasi-separation and/or rare outcomes (Firth, 1993). A core set of covariates was preselected based on available variables we believed to influence STB in this setting, and/or variables that had been demonstrated to be associated with STB in prior research. To avoid omitted variable bias, we tested additional variables (i.e., other psychiatric diagnosis, current medical conditions) for inclusion into the model based on improvement to model fit, measured by the Akaike information criterion (AIC).
Covariates were excluded outright from the model if they lacked sufficient variability (i.e., ADHD diagnosis, concerns with sexual identity) or were collected only from new patients (i.e., family history of suicide, prior suicide attempt). Crude and covariate-adjusted odds ratios (ORs) were calculated with 95% confidence intervals (CIs). A complete case analysis was performed; missing data were not imputed. With a total sample of 349 patients, the study was powered to detect a 30% difference between groups in prevalence of STB at a significance level of 0.05, which equated to an OR of 4.0. Two-sided p-values <0.05 were considered statistically significant for the final adjusted model. A statistical code check was performed by an independent epidemiologist. All analyses were conducted with Stata S/E Version 17.1 (StataCorp., 2021, Stata Statistical Software: Release 17; StataCorp LLC, College Station, TX, USA).
Results
Figure 1 shows how the sample (n = 349) was derived. Reasons for exclusion included: age younger than 6 years or older than 21 years; concomitant use of additional psychiatric medication other than SSRIs and stimulants; STB before beginning the medication of interest; and lack of follow-up after the initial evaluation.
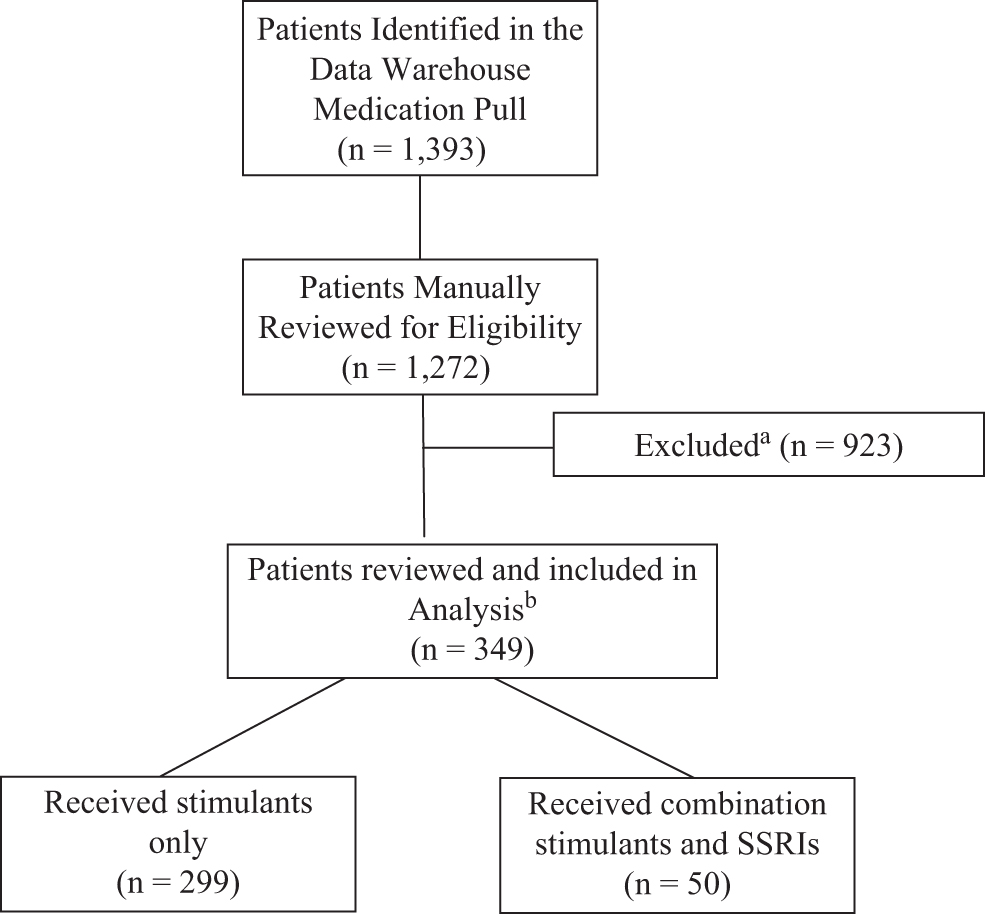
CONSORT flow diagram of patients. aReasons for exclusion include the following: Patients <6 or >21 years of age, concomitant use of additional medication, in addition to SSRIs and psychostimulants, suicidal thoughts and behaviors before beginning medication, and patients with an initial evaluation without follow-up. bThe total patients included reflect a final study population, which was optimally powered for analysis. CONSORT, Consolidated Standards for Reporting Trials; SSRIs, selective serotonin reuptake inhibitors.
Characteristics of the study population
Table 1 presents patient demographic and clinical characteristics according to STB, as defined by the study. The overall prevalence of STB was 5.7% (n = 20). Most study subjects were prescribed stimulants (85.7%, n = 299), whereas 14.3% (n = 50) were prescribed SSRIs and stimulants combined. The median age at the first clinical visit was 13.6 years (IQR: 10.2–16.0 years). Sixty-three percent of the study population was male (n = 221).
Patient Demographic and Clinical Characteristics By Suicidal Thoughts and Behaviors
ADHD, attention-deficit/hyperactivity disorder; IQR, interquartile range; SSRIs, selective serotonin reuptake inhibitors; STB, suicidal thoughts and behaviors.
Nearly all patients had a recorded diagnosis of ADHD (99.7%, n = 348), 21.2% of patients (n = 74) were diagnosed with an anxiety disorder, and 7.5% (n = 26) were diagnosed with a depressive disorder. Among patients with STB, 35.0% (n = 7) had an anxiety diagnosis and 25.0% (n = 5) had a depressive disorder. Other psychiatric diagnoses were noted in 35.0% (n = 7), including autism spectrum disorder (n = 2), disruptive mood dysregulation disorder (n = 1), dysthymia (n = 2), and oppositional defiant disorder (n = 2). Among new patients with STB, there was no report of previous suicide attempts or family history of suicide.
Univariable analyses
As seen in Table 2, we observed a crude association between medication regimen and STB, whereby patients prescribed SSRIs and stimulants had a 2.9-fold increase of STB compared to patients prescribed stimulants only (Crude OR: 2.9, 95% CI: 1.1–7.6, p = 0.03). We also found that having a depression diagnosis was associated with odds of STB (Crude OR: 5.1, CI: 1.8–14.8, p = 0.003). None of the other covariates reached the a priori level of significance (see Methods section) for putative associations with STB.
Associations Between Medication Regimen and Suicidal Thoughts and Behaviors
p = 0.049, rounded to 0.05 for clarity of presentation.
Model 1 adjusted for age at first active clinical visit, genetic sex, anxiety diagnosis, and depression diagnosis.
Model 2 adjusted for covariates in Model 1, as well as other psychiatric diagnosis and current chronic medical conditions.
n = 328 for crude model of genetic sex and STB.
CI, confidence interval; OR, odds ratio.
Multivariable analyses
The best-fit multivariable model, referred to as “Model 1” in Table 2, included our a priori selected set of covariates (first active clinical visit in years, genetic sex, anxiety diagnosis, and depression diagnosis). The AIC for Model 1 was 144.0, whereas the AIC for Model 2, which included two additional covariates (other psychiatric diagnosis and current medical conditions), was 144.2. In the final multivariable model (Model 1), the observed association of medication regimen with STB was attenuated (OR: 1.3, CI: 0.3–4.9, p = 0.7). The magnitude of the adjusted associated between depression diagnosis and STB was notable (OR: 3.6, CI: 1.0–12.6, p = 0.049). We did not observe any other significant adjusted association (p > 0.05 for all).
Discussion
This study assessed the association between STB, stimulants, and the combination of stimulants with SSRIs in children and adolescents. We found that 12.0% (6/50) of subjects treated with both stimulants and SSRIs had STB compared to 4.7% (14/299) of those prescribed stimulant medication only. In the crude model, patients treated with both SSRIs and stimulants had a 2.9-fold increase of STB compared with those on only stimulants. Notably, after adjusting for genetic sex, age, anxiety diagnosis, and depression diagnosis, the observed association between STB and combination stimulant and SSRI treatment was attenuated. This finding suggests that other factors, including depression, may have contributed to the association between SSRI treatment and STB.
To our knowledge, this is one of the first studies to examine the association between combination stimulant and SSRI medication treatments and STB in children and adolescents. Previous studies of suicide risk and psychoactive medication have largely focused on the SSRI medication class, especially following the FDA analysis of pediatric antidepressant medication trials that lead to the imposition of a boxed warning in 2004. Since that time, studies about the risk of SSRI medication contributing to STB have generated mixed results, along with confusion among pediatric clinicians. Because the use of medication combinations such as SSRIs and stimulants is quite common, it is important to clarify whether specific medication combinations might increase the risk of suicide. Somewhat reassuringly, this relatively small study did not find an adjusted association of stimulants alone or stimulants in combination with SSRIs with STB.
There were several strengths of this study. All patients included in the analytic sample were manually confirmed for medication prescriptions (stimulants or SSRI and stimulants), along with diagnoses, age, and all other variables of interest. In addition, the single-center nature of this study allowed for mitigation of potential bias due to differences in prescribing habits, and treatment thresholds from different clinicians across several health centers.
Study limitations include its retrospective nature, based on clinical chart review rather than prospective data. Heterogeneous suicide risk factors may have been inconsistently recorded in the EHR. While we attempted to measure all relevant suicide risk factors within this age group, omitted variable bias is possible. The study may have been underpowered with relatively small sample size. Variables such as history of family suicidal and prior suicide attempt were only evaluated in new patient evaluations; thus, no new patient evaluation before the study period was feasible because of the institutional change in EHR managing software. Because the study was powered to detect a 30% difference in prevalence for STB between the two treatment regimens of interest, it is possible that more subtle differences exist and were not able to be detected.
Notwithstanding these limitations, these findings warrant further investigation in larger, prospective cohort studies. Future studies should continue to examine the relationship between various combinations of psychopharmacologic agents and STB in pediatric and young adult populations where suicide remains among the leading causes of death in the United States.
Conclusion
This study aimed to clarify the risk of suicidal thoughts and behaviors with combination of SSRI and stimulant medications. In the crude model, results revealed patients treated with both SSRIs and stimulants had a 2.9-fold increase in suicidal thoughts and behaviors compared to those treated with only stimulants. After adjusting for confounding factors such as genetic sex, age, and psychiatric diagnoses, the observed association was attenuated. This suggests that factors other than medications may be contributory.
Clinical Significance
It is important to clarify risks of suicidal thoughts and behaviors from psychotropic medications given that SSRI medications have FDA indications for anxiety and depression diagnoses while having highest warning of safety for suicidal thoughts and behaviors. This study attempted to clarify such risk by exploring whether combination of SSRIs and stimulants influence the risk of suicidal thoughts and behaviors. Results revealed that other factors such as depression diagnosis may be contributing to the suicidal thoughts and behaviors. It is important to continue to examine the role of psychotropics in suicidal thoughts and behaviors as suicide remains the leading cause of death among pediatric and young adult populations.
Footnotes
Acknowledgments
The authors express appreciation to Sharon Ghazarian, PhD, for her guidance with statistical analysis design. We would also like to acknowledge John V, Campo, MD, for his substantive review and comments on the article.
Disclosures
The authors have no disclosures to make.
Appendix
Compiled List of Medication Prescribed to Patients in the Analytic Sample
| Stimulant: | |
|---|---|
| Amphetamine derivatives | Methylphenidate derivatives |
| Adderall XR | Aptensio XR |
| Adzenys XR-ODT | Concerta |
| Dexedrine Spansule | Cotempla XR-ODT |
| Dyanavel XR | Daytrana |
| Evekeo | Focalin |
| Mydayis | Focalin XR |
| Vyvanse Capsule | Jornay |
| Vyvanse Chewable | Metadate CD |
| Quillichew ER | |
| Quillivant XR | |
| Ritalin LA | |
| Ritalin |
| SSRI: | |
|---|---|
| Citalopram | |
| Escitalopram | |
| Fluoxetine | |
| Sertraline | |
| Fluvoxamine | |
| Paroxetine |