
Abstract
Study Design:
Retrospective case series.
Objectives:
The objective of this study was to provide naturalistic data on the use of guanfacine for the treatment of attention-deficit/hyperactivity disorder (ADHD) in a clinically referred sample of youth with Down syndrome (DS).
Methods:
The medical records of children and adolescents with DS who received guanfacine for the treatment of ADHD from a multidisciplinary neurodevelopmental disorder clinic between September 1, 2011, and September 10, 2021, were reviewed. Demographic and clinical characteristics, guanfacine dose and treatment duration, and adverse effects were recorded. Clinical Global Impression Scale (CGI) scores for ADHD symptom severity (S) and improvement (I) were retrospectively assigned by a child and adolescent psychiatrist based on review of the clinic notes. Response to guanfacine was defined as completion of at least 12 weeks of treatment and a Clinical Global Impression Improvement subscale rating ≤2 (1 = “very much improved” or 2 = “much improved”).
Results:
Twenty-one patients were eligible for inclusion, of whom 17 (81%) completed at least 12 weeks of guanfacine. Ten of the 21 patients (48%; 95% confidence interval [CI]: 28%–68%) responded to treatment. The median time on guanfacine treatment covered by the clinic notes was 50.4 weeks, with a range of 0.3 weeks to 7.5 years. Thirteen patients (62%) remained on guanfacine at the time of their most recent clinic note. Nine patients had adverse events documented in their clinic notes (43%; 95% CI: 24%–63%), most commonly sleepiness (n = 7) and constipation (n = 2).
Conclusion:
About half of patients with DS responded to guanfacine for the treatment of ADHD and many tolerated long-term use. Study limitations primarily relate to the retrospective nature of the study and small sample size.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder characterized by a persistent pattern of inattention and/or hyperactivity and impulsivity that interferes with functioning or development. The global point prevalence of childhood ADHD is estimated to be around 5%, with community estimates ranging from 2% to 7% (Sayal et al., 2018). Untreated ADHD is associated with poorer academic performance, motor vehicle accidents, substance use, antisocial behaviors, obesity, and lower self-esteem (Shaw et al., 2012). The American Academy of Pediatrics 2019 Clinical Practice Guideline for the Treatment of ADHD in Children and Adolescents supports the use of medications for the treatment of ADHD (grade A: strong recommendation), with the strongest evidence for stimulant (amphetamine or methylphenidate) medications as well as sufficient but less-strong evidence for atomoxetine (a selective norepinephrine reuptake inhibitor), guanfacine (a selective α-2 adrenergic agonist), and clonidine (also a selective α-2 adrenergic agonist) (Wolraich et al., 2019).
Down syndrome (DS), also known as trisomy 21, is among the most common chromosomal disorders and is caused by a complete or partial extra copy of chromosome 21. Clinical presentations of DS vary but often include characteristic facial features, hypotonia, cardiovascular and congenital heart disease, short stature, and neuropsychiatric comorbidities, including but not limited to ADHD, intellectual disability (ID), autism spectrum disorder (ASD), and dementia (Antonarakis et al., 2020; Santoro et al., 2020). Youth with DS are at increased risk for ADHD compared with the general population, with estimates as high as nearly 45% (Ekstein et al., 2011). Beyond the negative consequences of ADHD in the general population reviewed above, untreated ADHD in youth with DS interferes with participation in special education, behavioral therapies, and socialization, thereby limiting developmental progress (Capone et al., 2006; Pueschel et al., 2008). Furthermore, hyperactivity and impulsivity pose significant safety risks to youth with DS and ADHD, leading to behaviors such as elopement and accidents (Capone et al., 2006).
To date, the literature on pharmacotherapy for ADHD in DS is limited to two small studies: one prospective, open-label trial of guanfacine in 23 children (Capone et al., 2016) and one retrospective study of methylphenidate in 21 children (Roche et al., 2021). The prospective guanfacine trial demonstrated benefit on the Hyperactivity and Irritability subscales of the Aberrant Behavior Checklist (ABC) and was well-tolerated overall (Capone et al., 2016). In the retrospective methylphenidate study, 16 of the 21 (76%) children included showed improvement in attention/concentration and hyperactivity/impulsivity as judged by the child's parents/educators without the use of standardized rating scales (Roche et al., 2021). Twelve (57%) children experienced adverse effects (AEs). These were severe enough to prompt treatment discontinuation in 3 (14%) children.
Expert opinion has proposed the use of guanfacine, a nonstimulant medication with Food and Drug Administration (FDA) approval for the treatment of ADHD in children aged 6–17 years, as the first-line treatment for ADHD in DS (Palumbo and McDougle, 2018). It works via agonism of postsynaptic α2-adrenergic receptors, which, in the prefrontal cortex, may lead to enhanced norepinephrine signaling, thereby improving executive function (Arnsten 2020). Guanfacine is generally well-tolerated and side effects tend to be dose-dependent, most commonly including somnolence, sedation, headache, hypotension, and dizziness (Childress et al., 2020).
To date, evidence supporting clinical decision-making for the treatment of ADHD in youth with DS remains limited. The primary purpose of this retrospective study is to provide preliminary naturalistic data on the use of guanfacine for the treatment of ADHD in a clinically referred sample of youth with DS.
Materials and Methods
Study participants
The study was approved as exempt by the local institutional review board (Protocol #2021P002419). Patients who were potentially eligible for inclusion were identified using the research patient registry for a large academic hospital network in the northeastern United States.
Through review of the electronic medical record, patients were included in the study if they met the following criteria: diagnosis of DS; clinical diagnosis of ADHD based on the clinical documentation by a board-certified child and adolescent psychiatrist (M.L.P., C.J.M., C.J.K.) at a tertiary care outpatient center for neurodevelopmental disorders, where patients with DS are typically referred to psychiatry from the across the lifespan, multidisciplinary DS Program within the same hospital system; initiation of treatment with guanfacine at age 17 years or younger for symptoms of ADHD between September 1, 2011, and September 10, 2021; and at least one outpatient psychiatry follow-up visit after guanfacine initiation. Clinical notes were retrospectively reviewed and data were extracted and coded into a REDCap database.
Demographic and clinical characteristics
Demographic information and clinical characteristics of the sample included the presence/absence of ID, severity of ID, full-scale intelligence quotient (IQ) score, language ability, comorbid psychiatric and medical diagnoses at the time of guanfacine initiation, approximate age of onset of ADHD, ADHD subtype, prior psychiatric medication trials, and Clinical Global Impressions Severity subscale (CGI-S) score at the time of guanfacine initiation. The presence or absence of ID was determined through review of the medical records for documentation of “intellectual disability” or for documentation that the patient was a client of the state of Massachusetts “Department of Developmental Services” in a clinical note. Full-scale IQ was obtained through review of neuropsychological testing in the patient's medical record.
Severity of ID was estimated based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria (“mild” for IQ 50–69, “moderate” for 36–49, “severe” for 20–35, “profound” for <20). If neuropsychological testing was not available, the medical record was reviewed to determine the level of functioning/daily skills competency of the patient and the severity of ID was estimated according to the DSM, Fifth Edition (DSM-5), adaptive functioning criteria by a board-certified child and adolescent psychiatrist (R.P.T.).
Language ability was obtained through review of the medical records by searching for documentation including the words “verbal” or “language” or “communication” or “speech.” A language descriptor was then assigned: “nonverbal,” “minimally verbal (single words),” “phrase speech,” or “full sentences” based on review of the clinical documentation. Psychiatric and medical comorbidities were included if they were considered active/current at the time of guanfacine initiation, while historical/resolved comorbidities were not included. The ADHD subtype (combined presentation, predominantly inattentive presentation, or predominantly hyperactive/impulsive presentation) was determined through reviewing the medical record for coded diagnoses of relevant encounters. If the ADHD subtype was not in the medical record, a child psychiatry fellow (J.H.P.) reviewed the documentation from the visit when guanfacine was initiated to determine the ADHD subtype based on documented symptoms using the DSM-5 criteria for ADHD in consultation with a board-certified psychiatrist experienced in the care of youth with neurodevelopmental disabilities (R.P.T.).
If insufficient information was available in the record to determine the ADHD subtype, it was classified as “unknown.” The baseline severity of ADHD was retrospectively determined based upon medical record review of the clinical documentation using the CGI-S at the time of guanfacine initiation. The CGI-S is a 7-point scale used to rate symptom severity, ranging from 1 (“normal, not at all ill”) to 7 (“among the most extremely ill”).
Guanfacine treatment
Characteristics of guanfacine treatment data included guanfacine start and discontinuation date with reason for discontinuation if applicable, date of first psychiatry follow-up visit ≥12 weeks after guanfacine initiation, date of most recent psychiatry follow-up visit before the chart review cutoff date, concomitant psychiatric medications and nonmedication treatments at the time of guanfacine initiation, initial guanfacine dose, guanfacine dose at the first follow-up visit ≥12 weeks after guanfacine initiation, guanfacine dose at the final follow-up visit before the chart review cutoff date, and the optimal guanfacine dose. The optimal dose of guanfacine was defined as the stable dose with the greatest symptom improvement and fewest side effects. AEs documented at any point during guanfacine treatment were recorded. Vital signs (heart rate and blood pressure on guanfacine initiation date, and heart rate and blood pressure on first follow-up visit ≥12 weeks after guanfacine initiation) were also collected.
Improvement in ADHD symptom severity following treatment was retrospectively coded on the Clinical Global Impression Improvement subscale (CGI-I) based on the first clinical psychiatric note 12 or more weeks after starting guanfacine, or, for patients who discontinued treatment before 12 weeks, the psychiatric note documenting discontinuation. The CGI-I is a 7-point scale used by clinicians to rate the degree of change in illness severity compared with the patient's baseline, ranging from 1 (“very much improved”) to 4 (“no change”) to 7 (“very much worse”). The CGI-S and CGI-I ratings, anchored to ADHD symptoms, were assigned by a board-certified child and adolescent psychiatrist with expertise in treating children with developmental disabilities who was not the treating psychiatrist (R.P.T.).
Statistical analysis
Categorical variables were summarized using frequencies and percentages, while continuous variables were summarized using means, standard deviations (SDs), medians, and ranges. Variables with missing values for ≥30% of patients were excluded from analysis. Treatment response required completion of 12 or more weeks of guanfacine with an assigned CGI-I score ≤2 (“very much improved” or “much improved”). Nonresponse corresponded to a CGI-I score ≥3 (“minimally improved” or worse) or discontinuation of guanfacine treatment within the first 12 weeks. Wilson's method was used to calculate 95% confidence intervals (CIs) for percentages. Kaplan–Meier methods characterized time to discontinuation of treatment. Statistical analysis was conducted using version 9.4 of SAS (SAS Institute, Cary, NC) and version 17 of Stata (StataCorp, College Station, TX).
Results
Study flow
Records were identified for 59 potentially eligible patients, of whom 53 were ≤17 years old when guanfacine was started. Twenty-one patients met the full eligibility criteria for the study. Figure 1 shows the number of patients successively meeting each of our eligibility criteria.
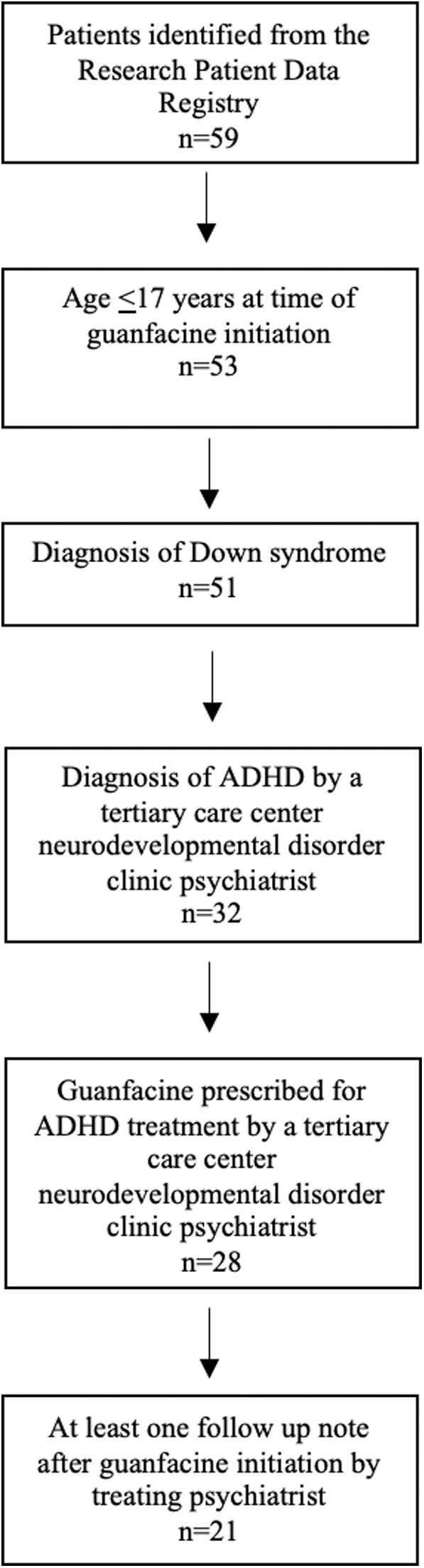
Identification of patients included in the study. Of the 59 potential patients identified, 21 met all the inclusion criteria and were included in the study.
Demographic and clinical characteristics of the sample
The demographic and clinical characteristics of the sample at the time of guanfacine initiation including prior psychiatric medication trials are presented in Table 1. Nine (43%) patients were female and 12 (57%) were male. The average age at guanfacine initiation was 10.0 years (SD 4.0; range 5.1–16.9 years). With regard to ADHD subtype, 12 (57%) patients had combined presentation, 5 (24%) had predominantly hyperactive/impulsive presentation, and zero had predominantly inattentive presentation. The ADHD subtype could not be determined for 4 (19%) patients. All 21 patients (100%) had ID. Nine patients (43%) had at least one comorbid psychiatric diagnosis and 20 patients (95%) had at least one active, comorbid medical diagnosis at the time of guanfacine initiation. Five patients (24%) had a history of treatment with any psychotropic medication before starting guanfacine. Four of the patients had previously been treated with a stimulant medication, which was discontinued before starting guanfacine.
Demographic and Clinical Characteristics of Patients with Down Syndrome and Attention-Deficit/Hyperactivity Disorder at the Time of Guanfacine Initiation
All patients had diagnoses of intellectual disability, although severity of intellectual disability could not be determined for one patient based on information available in the medical record.
Less frequent psychiatric diagnoses were generalized anxiety disorder (n = 1), impulse control disorder (n = 1), oppositional defiant disorder (n = 1), and social anxiety disorder (n = 1).
Less frequent medical diagnoses were asthma (n = 2), diarrhea (n = 2), eczema (n = 2), obesity (n = 2), acute myeloid leukemia (n = 1), dysmenorrhea (n = 1), Hirschsprung's disease (n = 1), hypotonia (n = 1), and irritable bowel syndrome (n = 1).
Selective serotonin reuptake inhibitor (n = 2), antipsychotic (n = 1), melatonin (n = 1), trazodone (n = 1), hydroxyzine (n = 1), and clonidine (n = 1).
ADHD, attention-deficit/hyperactivity disorder; CGI-S, Clinical Global Impressions Severity subscale; DS, Down syndrome; SD, standard deviation.
At baseline, the severity of ADHD as rated by the CGI-S ranged from “mildly ill” (CGI-S score of 3, n = 1) to “severely ill” (CGI-S score of 6, n = 8), with most patients rated as “markedly” or more ill (CGI-S ≥ 5, n = 17). Summary statistics for full-scale IQ and age of ADHD onset is not reported since they were not available in the records for >30% of the sample.
Characteristics of guanfacine treatment
All patients in the study were prescribed the immediate-release (IR) formulation of guanfacine. The majority of patients (n = 14) received twice-daily dosing of guanfacine, while the remainder received either once- or thrice-daily doses of guanfacine. The median time on guanfacine treatment covered by the clinical notes was 50.4 weeks, with a range of 0.3 weeks to 7.5 years. Characteristics of the guanfacine treatment course are presented in Table 2. Four patients (19%) discontinued guanfacine before completing 12 weeks of treatment. The mean (SD) starting, maximal, most recent, and optimal total daily doses of guanfacine were 0.32 (0.18) mg, 1.31 (0.57) mg, 0.83 (0.66) mg, and 1.28 (0.45) mg, respectively.
Characteristics of Guanfacine Treatment
Last follow-up dose of 0 indicates that the medication was discontinued.
Optimal dose was determined for 17 of 21 patients.
Includes patients ≤12 years (n = 12) and ≥13 years (n = 5) who completed at least 12 weeks of continuous guanfacine treatment.
Melatonin (n = 2), stimulant (n = 2), antipsychotic (n = 1), hydroxyzine (n = 1), selective serotonin reuptake inhibitor (n = 1), and trazodone (n = 1).
Refers to speech therapy, occupational therapy, physical therapy, and/or applied behavioral analysis/behavioral therapy.
SD, standard deviation.
Dosage by weight is not reported since weight was not available for >30% of patients. Rather, the total daily dose is reported by age group (≤12 and ≥13 years), for patients who completed at least 12 weeks of continuous guanfacine treatment. At the time of guanfacine initiation, 6 patients (29%) were taking concomitant psychotropic medications and 19 patients (91%) were receiving concomitant nonmedication (developmental) treatments, such as occupational therapy, speech-language therapy, physical therapy, and applied behavioral analysis/behavioral therapy.
Initial response to guanfacine treatment
Seventeen patients (81%) completed a 12-week course of guanfacine treatment. For these 17 patients, the median time between the first psychiatric visit and the first follow-up visit at least 12 weeks after starting guanfacine was 23.7 weeks, with a range of 12.0–47.9 weeks. Ten of the 21 patients (48%; 95% CI: 28%–68%) responded to guanfacine treatment (completion of 12 weeks of treatment and CGI-I = 1 or 2). Of the 10 patients who did respond (48%), four patients were rated as “very much improved” (CGI-I = 1) and six were rated as “much improved” (CGI-I = 2). Eleven patients did not respond to treatment. Of the 11 who did not respond, seven patients (33%) completed a 12-week course of treatment though had a CGI-I rating >2 (four patients rated as 3 = “minimally improved” and three patients rated as 4 = “no change”).
The remaining four patients who did not respond discontinued treatment before 12 weeks and two of these patients were rated as “no change” (CGI-I = 4), while the other two were rated as “minimally worse” (CGI-I = 5). Figure 2 summarizes CGI-I ratings after completion of 12 weeks of treatment or early discontinuation.
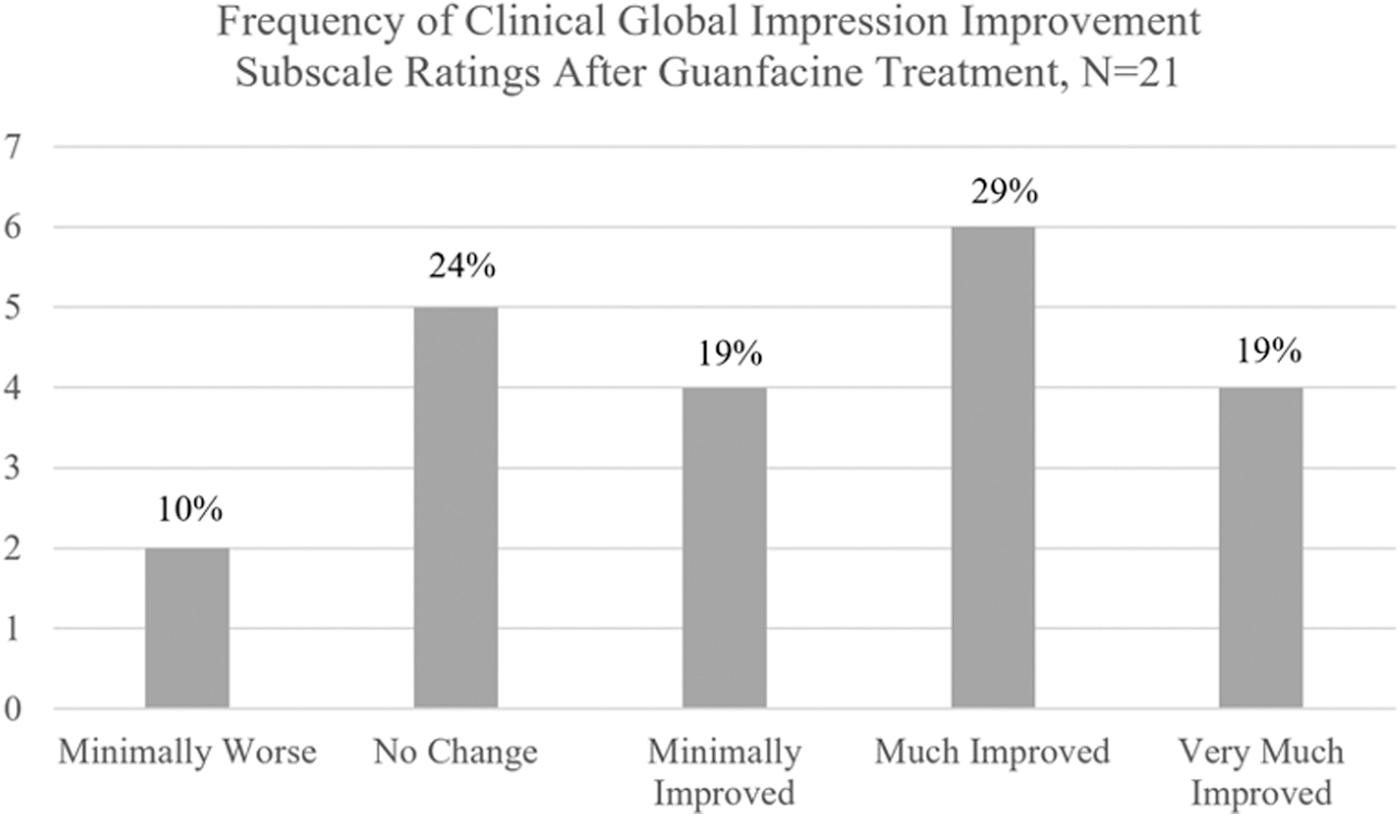
Frequency of CGI-I scores after guanfacine treatment. Ratings were assigned based on the earlier of the first clinical note 12 or more weeks after guanfacine initiation or the clinical note documenting treatment discontinuation. Response required completion of a 12-week course of guanfacine with a CGI-I rating of either “Much Improved” or “Very Much Improved.” Four patients discontinued treatment before 12 weeks, two with ratings of “No Change” and two with ratings of “Minimally Worse.” CGI-I, Clinical Global Impression Improvement subscale.
Adverse effects
AEs are presented in Table 2. Nine of the 21 patients (43%; 95% CI: 24%–63%) had AEs reported in their clinical notes. Sleepiness was reported by seven patients (33%), constipation was reported by two patients (10%), and insomnia, behavioral activation, and increased repetitive behaviors were each reported by one patient (5%). Changes in vital signs after treatment are not reported due to missing values at start date or follow-up for ≥30% of patients.
Treatment course
Figure 3 summarizes the time to discontinuation of guanfacine treatment. Eight of the 21 patients (38%) discontinued guanfacine during the period covered by clinical notes in the medical record, while 13 patients (62%) remained on guanfacine at the time of their most recent clinic note. Nearly 20% of patients discontinued treatment within the first 10 weeks, and nearly 30% of patients discontinued within the first year. Among the 10 patients treated with guanfacine for more than 1 year, one discontinued treatment between years 1 and 2, one discontinued treatment between years 2 and 3, and eight remained on treatment at the time of their most recent clinical note, between 2.5 and 7.5 years after initiation of guanfacine.

Time to discontinuation of guanfacine treatment. Tick marks correspond to the time of most recent clinical note for patients still taking guanfacine at their most recent psychiatric visit.
Among the eight patients who discontinued treatment during the period covered by their clinical notes, three discontinued due to treatment-limiting AEs: one due to behavioral activation at 0.3 weeks, one due to insomnia at 3.7 weeks, and one due to constipation at 8.0 weeks. Other individual reasons for discontinuation were pharmacy dispensing issues (9.3 weeks), guanfacine no longer effective (21.9 weeks), guanfacine no longer needed (22.6 weeks), and an abundance of caution during an unrelated medical admission (2.2 years). The eighth patient self-discontinued treatment at 1.4 years for unknown reasons.
Two patients were concurrently taking a stimulant medication when guanfacine was initiated. One patient was taking extended-release suspension methylphenidate, which was suboptimally treating their ADHD and perhaps leading to being more socially withdrawn and “hyperfocusing.” The treating child psychiatrist planned to transition the patient from this stimulant to guanfacine. At follow-up, the stimulant dose had been decreased by nearly 50% and guanfacine was uptitrated to 0.5 mg twice daily. This patient was considered a responder (CGI-I = 2). The second patient was taking extended-release methylphenidate 30 mg capsules daily and IR methylphenidate 15 mg tablets twice daily, with the side effect of moderate appetite suppression, when guanfacine was initiated to target ongoing hyperactivity and impulsivity. This patient discontinued guanfacine before 12 weeks of treatment due to not tolerating the medication and was considered a nonresponder.
Discussion
This naturalistic retrospective study evaluated the real-world effectiveness and tolerability of guanfacine for the treatment of ADHD in a clinical sample of youth with DS. Among the 21 youth included in the study, 17 patients were treated with guanfacine for at least 12 weeks. About half (48%; 95% CI: 28%–68%) of patients met the study's predefined criteria for treatment response including a CGI-I of ≤2 and completing at least 12 weeks of treatment. No serious side effects or AEs were reported in this sample.
The majority of patients in our study were diagnosed with combined (57%) or predominantly hyperactive/impulsive (24%) presentations of ADHD. Many patients in the sample had data covering a substantial duration of treatment, with a median duration of treatment of 50.4 weeks. Those who discontinued guanfacine did so for a variety of reasons, such as loss of effectiveness of the medication over time, issues with tolerating the medication (behavioral activation, insomnia, and constipation), no longer needing medication treatment, or pharmacy dispensing difficulties. The results from this study demonstrate that for a subset of patients with DS and comorbid ADHD, guanfacine was relatively effective and well-tolerated with no serious side effects or AEs.
The results of our study support and extend the findings of one of the only other published studies on pharmacologic treatment of ADHD in youth with DS (Capone et al., 2016). In Capone et al.'s prospective guanfacine trial, children with DS between 4 and 12 years of age who met the DSM-IV criteria for ADHD were prescribed guanfacine. Patients were initiated on 0.25–0.5 mg of guanfacine daily and doses were slowly uptitrated to maximize clinical benefit and minimize side effects, with the mean total daily dose at follow-up of 1.1 ± 0.5 mg per day (5 participants were on only bedtime dosing, 13 on twice-daily dosing, and 5 on thrice-daily dosing). The participants returned for a follow-up visit between 15 and 30 weeks after guanfacine initiation (average first follow-up was at 21 weeks), at which point response to guanfacine was assessed.
The primary outcome measure was the parent-reported ABC. Statistically significant decreases in the Irritability (25% decrease, effect size [d] of 0.47) and Hyperactivity (25% decrease, effect size [d] of 0.9) subscales as well as a significant decrease in the ABC composite score (24%, effect size [d] of 0.69) were reported. Notably, parents had access to their child's baseline behavior scores when completing the follow-up ratings. Aside from nighttime somnolence, the authors did not observe any treatment-emergent side effects. The study was primarily limited by its small sample size, significant psychiatric comorbidity (91% also had comorbid oppositional defiant disorder (ODD) or disruptive behavior disorder not otherwise specified), limited follow-up duration, and assessment of treatment response via parent report.
The results of our study, which used a retrospective clinician-rated outcome measure to assess response, add to the parent-reported ratings obtained by Capone et al., supporting the effectiveness of guanfacine for the treatment of ADHD in a subset of youth with DS. In addition, our study includes naturalistic treatment data for a longer duration of time and provides more robust evidence regarding guanfacine's long-term tolerability. One notable difference in results between the two studies is the rate of AEs. While no serious AEs occurred in either study, Capone et al. did not report any treatment-emergent side effects (besides the expected nighttime somnolence), whereas 43% of participants in our study experienced at least one side effect.
This may be because of the differences in the treatment periods covered in the studies—mean duration of treatment was 104 weeks in our study versus an average of 21 weeks of treatment in Capone et al.'s study. Both studies included sample populations with a high degree of externalizing behaviors, but did have notable differences in reported diagnoses. In Capone et al.'s study, 91% of patients (21/23) had comorbid ODD or disruptive behavior disorder, not otherwise specified, while in the present study, only 5% of patients (1/21) had ODD. Eighty-one percent of children in the present study had either combined or predominantly hyperactive/impulsive presentations of ADHD, however, this information is not provided in Capone et al.'s study.
In addition, the mean age in Capone et al.'s study (7.4 years) was younger than that of our study (10 years). Importantly, the mean total daily doses at first follow-up were comparable between studies: 1.1 ± 0.5 mg per day in Capone et al.'s study compared with1.04 ± 0.42 mg per day for patients ≤12 years and 1.20 ± 0.82 mg per day for patients ≥13 years in the present study. The rates of tolerability and effectiveness described in both studies despite differences in comorbid diagnoses, ADHD subtypes, age groups, and primary outcome measures provide broader support for the use of guanfacine for the treatment of ADHD in youth with DS.
The second of the only two previously published reports of the pharmacological treatment of ADHD in DS was a retrospective study assessing the use of methylphenidate (Roche et al., 2021). In that study, 21 children with DS and ADHD who were treated with methylphenidate for ADHD were identified for inclusion through review of databases and paper charts at a European clinical care and research center. A limitation of this study was that treatment response was based on parents' and educators' binary rating of either “improvement” or “no improvement” with regard to “attention/concentration” and “hyperactivity/impulsivity.” Seventy-six percent (16 out of 21) of parents/educators reported “improvement” in both “attention/concentration” and “hyperactivity” and 12 patients (57%) experienced AEs.
Given the notable differences in methodologies, it is difficult to directly compare the results of Roche et al.'s methylphenidate study with the results of Capone et al.'s guanfacine study and our guanfacine study, although rates of AEs were higher in the methylphenidate study. Future research comparing the effectiveness of stimulants and guanfacine is required to support clinical decision-making. Collectively, all three studies provide evidence that pharmacological treatment of ADHD in youth with DS may be effective.
Guanfacine has FDA approval for the treatment of ADHD in youth based on the efficacy established by four double-blind placebo-controlled trials (three placebo-controlled monotherapy trials and one placebo-controlled adjunctive trial with psychostimulants) that included otherwise normally developing youth, all of which demonstrated significant reductions in mean ADHD-Rating Scale-IV scores compared with placebo (Shire US, Inc., 2013). While the FDA approval for ADHD is for the extended-release formulation, which has the potential therapeutic advantage of maintaining a more consistent level of drug throughout the day, all of the patients in our study were treated with the IR formulation to start at lower doses. In addition, many children with DS have difficulty with pill swallowing, precluding the use of extended-release formulations.
While no specific treatment algorithm was followed by the treating child psychiatrists, often patients were typically started on guanfacine IR 0.25 mg every morning and the dose was uptitrated in this increment based on tolerability and effectiveness.
In one randomized controlled trial of children with ADHD treated with variable doses (2, 3, or 4 mg, respectively) of guanfacine, frequent AEs in patients taking 2 mg daily (dose most comparable with our study, although still higher than our average optimal total daily dose of 1.28 mg) included somnolence (24.1%), sedation (9.2%), fatigue (18.4%), lethargy (5.7%), upper abdominal pain (10.3%), decreased appetite (5.7%), and dizziness (4.6%) (Biederman et al., 2008). No controlled trials assessing guanfacine for ADHD in youth with DS have been published. However, two double-blind, placebo-controlled trials assessing the efficacy of guanfacine for the treatment of hyperactivity, impulsivity, and inattention in youth with ASD and/or ID have been published with response rates of 45% (5 of 11 subjects, crossover design, for hyperactivity only) (Handen et al., 2008) and 50% (15 of 30 guanfacine-treated subjects, as assessed by the CGI-I) (Scahill et al., 2015).
The response rate in our study of 48% is similar to those observed in these controlled trials in autistic youth and in otherwise normally developing youth. Furthermore, the prevalence of AEs and the side effect profile in our study is comparable with that reported in the two controlled trials of guanfacine for the treatment of ADHD symptoms in youth with ASD. The most common AEs in the larger of these two ASD trials included drowsiness (86.7%), fatigue (63.3%), decreased appetite (43.3%), emotional/tearful (40.0%), and dry mouth (40.0%) (Scahill et al., 2015).
In light of the medical complexity of persons with DS, the use of psychotropic medications in this population requires particular attention to medication safety and tolerability. Cardiovascular comorbidities such as cardiac defects, pulmonary hypertension, and obstructive sleep apnea (OSA) are common in DS. The prevalence of congenital heart disease and OSA in this study was 57% and 48%, respectively. Therefore, patients should be monitored carefully for cardiovascular AEs, including decreases in both heart rate and blood pressure. In addition, 33% of patients in our study experienced sleepiness as an AE, which may be clinically relevant to patients with OSA (in our study, 30% of patients with OSA reported sleepiness/drowsiness). Close monitoring should occur in patients with DS when initiating and titrating guanfacine.
It was common for the prescribing psychiatrists in our study to consult with the patient's cardiologist before initiating medication treatment and to recommend blood pressure and heart rate checks at home or school before and following dose adjustments. Moreover, constipation is a frequent comorbidity in DS (43% prevalence in our sample). As guanfacine may cause or worsen constipation, discussing this possible AE with patients and their families is warranted as well. In our sample, 10% reported treatment-emergent constipation.
One limitation of this study may have been an overly conservative definition of treatment response. Our predefined definition of treatment response was 12 or more weeks of continued guanfacine treatment and an assigned CGI-I score ≤2 (“very much improved” or “much improved”) at follow-up. This was a conservative definition of real-world treatment effectiveness requiring both tolerability (completion of at least 12 weeks of treatment) and symptom improvement. This approach may have underestimated the benefits of guanfacine for this population, as two patients who discontinued the medication before the first follow-up (and were therefore considered nonresponders) were later on retrialed on the medication with good effects. In addition, four patients received CGI-I scores of 3 (“minimally improved”).
Of the 17 patients who continued guanfacine for at least 12 weeks after first being trialed on the medication, 10 patients (58%) had a CGI-I ≤ 2, which falls within the 95% CIs (28%–68%) of the reported response rate using our original definition of response.
The other limitations of our study primarily relate to those inherent to its retrospective nature. The data obtained were limited by what was documented in the clinical records. Follow-up durations varied among patients and were not standardized. Practices regarding guanfacine starting doses and dose escalation were also not standardized. Furthermore, some patients in our sample who discontinued the medication before their first follow-up visit (when CGI-I was scored) were later restarted on the medication to good effect, yet according to our predefined response criteria, these patients were considered “nonresponders.” In addition, a limitation of our study is the generalizability of our results. Our sample was limited to 21 patients identified at one suburban tertiary care outpatient center and was not racially (81% white) or ethnically (81% non-Hispanic) diverse.
In conclusion, about half of youth with DS and ADHD in our sample responded to a 12-week course of guanfacine and many tolerated long-term use. Controlled studies are needed to further assess the efficacy, tolerability, and safety of guanfacine and other medications for the treatment of ADHD in youth with DS.
Conclusion
In this naturalistic, retrospective study of 21 youth with DS who were treated with guanfacine for ADHD, about half (48%) responded to guanfacine treatment. No serious side effects or AEs were reported and many tolerated long-term use. The study was primarily limited by its retrospective nature and small sample size. Given the unique medical and neuropsychiatric comorbidities relevant to DS, extrapolating evidence from studies on neurotypical youth and from youth with ASD or ID is not sufficient in providing equitable care to this underserved population. Controlled studies are needed to further assess the efficacy, tolerability, and safety of medications for the treatment of ADHD in youth with DS.
Clinical Significance
ADHD is a common comorbidity in youth with DS, yet evidence-based treatments remain limited. This naturalistic retrospective chart review study assessed the real-world effectiveness and safety of guanfacine for the treatment of ADHD in 21 youth with DS. Ten of the 21 patients (48%; 95% CI: 28%–68%) responded to treatment. Nine (43%; 95% CI: 24%–63%) had adverse events documented in their notes, most commonly sleepiness (n = 7) and constipation (n = 2). Guanfacine should be considered as a potential treatment for ADHD symptoms in this population.
Footnotes
Authors' Contributions
J.H.P.: conceptualization (lead), methodology (equal), investigation (equal), writing—original draft (lead), writing—review and editing (lead), and visualization (equal). M.W.: software (equal), validation (equal), formal analysis (lead), data curation (equal), writing—review and editing (supporting), and visualization (equal). M.P.: conceptualization (supporting), resources (equal), and writing—review and editing (supporting). C.J.K.: conceptualization (supporting), resources (equal), and writing—review and editing (supporting). C.J.M.: conceptualization (supporting), resources (equal), and writing—review and editing (supporting). C.R.: conceptualization (lead), methodology (equal), software (equal), validation (equal), formal analysis (equal), data curation (equal), writing—review and editing (equal), and supervision (supporting). R.P.T.: conceptualization (lead), methodology (lead), software (equal), investigation (equal), resources (equal), writing—original draft (supporting), writing—review and editing (lead), visualization (equal), supervision (lead), and project administration (lead). This statement confirms that all authors have read and approved the final version of the article and agree to be accountable for the work.
Availability of Data and Material
The data sets generated and/or analyzed during the current study are not publicly available due to protection of private health information but are available from the corresponding author on reasonable request.
Ethical Approval
The study was granted exception by the local institutional review board. This statement additionally certifies that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Disclosures
R.P.T.: Williams Syndrome Association—Research support; Piton—Research support; Harvard Medical School Dupont Warren Fellowship—Research support; Louis V. Gerstner III Research Scholar Award—Research support; the American Academy of Child and Adolescent Psychiatry—Research support; the Jerome Lejeune Foundation—Research support; Oxford University Press—Royalties; Springer Publishing—Royalties. C.J.M.: Sage Therapeutics—Consultant; Acadia Pharmaceuticals—Consultant; Oxford University Press—Royalties; Springer Publishing—Royalties. M.P.: Otsuka—Research support. C.J.K.: Biogen—Consultant; Ionis—Consultant; Maplight Therapeutics—Research support; Ovid Therapeutics—Research support. J.H.P.: no conflicts of interest reported. M.W.: no conflicts of interest reported. C.R.: no conflicts of interest reported.