
Abstract
The efficacy and tolerability of psychotropic medications can vary significantly among children and adolescents, and some of this variability relates to pharmacogenetic factors. Pharmacogenetics (PGx) in child and adolescent psychiatry can potentially improve treatment outcomes and minimize adverse drug reactions. This article reviews key pharmacokinetic and pharmacodynamic genes and principles of pharmacogenetic testing and discusses the evidence base for clinical decision-making concerning PGx testing. This article reviews current guidelines from the United States Food and Drug Administration (FDA), the Clinical Pharmacogenetics Implementation Consortium (CPIC), and the Dutch Pharmacogenetics Working Group (DPWG) and explores potential future directions. This review discusses key clinical considerations for clinicians prescribing psychotropic medications in children and adolescents, focusing on antidepressants, antipsychotics, stimulants, norepinephrine reuptake inhibitors, and alpha-2 agonists. Finally, this review synthesizes the practical use of pharmacogenetic testing and clinical decision support systems.
Introduction
Given the significant burden of psychiatric disorders in children and adolescents and the role of pharmacotherapy in treating these conditions, pharmacogenetic (PGx) testing has received considerable attention from clinicians, industry, and regulatory agencies who have recognized its potential to improve precision medicine approaches in child and adolescent psychiatry. Despite >30 years of research on PGx in mental health (Brown et al., 2022; Greden et al., 2019; Oslin et al., 2022) few studies have been conducted in youth, although studies now demonstrate—in children and adolescents—that variation in pharmacokinetic (PK) and/or pharmacodynamic (PD) genes produces differences in side effects (Aldrich et al., 2019; Strawn et al., 2020), response trajectory (Strawn et al., 2020), and dose titration (Poweleit et al., 2019).
This article aims to provide a background and an up-to-date review of current research and guidelines to enhance psychiatry clinicians' knowledge base and promote evidence-based pharmacogenetics application.
Terminology in Pharmacogenetics
This field has introduced new concepts that are often unfamiliar to the child and adolescent provider. As such, a review of relevant terminology in the field of pharmacogenomics is summarized in Table 1. In addition, identified relevant alleles that are most studied are summarized (Table 2). Table 3 reviews CPIC levels impacting actionability to help with clinical decision-making.
A Review of Relevant Terminology in the Field of Pharmacogenomics
AS, activity scoring; CPIC, Clinical Pharmacogenetics Implementation Consortium; CYP, cytochrome P450.
Examples of Common +Tier 1 Star Alleles, Based on Functionality
+Tier 1 variant allele criteria: (1) have a well-characterized effect on the function of the protein and/or gene expression; (2) have an appreciable minor allele frequency in a population/ethnicity group; (3) have publicly available reference materials (Pratt et al., 2021; Pratt et al., 2018).
CYP, cytochrome P450.
Source: PharmGKB (2023a).
Clinical Pharmacogenetics Implementation Consortium Levels Impacting Actionability for Pharmacogenomic Testing
CPIC, Clinical Pharmacogenetics Implementation Consortium.
Cytochrome system
The focus of much of the child and adolescent research in pharmacogenetics has been on the genes that code for the enzymes that are involved in the cytochrome P450 (CYP) pathway. This pathway consists of a superfamily distinctly classified into families, subfamilies, and isoenzymes following systematic nomenclature based on similar amino acid sequences. These pathways are allotted a family number (e.g., CYP1 and CYP2) followed by a subfamily letter (e.g., CYP1A and CYP2D) and are then distinguished by a number for the specific isoenzymes (e.g., CYP1A2 and CYP2D6) (McDonnell and Dang, 2013).
CYPs are most concentrated in the liver, followed by the intestines, kidneys, intestinal mucosa, lung, brain, lymphocytes, and placenta (Zhao et al., 2021). They play a key role in Phase I drug metabolism, primarily involving oxidation and reduction and hydrolysis (Zhao et al., 2021).
These P450 genes are among the PK genes, which code primarily for enzymes responsible for metabolizing medications. In contrast, PD genes code for target proteins on which medications act. Genetic polymorphisms can significantly affect drug effectiveness and tolerability (Ahmed et al., 2016) and polymorphisms in many CYP450 genes impact the metabolism of psychotropic medications, which is felt to play a role in the variation in clinical response (van Westrhenen et al., 2020).
Metabolizer status
The impact of allelic variations in the genes that code for P450 enzymes results in changes in metabolizer status. There are four primary metabolizer phenotypes for CYP2D6: normal, intermediate, poor, and ultrarapid metabolizer. Normal metabolizers have standard enzyme activity, leading to typical drug metabolism. Intermediate metabolizers show reduced enzyme activity, potentially altering drug responses. Poor metabolizers experience significantly reduced enzyme function, potentially increasing drug concentrations and the risk of adverse effects.
Ultrarapid metabolizers can have elevated enzyme activity, often resulting in rapid drug metabolism, which can lead to suboptimal therapeutic outcomes due to lower drug levels. Recognizing an individual's metabolizer status is crucial in clinical contexts to enhance drug effectiveness and reduce potential adverse reactions.
Variations in CYP phenotypes
Allelic frequencies range broadly across ancestrally diverse populations. For example, patients of Northern European and African descent have higher frequencies of normal metabolizer phenotypes for CYP2C19. In contrast, patients of Asian descent are more likely to be intermediate metabolizers for the same enzyme (Wehry et al., 2018). Similarly, in Hispanic populations in the United States the most common variants of CYP2D6 alleles are those coding for normal activity, followed by nonfunctional and reduced function alleles (Claudio-Campos et al., 2015).
PK Genes Relevant to Psychotropic Medications
Table 4 provides a review of the resources available that evaluate evidence-based pharmacogenetic information and Table 5 summarizes which psychotropic medications have guidelines based on genetic results and from which source. Hereunder, we provide a summary to highlight the actionable clinical considerations by relevant genes.
Resources to Access and Evaluate Evidence-Based Pharmacogenomic Information
CPIC, Clinical Pharmacogenetics Implementation Consortium; FDA, Food and Drug Administration; PGx, pharmacogenomics; PharmGKB, Pharmacogenomics Knowledgebase; SSRI, selective serotonin re uptake inhibitor; SNRI, serotonin and norepinenphrine re uptake inhibitors; TCA, tricyclic antidepressants.
Comprehensive Table of Psychiatric Medications That Have Evidence-Based Guidelines
Clinical recommendations.
(1) FDA guidelines for which data support therapeutic management recommendations.
(2) FDA guidelines for which data indicate a potential impact on safety or response.
(3) FDA guidelines for which data indicate a potential impact on pharmacokinetic properties only.
ADHD, attention-deficit/hyperactivity disorder; CNS, central nervous system; CPIC, Clinical Pharmacogenetics Implementation Consortium; CYP, cytochrome P450; DPWG, Dutch Pharmacogenetics Working Group; DRESS, drug reaction with eosinophilia and systemic symptoms; FDA, Food and Drug Administration; IM, intermediate metabolizer; NM, normal metabolizer; PM, poor metabolizer; RM, rapid metabolizer; SJS, Stevens–Johnson syndrome; TENS, toxic epidermal necrolysis; UM, ultrarpid metabolizer.
CYP2D6
Through Phase I oxidation, CYP2D6 plays a primary role in the metabolism of >470 medications, including fluoxetine, fluvoxamine, paroxetine, venlafaxine, atomoxetine, and tricyclic antidepressants (Wehry et al., 2018). CYP2D6 enzyme maturation occurs by 1 year of age, with the most rapid increase occurring in the first 2 weeks (Anderson and Lynn, 2009).
Recommendations relevant to 2D6 psychotropic substrates
Selective serotonin re uptake inhibitor (SSRIs)/Serotonin and norepinenphrine re uptake inhibitors (SNRIs)
Important clinical considerations for this category of medication include that for paroxetine, several studies showed that ultrarapid metabolizers had low or undetectable plasma paroxetine concentrations. This resulted in a recommendation by Clinical Pharmacogenetics Implementation Consortium (CPIC) to select a different medication that is not metabolized by CYP2D6.
Similarly, poor metabolizers showed an increased risk of side effects due to higher exposure to paroxetine, suggesting a 50% dose reduction. In intermediate metabolizers, initiating paroxetine at a lower dose with slower titration may reduce the risk of side effects (Bousman et al., 2023; Brouwer et al., 2022). With regard to fluvoxamine, for poor 2D6 metabolizers, there is an additional recommendation included in CPIC guidelines to consider prescribing at a 20%–50% reduction of the standard dose (Safer, 2016).
For venlafaxine, the CPIC recommendation for CYP2D6 poor metabolizers is to consider a clinically appropriate alternative antidepressant not predominantly metabolized by CYP2D6. With regard to vortioxetine, similar consideration should be made for poor metabolizers of CYP2D6 to start at 50% of the recommended dose to maximum of 10 mg or consider an alternative antidepressant, which is not primarily metabolized by CYP2D6. For ultrarapid metabolizers CPIC recommends either considering an alternate drug not metabolized by CYP2D6 or initiating therapy at a standard dose and titrating based on efficacy and tolerability keeping in mind that 50% or more may be needed (Bousman et al., 2023).
In youth who are poor CYP2D6 metabolizers, atomoxetine concentrations are elevated compared with normal metabolizers. In poor metabolizers, atomoxetine should be initiated at 0.5 mg/(kg·day) for youth up to 70 kg (40 mg for youth >70 kg) and only titrated to the usual target dose of 1.2 mg/(kg·day) (70 mg for youth >70 kg) if no improvement of symptoms is observed after 4 weeks, and if the starting dose is well-tolerated (Atomoxetine Package Insert, 2022).
Special notes on fluoxetine and duloxetine
CYP2D6 converts fluoxetine to s-norfluoxetine, whereas both CYP2D6 and CYP2C9 contribute to the conversion of fluoxetine to r-norfluoxetine. Although CYP2D6 ultrarapid and poor metabolizers exhibit varying parent-to-metabolite ratios, the total combined exposure to the parent drug and metabolites is similar across metabolizer groups. The complex interaction between these enzymes and their impact on drug efficacy and safety remain inadequately studied, resulting in no dosing recommendations for fluoxetine.
Similarly, there are no dosing recommendations for duloxetine, which is metabolized by CYP1A2 and CYP2D6, as no substantial clinical impact has been observed. Medications with minimal contributions from CYP2D6 in their metabolism, such as desvenlafaxine and levomilnacipram, also lack dosing recommendations (Bousman et al., 2023).
Tricyclic antidepressants
Most available guidelines are extrapolated from studies of nortriptyline (secondary amine tricyclic antidepressant [TCA]) and amitriptyline (tertiary amine TCA) as representative TCAs due to shared PK properties. CYP2D6 significantly metabolizes both nortriptyline and amitriptyline, and ultrarapid metabolizers may require higher doses of TCAs to achieve adequate plasma concentrations but risk metabolite-induced cardiotoxicity, warranting therapeutic drug monitoring. An alternative drug is favored in poor metabolizers receiving TCAs due to a higher risk of adverse effects. If the use of a tricyclic is unavoidable, CPIC strongly recommends a 50% dose reduction and therapeutic monitoring (Hicks et al., 2017).
CYP2C19
CYP2C19 metabolizes >50 medications, including citalopram and escitalopram, sertraline, and many tricyclic antidepressants. CYP2C19 metabolism increases above adult levels in early childhood and then drops to adult levels in adolescence (Ramsey et al., 2021) and matures by 5–6 months after birth (Ward and Kearns, 2013).
Recommendations relevant to 2C19 psychotropic substrates
SSRIs
Ultrarapid metabolizers of CYP2C19 have lower citalopram and escitalopram concentrations than normal metabolizers, rendering therapeutic doses less efficacious in this patient population. Dosing recommendations remain unavailable due to insufficient data.
However, due to higher es/citalopram discontinuation rates in pediatric patients who were ultrarapid metabolizers (Aldrich et al., 2019) and population PK studies in youth (Poweleit et al., 2023), an alternative medication not metabolized by CYP2C19 is recommended by CPIC (Bousman et al., 2023). If these medications are clinically necessary, titration to a higher dose may be justified.
In contrast, no recommendations exist for sertraline dose adjustment in ultrarapid metabolizers due to a lack of data supporting clinically significant alterations in drug exposures or treatment outcomes. Similar but less pharmacokinetically and clinically pronounced effects are observed for rapid metabolizers, making the recommendation for standard dosing, increased dosing, or alternative drugs optional.
Intermediate metabolizers may show higher plasma concentrations of citalopram, escitalopram, and sertraline. Whereas CPIC advises slower titration and lower maintenance dosing (Bousman et al., 2023), Dutch Pharmacogenetics Working Group (DPWG) recommends not exceeding 30, 15, and 75 mg, respectively (Brouwer et al., 2022).
Poor metabolizers of CYP2C19 have elevated citalopram, escitalopram, and sertraline concentrations, increased side effects, and higher discontinuation rates (Aldrich et al., 2019). Therefore, it is advisable to start poor metabolizers on lower initial doses, titrate the dosage slowly, and decrease the maintenance dose by 50% for these medications. Considering an alternative medication may also be prudent.
The Food and Drug Administration (FDA) recommends a 50% reduction in the dose of citalopram (with a maximum dose of 20 mg) for this patient group due to the heightened risk of QT interval prolongation, and cardiac assessments, including corrected QT interval measurements. Although the FDA labeling for escitalopram currently lacks the same recommendation and QT prolongation has not been observed in prospective randomized controlled trials of escitalopram in youth (Strawn et al., 2020), escitalopram may be associated with QT prolongation (Ojero-Senard et al., 2017).
There is increasing evidence revealing worse clinical outcomes in poor metabolizers receiving these medications, including increased risks of side effects and drug discontinuation. Therefore, it has been recommended in poor metabolizers to consider lower initial doses, slower titration, and a 50% decrease in the maintenance dose of these medications. Prescribing an alternative medication is to be considered. (Bousman et al., 2023).
TCAs
For amitriptyline, no change in the starting dose is recommended for normal metabolizers.
Similarly, there is no evidence to support changing the starting dose for intermediate metabolizers, despite an increased amitriptyline to nortriptyline ratio in plasma. For rapid and ultrarapid metabolizers carrying the CYP2C19*17 allele, low plasma concentration of amitriptyline combined with an increased concentration of nortriptyline may lead to treatment failure and an increased adverse effect (de Vos et al., 2011). Owing to the paucity of studies examining the possibility of altered plasma levels of amitriptyline, CPIC optionally recommends considering an alternative tricyclic antidepressant or another drug not metabolized by CYP2C19.
If amitriptyline is prescribed to CYP2C19 rapid or ultrarapid metabolizers, drug monitoring to ensure therapeutic levels is advised. For poor metabolizers of CYP2C19, elevated amitriptyline to nortriptyline ratios are expected, predisposing these patients to side effects (Shimoda et al., 2002). A 50% reduction in starting dose is recommended in addition to therapeutic drug monitoring (Hicks et al., 2017).
Other TCAs
Owing to shared PK characteristics, it may be possible to apply the same guidelines concerning the metabolism of amitriptyline to other tertiary amine TCAs (e.g., clomipramine, doxepin, imipramine, and amoxapine), while acknowledging scarcity of studies justifying dose adjustments for other TCAs relative to amitriptyline.
TCAs recommendations in combinatorial CYP2D6 and CYP2C19 phenotypes: Owing to limited studies on combinatorial phenotypes, recommendations remain optional. However, available studies show that individuals with no function CYP2D6 alleles and normal function CYP2C19 alleles were more likely to experience adverse effects while on amitriptyline. Conversely, individuals with no function CYP2C19 alleles and normal function CYP2D6 alleles showed a lower likelihood of experiencing adverse effects (Hicks et al., 2017).
CYP2B6
CYP2B6 is involved in the metabolism of >70 compounds, including both bupropion and sertraline. Variation in CYP2B6 was found to account for 1%–10% of the overall adult hepatic P450 content, with interindividual variability of up to 100-fold. CYP2B6 contributes 8%–13% of metabolism of clinically relevant drugs, including methadone, bupropion, and ketamine (Desta et al., 2021; Zanger and Klein, 2013). Approximately one-third of pediatric liver samples have no detectable levels of CYP2B6, and its expression doubled within the initial month of life compared with the fetal period.
Genetic factors may contribute to these variations in the maturation of CYP2B6 protein levels (Zanger and Schwab, 2013). Interestingly, girls have comparable or higher levels of hepatic CYP2B6 in vitro and faster CYP2B6 metabolism of drugs such as propofol and methadone.
Recommendations relevant to 2B6 psychotropic substrates
Ultrarapid and rapid CYP2B6 metabolizers experience only a slight increase in metabolism, thus no dose adjustment is advised by CPIC for sertraline. Intermediate metabolizers may exhibit higher sertraline plasma concentrations and, although adjusting the initial dose is not recommended, slower metabolizers may require a more gradual titration and a reduced maintenance dose compared with normal metabolizers.
Poor metabolizers have significantly reduced metabolism and higher sertraline exposure, indicating a need for a lower starting dose, slower titration, and a 25% reduction in maintenance dose. Recommendations for intermediate and poor metabolizers are considered optional due to the limited availability of supportive clinical data. The recommendations regarding sertraline are based on both 2B6 and 2C19 findings (Bousman et al., 2023).
ABCB1
The ABCB1 gene encodes P-glycoprotein (PGP) is an active efflux pump at the blood–brain barrier for several drugs implicating its use in multidrug resistance (Leschziner et al., 2007). Several documented polymorphisms may change PGP expression and substrate specificity, possibly affecting the drug levels of specific SSRIs (citalopram, escitalopram, and fluoxetine) (Brückl and Uhr, 2016) and SNRIs, including venlafaxine. Adults with modified ABCB1 alleles in PGP may respond more effectively to citalopram, resulting in improved clinical outcomes compared with those with functional PGP (Kalla et al., 2023), although data are limited. There are no guidelines available for ABCB1 genetic variants.
PD Genes
Generally speaking, PD genes encode drug targets, such as enzymes, proteins, and transporters (Namerow, 2020). Hereunder, we focus on a select few PD genes due to the limited current clinical evidence supporting their direct applications.
Transporters
The SLC6A4 gene, located on chromosome 17q11, encodes the serotonin transporter (serotonin transporter [5HTT) or SERT) (Lam et al., 2018), which plays a crucial role in presynaptic serotonin uptake, and reduces serotonin bioavailability (Lam et al., 2018). Alterations in the gene's expression can potentially affect serotonin availability. The SLC6A4 gene contains tandem repeats with embedded SNP, with the most significant polymorphism in the promoter region of the SLC6A4 gene, where an insertion at base 44 results in a long (l/l) or short (s/s) variant without the insertion.
The s/s variant is associated with reduced transporter expression and serotonin reuptake, whereas the l/l variant increases transporter expression and reuptake (Fig. 1). The s/s variant may be associated with reduced improvement in depressive symptoms in adults with depressive disorders (Huezo-Diaz et al., 2009) and with SSRIs in pediatric anxiety disorders (Strawn et al., 2020). However, it is important to note that the clinical effects of SSRIs on these two variant promoter regions of the SLC6A4 gene are observed in the Caucasian population but not in individuals of Asian ancestry (Lam and Scott, 2018).
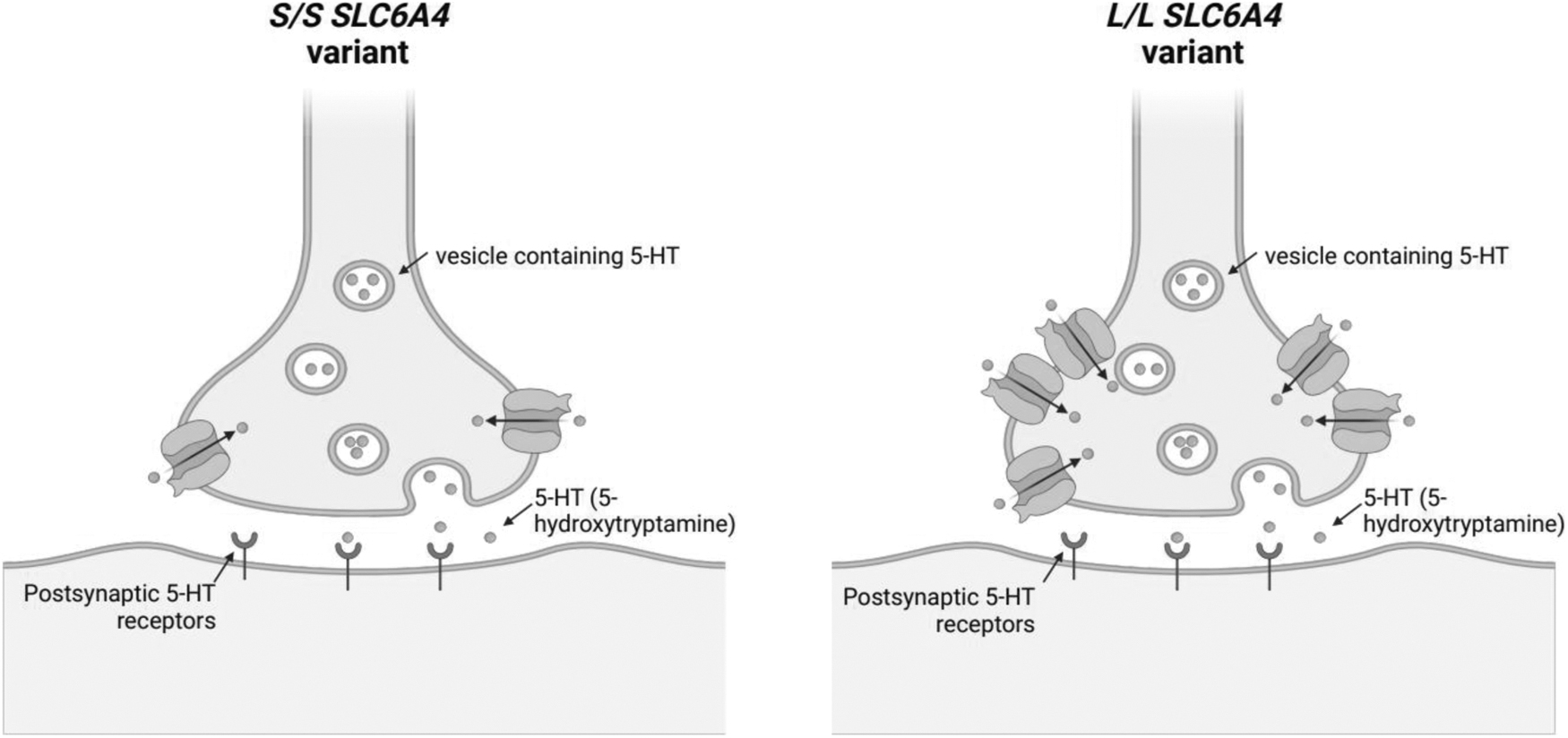
Serotonin transporter (5-HTT) promotes the reuptake of serotonin at the presynaptic membrane, effectively decreasing the amount of serotonin available for biological use. The (l/l) SLC6A4 variant has notably elevated 5-HTT expression (right), improving response to Selective Serotonin Reuptake Inhibitor and increasing the chance of remission in adults with MDD and some studies of youth with anxiety disorders compared with the (s/s) variant (left). MDD, major depressive disorder; SSRIs, selective serotonin reuptake inhibitor. Created with BioRender.com
Recent studies in the pediatric population have found no connection between the gene variant and sertraline response, but those with low predicted SCL6A4 promoter levels tolerated the drug better and were treated for longer periods (Poweleit et al., 2019). However, in a prospective randomized controlled trial of escitalopram in adolescents with generalized anxiety disorder, individuals with the s/s genotype had slower and less improvement (Strawn et al., 2020). Currently, there are no CPIC recommendations for SSRI antidepressant dosing based on SLC6A4 genotype (Bousman et al., 2023).
Receptors
The 5-HT2A receptor is encoded by the HTR2A gene, which may influence SSRI response (Kao et al., 2020). In adults, noteworthy polymorphisms include rs6313, associated with greater response. In children and adolescents, this polymorphism has been implicated in a better dose–response; children with more G alleles obtained a drug response at lower doses of sertraline (Poweleit et al., 2019). In a separate study, adolescents with generalized anxiety disorder with more G alleles had faster and greater responses to escitalopram than those with the A allele (Strawn et al., 2020). CPIC does not have specific dosing recommendations related to HTR2A polymorphisms (Bousman et al., 2023).
Enzymes
PD enzymes represent a significant class of PD protein products that are involved in the synthesis of neurotransmitters or are involved as active targets for pharmacological therapies. One such enzyme is methylenetetrahydrofolate transferase (MTHFR), encoded by the MTHFR gene. MTHFR plays a key role in the folate cycle (Fig. 2), converting folic acid into the active form
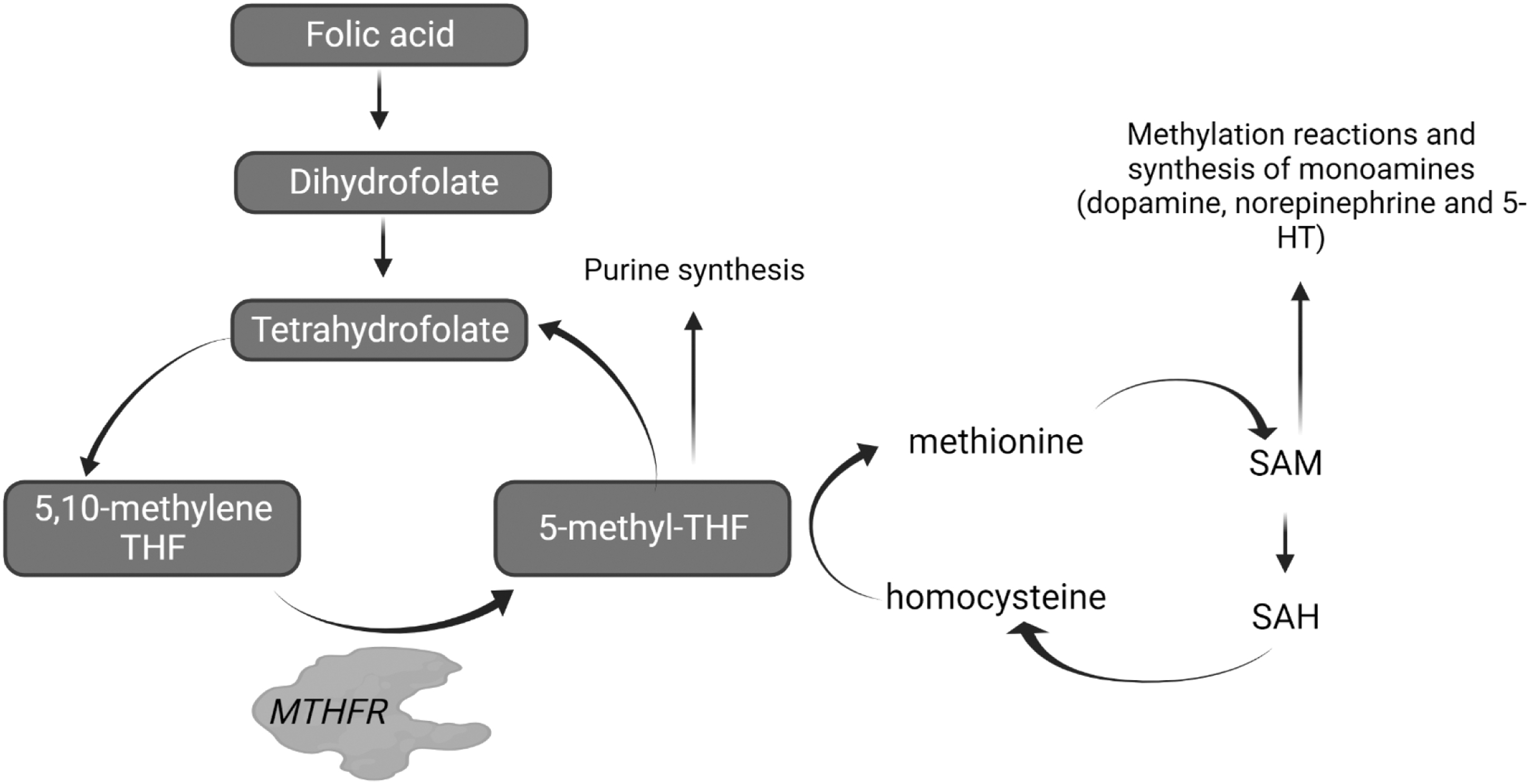
The folate cycle synthesizes dopamine, norepinephrine, and serotonin from folic acid by a series of enzymatic reactions. The enzyme MTHFR is a necessary step in this biochemical pathway to synthesize active folate, which allows the conversion of homocysteine into methionine. MTHFR, methylenetetrahydrofolate transferase. Created with BioRender.com
Approximately 34 MTHFR polymorphisms have been identified, leading to reduced enzyme function and diminished methyl-folate production and methylation. The most extensively studied polymorphisms include a C to T mutation at the 677 site (rs1801133) and an A to C mutation at the 1298 site (rs1801131) (Zhang et al., 2022). However, there are no CPIC guidelines or dosing recommendations related to MTHFR gene polymorphisms, and there is no evidence supporting the use of
Human leukocyte antigen genes
Variations in human leukocyte antigen (HLA) genes have received attention recently due to direct actionability related to risk for hypersensitivity reactions to certain mediations in adults and pediatrics. The HLA gene encodes specific cell surface proteins that specialize in antigen presentation to T cells and regulate immune responses (Mosaad, 2015). Specifically, the HLA-B 1502 and HLA-A 3101 alleles have been identified to significantly increase adverse outcomes with the anticonvulsant carbamazepine-treated patients, specifically increased hypersensitivity reactions in pediatric patients (Amstutz et al., 2018). In addition, patients with the HLA-B 1502 allele and of Asian ancestry are at an increased risk of Stevens–Johnson syndrome and toxic epidermal necrosis with carbamazepine treatment (Amstutz et al., 2018).
The FDA recommends genetic screening of HLA-B*1502 for those of Southeast Asian ancestry before starting carbamazepine (Amstutz et al., 2018). Since we cannot be certain about someone's ancestry without genomic analysis, both HLA-B*1502 and HLA-A*3101 testing should be considered before carbamazepine use in a naive person. Similarly, the HLA-A 3101 genotype increases the risk of Stevens–Johnson's syndrome, hypersensitivity syndrome, and other adverse outcomes with carbamazepine use across those of European and Southeast Asian descent (Yip and Pirmohamed, 2017).
Available Resources to Support the Use of PGx Information
A growing body of mechanistic, preclinical, and clinical data detail the clinical value of PGx in guiding drug dosing or selection for psychotropic medications in youth (Bousman et al., 2021a). CYP2D6, CYP2C19, CYP2B6, HLA-B, and HLA-A are key genes incorporated into evidence-based guidelines for various antidepressants, antipsychotics, attention-deficit/hyperactivity disorder (ADHD) medications, and mood stabilizers commonly used in youth (Beunk et al., 2023; Bousman et al., 2023; Brouwer et al., 2022; Brown et al., 2019; Hicks et al., 2017; Nijenhuis et al., 2023; Phillips et al., 2018) (Table 6).
Genes with Evidence to Support Drug Dosing or Selection Strategies for Mental Health Medications
Based on CPIC Guidelines, international guideline groups, or tables 1 and 2 of the FDA Table of Pharmacogenetic Associations.
CPIC, Clinical Pharmacogenetics Implementation Consortium; CYP, cytochrome P450; FDA, Food and Drug Administration; HLA, human leukocyte antigen.
To enhance the evidence-based application of PGx for psychotropic medications, familiarity with resources such as the CPIC, the Pharmacogenomics Knowledgebase (PharmGKB), the FDA Table of Pharmacogenetic Associations, and Sequence2Script is essential (Table 4).
Clinical Pharmacogenetics Implementation Consortium
The CPIC is a National Institutes of Health-supported, evidence-based, and peer-reviewed resource to support the clinical implementation of available PGx data into clinical practice (Caudle et al., 2014). These guidelines are freely available and generated from an expert consensus evaluation of a comprehensive compilation of published literature. CPIC guidelines and therapeutic recommendations are generated by international author groups representing methodological, therapeutic, and end-user expertise. Studies meeting inclusion criteria agreed upon by the guideline committee are reviewed, assigned a quality metric, and major findings from each publication are extracted.
Major findings statements are collated across studies with a consensus evidence grade determined for each. Therapeutic recommendations are generated from the major findings with a classification of weak, moderate, or strong assigned to each based on the agreed-upon strength of evidence supporting the statement (e.g., no recommendation, optional, moderate, or strong). At the CPIC website (
This searchable table provides information on the CPIC level of evidence for the gene–drug pair (A, B, C, or D) where levels A or B are considered to have evidence supporting the use of existing genotype information to guide selection or dosing of the paired drug (Fig. 3). This table also notes the presence of PGx information in the FDA label and links to any published guidelines for the selected pair. It is important to note that CPIC guidelines provide evidence-based guidance on what to do with existing/available genotype information, but not which patients to test or when a test should be obtained.
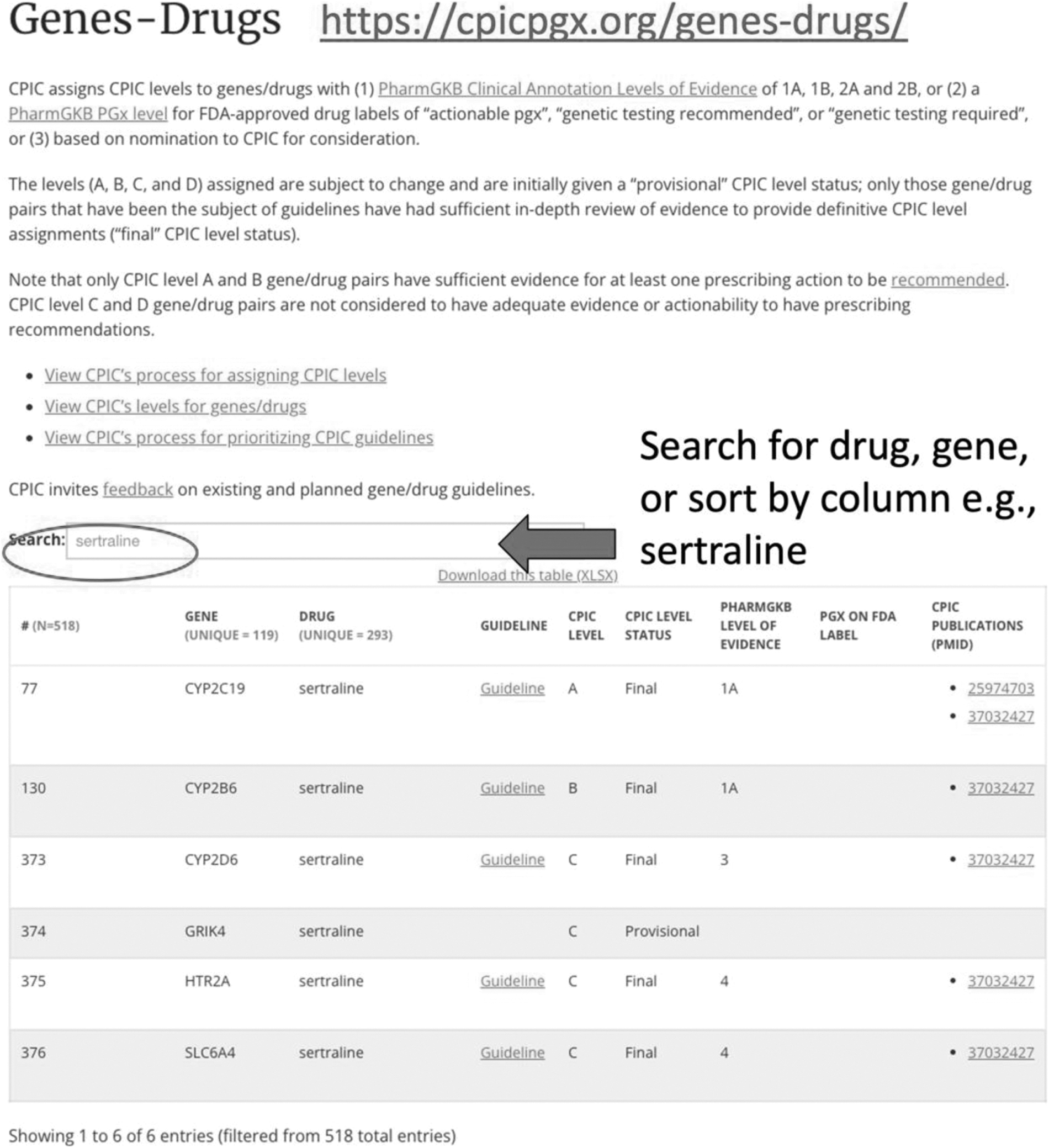
Clinical Pharmacogenetics Implementation Consortium Search for Drugs and Genes.
Pharmacogenomics Knowledgebase
The PharmGKB is a web-based resource that collates and disseminates knowledge about gene–drug associations and genotype–phenotype relationships (Caudle et al., 2016). PharmGKB is a good resource to learn more about specific genes and obtain executive summaries, detailed summaries, or links to primary literature for genes and drugs.
As a practical example, if a gene is included on a PGx testing panel that a clinician would like to learn more about, this is a user-friendly source for this information. This is important because different testing panels may contain differing lists of genes, and genes returned on clinically available PGx test panels do not all have the same level of evidence supporting clinical utility.
At the PharmGKB homepage (
The FDA Table of Pharmacogenetic Associations
The FDA recently developed a reference Table of Pharmacogenetic Associations (
The specificity of the information provided varies based on when a drug was evaluated and approved and which information sponsors elected or were required to submit. For example, language in older drug labeling is often not specific (e.g., “Poor metabolizers of CYP2D6 will metabolize perphenazine more slowly and will experience higher concentrations compared with normal or ‘extensive’ metabolizers”) to describe PK observations available at the time of drug approval.
Newer drug approvals may contain more specific information about genotype, phenotype, drug–gene effect, and clinical management implications (e.g., for citalopram: “The maximum dose should be limited to 20 mg once daily in patients who are CYP2C19 poor metabolizers”).
Despite the singularity of its name, this resource comprises three tables, stratified by the FDA's current assessment of clinical utility: Section (1) Pharmacogenetic Associations for which the Data Support Therapeutic Management Recommendations, Section (2) Pharmacogenetic Associations for which the Data Indicate a Potential Impact on Safety or Response, and Section (3) Pharmacogenetic Associations for which the Data Demonstrate a Potential Impact on Pharmacokinetic Properties Only.
In addition to the earlier caveats regarding variability in FDA product labeling, it is important for viewers to be aware that the content may be subject to some further review. One notable example is an actionable clozapine-CYP2D6 consideration in Section (1), where more contemporary reviews and data syntheses note that this is likely not clinically relevant (Beunk et al., 2023; Lesche et al., 2020; Milosavljevic et al., 2021).
A second example includes citalopram and escitalopram, which are positioned separately in Sections (1) (actionable) and (3) (PK impact only), respectively, whereas recent consensus evaluations note that the PGx implications are the same for these two related drugs (e.g., escitalopram is the s-isomer of citalopram) (Bousman et al., 2023). Despite these limitations, some third-party reimbursement guidelines for PGx tests reference FDA-sourced information, making awareness of this regulatory resource important (Fahim et al., 2023).
Sequence2Script
Sequence2Script is a free online tool to help health care clinicians and clinical laboratories translate pharmacogenetic test results into clinically useful recommendations (
The information entry portal also allows users to enter medications that are being considered so that the report generated focuses on medications relevant to the end user. The recommendations generated by this tool are based on expert peer-reviewed guidelines developed by the CPIC, an international guideline group called the DPWG, and the FDA. This is a resource, where users can enter genotypes obtained from a clinical laboratory into the database, which then creates a report populated by the recommendations for each of the CPIC, DPWG, and FDA resources so they can be viewed together. This is helpful for clinicians to evaluate consistencies to make an informed decision on how or whether to consider PGx information.
PGx-Informed Therapeutic Recommendations
PGx information should support or supplement an evidence-based drug selection process. The test results should not be the driver used to guide drug selection. Similarly, PGx results should not be used to create a truncated list of medications to choose from. The reason for this is that drug–gene interactions may not necessarily require complete avoidance of medications (e.g., in the case of dose adjustments or refining titration schedules) that may be preferred treatments for youth. The spirit of this approach is that PGx information should be used to refine an evidence-based selection of medications in the context of the patient's other unique characteristics.
Clinical PGx reports commonly highlight potential drug–gene interactions, although the presentation of this information may differ across laboratories. Some commercially available laboratories include variations of “minor, moderate, major,” “use as directed, caution, avoid,” or stoplight color-coding. Stoplight colors red, yellow, and green are intended to improve the understanding of test results, but green and red may also convey interpretations of “use this medication” or “stop taking this medication.”
Although categorical groupings are intended to improve clinician and patient understanding of test results, a critical evaluation of the clinical relevance of specific drug–gene interactions (vs. categorical groupings) in the context of patient-specific factors is needed to embrace a person-centered approach to care (vs. a laboratory report-centered approach).
These may include factors that may biologically moderate the severity of a drug–gene interaction or likelihood of clinical relevance (e.g., concomitant enzyme inhibitors or inducers, renal function, liver function, PD drug interactions, smoking status, age, weight, and sex). Patient-specific factors to consider also include response and tolerability to other medications, concomitant disease states, health care access, and financial factors that may influence the accessibility of some options.
To provide a summary of this important clinically relevant information, we created tables regarding CPIC lines of evidence (Table 3) (CPIC, 2022); genes with evidence to support drug dosing or selection strategies for psychotropic medications (Table 6); resources to access and evaluate evidence-based pharmacogenomic information (Table 4); and a comprehensive table reviewing different classes of commonly used medications with appropriate guidelines (Table 5).
Conclusion
Pharmacogenomics holds the promise of improving the use of psychotropic medications in pediatric patients by incorporating genetic data to assist clinicians in making more informed choices regarding medication selection and dosage. There is now an abundance of available resources to aid clinicians in applying these insights using up-to-date evidence-based recommendations.
In 2020, we introduced a clinical workflow that advocated for a systematic approach to determine when and at which stage of the clinical evaluation process pharmacogenetics should be employed (Ramsey et al., 2021). We suggested that, after a comprehensive clinical evaluation and a confirmed need for pharmacotherapy, pharmacogenetic testing, if available and if specific recommendations existed for that particular medication, should be used to tailor treatment.
Given the existing evidence supporting specific gene–medication associations, we now propose that for medications with actionable recommendations based on CPIC guidelines, pharmacogenetic testing should be strongly considered. As our knowledge expands, it is likely that data for additional relevant gene–medication relationships will emerge.
In essence, this field is rapidly advancing, and with a collective commitment from our community to enhance clinician education and promote ongoing research and technological advancements, pharmacogenomics has the potential to become a valuable component of pediatric psychiatry, ultimately improving treatment outcomes for children and adolescents with psychiatric disorders.
Footnotes
Authors' Contributions
Conceptualization (lead), writing (original draft), review, and editing by S.M. Writing (original draft), review, editing, and visualization (equal) by P.V. Conceptualization; writing (original draft), review, editing, and visualization (equal) by G.R. Visualization; writing (original draft), review, and editing (equal) by A.A.S. Writing (original draft), review, and editing (equal) by A.D. Writing (original draft; supporting), review, and editing (equal) by J.R.B. and J.R.S. Conceptualization (supporting), writing—original draft (equal), and writing—review and editing (equal) by L.B.N.
Disclosures
Dr. Strawn has received research support from PCORI, the National Institutes of Health, and the Yung Family Foundation. He has provided consultation to Cerevel, Intracellular Therapeutics and the Roche. He receives royalties from Springer Publishing, Cambridge University Press, and UpToDate and receives material support from Myriad. He has also received honoraria from Medscape Live and Neuroscience Education Institute.” Dr. Bishop has served as a consultant to OptumRx. Dr. Namerow provided and hour of CME to Genomind. Dr. Malik, Dr. Ruaño, Dr. Verma, Ms. Dilawar, Dr. Alsiaghy report no disclosures.