
Abstract
Objective:
Evidence for pharmacogenomic (PGx) guided treatment in child and adolescent psychiatry is growing. This study evaluated the impact of PGx testing on psychotropic medication prescribing in an ambulatory child and adolescent psychiatry and a developmental pediatrics clinic.
Methods:
This was a single-center, retrospective, descriptive analysis of patients who underwent PGx testing between January 2015 and October 2022 at a child and adolescent psychiatry clinic or developmental pediatrics clinic. The primary outcome was the proportion of patients with at least one psychotropic medication modification made 6-month posttesting that could be attributed to CYP2C19, CYP2D6, HLA-B*15:02, or HLA-A*31:01. Secondary outcomes included reason for testing, types of therapeutic modifications made, and whether the therapeutic modifications concorded with PGx guidelines.
Results:
A total of 193 patients were analyzed. The average age was 10 ± 4 years old, 60% were male, 78% were Caucasian. Sixty-eight percent had a primary diagnosis of a neurodevelopmental disorder, namely autism spectrum disorder (51%), and attention-deficit/hyperactivity disorder (14%). The reasons for PGx testing included medication inefficacy (34%), medication intolerance (20%), and family request (19%). At the time of PGx testing, 37% of patients were taking ≥1 psychotropic medication with PGx annotation. Overall, 35 PGx-related therapeutic modifications were made in 32 (17%) patients. These included continuing current PGx medication (6.2%) and starting PGx medication (5.2%). These modifications mainly involved antidepressants. Out of these 35 PGx-related therapeutic modifications, 94% were concordant with PGx guidelines. Among 29 patients who were prescribed at least one CYP2D6 inhibitor, 25 (86%) underwent CYP2D6 phenoconversion.
Conclusions:
It is critical to apply pediatric age-specific considerations when utilizing PGx testing in child and adolescent psychiatry. PGx testing stewardship could provide a framework to guide the clinical utility of PGx in a pediatric population with mental health conditions, including neurodevelopmental disorders.
Introduction
It is estimated that 25% of youth are diagnosed with a mental health condition and that 8%–12% are prescribed a psychotropic medication, with stimulants, nonstimulants (i.e., alpha-2 agonists), antidepressants, and atypical antipsychotics among those most frequently prescribed (Stutzman, 2021). Given pediatric-specific risk for adverse effects and variable rates of treatment response, there is interest in genotype-guided prescribing among children and adolescents to prevent adverse reactions and optimize therapeutic response (Poweleit et al., 2019; Ramsey et al., 2020). Widespread clinical implementation is challenging given the limited pediatric-specific pharmacogenomic (PGx) guidelines, development-related (ontogeny) effects on drug metabolizing enzyme maturation, and limitations of commercially available pharmacogenetic tests (Ramsey et al., 2020; Wehry et al., 2018). In the setting of these limitations, the American Academy of Child and Adolescent Psychiatry issued a recommendation to avoid using PGx testing to select psychotropic medications in children and adolescents, and that high-quality prospective studies are needed (AACAP, 2020; Brown et al., 2021; Claudio-Campos et al., 2021; Olson et al., 2017; Wehry et al., 2018).
Questions still exist regarding the most appropriate timing of testing, which genes to test, and which pediatric patient populations benefit most from testing. While psychotropic medications are of high interest, most PGx studies are conducted in adults with pediatric patients often excluded, including those with neurodevelopmental disorders, intellectual disabilities (IDs), and those with multiple previous medication trials. This study aims to evaluate the impact of PGx testing on psychotropic medication prescribed in an ambulatory care developmental pediatrics and a child and adolescent psychiatry clinic.
Methods
Study design
This was a retrospective chart review and descriptive analysis of pediatric patients who underwent PGx testing at an ambulatory care developmental pediatrics clinic or child and adolescent psychiatry clinic at Children's Hospital Colorado in Aurora, Colorado between January 1, 2015 and October 1, 2022. The study was approved by the Colorado Multiple Institutional Review Board with a waiver of informed consent.
PGx testing and participants
Children's Hospital Colorado is a quaternary care pediatric hospital with a variety of specialty ambulatory care clinics including child and adolescent psychiatry and developmental pediatrics. PGx testing was ordered at the discretion of the provider, using a commercial 28-gene PGx panel (OneOme® RightMed Comprehensive test, Minneapolis, MN). Our study focused on four genes (CYP2C19, CYP2D6, HLA-B*15:02, and HLA-A*31:01) with PGx guidance available from the Clinical Pharmacogenetics Implementation Consortium (CPIC), the Dutch Pharmacogenetics Working Group (DPWG), and Food and Drug Administration (FDA) label for psychotropic medications. DNA was collected using a buccal swab which was sent to OneOme LCC (Minneapolis, MN) for genotyping. The results were uploaded as a portable document format in the electronic medical record (EMR; Epic systems, Verona, WI) as no PGx clinical decision support tool was available. The results were reviewed by the provider and/or pharmacist (upon request) to guide treatment decisions. At the time of test review, providers and/or pharmacists had access to the 2015 CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors, 2016 CYP2D6 and CYP2C19 Genotypes and Dosing of Tricyclic Antidepressants, 2017 HLA Genotype and Use of Carbamazepine and Oxcarbazepine, and 2019 CYP2D6 Genotype and Atomoxetine CPIC Guidelines (Brown et al., 2019; Hicks et al., 2017; Hicks et al., 2015).
Patients were included if they were below 21 years old, and PGx testing was ordered at the child and adolescent psychiatry or developmental pediatrics clinics. Patients were excluded if the test was ordered by other clinics, a PGx test other than OneOme was used, or a patient had no follow-up visit 6-month posttesting to evaluate.
Study outcomes
The primary outcome was to describe the proportion of patients with at least one psychotropic medication change made due to PGx results within 6-month posttesting. Secondary outcomes included (1) reason for testing and (2) the therapeutic modification made with PGx-annotated psychotropic medications post-PGx testing.
Data collection
Data collected from the EMR included age, sex, race, ethnicity, primary Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) diagnoses, medical comorbidities, baseline psychotropic medications at the point of PGx testing, prior psychotropic medications trialed, reason for testing, therapeutic modifications made with psychotropic medications attributable to PGx (defined as starting new medication, continue current medication, change medication, change dose, or add PGx information to chart) within 6-month posttesting, and documented reason for the modification made. The therapeutic modifications were also evaluated to determine if the medication changes made were concordant with CPIC, DPWG, or FDA label PGx recommendations for the respective phenotypes. The turnaround time between sample collection to receiving PGx results was also evaluated.
The CYP2C19, CYP2D6, HLA-B*15:02, and HLA-A*31:01 genotypes were extracted from patient's OneOme laboratory report. This study followed the CPIC's CYP2C19 and CYP2D6 phenotype classification. We acknowledged that OneOme used their own CYP2D6 phenotype classification in their reports. Patients who were exposed to a moderate (e.g., duloxetine) or strong CYP2D6 inhibitor (e.g., bupropion, fluoxetine, or paroxetine) during the study period were evaluated for CYP2D6 phenoconversion as previously described (Cicali et al., 2021).
Statistical analysis
Descriptive statistics were utilized to analyze patient demographics and clinical characteristics. Data were presented as mean ± standard deviation (SD) for continuous variables, and frequencies (percentages) for categorical variables. Analyses were conducted using IBM SPSS Statistics (Version 29, Armonk, NY).
Results
Patients
A total of 336 patients underwent PGx testing during the study period. One hundred forty-three patients were excluded, leaving 193 patients in the final analysis (Fig. 1). Table 1 summarizes the baseline patient demographics. The mean (SD) age was 10.6 ± 4.2 years (range 2–19 years), 60% were male, and 78% were Caucasian. The primary DSM-5 diagnoses were a neurodevelopmental disorder (68%) followed by anxiety disorder (18%), and depressive disorder (16%). Further analysis of DSM-5 diagnoses showed about half of the cohort had autism spectrum disorder (ASD; 51%), followed by attention-deficit/hyperactivity disorder (ADHD; 14%), generalized anxiety disorder (11%), and major depressive disorder (8%). IDs (4%) was present in a small proportion of patients.

Study flow. PGx, pharmacogenomics.
Patient Demographics
Some patients had more than one reason for PGx testing.
DSM-5, Diagnostic and Statistical Manual 5th Edition; PGx, pharmacogenomics; SD, standard deviation.
Most of the patients were from the developmental pediatrics clinic (68%) with PGx testing ordered by a developmental pediatrician (61%). Most of the patients did not have a documented reason for PGx testing (41%). Among those with a documented reason, PGx testing was initiated due to medication inefficacy (34%) followed by medication intolerance (20%), and family request (19%). The average number of failed psychotropic medication was 1.8 ± 1.9 per patient (range 0–9 medications), with the top 10 medications being methylphenidate (24%), guanfacine (21%), sertraline (17%), fluoxetine (16%), mixed amphetamine salt (15%), clonidine (12%), risperidone (11%), aripiprazole (8%), lamotrigine (8%), and atomoxetine (8%) (Fig. 2). Among these medications, sertraline, aripiprazole, and atomoxetine had PGx annotations.
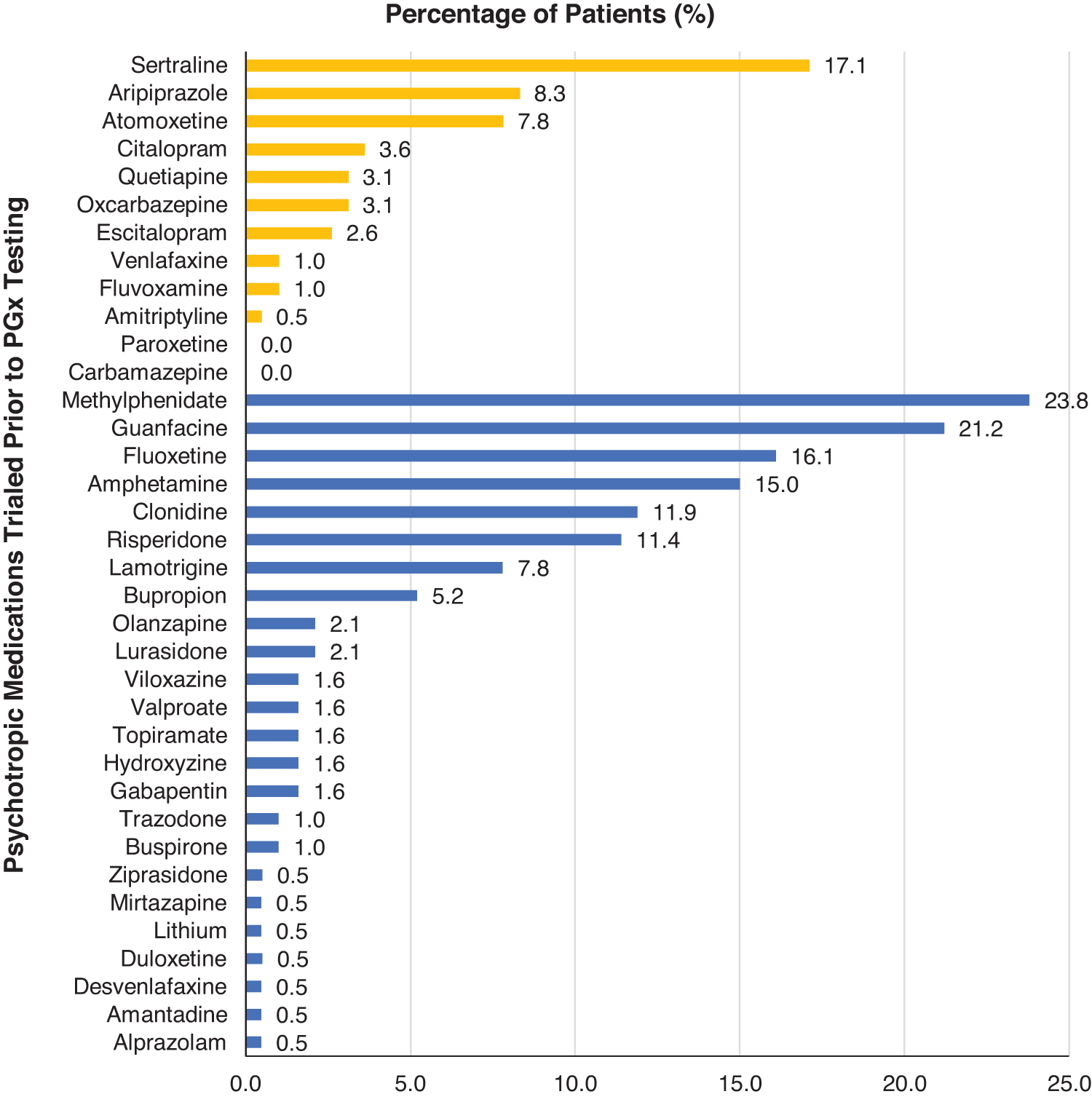
Psychotropic medications trialed before PGx testing with PGx annotation (yellow) and without PGx annotation (blue) in the study cohort (n = 193). PGx, pharmacogenomics.
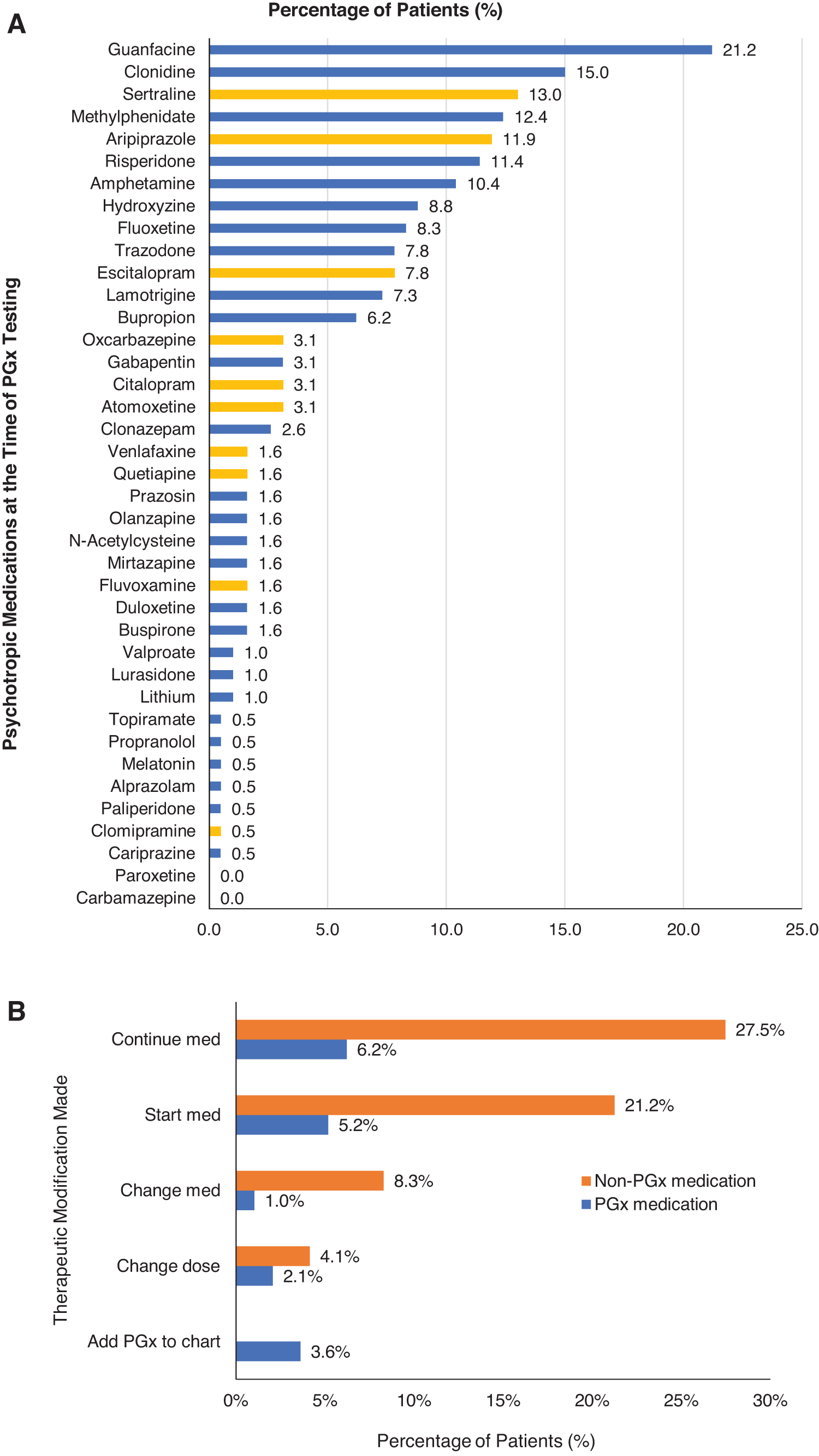
The most common psychotropic medications taken at the time of PGx testing were alpha-2 agonists (guanfacine 21%, clonidine 15%), antidepressants (sertraline 13%), stimulants (methylphenidate 12%), followed by atypical antipsychotics (aripiprazole 12%, risperidone 11%) (Fig. 3A). At the point of PGx testing, 37% of the patients were taking at least one PGx-annotated psychotropic medication with sertraline (13%) being the most common followed by aripiprazole (12%) and escitalopram (8%). The average turnaround time to receive PGx results was 9 days (range 3–14 days). The frequency distribution of CYP2C19 and CYP2D6 phenotypes was comparable to that for Europeans (PharmGKB) (Table 2). Out of 193 patients, 29 patients (15%) were exposed to at least one CYP2D6 inhibitor with 25 (86%) of these patients undergoing CYP2D6 phenoconversion.
HLA-B*15:02, HLA-A*31:01, CYP2D6 and CYP2C19 Phenotype Distribution and the Proportion of Patients Who Were Prescribed CYP2D6 Inhibitor with the Phenotype Frequencies Pre- and Post-CYP2D6 Phenoconversion
Some patients were exposed to more than one CYP2D6 inhibitor during the study period.
Study outcomes
For the primary outcome, 32 (17%) patients had 35 documented PGx-related therapeutic modifications (Fig. 3B; Table 3). These PGx-related therapeutic modifications were to continue current PGx-annotated psychotropic medication (6.2%), start new medications (5.2%), add PGx information to patient's chart (3.6%), change dose (2.1%), followed by change in medication (1.0%). The PGx medications continued were primarily selective serotonin reuptake inhibitor (SSRI)/serotonin norepinephrine reuptake inhibitor (i.e., escitalopram, sertraline, venlafaxine) and atypical antipsychotic (i.e., aripiprazole) (Supplementary Table S1). The PGx psychotropic medications started included SSRIs (i.e., escitalopram, fluvoxamine, sertraline), atypical antipsychotic (aripiprazole), and nonstimulant (viloxazine). Although 17 patients were positive for HLA-variants, 3 patients had this information added to their charts. Two patients had a note added that PGx results were available to inform future prescribing; while two patients had a note to avoid thioridazine due to their CYP2D6 phenotype added.
Types of Pharmacogenomic Therapeutic Modifications Made and the Psychotropic Medications Involved
Some patients have more than one PGx-guided therapeutic modification.
PGx, pharmacogenomics.
In contrast, more non-PGx-related therapeutic modifications were made, namely, to continue current non-PGx psychotropic medication (27.5%), start non-PGx psychotropic medication (21.2%), change medication (8.3%) followed by change in dose (4.1%). The non-PGx psychotropic medications continued included nonstimulants (i.e., clonidine, guanfacine), stimulants (i.e., amphetamine salts, methylphenidate), antipsychotics (risperidone), and mood stabilizers (i.e., lamotrigine, valproate). Among the new non-PGx medications started, half of them involved L-methylfolate followed by stimulants (i.e., amphetamine salts, methylphenidate), antidepressants (i.e., bupropion, desvenlafaxine, fluoxetine), and other psychotropics.
Out of 35 PGx-related therapeutic modifications, 33 (94.3%) were concordant with PGx recommendations based on CPIC, DPWG, or FDA label (Supplementary Table S1). Among the two discordant cases, one patient (Patient #15) was started on standard aripiprazole dose since the PGx report showed CYP2D6 normal metabolizer phenotype. This patient was on fluoxetine which phenoconverted the patient to be a CYP2D6 poor metabolizer. Consequently, the aripiprazole dose should have been reduced per FDA label recommendation. The second case (Patient #105) involved continuing aripiprazole in a patient whose commercial report showed “CYP2D6 intermediate to poor metabolizer (range).” Based on CPIC's CYP2D6 classification (Caudle et al., 2020), patient was a CYP2D6 intermediate metabolizer. The provider regarded patient as a poor metabolizer but continued aripiprazole since a very low dose was used, but wrote in the chart to apply further (dose) increases with caution, with “no plan to make any changes at this time since no side effects have been experienced.”
Discussion
Our study evaluated the impact of PGx testing on psychotropic medication prescribing in an ambulatory child and adolescent psychiatry and developmental pediatrics clinic where most patients (68%) had a primary diagnosis of a neurodevelopmental disorder, namely ASD followed by ADHD. The majority had trialed or were taking alpha-2 agonists (i.e., clonidine and guanfacine) and stimulants (i.e., methylphenidate), targeting hyperactivity, inattentiveness, and impulsivity, symptoms commonly seen in youth with ADHD and ASD (Hyman et al., 2020). Therapeutic modifications made posttesting mainly involved non-PGx psychotropic medications, including continue current non-PGx medication (28%; e.g., stimulants, nonstimulants), start non-PGx medication (21%; e.g., L-methylfolate), followed by change non-PGx medication (8%).
Adding L-methylfolate in response to the methylenetetrahydrofolate reductase (MTHFR) genetic result was a surprising finding, as evidence to support supplementation based on MTHFR status is conflicting in pediatric patients (Dartois et al., 2019). While a case series have suggested improvements in depression, anxiety, and irritability in youth treated with L-methylfolate as adjunct to antidepressant therapy, systematic evaluation of this treatment strategy is needed to fully understand its role in treatment, optimal pediatric dosing, duration of treatment, and pharmacogene impact (Dartois et al., 2019).
At the time of PGx testing, 72 patients (37%) were prescribed at least one psychotropic medication with a PGx annotation. Posttesting, 17% (n = 32) of patients had PGx-related therapeutic modifications (N = 35), which were predominantly antidepressant-related, most often supporting continuation of or initiating a new antidepressant. Acknowledging high comorbid rates of anxiety in youth with neurodevelopmental disorders, antidepressant continuation, or initiation was expected (Hyman et al., 2020; Wolraich et al., 2019). Additionally, this aligns with current pediatric PGx studies that primarily focus on CYP2C19 and CYP2D6 associations with antidepressant side effects or treatment outcomes (Claudio-Campos et al., 2021; Namero et al., 2020; Roberts et al., 2021).
Notably, one study found that among children and adolescents (N = 263) admitted to a children's hospital, those with reduced CYP2C19 function had more side effects, higher discontinuation rates, and increased likelihood of additional psychiatric inpatient days. Interestingly, metabolizer phenotype did not influence the overall proportion of responders (Aldrich et al., 2019). The ability to predict antidepressant side effects in youth with ASD is particularly appealing, given higher rates of adverse effects (e.g., irritability, gastrointestinal upset) in this group (Stutzman et al., 2023).
Our findings highlight the importance of PGx testing stewardship in child and adolescent psychiatry. Similar to antimicrobial stewardship, psychotropic stewardship has been proposed as a model to optimize psychotropic prescribing in children and adolescents through a patient-centered, interprofessional, and collaborative model to optimize evidence-based and value-based outcomes (e.g., metabolic monitoring with atypical antipsychotics) (Haight et al., 2023; Stutzman et al., 2023).
Optimal age for PGx testing, which pharmacogenes to test, and how to integrate the PGx results throughout patient's lifetime in the pediatric health system as the child develops must all be considered to inform PGx stewardship. While our study cannot fully address all these considerations, our unique study population and clinic settings offer a real-world perspective of young patients with neurodevelopmental disorders and co-occurring physical health and mental health comorbidities.
Another study evaluating prescribing outcomes post PGx testing in youth with neurodevelopmental disorders reported that 34% of patients started new medications, while 51% continued current medications (Patel et al., 2020). Notably, this study group used a PGx algorithm that incorporated actionable (e.g., CYP2C19, CYP2D6) and nonactionable (e.g., adrenergic alpha-2 receptor and catechol-o-methyltransferase) results to provide recommendations under three categories: “use as directed,” “use with caution,” and “use with increased caution.” In contrast, our study focused on actionable pharmacogenes (i.e., CYP2C19, CYP2D6, and HLA-genes), and we had lower rates of PGx-related therapeutic modifications (6.2% continue current medications, 5.2% start PGx medications). Additionally, our study reviewed the 35 PGx-related therapeutic modifications and found 94% were concordant with PGx recommendations.
The ontogenic or age-dependent changes on gene expression is a critical developmental factor to consider when applying pediatric PGx results in clinical practice to children at different stages of development (Bousman et al., 2021; Hoshitsuki et al., 2021; Ramsey et al., 2021; Ramsey et al., 2020; Wehry et al., 2018). Not all pharmacogenes follow the same ontogenic profile. For instance, CYP2D6 enzyme activity matures as early as 2 weeks after birth (Blake et al., 2007), while CYP2C19 enzyme activity increases to at least 1.5 times adult values during childhood and then decreases to adult levels by the end of puberty. Among our young patient cohort, many were prescribed antidepressants primarily metabolized by CYP2C19, namely escitalopram, citalopram, and sertraline.
While all the therapeutic modifications related to CYP2C19 and antidepressants were concordant with PGx recommendations in our study, there was no documentation suggesting the consideration for ontogeny. The two discordant cases involved CYP2D6: with one due to phenoconversion by a concurrent strong CYP2D6 inhibitor, while the other was related to the CYP2D6 phenotype classification adopted by the commercial company. The impact of CYP2C19 metabolizer status on serum concentrations of escitalopram, citalopram, and sertraline have been evaluated by other studies that found variable impact on ability to predict response in pediatric patients, highlighting the developmental complexity aspect of applying pediatric PGx (Aldrich et al., 2019; Brown et al., 2022; Strawn et al., 2019; Ramsey et al., 2019; Thiele et al., 2022).
While panel-based PGx testing may be cost-effective compared to ordering single gene tests, caution is warranted with interpretation as many panel-based reports use combinatorial clinical-decision based algorithms that incorporate genes with weak evidence. When reviewing these reports, it is essential to consider CYP2D6 and CYP2C19-based PGx guidelines for certain antidepressants and antipsychotics, and HLA-based guidelines for mood stabilizers. Pertinent to our patient population, these results can also be used to inform the prescribing of PGx-annotated medications for other comorbidities, such as antiseizure medications, antimicrobials, and gastrointestinal medications, which also have PGx guidelines (Ramsey et al., 2020).
While PGx guidelines are not available for alpha-2 agonists and stimulants, medications frequently prescribed in our patient population, guidance for CYP2D6-atomoxetine, CYP2D6-aripiprazole, and CYP2D6/CYP2C19-antidepressants suggest potential clinical utility of PGx testing in youth with neurodevelopmental disorders given high rates of cooccurring anxiety, depression, and ADHD. Notably, updated CPIC guidelines pertaining to serotonin reuptake inhibitors and CYP2C19/CYP2D6 were published since this retrospective review. While they were not available to inform clinical decision-making, they were considered in the review of the retrospective data.
Our study has several limitations. This was a single-center, descriptive, retrospective chart review that relied on chart documentation. While our study described utilization and application of PGx testing in two unique pediatric clinic settings, ongoing studies are needed to evaluate its impact on clinical care. This warrants careful consideration for improvement in treatment outcomes among diverse pediatric populations. We hoped to evaluate clinical outcome measures in our clinic populations to assess the impact of PGx testing on clinical care, but low adherence to measure completion made this unsuccessful. Future studies should evaluate improved medication efficacy (e.g., rates of recovery, remission), tolerability, and safety outcomes (e.g., significant adverse effects). While our study cohort represents real-world clinical settings (e.g., many previous medication trials, psychiatric and physical health comorbidities), the majority were Caucasian limiting broad generalizability. Lastly, this study did not evaluate other PGx drugs such as CYP3A4 for quetiapine and CYP2B6 for sertraline.
These findings add value to the available literature given that pediatric patients with cooccurring neurodevelopmental disorders and physical health comorbidities are often excluded in PGx literature (Bose-Brill et al., 2017; Hefti and Blanco, 2017). Pediatric patients with neurodevelopmental disorders are vulnerable to polypharmacy making them favorable candidates for PGx testing, although specific guidelines are lacking. More prospective studies are needed to clearly identify reasons for testing, PGx-related medication changes made, the clinical outcome of PGx-related medication changes, and optimal timing of PGx testing.
Next steps for enhanced integration of pediatric PGx in clinical practice include implementing a PGx testing stewardship within the pediatric population that takes into account pediatric ontogeny, and the impact of interacting drugs that may cause phenoconversion. This may include optimization of clinical decision support tools within the EMR to alert providers on the limitations of interpreting certain PGx results for certain genes and patient age groups, while other genetic results such as HLA-related genes are independent of age. Another resource to facilitate PGx testing stewardship is the involvement of pediatric/psychiatric pharmacists who already provide input on medication selection and dosing (Brown et al., 2018; Kennedy et al., 2011). Finally, other supports can include accessibility of genetic information for patients, families, and providers, and elimination of barriers to testing (e.g., cost and availability).
Conclusions
It is critical to apply pediatric age-specific considerations when utilizing PGx testing in child and adolescent psychiatry. As more pediatric PGx studies are being conducted and the pediatric PGx landscape evolves, PGx testing stewardship can facilitate the appropriate use of PGx results in addition to the evolving clinical factors in a child's journey through a health care system.
Footnotes
Clinical Significance
This study provides a unique description of PGx testing in youth with neurodevelopmental disorders.
Disclosures
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.