
Abstract
S
In 2019, the Joint Commission (TJC) revised its guidelines on suicide risk screening, requiring the use of a validated screening tool for suicidal ideation in all individuals aged ≥12 years treated in a behavioral health setting. In December 2019, our university-affiliated urban multidisciplinary center serving children with I/DD established a model of feasible and routine suicidality screening for children aged ≥10 years, incorporating a screening tool, Ask Suicide-Screening Questions (ASQ), at the initial visit of the multidisciplinary evaluation. The objectives of this study were to examine compliance with universal suicide risk screening using the ASQ and the prevalence of positive suicide screening in youth with I/DD.
A review was conducted of all children aged ≥10 years who presented for their initial visit in 2020. Data reviewed included demographics, use of ASQ, and patient's developmental diagnoses. With the onset of the COVID-19 pandemic, our center's initial visits were converted from in-person to telehealth in March 2020, so we compared rates of screening by type of visit (in-person vs. telehealth). Descriptive statistics were used to summarize the collected information. Statistical analysis included chi-square and independent t-test. This study was approved by the Montefiore Institutional Review Board.
In 2020, 213 children (aged ≥10 years) were seen for an initial visit, 188(88%) were verbally/cognitively able to complete the ASQ (as determined by evaluator). The other 25 (12%) of patients were either documented to be nonverbal or were documented as unable to understand or respond to the ASQ when it was attempted. In total, 50 (26%) patients were seen in-person and 138 (74%) through telehealth. The ASQ was administered to 111 (59%) of the patients, and 5 screened positive: 3 females, 2 males, average age 12.7 ± 2 years old. One had a diagnosis of autism spectrum disorder (ASD) and learning disability, one of ADHD, and three did not complete the multidisciplinary evaluation (lost to follow-up). Two had a family history of depression and one of schizophrenia. Positive screens were further evaluated and found to be low risk.
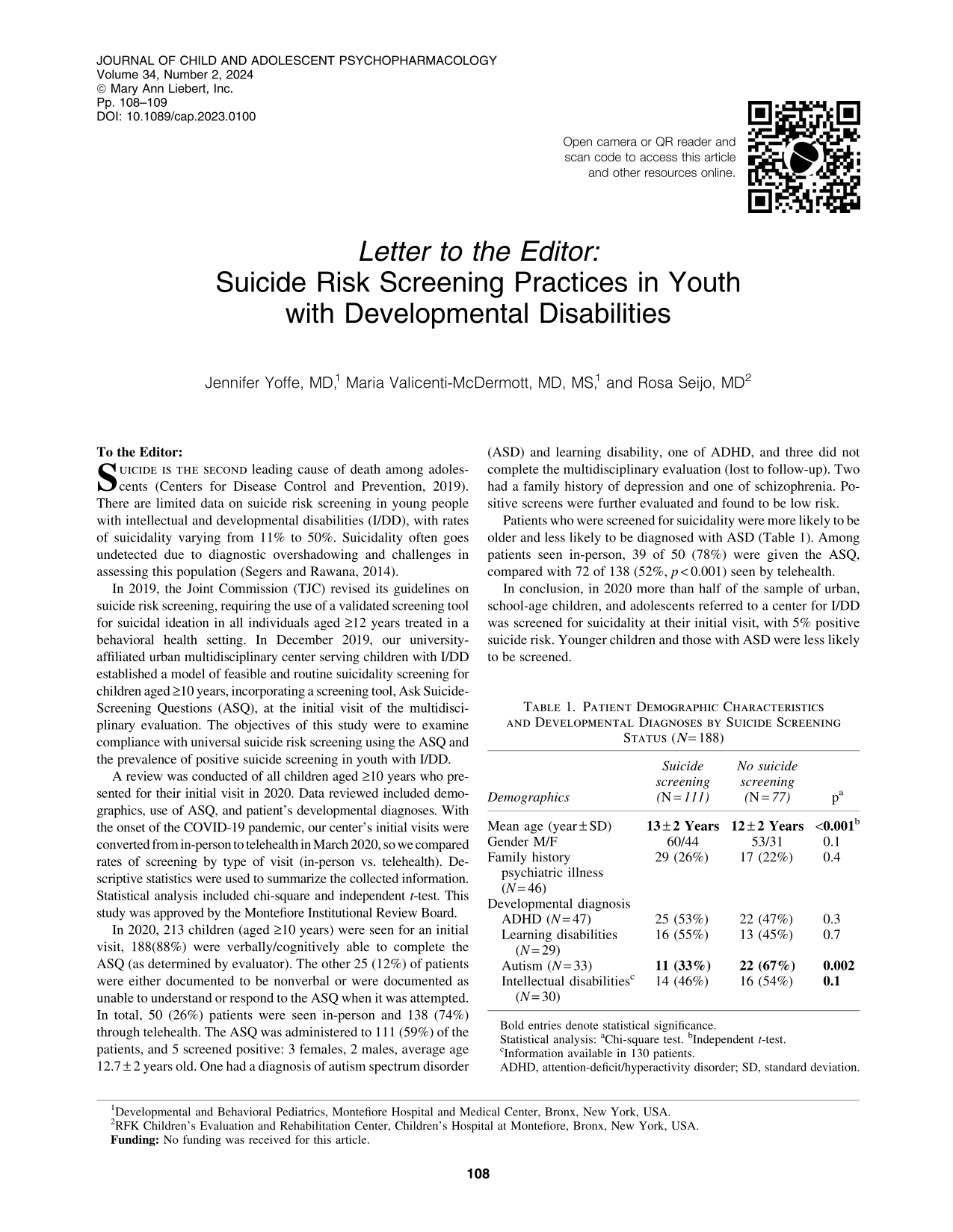
Patients who were screened for suicidality were more likely to be older and less likely to be diagnosed with ASD (Table 1). Among patients seen in-person, 39 of 50 (78%) were given the ASQ, compared with 72 of 138 (52%, p < 0.001) seen by telehealth.
Patient Demographic Characteristics and Developmental Diagnoses by Suicide Screening Status (N = 188)
Bold entries denote statistical significance.
Statistical analysis: aChi-square test. bIndependent t-test.
Information available in 130 patients.
ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation.
In conclusion, in 2020 more than half of the sample of urban, school-age children, and adolescents referred to a center for I/DD was screened for suicidality at their initial visit, with 5% positive suicide risk. Younger children and those with ASD were less likely to be screened.
This study is one of few looking into suicide screening in an I/DD population. Our 5% positive suicide risk screening rate was similar to that in a recent study of suicidality in youth with I/DD using the same screening tool (Rybczynski et al., 2022).
Limitations include the retrospective nature and change in type of visit from in-person to telehealth; however, this report represents the extent of yearly screening conducted in an urban developmental center. Efforts to follow the TJC guidelines should continue in youth with I/DD.
Footnotes
Disclosures
No competing financial interests exist.