
Abstract

Chief Complaint and Presenting Problem
S. was a 16
History of Present Illness
S. reported ongoing depressive symptoms since eighth grade. Most recently, S. had experienced several weeks of worsening depressive symptoms including anhedonia, worthlessness, hopelessness, lack of motivation, and overwhelming guilt. S. described a history of low self-esteem, which she felt was due to her parents having called her “stupid,” “lazy,” “selfish,” and “ungrateful.”
S. reported ingestion of 40 pills of different medications including quetiapine 50 mg, methylphenidate 5 mg, and bupropion 150 mg. She reported that she did not think anything would happen to her when she ingested the medication, stating that she had overdosed many times in the past. She became worried when she was having difficulty walking. She reported that she was thankful to be alive but was having trouble identifying reasons to live.
S. had a chronic history of self-harm (punching, cutting, biting, and hitting herself) and five prior hospital admissions for suicide attempts through choking, cutting, and overdosing. Multiple past medication trials (see Tables 2 –5) had been unsuccessful. Despite this, S. had been most recently taking quetiapine and bupropion and reported some improvement in mood. She reported her suicidal thoughts had been less frequent, but she still experienced intermittent episodes of intense suicidal ideation. In addition to chronic suicidal ideation, she endorsed anhedonia most days, overwhelming guilt secondary to suicide attempts, and difficulty concentrating.
S. had previously been diagnosed with anorexia nervosa, which had resolved a few years before referral after multiple levels of care (outpatient, intensive outpatient [IOP], partial hospitalization [PHP], and residential). She also reported body dysmorphia symptoms, wanting to “look different,” and change her facial features, and feeling dissatisfied with herself, wishing she could be more social and talented.
Review of systems revealed no past or present symptoms of mania, hypomania, drug abuse, psychosis or previous sexual, physical, or emotional trauma.
Psychiatric History
At 12 years, S. had been diagnosed with MDD in the context of loneliness in school and academic pressure. S. had a history of five psychiatric hospitalizations (see Table 1).
Psychiatric Treatment
IOP, intensive outpatient; PHP, partial hospitalization.
At age 13 years, she was diagnosed with anorexia nervosa, restrictive type, which started as a resolution to lose weight. Her anorexia had resolved after two inpatient psychiatric hospitalizations and residential treatment for eating disorders with a transition to PHP and IOP (see Table 1).
Developmental History
S. was the product of a 33-week pregnancy in a 38-year-old mother complicated by pre-eclampsia. There was no in utero exposure to teratogens. She was delivered by C-section; birth weight was 1.98 kilograms. S. spent 10 days in the NICU and was treated for jaundice.
S. was reported to have had an appropriate level of socialization. S. had no delays in motor, social, or language milestones, and toilet training occurred at an appropriate time.
Educational History
S. was home schooled through a virtual school starting in ninth grade. In 10th and 11th grade, S. attended a magnet school for the performing arts, where she excelled at piano. She maintained high academic performance with above average grades while also attending classes at the local community college. She denied failing grades, suspensions, detentions, or repeating years of school.
Substance Use History
S. admitted to using inhalants in the past at ages 12–13 years. She reported using them every day by spraying deodorant on a rag, which gave her relief when inhaled. She would use it up to five times a day, especially when she was upset at her family or frustrated. She denies any other substance abuse.
Social History
S. was raised in an urban area by both parents, with whom she was currently living at the time of referral. S. reported having 10 close friends, including 2 best friends. She reported a history of two romantic partners and reportedly identified as pansexual. She reported she enjoyed playing and teaching piano.
Family History
Both maternal grandmother and mother had a history of treatment-resistant depression (TRD) in the context of sexual trauma. Mother also had history of bulimia with one psychiatric hospitalization at age 20 years secondary to suicidal thoughts and self-harm. There was also reportedly a history of eating disorders on the father's side of the family.
S.'s older sister had a history of depression, anxiety, psychosis, and attention-deficit/hyperactivity disorder. Both parents had type 2 diabetes. Father also had Parkinson's disease and gastritis.
Medical History
S. underwent myringotomy twice as a child. There was no history of traumatic brain injury, seizures, head injury, or episodes of loss of consciousness. S. had a history of nonclassical congenital adrenal hyperplasia, which was stable, for which she was followed by endocrinology. Though she did not require medication, this did lead to precocious puberty.
S. had previously been diagnosed with anemia and bradycardia, both of which resolved after treatment for anorexia and improvement in nutritional status. At the time of referral, her weight was in the healthy range. Otherwise, growth and development were within normal limits. Menarche occurred at 11 years.
She used corrective lenses for myopia. S. denied any known allergies, and vaccinations were up to date.
Medication History
See Tables 2 –5 for a full history of S.'s treatment and failure of several antidepressants, antipsychotics, one anxiolytic, and several stimulants.
Antidepressant History
Antipsychotic History
Anxiolytic History
Stimulant History
ADHD, attention-deficit/hyperactivity disorder.
S. first failed a trial of fluoxetine and aripiprazole due to heartburn on fluoxetine and subsequent nonadherence. The second selective serotonin reuptake inhibitor trial was escitalopram, which S. also failed for emesis. After pharmacogenomic testing had been conducted to help guide treatment, S. was treated with desvenlafaxine. S. failed this medication due to intolerable somnolence. Duloxetine, in combination with olanzapine, was failed due to lack of efficacy. Olanzapine led to intolerable galactorrhea. Bupropion was slightly effective for depressive symptoms (despite some initial anxiety) in combination with quetiapine. Despite some improvement in mood, S.'s chronic suicidal ideation continued.
Mental Status Examination
On initial mental status examination, S. appeared her stated age and was appropriately dressed, but had poor grooming and hygiene. There were no dysmorphic features. She was calm and superficially cooperative during the interview. She was awake, alert, and oriented to person, location, date, and situation. S. displayed fair eye contact and spoke with spontaneous, clear, comprehensible speech of appropriate volume, rate, and prosody. There was no evidence of psychomotor retardation, psychomotor agitation, or abnormal involuntary movements, and gait was appropriate.
S. described her mood as “fine.” Her affect was generally constricted, and she smiled inappropriately throughout the interview. Thought process was organized, linear, and goal directed. There were no phobias, obsessions, or compulsions. She denied auditory/visual/tactile hallucinations and did not appear to be overtly responding to internal stimuli. She endorsed chronic intermittent suicidal ideation, without plan or intent. She denied homicidal ideation. No delusions were elicited. She exhibited limited insight as well as impaired judgment. Attention and concentration were fair. She spoke fluent English. Memory was not formally assessed but appeared grossly intact. Fund of knowledge appeared appropriate for her level of education.
Formulation
In summary, S. was a 16-year-old adolescent girl with a history of MDD, recurrent, severe; anorexia nervosa, restrictive type; inhalant use disorder; and congenital adrenal hyperplasia referred for emergency psychiatric evaluation after a suicide attempt by overdose of medication.
Predisposing factors included family history of psychiatric illness, preterm birth, low birth weight, and poor coping skills. Precipitating factors included extreme pressure from parents to do well in school, low self-esteem, and belief she was a failure in all aspects of her life. Perpetuating factors included failure of multiple pharmacological interventions and several inpatient psychiatric hospitalizations. Protective factors included adaptive developmental milestones, supportive parents, religious beliefs, academic success, and engagement with outpatient mental health treatment.
Multi-Axial Diagnoses
Current suicidal self-injury History of suicidal behavior Anorexia nervosa, restrictive type, in sustained remission Inhalant use disorder, in sustained remission
History of anemia, now resolved. History of bradycardia, now resolved. Myopia, treated with corrective lenses.
Treatment Course
S. was admitted involuntarily to a child and adolescent psychiatric unit. On admission, S. had stable vital signs, however, was found to be slightly tachycardic. Routine laboratories revealed the following abnormalities: slightly elevated sodium, elevated total protein, slightly elevated magnesium, slightly elevated high-density lipoprotein, and elevated urine protein. Other laboratory tests including CBC, calculated low-density lipoprotein, hemoglobin A1c, thyroid-stimulating hormone, free thyroxine, urinalysis, drugs of abuse screen, and urine pregnancy test were all within normal limits.
S. was continued on quetiapine and bupropion sustained release, but quetiapine was increased to 50 mg BID and bupropion sustained release was increased to 100 mg BID. Throughout admission, these medications were increased to quetiapine 150 mg BID and bupropion extended release 300 mg daily. Throughout the hospitalization, S. was cooperative with treatment. She was initially placed under 24-hour monitoring through a patient attendant for her high risk of self-harm, but after 3–4 days this was discontinued.
She did not require any as needed medications, nor did she require any emergency treatment orders. On discharge, she endorsed improvement in mood symptoms, suicidal thoughts, and appeared to return to her baseline level of functioning. She was discharged with a plan to follow up with individual psychotherapy and medication in the outpatient clinic.
After discharge, S. was evaluated by her outpatient psychiatrist and continued to experience passive suicidal ideation. At this time, ketamine and repetitive transcranial magnetic stimulation (rTMS) therapy were recommended. She also continued individual therapy with close collaboration between providers. Given strong alliance and good support, family therapy was deferred.
S. began rTMS with a Patient Health Questionnaire 9 (PHQ-9) score of 19 at initiation of treatment, which corresponded to a moderately severe level of depression. Mild improvement in depressive symptoms occurred, although S. was still experiencing passive suicidal ideation.
S. was initiated on a depression protocol of 36 consecutive rTMS treatments to the left prefrontal cortex, 3000 pulses at 10 Hz per session, with four second trains and 11 seconds of pause at 120% of her motor threshold. After the first two sessions of rTMS, S.'s PHQ-9 decreased to 11 and continued to decrease from session 3 to session 13 to a score of 6. It remained at 6 for 9 sessions over the course of 2 weeks before increasing to 9.
After four sessions over the course of 1 week, her PHQ-9 decreased to 8 and remained at 8 for the following four sessions over the next week. Although she continued to receive rTMS treatments for an additional seven sessions, it was at this point that a switch to ketamine was recommended for continued passive suicidal ideation despite a low PHQ-9 score.
S. received weekly IV infusions of ketamine, dosed at 1.0 mg/kg, for 6 weeks resulting in six infusions. Her first dose was a 60 mg infusion that was delivered through IV route over the course of 60 min (see Fig. 1). Her second dose 1 week later was also 60 mg IV over 60 min. Over the following 3 weeks, she received IV infusions of 80, 80, and 90 mg, respectively, all over a 60-min period. For her final infusion session, she received 65 mg through the intramuscular (IM) route, and after 15 min, she received another 70 mg dose through the IM route. During the ketamine treatment, she continued to take quetiapine 200 mg BID and bupropion extended release 300 mg daily.

Ketamine dosage and route.
S. was regularly evaluated using the PHQ-9 scale. Figure 2 illustrates the effects of ketamine infusions on S.'s depression as measured by the PHQ-9. Two days after the first infusion, S.'s PHQ-9 decreased to 4 and remained at 4 over the next three rTMS sessions. Of note at this time, S. denied suicidal ideation, thoughts, or plan for the first time in her life. After the second infusion, her PHQ-9 decreased to 2 and over the course of the following four infusions (over 3 weeks), her depressive symptoms continued to improve as evidenced by her PHQ-9 score of 1 (see Fig. 2 below).
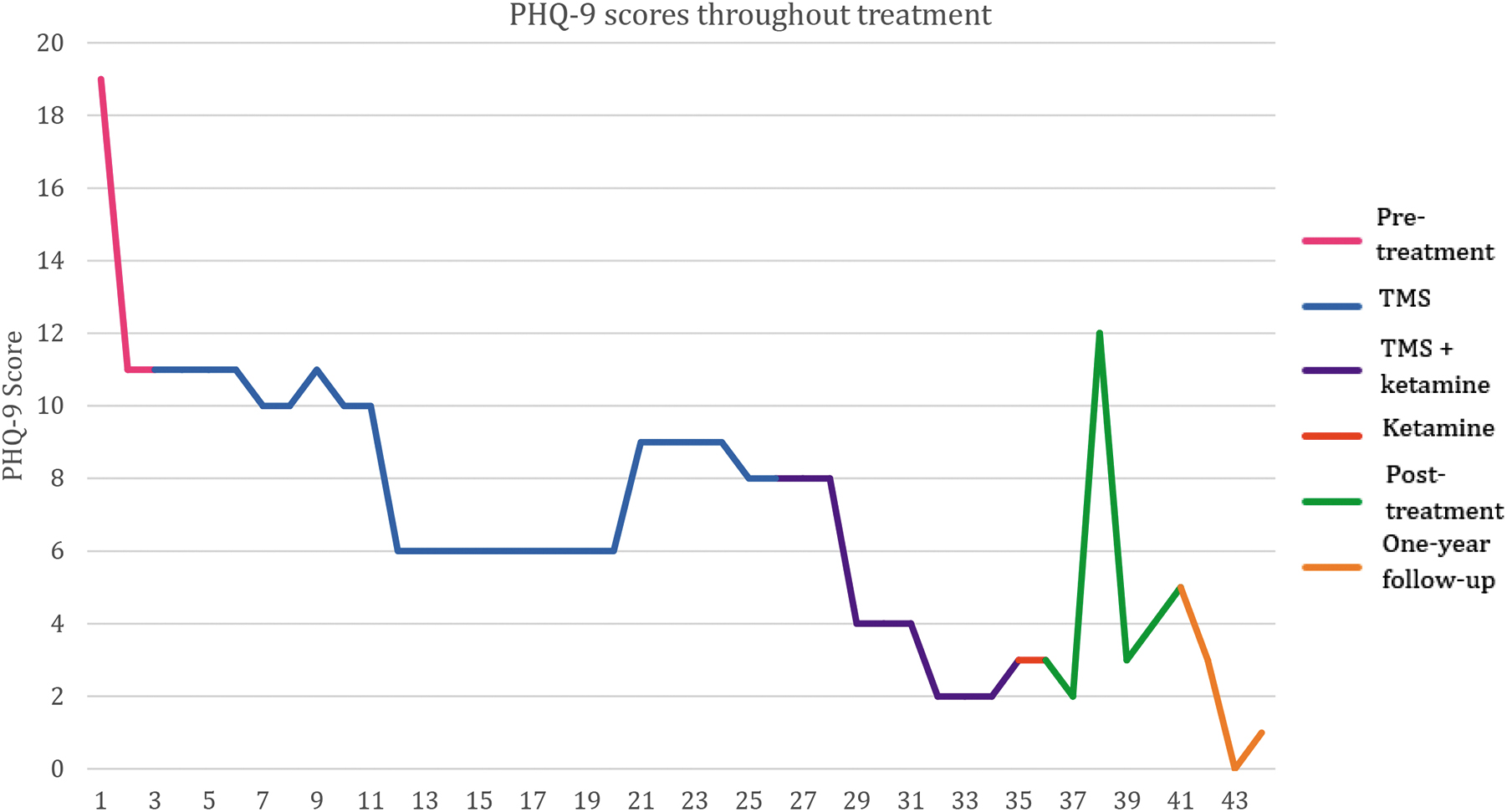
PHQ-9 scores showing improvement of depressive symptoms after TMS and improvement in suicidality after ketamine administration. PHQ-9, Patient Health Questionnaire 9; TMS, transcranial magnetic stimulation.
Three months after the last ketamine infusion, S. showed a temporary increase in depressive symptoms due to challenges in school, which improved once she changed schools. S. did not report any adverse effects of ketamine. Bupropion extended release 300 mg po daily was continued and quetiapine had been increased from 200 mg po BID after her last inpatient admission to 500 mg and increased further to 700 mg qhs; no further ketamine treatments were required. S. experienced decreased mental acuity and blurry vision with quetiapine 700 mg, requiring a decrease in dose.
Approximately a year after her last ketamine infusion, S. had a PHQ-9 score of 1 and she was receiving bupropion extended release 300 mg daily and quetiapine 500 mg qhs at this time.
Discussion
MDD is a severe health condition in youth worldwide, leading to poor psychosocial and academic functioning, physical illness, substance use, and heightened risk of suicidal behavior (Boylan et al., 2020; Dwyer et al., 2020; Walter et al., 2023). In adolescents of age 12–17 years, the lifetime prevalence is 13.3% (Ghandour et al., 2019). Even when appropriate treatment is available, it is estimated that between 20% and 60% of patients do not respond adequately to first-line interventions (Boylan et al., 2020; Brent et al., 2019; Dwyer et al., 2020; Gabriel et al., 2023; Liu et al., 2022; Murrough et al., 2013). According to the STAR D trial, after failing two antidepressants, the chance of responding to a third medication is 16% (Gaynes et al., 2008).
TRD is defined as the failure to achieve remission of symptoms or a substantial reduction of symptoms despite undergoing adequate treatment with multiple appropriate interventions (i.e., failing two or more antidepressants) (Boylan et al., 2020). TRD poses a significant challenge for clinicians as it is difficult for these individuals to achieve sustained remission. As traditional approaches fall short in addressing the complexity of TRD, novel alternative approaches have emerged. Two alternative treatments that have received increasing attention recently are transcranial magnetic stimulation (TMS) and ketamine. In the AACAP Clinical Practice Guideline for the assessment and treatment of children and adolescents with major and persistent depressive disorders, it is stated that research is urgently needed to support treatment in the domain of TMS and new psychopharmacological agents such as ketamine (Walter et al., 2023).
Ketamine, a general anesthetic and analgesic agent with potent noncompetitive N-methyl-D-aspartic acid (NMDA) receptor antagonist action, had its s-enantiomer esketamine approved by the FDA for TRD in adults in 2019 (Food and Drug Administration, 2023; Fedgchin et al., 2019; Liu et al., 2022). The effects of ketamine and esketamine in different formulations—intranasal spray, intravenous infusions, and subcutaneous injections—have been well studied in depression and suicidality in adults in multiple centers around the globe (Anzolin et al., 2023; Chen et al., 2023; Ochs-Ross et al., 2022; Su et al., 2023; Vasiliu et al., 2023).
For children and adolescents, however, the safety and efficacy of ketamine in depression are not well understood (Meshkat et al., 2022). Although studies have shown promising results (Cullen et al., 2019; Dwyer et al., 2017; Dwyer et al., 2021; Kim et al., 2021; Roy et al., 2021; Wolfson et al., 2023), ketamine is still not FDA approved for depression in children and in adolescents. TMS, in contrast, involves a noninvasive, nonpharmacological neuromodulator activity through the application of electromagnetic pulses targeting specific regions of the brain that are thought to be involved in mood regulation. Although TMS is known to be used with good effect in adults, it is not well studied in children and adolescents.
In S., we see a case of a teenage girl with TRD who was successfully treated with ketamine and TMS. S. first started treatment with TMS as an attempt to try more conservative methods. Despite research demonstrating the efficacy of rTMS in remission of depression, S. continued to experience suicidal ideation after 1 month of treatment. Mother agreed to allow S. a trial of IV ketamine. A unique finding was the rapidity and long-lasting effects (more than a year) of remission. Ketamine usually requires maintenance treatments every 2–6 weeks and some respond for only 1 week.
There is also the concern for partial response in ketamine treatments as well as tolerance as more and more ketamine might be needed for response. In this case, TMS helped extend the response. After S. was given TMS and multiple sessions of IV ketamine over the course of 2 months, her depressive symptoms remitted leading to improvement in social and academic functioning, and overall mental health recovery. After the treatment course, S. remained stable, with no reported adverse effects, no hospitalizations, and only minor changes in the dose of her medications. Her PHQ-9 scores improved significantly from 19 to 2 with both TMS and ketamine; the one spike after 3 months was managed with a change in her medications and without the need for more ketamine treatments.
Of note, TMS effects usually last longer than ketamine, from 6 to 12 months, and can help with anxiety symptoms as well (24). Despite the possibility of longer lasting effects, rTMS requires a daily commitment and there can be a delayed time to reduction of depressive symptoms; in this case, there was a delayed time to improvement in suicidal thoughts. Ketamine response is usually faster and helps with suicidal thoughts. In individuals with severe TRD, combining both ketamine and TMS, two treatments with disparate mechanisms of action and time to effect, could potentially increase the chances of achieving a positive result (Leuchter et al., 2017). This may be of particular importance in those individuals who have not responded adequately to ketamine or TMS alone.
Both TMS and ketamine work synergistically and can lead to longer remission of symptoms as shown in this case (Leuchter et al., 2017). Di Lazzaro et al. (2003) suggest that ketamine first might be more beneficial to treatment than TMS first, as ketamine can strengthen TMS effects through neuroplasticity changes in the prefrontal cortex, AMPA transmission, brain-derived neurotrophic factor and interactions with its receptor, tropomycin receptor kinase B, and glutamate NMDA interactions. TMS can improve the effect of ketamine as each works through different mechanisms in the brain (Best et al., 2021; Best et al., 2019).
TMS effects the anterior cingulate gyrus, important in emotional regulation, and lessens some pathological functioning seen in mood disorders, whereas ketamine works on glutamate neurotransmission by acting as an NMDA antagonist and impacts neural connectivity of prefrontal-striatal structures (Best et al., 2019). Best's studies in 2019 and 2021 demonstrate that a group of 28 adult patients with depression or bipolar depression showed improvement (Best et al., 2021; Best et al., 2019). This case report illustrates that adolescents with TRD may also show a favorable and rapid response to ketamine with resolution of symptoms and potentially long-lasting effects.
In S., ketamine was started after 3 years of persistent symptoms, but showed benefit in combination with rTMS, a novel approach. Potential obstacles to initiation of ketamine treatment include lack of FDA approval for youth, expense, and the risk profile, which includes its potential for harmful adverse effects such as transient dissociative episodes. Past studies in youth with TRD have mostly been limited by small sample size and only IV ketamine use.
This case report suggests more research on ketamine in TRD in youth is needed. Identification of which adolescents, what symptoms, and which risk factors predict benefit from ketamine are key challenges. Early initiation of these interventions has the potential to change the trajectory of lives of youth at high risk and reduce disability burden and productivity loss.