
Abstract
Background:
Antipsychotics carry a higher-risk profile than other psychotropic medications and may be prescribed for youth with conditions in which other first-line treatments are more appropriate. This study aimed to evaluate the population-level effect of the Safer Use of Antipsychotics in Youth (SUAY) trial, which aimed to reduce person-days of antipsychotic use among participants.
Methods:
We conducted an interrupted time series analysis using segmented regression to measure changes in prescribing trends of antipsychotic initiation rates pre-SUAY and post-SUAY trial at four U.S. health systems between 2013 and 2020.
Results:
In our overall model, adjusted for age and insurance type, antipsychotic initiation rates decreased by 0.73 (95% confidence interval [CI]: 0.30, 1.16, p = 0.002) prescriptions per 10,000 person-months before the SUAY trial. In the first quarter following the start of the trial, there was an immediate decrease in the rate of antipsychotic initiations of 6.57 (95% CI: 0.99, 12.15) prescriptions per 10,000 person-months. When comparing the posttrial period to the pretrial period, there was an increase of 1.09 (95% CI: 0.32, 1.85) prescriptions per 10,000 person-months, but the increasing rate in the posttrial period alone was not statistically significant (0.36 prescriptions per 10,000 person-months, 95% CI: −0.27, 0.99).
Conclusion:
The declining trend of antipsychotic initiation seen between 2013 and 2018 (pre-SUAY trial) may have naturally reached a level at which prescribing was clinically warranted and appropriate, resulting in a floor effect. The COVID-19 pandemic, which began in the final three quarters of the posttrial period, may also be related to increased antipsychotic medication initiation.
Introduction
In the last few decades, antipsychotics have been increasingly prescribed for youth with conditions where antipsychotics may not be an appropriate first-line treatment, including attention-deficit/hyperactivity disorder, disruptive behavior disorders, Tourette’s syndrome, anxiety, depression, eating disorders, and sleep disorders (Cheng-Shannon et al., 2004; Correll et al., 2021; Crystal et al., 2009; Penfold et al., 2013). One study found that, in 2004, 70.2% of privately insured youth aged 6–17 and 73.2% of Medicaid-insured youth aged 6–17 receiving antipsychotics in seven states did not have a diagnosis of a psychotic disorder, bipolar disorder, autism spectrum disorder, or developmental disability—the diagnoses for which antipsychotics are approved (Christian et al., 2012; Crystal et al., 2009). Other studies report that most antipsychotic medication use in youth is for disruptive behavior, suggesting that antipsychotics may be overused or that access to appropriate first-line treatment is insufficient (Penfold et al., 2013). This is worrisome because antipsychotics carry many side effects, including weight gain, cardiometabolic risk, prolactin elevation, sedation, and extrapyramidal symptoms (e.g., dystonia, tardive dyskinesia) (Bretler et al., 2019; Cheng-Shannon et al., 2004; Correll, 2008; Correll et al., 2009; Galling et al., 2016; Nicol et al., 2018).
Owing to the high-risk profile, increasing trends of antipsychotic prescribing in the United States in the 1990s and 2000s elicited widespread concern and prompted states to implement oversight programs, including prior authorization and database and peer review processes, some of which may be effective in reducing antipsychotic use (Akincigil et al., 2020; Barclay et al., 2017; Finnerty et al., 2011; Hilt et al., 2013; Mackie et al., 2017; Schmid et al., 2015; Zito et al., 2018). Multiple studies have shown that antipsychotic prescribing trends rose in the 1990s and early 2000s, peaked in the late 2000s, and have since started declining slightly (Bushnell et al., 2021; Comer et al., 2010; Crystal et al., 2016; Edelsohn et al., 2017; Kalverdijk et al., 2017; Olfson et al., 2006; Olfson et al., 2012; Olfson et al., 2015; Olfson et al., 2002; Zito et al., 2000). However, more recently, there are limited data on prescribing trends (Chavez et al., 2021) despite initiatives to decrease potentially inappropriate prescribing (Penfold et al., 2020). In addition, previous studies have largely relied on claims data, focused separately on either private or Medicaid-insured youth, and examined overall prescribing trends for all diagnoses—both those that are appropriate for first-line antipsychotic treatment and those that are not. Disaggregation of diagnosis type (e.g., excluding people diagnosed with psychotic disorders) is necessary to accurately estimate the effectiveness of interventions geared at antipsychotic prescribing for conditions where there are potentially safer first-line treatments.
The Safer Use of Antipsychotics in Youth (SUAY) study was a National Institute of Mental Health–funded pragmatic randomized controlled trial with the aim of reducing antipsychotic use in youth and addressing some of the limitations of previous studies (Penfold et al., 2020). SUAY was implemented at a health system level between March 2018 and December 2020 in four U.S. health systems: Kaiser Permanente (KP) Washington, KP Northwest, KP Colorado, and Nationwide Children’s Hospital (NCH) in Columbus, Ohio (Penfold et al., 2020). The SUAY trial used a novel approach that included automated recruitment, medication review and consultation from a study psychiatrist, health care navigation assistance for families, and expedited access to psychosocial care and telemental health (Penfold et al., 2020).
Providers with prescribing privileges were prerandomized to the study following a Zelen design. Provider participation in the study began when they signed a new medication order for an antipsychotic in the medical record for an eligible patient (Penfold et al., 2020). Providers were randomized to either receive the intervention or control best practice alert, and their patients would receive different follow-up options accordingly (Penfold et al., 2020). However, the SUAY study was unable to collect information on providers’ decision-making when they did not order new antipsychotic prescriptions (e.g., the order was canceled after viewing the best practice alert). Thus, it was not possible to observe how providers’ prescribing behavior was influenced by external factors (guidelines and oversight programs), by knowledge of SUAY study activities (Hawthorne effect) (Sedgwick & Greenwood, 2015), or by an exposure to SUAY trial components during prescribing decisions on earlier patients, which could affect the treatment plan of subsequent patients. Although this prescribing behavior could not be captured by the clinical workflow, it may be captured in overall population trends in antipsychotic initiation for all youth “at risk” of an antipsychotic medication prescription.
To identify and adjust for any underlying trend in initiation of antipsychotics at the health system population level (rather than just SUAY participants) and evaluate the effect of introducing the SUAY trial across health systems on changing prescribing practices, we conducted an interrupted time series analysis to measure changes in the level and trend of antipsychotic initiation rates pre-SUAY and post-SUAY beginning. We hypothesized that (1) the SUAY trial accelerated the declining antipsychotic initiation rates and (2) there was significant variation in the change in trend pretrial and posttrial between stratified subgroups.
Methods
Study design
In this retrospective, quasi-experimental, single-group interrupted time series analysis (Bernal et al., 2017; Penfold & Zhang, 2013; Shadish et al., 2002; Wagner et al., 2002), we used segmented regression to evaluate changes in the level and slope of antipsychotic initiation rates for youth aged 3–17 years, who did not have a diagnosis for a psychotic disorder, bipolar disorder, autism spectrum disorder, or developmental disability (SUAY-eligible population), at a health system population level before and after SUAY was implemented. We also conducted stratified analyses by study site, age group (3–12 and 13–17 years), gender (male or female), race (White, non-Hispanic, or Youth of Color), and insurance type (commercial or Medicaid). We selected these subgroups in accordance with a previous study on prescribing trends at NCH (Chavez et al., 2021).
Study setting
We examined population-level rates of antipsychotic initiations at the four U.S. health systems where SUAY was implemented: KP Washington, KP Northwest, KP Colorado, and NCH in Columbus, Ohio (Penfold et al., 2020). At NCH, patients were limited to those who had encounters in either the Psychiatry or the Developmental and Behavioral Pediatrics departments (Penfold et al., 2020). To ensure comparability between the KP sites and NCH, we also limited patients at the KP sites to those who had visits in mental health specialty departments. At three of the sites (KP Washington, KP Colorado, and NCH), SUAY study activities began in spring 2018, with study notification letters, protocol implementation, and provider enrollment spanning March–July 2018. For those three sites, we centered the postimplementation time period on the quarter beginning May 2018, as an average study start date. At KP Northwest, the trial began in May 2019, resulting in four extra pretrial time periods (quarters) and four fewer posttrial time periods (quarters). We excluded these four extra pretrial time periods, where we only had data from KP Northwest, as they skewed the pretrial trend.
Study participants
We used similar inclusion and exclusion criteria to those used in the SUAY study (Penfold et al., 2020). For the crude antipsychotic medication initiation rate numerator, we included incident antipsychotic prescriptions for patients ≥3 and <18 years of age. We excluded prescriptions if the antipsychotic was initiated in an inpatient, urgent care, or emergency department setting; the patient had a recorded International Classification of Diseases, ninth revision, clinical modification (ICD-9-CM) or International Classification of Diseases, 10th revision, clinical modification (ICD-10-CM) diagnosis of a psychotic disorder, mania, autism spectrum disorder, or intellectual disability in the health system electronic health record (EHR); the antipsychotic was prochlorperazine; an antipsychotic was ordered within the prior 180 days for the patient (short-term orders placed by a “doc of the day” did not count toward the 180-day washout period); the patient primary language was not English; or the prescription order status was missing or unknown (less than 5% of orders).
For the antipsychotic initiation rate denominator, we included all patients from the study sites who were ≥3 and <18 years of age at the time of their visit, who had a visit with an eligible provider in a mental health specialty department in the current month and at least one visit in the prior 11 months, and who did not have an ICD-9-CM or ICD-10-CM diagnosis of a psychotic disorder, mania, autism spectrum disorder, or intellectual disability (SUAY-eligible population). As youth could be eligible in multiple months, our design is an open cohort wherein youth continually enter and leave the population. Accordingly, the denominator does not represent the number of individuals treated at each of these sites but rather an aggregate total number of youths each month who could, in principle, have been prescribed antipsychotics. Youth with Medicaid insurance at KP Colorado were excluded from these analyses, as we did not have complete capture of claims information for these youth.
Data collection
We used aggregated administrative and EHR data for eligible patients. Data included patient demographics (age, gender, race, and insurance type) and medications ordered (not prescription fills). Institutional review boards at each site approved a waiver of informed consent to use record data to ascertain medication utilization outcomes. For this data-only analysis, the KP Washington Institutional Review Board approved the use of aggregated, summary data from the four sites.
Data analysis
We used segmented regression to measure changes in the level and slope of antipsychotic initiation rates in the post-SUAY time period compared with the pre-SUAY time period (Bernal et al., 2017; Penfold & Zhang, 2013; Shadish et al., 2002; Wagner et al., 2002). The pretrial trend projected into the posttrial period served as the counterfactual (Linden, 2018). Using the itsa command in Stata, we fit an ordinary least-squares regression model using Newey–West standard errors (Linden, 2018).
We assumed the following model for our interrupted time series:
Rate t is the aggregated outcome variable, the crude rate of antipsychotic initiations per 10,000 person-months in the SUAY-eligible population following a linear model, at each time point (month) t. We calculated rates monthly but report the average monthly rates over each quarter, centered on the study start month (May 2018 or May 2019 depending on study site), because of small numbers of new antipsychotic orders during some months. Aggregating the rates to quarterly observations helped reduce the level of variability at each time point and facilitated trend comparison over time (Wagner et al., 2002). We evaluated this variability and seasonality and corrected for autocorrelation up to the fourth order (four quarters) using the Cumby–Huizinga test for autocorrelation and a type-1 error of 0.05.
Time t is the time (in months, aggregated to quarters) since the start of the baseline data collection period. β0 is the intercept, or starting rate of antipsychotic initiation at time zero. β1 is the slope, or baseline trend, of the rate of antipsychotic initiations before the introduction of the SUAY trial. β2 is the change in the rate of antipsychotic initiation that occurs in the month immediately following the introduction of the SUAY trial compared with the counterfactual. SUAY t is a binary dummy variable indicating when the SUAY trial went into effect (0 for pretrial and 1 for posttrial). β3 is the difference between the slopes of the rate of antipsychotic initiations pretrial and after the introduction of the SUAY trial. Time_after t measures the time since the start of trial. ϵ t is the random variability not explained by the model (Wagner et al., 2002).
In our model, a statistically significant β2 would indicate that the SUAY trial had an immediate statistically significant impact on the rate of antipsychotic initiations (shift in the intercept). We did not a priori expect this result, as providers encountered the trial components at different times, and sudden behavior change in prescribing is extremely uncommon (Brunette et al., 2018; Soumerai & Avorn, 1990; Tani et al., 2013). A statistically significant β3 would indicate that the SUAY trial had an effect over time on the rate of antipsychotic initiations. We hypothesized that β3 would be negative and statistically significant in the overall analysis and all stratified analyses. The model described previously allowed us to control for the baseline rate and trend of antipsychotic initiations before the SUAY trial was implemented (Wagner et al., 2002). This model also assumed the initiation trends were linear.
The single-group interrupted time series model assumes any time-varying unmeasured confounder, such as other policy implementations, can be differentiated from the trial variable (Linden, 2018). We hypothesized that there may have been a competing intervention effect from a previous EHR alert at NCH before the SUAY study, which directed providers to order laboratory assessments along with antipsychotic orders. To test this assumption and to differentiate between the effect of that previous best practice alert, or other time-varying confounders, and the SUAY trial, we tested for interruptions in the trend of the β2 and β3 variables at the median time point of the pretrial period (Linden, 2018).
We adjusted for the precomposition and postcomposition differences in age and insurance type using direct standardization (Tripepi et al., 2010). We used the distribution of age and insurance type in the quarter during which the SUAY trial began.
Results
Baseline characteristics
In our overall SUAY-eligible population, there were 11,233 monthly average eligible youth in the 21 quarters pre-SUAY trial and 12,460 in the 6–10 quarters post-SUAY trial (Table 1). A majority of our SUAY-eligible youth were patients at NCH (69.3% in the preperiod and 73% in the postperiod), were between 3 and 12 years of age (58% in the preperiod and 53.5% in the postperiod), were White, non-Hispanic (64.9% in the preperiod and 65.7% in the postperiod), and had commercial insurance (69.8% in the preperiod and 54.7% in the postperiod) (Table 1). The proportion of females in the SUAY-eligible population shifted from 48.3% in the preperiod to 50.1% in the postperiod (Table 1). Visual inspection of the initiation rates across our pretime and posttime periods revealed a declining rate of initiation beginning in January 2013, which appeared to level out or slightly increase again starting in 2019 (Fig. 1).
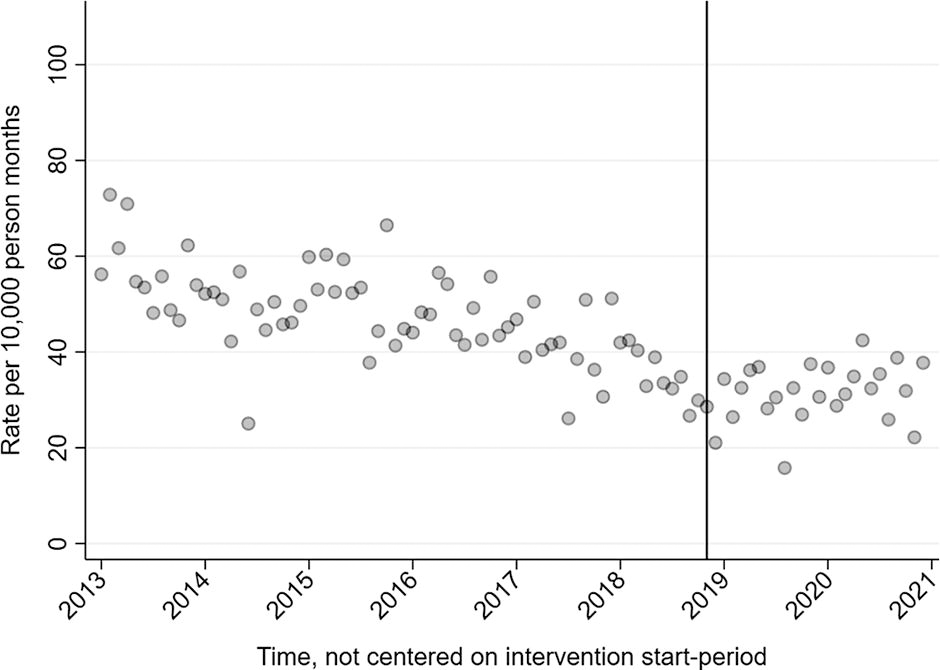
Rate of antipsychotic initiations per 10,000 person-months in the Safer Use of Antipsychotics in Youth (SUAY)-eligible population between 2013 and 2020, not centered on trial start time period. The vertical line depicts the approximate start of the SUAY trial.
Sociodemographic Characteristics of the SUAY-Eligible Population, Pre-SUAY and Post-SUAY Trial
Average monthly eligible youth is not equivalent to the number of individuals treated at each of these sites, as youth could be eligible in multiple months and it was an open cohort with youth entering and leaving the population.
KP Northwest implemented the SUAY trial one year later than the other three sites, resulting in a different denominator for the posttrial time period stratified by site.
KP, Kaiser Permanente; NCH, Nationwide Children’s Hospital; SUAY, Safer Use of Antipsychotics in Youth.
Overall analysis
In our overall model, adjusted for age and insurance type, the rate of antipsychotic initiation in the study population at the beginning of the baseline data collection period (January 2013 or 2014, depending on site) was 52.44 (95% confidence interval [CI]: 46.53, 58.36) prescriptions per 10,000 person-months. This rate decreased before the start of the SUAY trial by 0.73 (95% CI: 0.30, 1.16) prescriptions per 10,000 person-months. In the first quarter after the trial began (β2), there was an immediate decrease in the rate of antipsychotic initiations of 6.57 (95% CI: 0.99, 12.15) prescriptions per 10,000 person-months. In the posttrial period, the rate of antipsychotic initiations increased at a rate of 0.36 (95% CI: −0.27, 0.99) prescriptions per 10,000 person-months, but this trend was not statistically significant. When comparing the posttrial period to the pretrial period (β3), there was an increase of 1.09 (95% CI: 0.32, 1.85) prescriptions per 10,000 person-months (Table 2, Fig. 2).
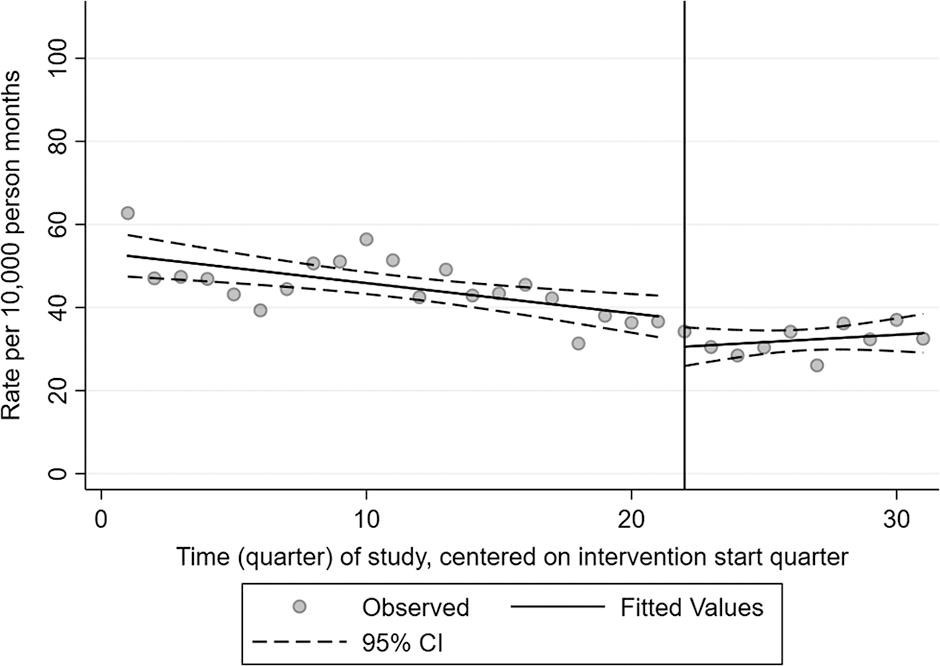
Time series of the rate of antipsychotic initiations per 10,000 person-months in the overall Safer Use of Antipsychotics in Youth (SUAY)-eligible population, adjusted for age and insurance type. Fitted trend lines show predicted values from the segmented regression analysis, with 95% confidence intervals. The vertical line depicts the start of the SUAY trial.
Interrupted Time Series Analysis of the Effect of the SUAY Trial on Antipsychotic Initiation Rates in All SUAY-Eligible Youth, Adjusted for Age and Insurance, 2013–2020
SUAY, Safer Use of Antipsychotics in Youth.
Stratified subgroup analyses
Stratified by site, at KP Northwest, there was an increase in the rate of antipsychotic initiations in the posttrial period relative to the pretrial period (β3) of 3.61 (95% CI: 2.24, 4.99) prescriptions per 10,000 person-months and an increase in the rate of initiations in the posttrial period of 2.19 (95% CI: 1.33, 3.04) prescriptions per 10,000 person-months (Table 2, Fig. 3). At NCH, we did see evidence of a competing intervention effect, possibly from a previous EHR alert before the SUAY study, which directed providers to order laboratory assessments along with antipsychotic orders (Table 2).
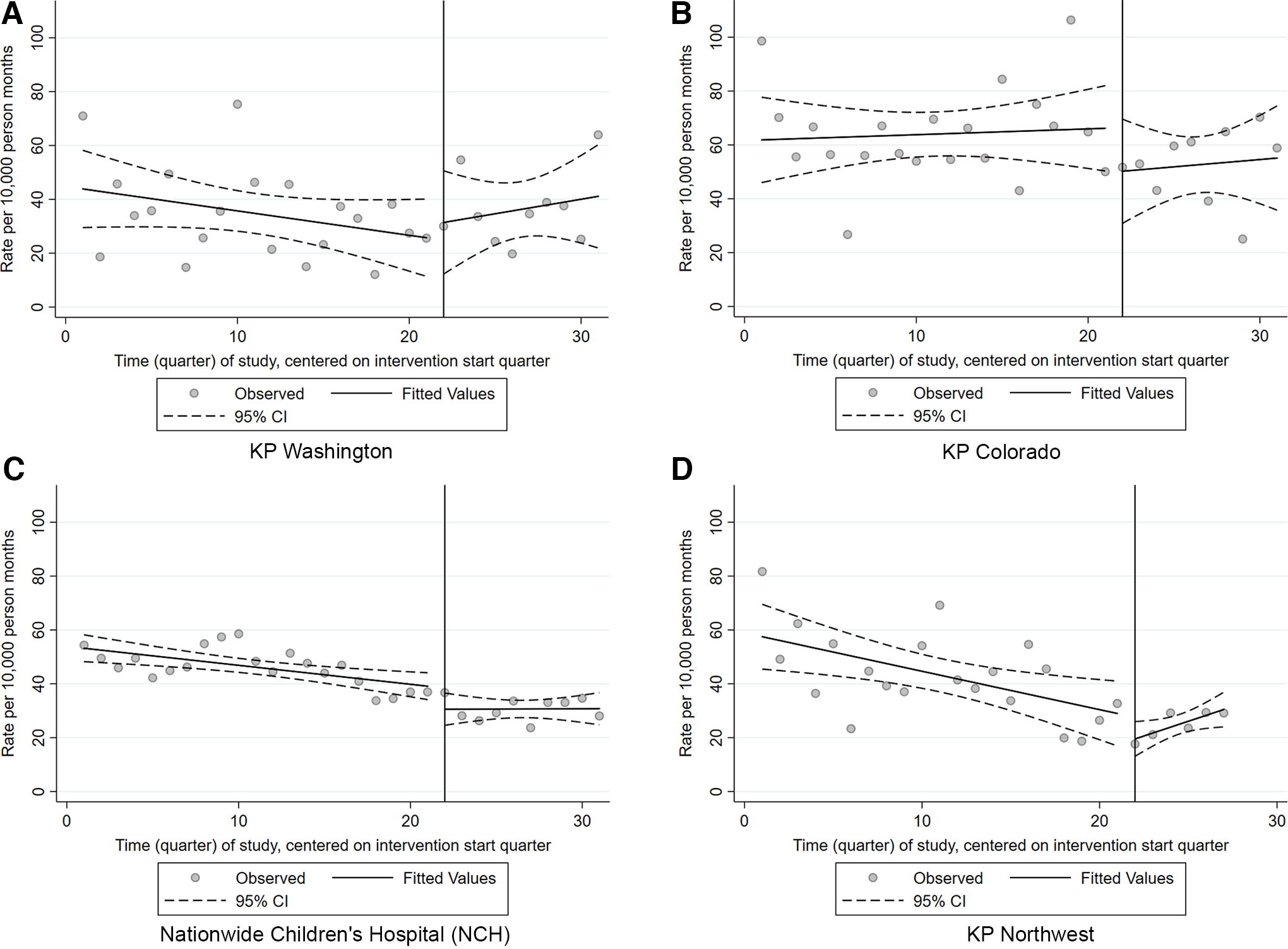
Time series of the rate of antipsychotic initiations per 10,000 person-months in the Safer Use of Antipsychotics in Youth (SUAY)-eligible population by site. Fitted trend lines show predicted values from the segmented regression analysis, with 95% confidence intervals. The vertical line depicts the start of the SUAY trial.
Stratified by age, for those 3–12 years of age, there was an immediate decrease in the rate of antipsychotic initiations in the first quarter after the trial began (β2) of 7.05 (95% CI: 0.60, 13.51) prescriptions per 10,000 person-months (Table 2, Fig. 4). For those 13–17 years of age, there was an increase in the rate of antipsychotic initiations in the posttrial period relative to the pretrial period (β3) of 1.61 (95% CI: 0.44, 2.78) prescriptions per 10,000 person-months (Table 2, Fig. 4).

Time series of the rate of antipsychotic initiations per 10,000 person-months in the Safer Use of Antipsychotics in Youth (SUAY)-eligible population by age and gender. Fitted trend lines show predicted values from the segmented regression analysis, with 95% confidence intervals. The vertical line depicts the start of the SUAY trial.
Stratified by gender, in females, there was an immediate decrease in the rate of antipsychotic initiations in the first quarter after the trial began (β2) of 8.92 (95% CI: 2.22, 15.62) prescriptions per 10,000 person-months and an increase in the rate of antipsychotic initiations in the posttrial period relative to the pretrial period (β3) of 1.34 (95% CI: 0.48, 2.20) prescriptions per 10,000 person-months. In the posttrial period, the rate of antipsychotic initiations for females increased at a rate of 0.96 (95% CI: 0.33, 1.60) prescriptions per 10,000 person-months (Table 2, Fig. 4).
Stratified by race, for White, non-Hispanic youth, there was an immediate decrease in the rate of antipsychotic initiations in the first quarter after the trial began (β2) of 12.82 (95% CI: 5.06, 20.58) prescriptions per 10,000 person-months and an increase in the rate of antipsychotic initiations in the posttrial period relative to the pretrial period (β3) of 1.50 (95% CI: 0.61, 2.38) prescriptions per 10,000 person-months (Table 2, Fig. 5).

Time series of the rate of antipsychotic initiations per 10,000 person-months in the Safer Use of Antipsychotics in Youth (SUAY)-eligible population by race and insurance type. Fitted trend lines show predicted values from the segmented regression analysis, with 95% confidence intervals. The vertical line depicts the start of the SUAY trial.
Stratified by insurance type, for youth with commercial insurance, there was an immediate decrease in the rate of antipsychotic initiations in the first quarter after the trial began (β2) of 15.77 (95% CI: 7.59, 23.94) prescriptions per 10,000 person-months and an increase in the rate of antipsychotic initiations in the posttrial trend relative to the pretrial trend (β3) of 1.81 (95% CI: 0.97, 2.66) prescriptions per 10,000 person-months. In the posttrial period, the rate of antipsychotic initiations for youth with commercial insurance increased at a rate of 0.78 (95% CI: 0.09, 1.47) prescriptions per 10,000 person-months (Table 2, Fig. 5). Please see online Supplementary Appendix Table S1 for the stratified ITS model results.
Discussion
In this retrospective, quasi-experimental, interrupted time series analysis, we found that the SUAY trial may have contributed to a temporary, immediate decrease in the rate of antipsychotic initiations, followed by an increased rate of antipsychotic initiations in the posttrial time period relative to the pretrial time period for SUAY-eligible youth. This finding was also true in some but not all the stratified subgroups. Only in the stratified subgroups of youth at KP Northwest, females, and youth with commercial insurance, there was a statistically significant increase in initiation rates when looking at the posttrial time period alone.
One of the goals of the SUAY trial was to reduce antipsychotic prescribing for youth with diagnoses where other first-line treatments might be more appropriate, such as antidepressants, stimulants, or first-line psychosocial therapy. However, it is possible that the declining trend of antipsychotic initiation seen during the pretrial period had reached a level as of the SUAY trial in 2018, at which prescribing was clinically warranted and appropriate regardless of the trial itself. In the SUAY study, child and adolescent psychiatrists performed second-opinion medication reviews and agreed with around half of the prescriptions (R.B. Penfold, personal communication, May 25, 2022). In addition, the SUAY study found that a higher percentage of youth in the study were engaged in therapy from the beginning than originally anticipated, further indicating that some of the prescribing in the SUAY population may have been appropriate. This health system population-level analysis did not capture clinical context through case reviews or diagnosis codes.
Although we were able to test for competing trends in the pretrial time period by using the median of the pretrial time period as a pseudo start point, there were not enough time periods in the posttrial to do a similar test. It is possible that the leveling out or slight uptick in antipsychotic initiation rates beginning in 2018–2019 is part of a larger trend. Similarly, it is clear that the COVID-19 pandemic had an impact on youth mental health (Becker et al., 2020; Bobo et al., 2020; Hawrilenko et al., 2021; Hertz et al., 2022; Palinkas et al., 2021; Pieh et al., 2021; Roy et al., 2022) and has changed the way patients interact with providers (e.g., telehealth visits) (Curfman et al., 2021), both of which are likely to have impacted antipsychotic initiation rates beginning in 2020. We only had two full quarters of data during the COVID-19 pandemic and were therefore unable to test the pandemic’s impact on prescribing trends. Thus, we cannot rule out that the pandemic increased antipsychotic medication initiation, but we can look at subsequent studies that explore COVID-19 trends. A study investigating antipsychotic prescribing before and during the COVID-19 pandemic at KP Northern California found that overall and off-label prescriptions increased significantly following the onset of COVID-19, driven by increases in prescribing to females and adolescents aged 10–14 (Costales et al., 2024).
This analysis filled gaps in the existing literature by reporting trends in antipsychotic initiation rates from 2013 to 2020, including both commercially and publicly insured patients, focusing only on youth with conditions for which antipsychotics are not an appropriate first-line treatment, and utilizing prescription order data, as opposed to administrative claims data from prescription fills. Prescription order data allowed us to measure and focus on changes in provider prescribing behaviors, as opposed to patient behaviors. Stratified analyses helped us identify any difference in prescribing trends by health system model, age, gender, race, and insurance type.
Limitations
Collecting data on a control population, such as a health system where the SUAY study was not implemented, would have strengthened the study design but was not feasible for this analysis. However, a strength of the interrupted time series model is that it is possible to perform a robust analysis without a control group and sufficiently address threats to internal validity (Linden, 2018; Wagner et al., 2002).
Following the design of the SUAY study, the rate numerator includes ordered prescriptions, as opposed to filled prescriptions, and includes new prescriptions, as opposed to prevalent prescriptions, as it is less likely that a best practice alert would change provider behavior for refill orders or for medication that a patient had already used. There could be subgroup-related differences in preferences for starting new medications and filling prescribed medications that we are unable to measure. However, the choice to use incident prescription order data is a unique strength of this study because it allows us to isolate and measure the effect of the trial on provider prescribing behavior.
Limiting the SUAY-eligible population to those who had visits in mental health specialty department limits generalizability to those with access to psychiatrists. Thus, our study findings may be more generalizable to populations that are engaged and actively receiving behavioral health services. In addition, there may be limited generalizability to smaller health care settings and/or other geographic regions of the United States and elsewhere. Although we adjusted for age and insurance group in our overall model, we could not adjust for these in the stratified subgroup analyses by virtue of using aggregate data.
Finally, we observed high variation in initiation rates, even when aggregated by quarter, which made it difficult to interpret the results.
Conclusion
The “light touch” intervention components of the SUAY trial may not have been sufficient to meaningfully change prescribing trends in large health systems treating pediatric patients at risk for antipsychotic prescribing. The rate of antipsychotic initiations in youth aged 3–17, who did not have a documented diagnosis for a psychotic disorder, bipolar disorder, autism spectrum disorder, or developmental disability, followed a decreasing trend from 2013 to 2018, at which point it leveled off and may have since started increasing. It is unclear if this apparent increase in antipsychotic prescribing is a result of the SUAY trial or part of a larger trend. More analyses with prescribing data from recent years are needed, especially during the COVID-19 pandemic, as the pandemic impacted youth mental health (Becker et al., 2020; Bobo et al., 2020; Hawrilenko et al., 2021; Hertz et al., 2022; Palinkas et al., 2021; Pieh et al., 2021; Roy et al., 2022), patient–provider interactions (e.g., telehealth visits) (Curfman et al., 2021), and antipsychotic prescribing trends (Costales et al., 2024). If prescribing trends continue in a flat or upward trajectory, more stringent interventions, policies, and laws should be considered.
Clinical Significance
It is well known that changing prescribing behavior is difficult. The components of SUAY were designed to support clinicians in considering alternative therapies and making lower risk alternatives easy to access (e.g., psychotherapy). Commonly cited reasons for prescribing antipsychotic medications to youth (such as lack of access to psychotherapy), do not appear to be the main drivers of prescribing.
Footnotes
Acknowledgment
The authors thank Swan Bee Liu, Vina Graham, Artie Runkle, Leeann Quintana, Karen Glenn, and Phillip Crawford for their work in preparing and extracting the data.
Authors’ Contributions
L.M.W.: analyses and drafting manuscript; S.J.M.: design and interpretation of findings; L.C.: design and interpretation of findings; A.B.: design and interpretation of findings; G.N.C.: design and interpretation of findings; C.J.P.: programming and drafting manuscript; A.D.R.: project management and drafting manuscript; R.B.P.: design, funding, analyses, drafting manuscript.
Author Disclosure Statement
The authors have no conflicts to disclose.
Supplementary Material
Supplementary Appendix Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.