
Abstract
Objectives:
There are currently no long-acting injectable antipsychotics (LAIAs) that are approved by the Food and Drug Administration for use in child and adolescent patients, however these agents are used off-label for the treatment of various psychiatric disorders. This study aims to describe the initiation and maintenance dosing strategies of LAIAs in child and adolescent psychiatry inpatients.
Methods:
This was a single-site retrospective chart review of patients less than 18 years of age initiated on an LAIA during an acute psychiatric hospitalization between October 1, 2015, and October 31, 2022. Patient demographics and hospital encounter information were collected and analyzed using descriptive statistics.
Results:
Of the 6402 unique pediatric patients discharged from the acute psychiatric hospital within the specified timeframe, 45 (0.7%) were newly initiated on an LAIA. The average age was 15.6 years (range 10–17), with a greater proportion of male (n = 26, 57.8%) and Black or African American (n = 27, 60%) patients. The LAIA agents prescribed included paliperidone palmitate (n = 21, 46.7%), aripiprazole monohydrate (n = 15, 33.3%), aripiprazole lauroxil (n = 7, 15.6%), haloperidol decanoate (n = 1, 2.2%), and risperidone microspheres (n = 1, 2.2%). Primary diagnosis via International Classification of Diseases-10 code at discharge included schizophrenia spectrum and other psychotic disorders (n = 19, 42.2%); bipolar disorder (n = 14, 31.1%); disruptive, impulse control, and conduct disorders (n = 6, 13.3%); autistic disorder (n = 5, 11.1%); and attention-deficit/hyperactivity disorder (n = 1, 2.2%). Seventeen patients (37.8%) received a loading dose regimen and/or a maintenance dose regimen that differed from adult package-insert dosing. The mean length of stay was 23.7 days, and 14 patients (31.1%) were readmitted to the psychiatric hospital within 6 months of discharge. The mean number of days to readmission was 71.9 days.
Conclusions:
This retrospective study is the first to focus on LAIA initiation and maintenance dosing strategies of multiple agents in both a child and adolescent patient population. Further research is required to evaluate the impact of LAIAs on clinical outcomes in this patient population.
Introduction
Oral antipsychotics are a mainstay of treatment for patients with psychiatric disorders such as schizophrenia, and several oral antipsychotics are approved by the Food and Drug Administration (FDA) for use in child and adolescent patients (McClellan et al., 2013). Prescribing trends of oral antipsychotics in child and adolescent patients have fluctuated; while some studies have shown a decrease in prescribing, other studies have shown an increase in prescribing trends of oral antipsychotics in this patient population (Bushnell et al., 2021; Chavez et al., 2021; Harrison et al., 2012; Klau et al., 2023; Patel et al., 2005; Radojcic et al., 2023; Shuang et al., 2021). Long-acting injectable antipsychotics (LAIAs) are widely known to be an effective treatment option for adult patients with schizophrenia, schizoaffective disorder, and bipolar 1 disorder. LAIA use in this patient population has been associated with improved outcomes such lower relapse rates, longer time to relapse, and fewer hospital days when compared to adult patients treated with oral antipsychotics (Huang et al., 2021; Lytle et al., 2017; Park et al, 2018; Thaman et al., 2024). Despite these findings, the use of LAIAs in child and adolescent patients remains unclear, as showcased by lack of concrete guidance from various guidelines and continued off-label usage of these agents in this patient population.
The American Psychiatric Association’s Clinical Manual of Child and Adolescent Psychopharmacology acknowledges the theoretical benefit of LAIA use in child and adolescent patients who are nonadherent to oral medications but does not offer explicit guidance for use (McVoy and Findling, 2017). In contrast, the American Academy of Child and Adolescent Psychiatry cautiously recommends LAIAs as a treatment option in adolescent patients with schizophrenia who have both chronic psychotic symptoms and nonadherence to oral medications (McClellan et al., 2013). There are currently no LAIAs FDA-approved for use in patients less than 18 years of age; however, there have been case reports and studies documenting off-label use in this patient population that suggest clinical benefit (Ceylan et al., 2017; Fortea et al., 2018; Jacob et al., 2021; Lytle et al., 2017; Modesitt et al., 2018; Moon et al., 2023; Pope and Zaraa, 2016).
Previous studies have either reported on LAIA use in adolescent patients or provided dosing strategies for one singular LAIA agent (Ceylan et al., 2017; Moon et al., 2023; Pope and Zaraa, 2016). Our present study aims to provide a more comprehensive overview of LAIA initiation and maintenance dosing strategies in both child and adolescent patients with psychiatric disorders. Specifically, we report on the use of five different LAIA agents, primary diagnosis at discharge, and initiation and maintenance dosing regimens. In addition, we report on average length of stay, 6-month rehospitalization rates, reported adverse effects, and treatment retention for LAIA therapy.
Methods
This was a single-center retrospective chart review of patients less than 18 years of age who were initiated on an LAIA on one of two child or three adolescent units within an acute psychiatric hospital between October 1, 2015, and October 31, 2022. These dates were selected to align with the implementation of International Classification Diseases (ICD)-10 codes, as primary diagnoses were extracted from the electronic health record via ICD-10 codes (Hirsch et al., 2016). Given the retrospective nature, this study was designated as a quality improvement study that was approved by the institution’s Quality Review Committee. Patients were included if they were newly initiated on an LAIA during the hospitalization (see Fig. 1).
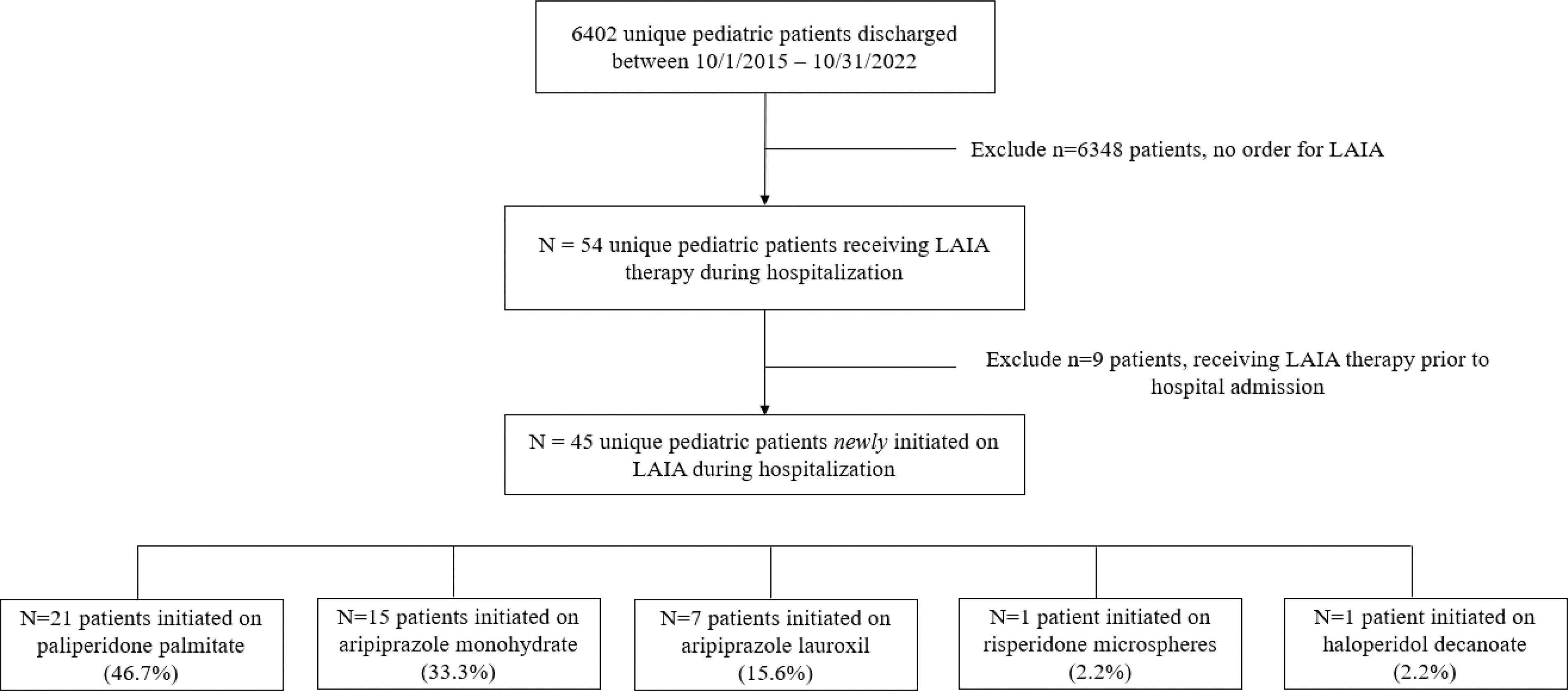
Patients included in study. LAIA, long-acting injectable antipsychotic.
For patients with multiple admissions during the specified timeframe, only the initial hospitalization when LAIA therapy was initiated was included in the study. LAIAs administered included aripiprazole lauroxil (Aristada®), aripiprazole monohydrate (Abilify Maintena®), paliperidone palmitate (Invega Sustenna®), risperidone microspheres (Risperdal Consta®), and haloperidol decanoate (Haldol Decanoate). As part of the pharmacist-led LAIA consult process, insurance coverage was verified and all prior authorizations were completed prior to LAIA initiation.
Patient demographics including age at admission, date of birth, gender, sex, and race were collected from the electronic health record and are shown in Table 1. Clinical and hospital encounter information including admission date, discharge date, primary discharge diagnosis, LAIA loading dose regimen, dose and duration of oral antipsychotic overlap, and concomitant psychotropic medications were additionally extracted from the electronic health record. Outcomes data including hospital length of stay, treatment retention (up to 6-months post-discharge), 6-month readmission rates, and adverse effects to LAIA therapy were collected and evaluated via descriptive statistics.
Baseline Demographics
Baseline demographic information.
Additional scheduled antipsychotic that differs from primary long-acting injectable antipsychotic compound.
Selective serotonin reuptake inhibitors and serotonin norepinephrine reuptake inhibitors included.
Divalproex, lithium, lamotrigine, carbamazepine, and oxcarbazepine included.
ICD, International Classification of Diseases.
Results
Patient demographics
Between the dates of October 1, 2015, and October 31, 2022, there were 6402 unique pediatric patients discharged from the acute psychiatric hospital, 54 of whom were ordered an LAIA. Of these 54 patients, 45 were newly initiated on the LAIA and were ultimately included in the study. For newly initiated patients, the mean age was 15.6 years ± 1.67 years, with the youngest patient being 10 years of age. Sex and race were reported by the patient and clinician documented in the electronic health record. There were more male (n = 26, 57.8%) than female (n = 19, 42.2%) patients and a greater proportion of Black or African American patients (n = 27, 60%) than White patients (n = 17, 37.8%). The primary diagnosis at discharge was captured via ICD-10 codes and categorized into one of five categories: schizophrenia spectrum and other psychotic disorders (n = 19, 42.2%); bipolar disorders (n = 14, 31.1%); disruptive, impulse control, and conduct disorders (n = 6, 13.3%); autistic disorder (n = 5, 11.1%); and attention-deficit/hyperactivity disorder (n = 1, 2.2%). Paliperidone palmitate was the most commonly prescribed LAIA (n = 21), accounting for 46.7% of all LAIAs, followed by aripiprazole monohydrate (n = 15, 33.3%), aripiprazole lauroxil (n = 7, 15.6%), haloperidol decanoate (n = 1, 2.2%), and risperidone microspheres (n = 1, 2.2%).
Over a quarter of the patients had at least one concomitant psychotropic medication prescribed at discharge from the hospitalization in which the LAIA was initiated. Antidepressants were the most commonly coprescribed psychotropic medication with 12 patients (26.7%) receiving a selective serotonin reuptake inhibitor or serotonin norepinephrine reuptake inhibitor. Other concurrent psychotropics included stimulants (n = 8, 17.8%), alpha-2 agonists (n = 8, 17.8%), mood stabilizers (n = 4, 8.9%), and an additional scheduled antipsychotic that differed from the LAIA agent (n = 1, 2.2%).
Dosing regimens
Of the 45 patients included in the study, 33 patients (73.3%) received a loading dose or oral overlap regimen consistent with adult dosing and 12 patients (26.7%) received a loading dose or oral overlap regimen that deviated from recommended adult dosing (Fig. 2). Similarly, 37 patients (82.2%) were prescribed maintenance LAIA doses that were consistent with adult dosing recommendations, whereas 8 patients (17.8%) were prescribed a maintenance dose that deviated from recommended adult dosing (Fig. 3). Three patients received both a nonstandard loading dose or oral overlap regimen and a nonstandard maintenance dose, resulting in a total of 17 patients (37.8%) receiving nonstandard doses in some capacity and 28 patients (62.2%) receiving adult standard dosing. The nonstandardized dosing regimens are summarized in Table 2. The majority of patients receiving nonstandard loading doses or oral overlap regimens were due to either varying lengths of oral overlap for aripiprazole monohydrate, or reduced loading doses for paliperidone palmitate, specifically receiving 156 mg intramuscularly (IM) as a first loading dose followed by 117 mg IM as a second loading injection.
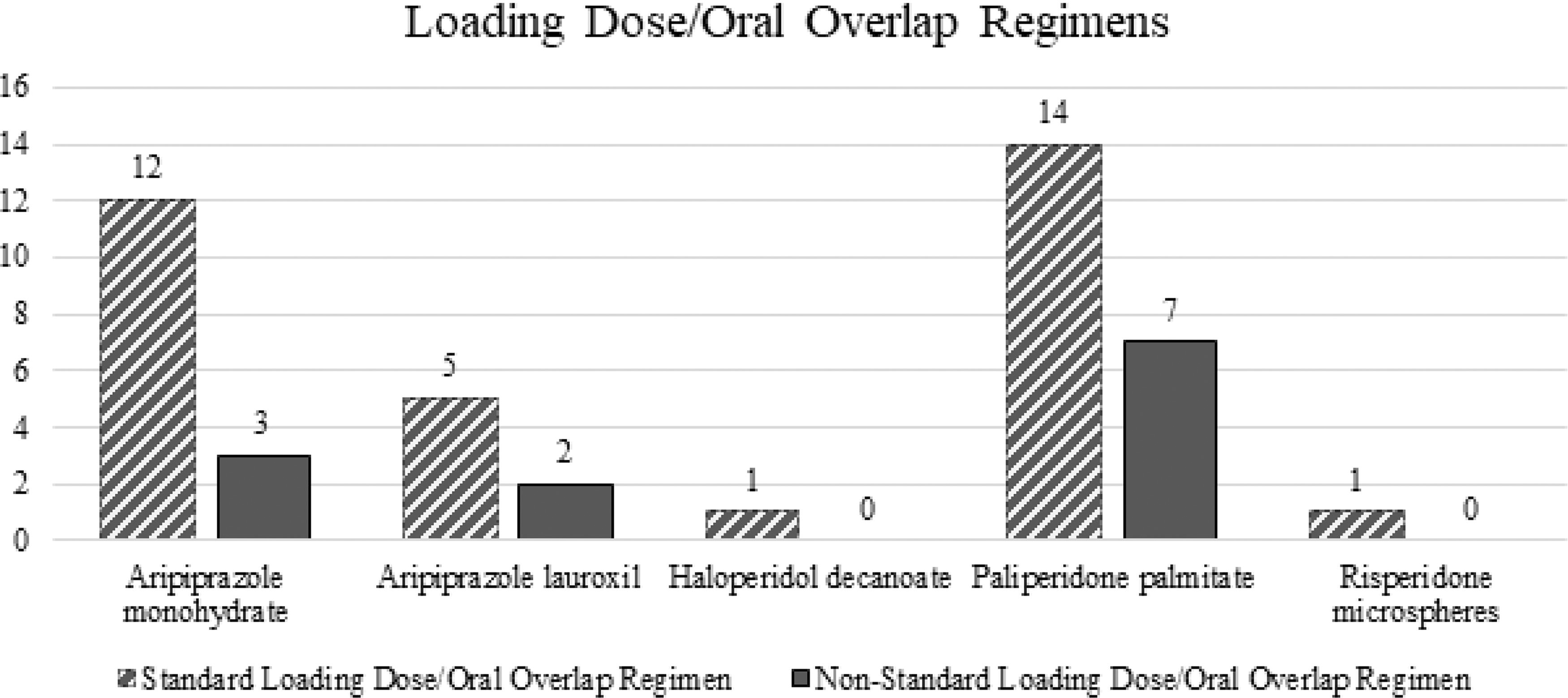
Loading dose and oral overlap regimens.
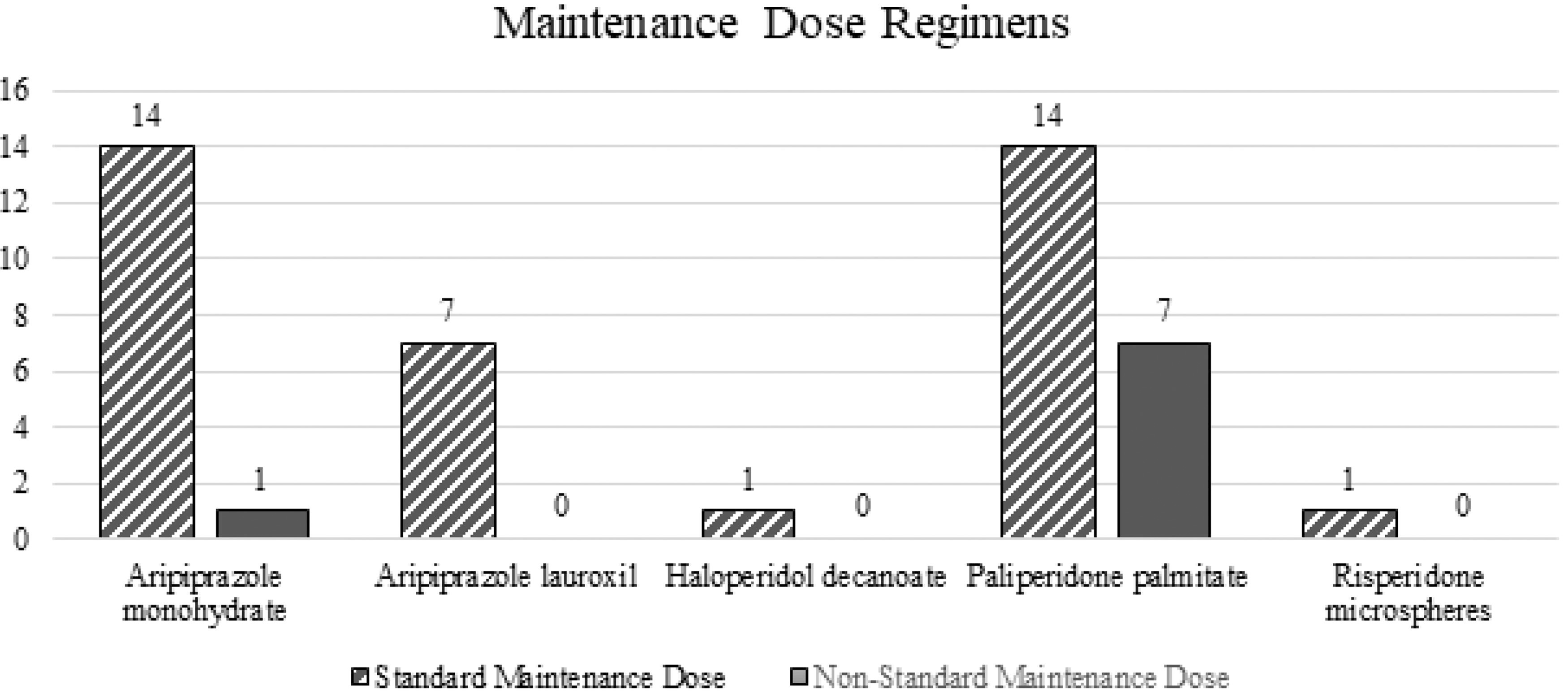
Maintenance dose regimens.
Non-Standard LAIA Dosing Regimens
Description of dosing regimens that deviated from adult package-insert recommended dosing.
LAIA, long-acting injectable antipsychotic; IM, intramuscular; M, male; F, female.
Length of stay and readmission rates
As shown in Table 3, the average hospital length of stay for all patients was 23.7 days (standard deviation 19.4). Across all 45 patients, 14 (31.1%) were readmitted to the same psychiatric facility within 6 months after discharge. The mean number of days to readmission was 71.9 days (standard deviation 45.7).
Length of Stay and Readmission Rates
Length of stay and readmission rates for patients receiving long-acting injectable antipsychotic therapy.
LOS, length of stay; SD, standard deviation.
Adverse effects
Chart review was performed to search for any documentation of adverse effects to the LAIA. An adverse effect was included if it was documented in the electronic health record as occurring after LAIA initiation or if it was documented in subsequent outpatient behavioral health notes (if available). As shown in Table 4, a total of 13 patients (28.9%) had an adverse effect that was documented in an electronic health record note. Five patients receiving aripiprazole monohydrate reported adverse effects including akathisia, tremor, drooling, headache, and injection site soreness. Five patients receiving paliperidone palmitate reported adverse effects consisting of weight gain, metabolic effects, constipation, difficulty thinking/concentrating, and extrapyramidal symptoms. One patient included in this study was initiated on haloperidol decanoate; this patient reported akathisia and had laboratory-confirmed neutropenia.
Clinician Documented Patient Reported Adverse Effects
Clinician-documented patient-reported adverse effects to long-acting injectable antipsychotic therapy.
LAIA, long-acting injectable antipsychotic.
Treatment retention
Of the 45 patients included in this study, 26 (57.8%) received psychiatric care post-hospitalization at an outpatient clinic associated with the inpatient psychiatric hospital, thus allowing for outpatient records to be reviewed. Chart review was performed to assess LAIA adherence for up to 6-months post-discharge. Only 10 of the 26 patients (38.5%) remained adherent to the LAIA at 6 months post-discharge. Please refer to Fig. 4 for further breakdown of 1-month and 3-month retention rates. The reason for discontinuation varied widely among patients and is shown in Table 5.

LAIA treatment retention rates. Retention rates for LAIA therapy captured for patients receiving psychiatric care at an associated outpatient clinic. LAIA, long-acting injectable antipsychotic.
Reason for Long-Acting Injectable Antipsychotic Discontinuation
Reported reason for long-acting injectable antipsychotic discontinuation.
Discussion
This study outlined 45 child and adolescent patients receiving LAIA therapy for a wide variety of diagnoses. The greatest proportion of patients had a primary ICD-10 discharge diagnosis of schizophrenia spectrum and other psychotic disorders (42.2%), followed by bipolar disorders (31.1%); disruptive, impulse control, and conduct disorders (13.3%); autistic disorder (11.1%); and attention-deficit/hyperactivity disorder (2.2%). This range of diagnoses is broader than what LAIAs are utilized to treat in the adult population, aligning with the broadened indication of oral antipsychotics in child and adolescent patients (Citrome, 2021; Rettew et al., 2015).
There were a few patients included in this study that warrant additional discussion. First, one individual initiated on paliperidone palmitate had a primary diagnosis of attention-deficit/hyperactivity disorder. This patient had a concurrent ICD-10 diagnosis of autistic disorder and was receiving oral risperidone therapy for this indication prior to admission. Due to concerns for nonadherence, the patient was initiated on paliperidone palmitate. Next, the patient initiated on haloperidol decanoate was readmitted 2 days after discharge, as noted in Table 3. This patient had a history of hospitalizations due to worsening psychotic symptoms, likely induced by medication noncompliance and cannabis use. The patient's subsequent dose of haloperidol decanoate was increased from a maintenance dose of 100 mg IM every 4 weeks to 130 mg IM every 4 weeks. Lastly, one patient had an additional antipsychotic compound prescribed at the time of discharge. This patient had a primary ICD-10 diagnosis of autistic disorder and was admitted to the hospital on oral aripiprazole. During the hospitalization, the patient was restarted on oral risperidone and transitioned to paliperidone palmitate LAIA. Due to a history of concern for hyperprolactinemia with oral risperidone, the patient remained on oral aripiprazole and was ultimately discharged from the hospital on aripiprazole 5 mg daily in addition to monthly paliperidone palmitate, with prolactin levels within normal limits. Risperidone has been documented to induce hyperprolactinemia in child and adolescent patients; however, the role of adjunctive aripiprazole therapy in the treatment of this risperidone-induced hyperprolactinemia is not as well established (Kroigaard et al., 2022; Saito et al., 2004; Raghuthaman et al., 2015).
Notable limitations of this study include the retrospective nature of the chart review used to capture the incidence of adverse effects and the rationale for LAIA discontinuation. Previous antipsychotic trials were not expanded upon in this study. In addition, the sample size was small, although larger than other studies documenting LAIA use in child and adolescent patients. Heterogeneity of the diagnoses may not reflect safety and efficacy for child and adolescent patients using LAIAs for other diagnoses. Subsequent admissions to other hospitals within or outside of the health system were not included in the readmission data. Finally, readmission rates and treatment retention were only evaluated up to 6 months post-discharge. Future studies should focus on longer-term safety and efficacy outcomes as well as treatment outcomes compared with similar child and adolescent patients prescribed oral antipsychotic therapy.
Conclusions
This retrospective chart review describes the initiation and maintenance dosing regimens, primary diagnosis, 6-month rehospitalization rates, length of stay, reported adverse effects, and LAIA treatment retention of 45 child and adolescent patients with psychiatric disorders initiated on LAIA therapy. The results of this study indicate that LAIAs may be a potentially safe and efficacious treatment option for child and adolescent patients with a wide variety of psychiatric disorders; however, further studies are warranted.
Clinical Significance
This study is the first to describe initiation and maintenance dosing regimens of multiple LAIA agents in patients less than 18 years of age. More than half of the included patients received dosing consistent with adult package-insert dosing, suggesting that adult dosing may be generalizable to patients under 18 years of age. However, a smaller proportion of patients were documented to have dosing regimens that deviated from adult recommended doses. Factors that contributed to these dosing variations include previous antipsychotic exposure and tolerability and provider preference.
All patients were verified to have active insurance coverage with all prior authorization forms submitted and approved prior to LAIA initiation. Although insurance prior authorizations were successfully obtained for the 45 patients included in this study, there have been circumstances where patients have been denied insurance coverage due to nonstandard dosing regimens or off-label utilization. By publishing this paper, we aim to contribute to and facilitate discussion regarding LAIA dosing and use in child and adolescent patients. Further studies specifically targeting long-term safety and efficacy, as well as comparing outcomes between child and adolescent patients on oral antipsychotic therapy and LAIAs, are warranted to fully understand the impact of LAIA therapy in this special patient population.
Footnotes
Disclosures
No competing financial interests exist, and none of the authors have any conflicts of interest to disclose.