
Abstract
Introduction:
Professional guidelines recommend that providers routinely monitor children prescribed second-generation antipsychotics (SGA) to reduce the risk of adverse metabolic events associated with the medication. Despite this guidance, many studies show low rates of monitoring compliance. In this study, we interviewed child psychiatrists for their views of possible barriers to monitoring.
Methods:
Semi-structured qualitative interviews, developed according to the Regehr model of influences upon patient–provider decision making, were conducted with child and adolescent psychiatrists in current practice and recruited by convenience and snowball sampling. Interviews were conducted through internet video meetings and were recorded. Interview data were analyzed following Framework Analysis qualitative methods.
Results:
We recruited and completed interviews with 17 psychiatrists. Patient-level barriers included travel difficulties, limited family time for health care appointments, patient fear of blood draws, and more. Provider-level barriers included professional judgment versus guideline guidance, perceived family burden, assumption of low-risk, short-term SGA use, and more. Organizational level barriers included lack of organizational mandates or incentives, limited appointment time per patient, lack of care coordination, lack of co-located labs, personnel turnover, and more. Barriers at the social and cultural level include stigma and low health literacy.
Conclusion:
These practicing prescribers provided a wide range of possible barriers to metabolic monitoring in children and adolescents prescribed SGAs. The next step is to explore which may be present in certain settings, and to pilot quality improvement interventions. Addressing barriers can reduce risk of metabolic disorders arising from long-term use of SGAs in children and adolescents.
Introduction
Metabolic adverse effects such as weight gain, obesity, hyperglycemia, dyslipidemia, hypertension, type 2 diabetes, and hyperprolactinemia associated with Second-Generation Antipsychotics (SGAs) (Correll, 2008; Rodday et al., 2015) affect up to 60% (Libowitz and Nurmi, 2021) children and adolescents. Accumulation of these adverse effects early in life can result in long-term complications of cardiovascular mortality, morbidity, and other metabolic syndromes (Correll et al., 2009; Libowitz and Nurmi, 2021). In 2011, the American Academy of Child and Adolescent Psychiatry (AACAP, 2011) released practice parameters for the safe and effective use of atypical antipsychotic medications for children and adolescents modeled after the seminal American Diabetic Association, American Psychiatric Association, and American Association of Clinical Endocrinologists (ADA, APA, AACE, and NAASO, 2004) guidelines, which recommended baseline and periodic metabolic monitoring for those prescribed SGAs.
The metabolic monitoring uptake in children and adolescents on SGAs has remained suboptimal even a decade after the release of AACAP guidelines. A study among children prescribed atypical antipsychotics reported that, among 164 Medicaid health plans across many states in 2016, only 33% had documented metabolic monitoring (Olin et al., 2019). In a recent study (Sanyal et al., 2023a), it was shown that the publication of AACAP guidelines led to an immediate increase of 12.61% in BMI monitoring rate; however, there was no clinically significant sustained improvement for BMI, blood glucose, or cholesterol monitoring. In addition, a follow-up study also revealed that full and partial adherence to guideline-recommended monitoring of children and adolescents prescribed SGAs were poor with 1%−6.5% of full adherence to different metabolic parameters (Sanyal et al., 2023b).
To understand the barriers to SGA metabolic monitoring in children, Rodday et al. (2015) found that being board-certified and able to measure vital signs on site was associated with higher levels of monitoring, while perceptions of patients being nonadherent with blood work were associated with lower glucose and lipid monitoring. A qualitative interview (Aouira et al., 2022) conducted among 10 Australian child psychiatrists found that lack of adequate resources to conduct monitoring, career disengagement in treating youth, and patient refusal to blood tests are also barriers to metabolic monitoring. These studies suggest that provider perceptions of patient willingness and organizational constraints may be barriers to monitoring. However, the discovery of barriers was not queried in the questionnaire of Rodday et al.’s study, and in Aouira et al.’s study, Australian health care system and culture may not apply for the U.S. experience.
Although, the discovery of barriers were not directly queried, the semi-structured interview along with exploratory probes was guided by a multi-level conceptual model to understand the psychiatrists' perception of possible barriers to metabolic monitoring.
Methods
Study design
To discover the range of reasons of the low monitoring compliance in the United States, we conducted semi-structured qualitative interviews with practicing psychiatrists who regularly provide care for children and adolescents and asked them why adherence to guidelines might be low. The interview asked why adherence might be low among some providers, generally, but did not ask interviewees about why they, themselves, might have low adherence to guidelines, as this seemed too accusatory and assumptive, and so would not elicit realistic, likely answers. Interviewer responses were analyzed by Framework Analysis, a qualitative research methodology developed for policy-relevant health care topics.
Semi-structured interview
To sufficiently probe a full range of possible reasons, interview development was guided by the Regehr Model of clinical decision making (Regehr et al., 2007). This model declares that clinical decision making is a complex process open to influences at each of three levels: the patient–provider level, the organizational level, and the societal/cultural level. This model emerged in response to the limits of evidence-based practice. In the first of three levels, the provider has three influences: the evidence basis, as part of the intent to practice evidence-based medicine; his or her own knowledge and judgment regarding specifics of the individual clinical situation; and preferences of the patient and family. Thus, clinician decision making can not only be evidence based but also patient centered and based on autonomous professional judgment.
Surrounding this first level is the organizational level of influences, including “organizational mandates,” “training/supervision,” and “organizational resources and constraints,” and local “community.” At the third, social and contextual level, are another four categories of influence: “professional context,” “economic context,” “political context,” and “socio-historical context.” Figure 1 provides an illustration of this model; an article by Satterfield et al. (2009) presents this model more completely.
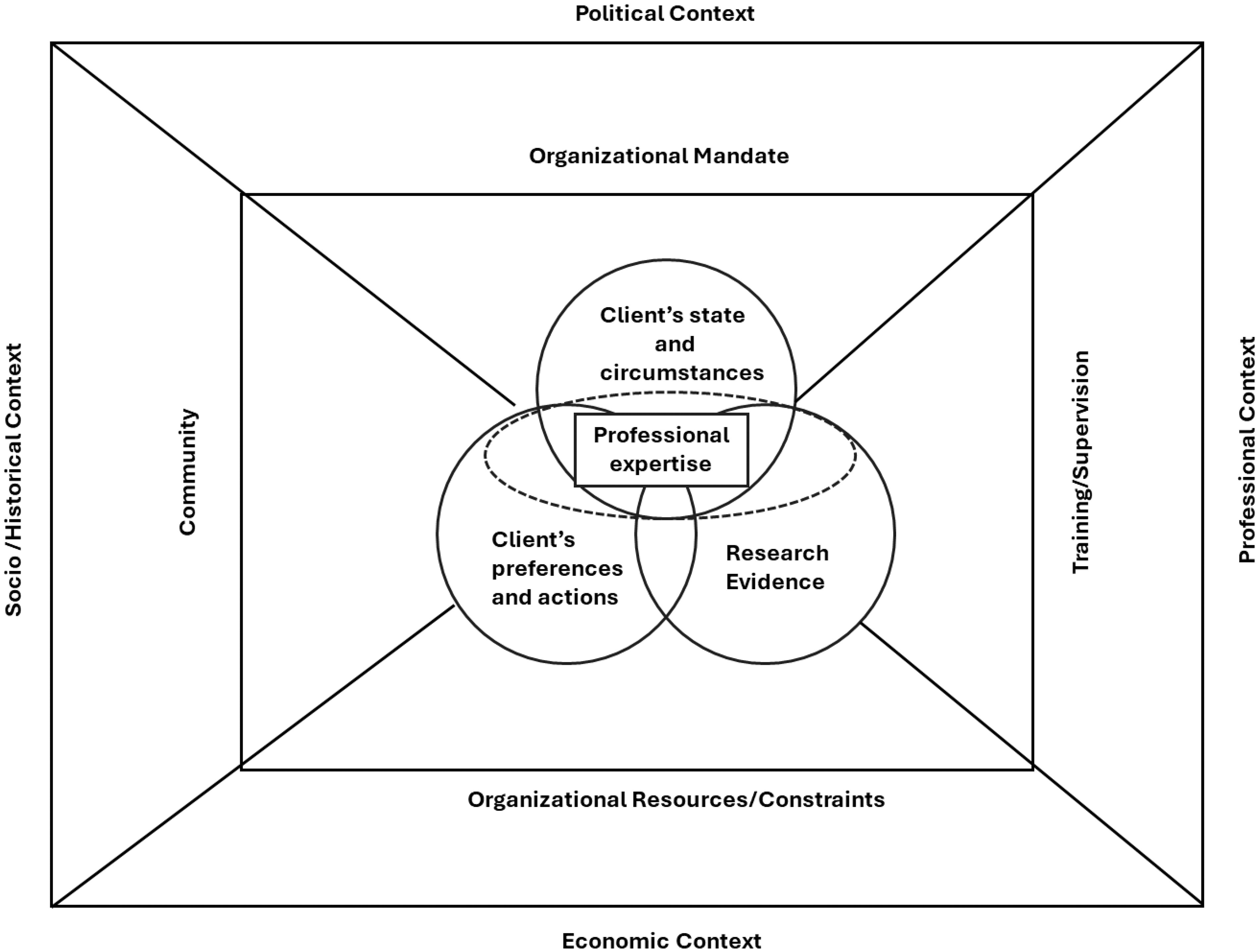
Elements of Evidence-Based Policy and Practice (EBPP). Adapted from Satterfield et al., (2009).
The details of the semi-structured interview are presented in Supplementary Appendix.
Sample
Eligible interviewees were child psychiatrists in the Greater Houston area, with at least 50% of their time dedicated to clinical care. Potential participants were identified through purposive sampling method (Sellars et al., 2022), beginning with personal contacts of the research team. From January, 2022, to April, 2022, recruitment letters asking potential interviewees to participate in an online research interview to be recorded were sent by email to 25 practicing child psychiatrists, who met the inclusion criteria. Also included in this email was the study consent document, and a version of the semi-structured interview that did not include interviewer prompts.
Recruitment email and consent form both noted that the interview would be recorded, and that responses would be anonymous, with no specific interviewee connected to any comment. The participant interviews were conducted by two of the study researchers (S.S. and P.R.). Once the interviewee joined online, research consent information was reviewed, verbal consent was obtained, and the interview commenced. The auto-caption option for this video conference service was used to provide an initial transcript. At the conclusion of the interview, interviewees were informed that they were free to email along any further thoughts or ideas. After the interview, a researcher reviewed the transcript against the recording to correct mistakes, and thus provide a transcript of the interview. Transcribed interviews served as the raw data for analysis.
Data analysis
The “Framework Analysis” qualitative research method (Brooks et al., 2015; Ritchie et al., 2013; Spencer et al., 2014) was used for interview analysis. Framework Analysis is a qualitative research approach, drawing upon template analysis (Braun and Clarke, 2006), which was developed for policy-relevant health care topics. This approach is in a “realist” epistemological approach (Maxwell and Mittapalli, 2010: 156–157), particularly because providers and patients generally recognize and participate in a social context with shared clinical and health care concepts, and social roles. Further, this analysis depends on a recognized model of health care decision making, and so justifies a corresponding a priori-developed coding template, with further coding, per template analysis, being performed on interview data, per Framework Analysis methods. This data analysis approach is well-suited for the goals of understanding how compliance with metabolic monitoring might be improved, but it is acknowledged that this approach can fail to detect phenomena that otherwise would be discovered with other qualitative approaches.
Framework Analysis requires five stages of analysis to arrive at conclusive findings. In the first step, “familiarization,” the transcripts were read to provide familiarity with the content. In the next step, “Identify Thematic Framework,” all concepts were noted to develop a content coding system. There can be major coding categories and subcategories. Two researchers (S.S. and P.R.) independently coded the first few interviews, and reconciled these to arrive at a single content coding system. In the next step, “Indexing,” all transcripts were coded by two researchers (S.S. and P.R.), using the noted Index. This coding was reviewed, and discrepancies were reconciled. In the “Charting” step, text from all interviews was rearranged to be grouped by the Index coding framework. Content in each major coding category was reviewed to develop an optimal arrangement (subcategories, lists, etc.) for all the content within each major category. This “Charting” was compared to the Regehr model to determine whether the Regehr model served well as an organizing conceptual guide. In the “Mapping and Interpretation” step, a description was given to the coded and arranged content. Study findings were drafted from this final stage.
Saturation of concepts (i.e., the point at which no new information emerges from the data) was also assessed using a process that examines concepts across sets of consecutive interviews. All study methods, including verbal/online consent from interviewees, were approved by the Institutional Review Board of the University of Houston.
Results
Characteristics of participants
Of the 25 child psychiatrists invited, 17 responded and completed the study. Of these, 10 worked in a group outpatient clinic, 2 in the hospital inpatient setting (consultant liaison for child and adolescent psychiatry), and 5 at a federally qualified health center. There were 4 who were early-career psychiatrists with 1–2 years of experience posttraining and specialization, 5 who had 3 to 10 years of experience, and 8 who had 11 or more years of experience. The median years of clinical practice experience of the participants were 10.5 (IQR 3.5–14) years. Interviews were transcribed and coded per stated methods. We had four major categories, per our a priori template. Upon developing the complete coding template, one of these had two sublevels, and one had three. Within these categories, there were 24 specific content codes regarding why metabolic monitoring might not be performed as specified by clinical guidelines. These were revealed by the twelfth of the 17 interviews, yielding content saturation.
Barriers to Metabolic Monitoring
The reported likely barriers to guideline-recommended rates of metabolic monitoring, elicited from these prescribers, did conceptually fit in the Regehr model of clinical decision making, with barriers at the patient–provider level, organizational level, or the social and contextual level. Table 1 also summarizes the findings.
Suggested Barriers to Metabolic Monitoring in Children and Adolescents Prescribed SGAs, Following the EBPP Model of Influences Upon Clinical Decision Making
EBPP, Elements of Evidence-Based Policy and Practice; SGA, second-generation antipsychotics.
A.
There were three patient-oriented barriers, as follows:
Patient Fear of Blood Draw: Interviewees noted that many patients are afraid of blood draw. Some families are very hesitant to make their child overcome this fear, since they know their child may act aggressively when irritated or scared.
Excessive Blood Draws: Interviewees noted that, on occasion, adding a blood draw for metabolic monitoring may seem excessive to the patient or family, since blood draws may have recently been ordered by other providers for other purposes. Families may not comply if they believe too many are being ordered or that multiple providers may not be aware of other blood draw orders, and so orders are duplicative.
Burden Upon Family: There are a few ways that compliance with labs may be a burden on the child’s family. Families may be overburdened dealing with the child’s behavior, such as aggressiveness, which is part of the mental disorder. Getting a young child to fast was also noted as possibly being burdensome for a family. Families may be burdened by multiple medical appointments and the complexity of health care, including being aware of insurance coverage. Some families may be burdened by time restraints, travel distance, and costs such as traveling to a different location for lab draws instead of the prescriber visit location
There were seven provider-oriented barriers, as follows:
Professional Judgment: Some providers expressed that, in this as well as other clinical situations, professional judgment and discretion take precedence over guideline recommendations.
Perceived Family Burden: Psychiatrists may take the path of least resistance and skip metabolic monitoring because families seem overburdened with the challenges of child management for a child who has a psychiatric condition.
Complacency: Interviewees said that they believe some providers probably get complacent regarding monitoring.
Assuming Low Risk: Some interviewees indicated that some providers may assume that the patient is at low risk.
Short-Term Use: Some providers may fail to order metabolic monitoring because they only plan to use the SGAs for short term.
Fear of Alarming Patient/Family: Psychiatrists may be reluctant to explain the side effects for which the metabolic monitoring is required since the provider may believe that the possibility of these side effects may alarm the parents and lead to nonadherence.
Relying on Previous Test: For long-term SGA recipients, providers may assume no change in laboratory values if there was none reported earlier. Psychiatrists could stop monitoring for long-term use when patients get to a good dose and when patients are responding well.
B.
There were several organization-level barriers, and after coding and review, these seemed to fit well in the Regehr model categories of “Organizational Mandates,” “Organizational Resources and Restraints,” “Training/Supervision,” and “Community.”
1. “Organizational Mandates” category
Lack of Organizational Mandates: Providers from the Federally Qualified Health Centers (FQHC) noted that they were mandated to carry out guideline-based monitoring, and that this was assessed as a performance measure by monthly and quarterly tracking; interviewees from other settings noted no such organizational mandate.
Lack of Performance Standard/Lack of Financial Incentive: Some workplaces set, and review, performance standards and so promote guideline-adherent metabolic monitoring. Performance monitoring also can be incentivized by a performance bonus, so lack of a bonus may be a barrier to monitoring.
The following are listed barriers in the “Organizational Resources and Restraints” category:
Overburdened Providers: Workplace demands may overburden providers, and so providers shift to getting the most essential aspects of care completed, and so some may delay or ignore metabolic monitoring.
Organizational Pressure for Limited Time per Patient Visit: Interviewees noted that scheduled appointment times do not leave enough time for all desired tasks for patients with complex care needs, so ordering or discussing labs may be one of the possible range of tasks delayed or ignored. Also, the need to document all covered topics may lead to pressure to not discuss, and thus not need to document, metabolic labs.
Monitored Elsewhere: Psychiatrists may assume that metabolic monitoring is being done elsewhere (such as pediatric primary care) for patients with multiple comorbidities.
Lack of Co-Located Labs: Interviewees noted that when lab facilities are not co-located, families may be less likely to follow through with directions to get labs drawn, and providers may also be sensitive to the greater difficulty for the family to get labs if not co-located, and so may emphasize this less.
Lack of Care Coordination Staff, Lack of Care Pathway: While the prescriber has the role of reviewing symptoms and treatment with each patient, in some care settings, there may be no staff to help navigate or coordinate a patient and family through the process of accessing a lab to comply with lab orders.
Lack of EMR Support: EMRs can include prompts or reminders for guideline-compliant labs, but not all include this. EMRs generally are customizable, but a care setting’s specific system may not be customized to provide prompts and guidance particular to behavioral health care needs, including those that are specific to SGA prescription. A provider’s EMR may lack inter-operability with other systems, such as not having a link with an affiliated lab for automated or facilitated lab order entry. A provider’s EMR may not be designed to have lab results automatically populated; thus, receiving lab results requires more direct effort. A provider may face a high burden of EMR-based documentation, which can reduce compliance with any of the mandated or promoted EMR activities.
2. “Training/Supervision” category
Unfamiliarity with Addressing Metabolic Disorder: Providers may be hesitant to order metabolic monitoring because they may be unsure of how to clinically respond to any elevated labs, since this is not their specialty.
Personnel Turnover: Turnover rates in the health care setting, whether it is the prescriber or other staff, can be a barrier in many ways to consistent clinical care performance. A family may opt to not return once they realize that they will not be with the same provider on the subsequent visit.
3. “Community” category
Lack of Lab Staff Specially Trained to Handle Difficult Behaviors: While some labs may have lab staff who are experienced at managing children with aggression or other challenging behavior problems, this is not very common.
Cross-Provider Communication: Prescribers may have barriers in record transfer and retrieval with other health care providers and organizations, such as a pediatric primary care provider in another health care setting, or from a recent hospitalization. A provider may have difficulty getting a lab order to a lab and may have difficulty getting lab results after the lab is completed. Also, a behavioral health provider may have difficulty communicating with a primary care pediatric provider, such as to find out what labs have been performed recently, or to share abnormal lab results. This can occur in-house and may be more likely when another provider is in a different health care system. Finally, there can be gaps in care, including missing timely metabolic monitoring labs, if patients make a care transition, such as transitioning from having the primary pediatric care provider oversee behavioral care to specialty behavioral care, with a pediatric psychiatrist.
Reimbursement for Services: A barrier to monitoring may arise when the provider and setting have difficulty submitting services for reimbursement, or when reimbursement is denied, for claims submitted. From interviews, this seems to be less of a problem for larger health care organizations, and for patients with public versus private insurance. Furthermore, the burden of documentation required to submit a successful claim for metabolic monitoring, frequent changes in documentation required, and different documentation requirements between payers may be a disincentive.
C.
At the level of social and contextual barriers, there were two main categories of reasons why providers may not adhere to metabolic monitoring:
Stigma: Although families may be bringing their child for psychiatric care, the family may still have stigma regarding mental illness, and may prefer to avoid getting labs drawn as one way to avoid cultural stigma. One interviewee noted that families can have suspicion about the anonymity of lab work, and so may preserve anonymity, and avoid stigma, by avoiding lab work. One interviewee specifically noted that there may be stigma in the Hispanic community. Some interviewees noted that there may be stigma against weight gain in some cultural or ethnic groups, and this may lead to avoidance of metabolic monitoring labs. Others commented that weight gain may not be a troubling concern in some cultural or ethnic groups, since being overweight is not stigmatized in some cultures, and so there was not a pressing need for guarding against weight gain.
Lack of Appreciation of Risk of Metabolic Disorder: Some interviewees noted that families may not be concerned about metabolic side effects if they cannot perceive the risk. Some interviewees noted that families, despite education, may not grasp the threat of metabolic disorder, possibly as part of an overall low level of health literacy.
Discussion
Despite practice guidelines recommending regular metabolic monitoring for children and adolescents prescribed SGAs, monitoring rates are low—hovering around 5%–30% (Morrato et al., 2009; Connolly et al., 2015; Haupt et al., 2009; Rodday et al., 2015; Sanyal et al., 2023a).
This study was conducted to understand why child and adolescent psychiatrists may not comply with these recommendations. A range of patient, practice, and organizational barriers has been revealed through these prescriber interviews. The most prominent barriers identified include children’s fear of blood draws and resource constraints such as the absence of an onsite or co-located lab, limited interaction time with patients, EMR systems that do not support monitoring practice, and poor health care coordination. The requirement of an organizational mandate resulting in better monitoring rate was a recurring theme among providers at FQHC. Early career providers often encountered high personnel turnover rates. Basic elements of themes for barriers and challenges were present as early as 7 interviews conducted. Overall saturation of themes such as organizational mandate was observed much earlier for providers practicing within similar settings such as providers affiliated to FQHC. Overall, providers readily identified influences that fit on the more central categories of the Regehr model (Regehr et al., 2007), and this may be because these are more obvious than the more abstract parts of this model. Providers know their training and experience, their work settings, and their patients.
These noted barriers overlap with the only qualitative study we could locate, conducted in Australia, which noted a lack of adequate resources to conduct monitoring and patient’s refusal to undergo blood tests were the major barriers to SGA metabolic monitoring in children and adolescents. With barriers identified by this study, health care settings, professional organizations, and policymakers can emphasize corresponding solutions.
Along with those findings in common with previous studies, our study reveals some original findings. For example, our data showed that the lack of specific recommendations in current guidelines on mitigating interventions for SGA metabolic adverse events and the appropriate timing of the intervention initiation is a barrier to monitoring. Some providers expressed that, without specific guideline recommendations, child psychiatrists may be hesitant to order metabolic monitoring because they may be unsure of how to clinically respond to any elevated labs since that is not their specialty. The finding of this qualitative interview explains the reasons behind the findings of a quantitative study (Morrato et al., 2009) that reported the presence of abnormal metabolic parameters in adults on SGAs was not consistently associated with the selection of an SGA with lower metabolic risk, which was also supported by recent study in which a statistically significant association was not observed between the abnormal reading of metabolic parameters, such as hyperglycemia and dyslipidemia, and subsequent interventions for metabolic adverse events in children and adolescents on SGA (Sanyal et al., 2023c).
In addition, some interviewees noted that families, despite education, may not grasp the threat of metabolic disorder, possibly as part of an overall low level of health literacy. It requires some health literacy regarding metabolic health and illness to interpret the risk of elevated blood glucose levels, or rapid weight gain in children who are expected to be gaining weight normally as they grow older. Patients tend to make different decisions under the conditions of gains or losses in health (Schulman, 2019). Specifically for preventive care such as SGA metabolic screening, family members often do not perceive the metabolic ADEs associated with SGA as a loss of health, given the change is not visually apparent (i.e., hyperglycemia), They may misunderstand adverse drug event (ADE) with normal growth (i.e., weight gain). In contrast, they are more likely to perceive the missed workday, the child’s school day, and the cost associated with the monitoring as a loss.
While low rates of metabolic monitoring have been well-documented, this is one of the very few qualitative studies assessing possible reasons. The open-ended approach has permitted a range of possible barriers to be noted. While these are valid suggestions, it remains to be determined which barriers are operating in which settings, with which patient and provider populations. This set of possible barriers can contribute to quality improvement efforts.
Limitations
While providing valuable information regarding this issue, our study has weaknesses. A leading limitation is that these are perceived barriers. While they are based on the authentic experiences of prescribers, all noted perceived barriers may not necessarily operate in all settings. Providers with different training and in different settings, and in different jurisdictions such as other countries, might generate different barriers. Moreover, the sample size was small. This restricts the generalizability of results as some perceived barriers may be specific to the individual setting. Although, the semi-structured interview guide only allowed for probes after independent responses of participants, there could be some potential bias that might have occurred inadvertently through interviewer’s assumptions and preconceptions. However, generalizability and potential bias are inherent limitations of qualitative research based on semi-structured interviews (Blagden et al., 2021; Verville et al., 2021). Another limitation is that this study drew upon only one group of stakeholders. Other stakeholder groups, including patients, families of patients, pediatric clinic coordinators, and lab personnel, could also be queried. Thus, lack of sampling of nonclinicians and their perceptions about metabolic monitoring of SGAs in children and adolescents might also have affected the qualitative findings. Also, this study used convenience sampling; different prescriber recruitment strategies might elicit further possible barriers. While this may be true, it is also likely to provide diminishing returns; at some point, the most profound barriers will be noted. With our model-based interview, responses likely included the most impactful barriers.
There could be other barriers identified from other stakeholder perspectives. Future studies can focus on identifying barriers from the standpoint of a different group of stakeholders. Also, there may be more barriers to be detected by focusing on different patient populations, including cultural and racial/ethnic differences.
Conclusions
This study drew upon experienced prescribers to identify possible barriers explaining why the rate of metabolic monitoring of SGAs is low in children. The next steps are to determine which might be most impactful in a setting, and to pilot quality improvement strategies. The possible barriers noted in this study suggest many avenues for intervention, especially those focused on the organization and delivery of behavioral health care. This study paves the way for the design of targeted interventions and policies that will improve the management of metabolic syndrome associated with SGA use and reduce its associated long-term complications in children and adolescents.
Clinical Significance
Even a decade after the publication of pediatric guidelines for monitoring adverse events associated with second-generation antipsychotics (SGAs), many studies have shown that the compliance rate of metabolic monitoring is quite low.
There is a gap in current evidence from a real-world perspective regarding the barriers and challenges for low adherence to metabolic monitoring guidelines.
To thoroughly explore barriers to metabolic monitoring of child and adolescent patients in the United States, the authors conducted a qualitative study, with practicing child psychiatrists to discover their views of possible barriers to metabolic monitoring.
A range of patient, practice, and organizational barriers has been revealed through these prescriber interviews. The most prominent barriers identified include children’s fear of blood draws and resource constraints such as the absence of an onsite or co-located lab, limited interaction time with patients, EMR systems that do not support monitoring practice, and poor health care coordination.
This study paves the way for the design of targeted interventions and policies that will improve the management of metabolic syndrome associated with SGA use and reduce its associated long-term complications in children and adolescents.
Footnotes
Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Supplementary Material
Supplementary Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.