
Abstract
Objectives:
Patterns of psychotropic medication use in children and adolescents with Down syndrome (DS) are largely unknown. Clinical decisions are often made from evidence and experience from individuals with autism spectrum disorder (ASD) or intellectual disability (ID).
Methods:
Longitudinal data from 670 children with DS who received care in a specialty DS clinic from March 2021 to February 2024 were collected. After each clinic visit, the clinician indicated the presence or absence of co-occurring neurodevelopmental (ND) or mental health (MH) diagnoses, as well as whether the individual was prescribed a psychopharmacological treatment. We used descriptive statistics and analyzed associations between psychotropic medication use, co-occurring ND/MH conditions, and demographic data.
Results:
19.1% of patients were prescribed at least one psychotropic medication at their most recent clinical visit. Alpha-agonists were the most commonly prescribed medication class (30.8%), followed by stimulants (18.9%), and antidepressants (16.7%). There was a significant difference in psychotropic medication use by age, with older children having increased odds of being prescribed a psychotropic medication. There were no differences in psychotropic medication use across sex (p = 0.10), race (p = 0.10), or household income (p = 0.16).
Conclusions:
We found that one-fifth of patients with DS were prescribed psychotropic medications. Nearly every individual with DS who was prescribed a psychotropic medication had a co-occurring ND/MH condition, yet these rates were lower than what have been reported in children with ID, ASD, and attention deficit/hyperactivity disorder. Further research needs to include those with DS to further understand medication efficacy and safe dosing practices to ensure optimal outcomes.
Introduction
Down syndrome (DS) is the most common genetic condition associated with intellectual disability (ID). Neurodevelopmental (ND) and psychiatric conditions are commonly diagnosed among children and adolescents with DS, with estimates of at least one co-occurring diagnosis to be around 18%–38% (Capone et al., 2006). Although behavioral and educational interventions are primarily used to promote development and learning, psychotropic medications are also used to target various behavioral symptoms such as inattention, hyperactivity, anxiety, or aggression.
Little evidence exists regarding the patterns of psychotropic medication use in DS, with most clinicians relying on expert opinion and experience-driven recommendations (Palumbo, and McDougle 2018). Most clinicians make decisions based on experience with other populations, including cross-sectional and review articles evaluating psychotropic medication use in children with ID (Ji and Findling, 2016; Herzig et al., 2018; McLaren et al., 2021) or autism spectrum disorder (ASD) (Caplan et al., 2022; Madden et al., 2017). A recent article by Baumer and Capone (2023) provides a review of current literature and expert opinion for a practical approach to psychopharmacology in DS. Among the limited studies in individuals with DS, there is one cohort study that evaluates the association between age and psychotropic medication use among children and adolescents with DS, which found that the rates of psychotropic medication use were higher among adolescents and young adults compared with school-aged children (Downes et al., 2015).
With the lack of literature regarding use of psychotropic medication in DS, prescription patterns in the context of commonly diagnosed neurodevelopmental and mental health (ND/MH) conditions among children with DS, such as ASD, attention-deficit/hyperactivity disorder (ADHD), anxiety, and depression, are unknown. In this study, we aim to characterize the use of psychotropic medications among children and adolescents with DS at a tertiary care center, by (1) exploring the rates of psychotropic medication use among our study population across age and gender, (2) comparing the use of psychotropic medication based on the presence or absence of a co-occurring ND/MH conditions, and (3) investigating the rates of polypharmacy among the study population.
Methods
Longitudinal data were collected from a cohort of children, adolescents, and young adults with DS who received routine care in a DS clinic at a specialty pediatric referral hospital from March 2021 to February 2024. The DS clinic is a multidisciplinary program with team members consisting of developmental-behavioral pediatricians, an ND disability specialist child neurologist, a psychologist, and a pediatric nurse practitioner who provide specialty care for overall health and developmental needs. Patients primarily live in Massachusetts and the surrounding New England area with others who come from across the United States and the world. Individuals cared for in this clinic are seen approximately every 6–12 months, if not prescribed psychotropic medications, and approximately every 3 months, if prescribed medication by a DS clinician. For each encounter, the specialty DS clinician indicated any confirmed diagnosis of a co-occurring ND/MH using the Diagnostic Statistical Manual-5 diagnostic criteria. Clinicians also indicated whether the individual was prescribed a psychopharmacological treatment, either by that clinician or other community providers, and if so, the class of medication used. For this study, we included information from the most recent encounter. More information on the longitudinal database that houses the data used for this study can be found in (Baumer et al., 2024). The study was approved by the Boston Children’s Hospital Institutional Review Board.
Procedures
Co-occurring ND/MH (ASD, ADHD, anxiety or obsessive-compulsive disorder, depression, stereotypic movement disorder, tic disorder, developmental regression in DS, and catatonia) and sociodemographic factors (patient’s age at their most recent clinic visit, sex assigned at birth, self-reported race, primary language, and estimated household income) were extracted from the database. We included the following psychotropic medication classes: alpha-agonists, antidepressants (e.g., selective serotonin reuptake inhibitors; SSRIs, selective norepinepherine reuptake inhibitors; SNRIs, tricyclic antidepressants; TCAs, and bupropion), antipsychotics, antiseizure, anxiolytics (e.g., benzodiazepines, buspirone), and stimulants. Although SSRIs treat both anxiety and depression, we classified them under antidepressants. We did not include anyone who was taking an antiseizure medication if they had a known seizure disorder. Additionally, we did not include supplements or other over-the-counter therapies such as cannabidiol, probiotics, magnesium, fish oils, and others. Socioeconomic status was estimated using a zip code proxy linked to state census data as an estimate for the family’s household income. We divided the patients into the following age groupings: 0–6, 7–13, 14–17, and 18+ years old, per common pediatric age groupings (preschool, school-age, teenager, young adult) (Baumer et al., 2024).
Data analysis
We used frequency counts and mean values to summarize demographic characteristics of the sample. We used independent sample two-tailed t tests and χ2 tests when contrasting means and proportions to analyze the association between psychotropic medication use and demographic data. We used odds ratios adjusted for any co-occurring ND/MH condition to compare the rate of medication use across different sociodemographic variables. Statistical analyses were conducted in SAS 9.4 (SAS Institute, Cary, NC).
Results
In total, 670 unique patients with DS were seen for follow-up between March 2021 and February 2024 (Table 1). The mean age was 8.6 (standard deviation [SD] = 5.9) years, with 56.7% being male; 3.0% were Asian, 9.4% Black/African American, 12.7% other race, 7.6% unknown, and 67.3% were White. Our sample included data collected from 30 0- to 6-year-olds, 103 7- to 13-year-olds, 57 14- to 17-year-olds, and 37 18+-year-olds. English was the primary language for a substantial majority of the sample (86.0%) with a small minority speaking Spanish (6.6%), Portuguese (3.3%), or another language (4.2%). The majority of the sample (80.2%) were in the ‘moderate’ or ‘middle’ median household income brackets (>$34,282 to <$82,276). One-third (33.9%) of the sample had at least one co-occurring ND/MH diagnosis. The most common co-occurring disorders included ASD (11.9%), ADHD (11.3%), and behavioral disorder (11.0%).
Characteristics of Total Sample and Psychotropic Medication Usage
Information regarding race, annual household income, and primary language spoken were taken from the EMR and parents could decline to answer. Race and ethnicity categorizations were taken directly from preset options in the EMR; “Other” designation was selected at the time of registration into EMR.
Income quartiles were divided on median household income per individual’s zip code.
Subjects may have more than one neurodevelopmental or mental health condition; therefore, percentages exceed 100%.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; DS, Down syndrome; EMR, Electronic Medical Records; MH, mental health; ND, neurodevelopmental; OCD, obsessive-compulsive disorder; SD, standard deviation.
Psychotropic medication use
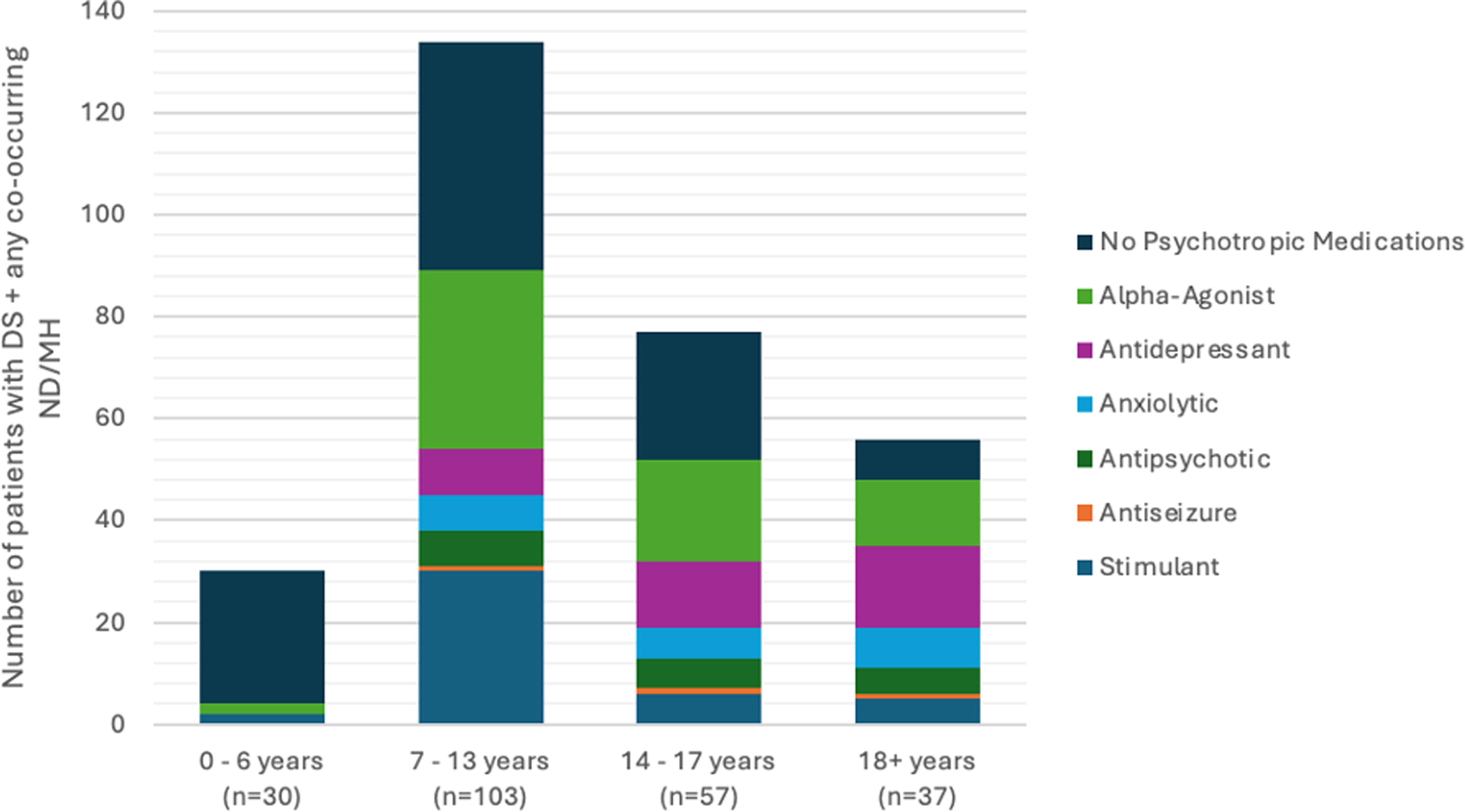
Nearly 20% (n = 128) of the patients were prescribed at least one psychotropic medication at their most recent clinical visit (Table 1). Of the patients with DS and at least one co-occurring ND/MH condition, alpha-agonists were the most commonly prescribed medication class (30.8%) followed by stimulants (18.9%) and antidepressants (16.7%) (Table 2). There was a significant difference in psychotropic medication use by age, with older children having increased odds of being prescribed a psychotropic medication (Fig. 1). After adjusting for co-occurring ND/MH, with each one year increase in age, the odds of being prescribed any psychotropic medication increased by 15% (adjusted odds ratio = 1.15; 95% confidence interval = 1.09–1.21). There were no differences in psychotropic medication use across sex (p = 0.10), race (p = 0.10), and household income (p = 0.16). English speakers were more likely to be prescribed a psychotropic medication (95.3% vs. 83.8%, p = 0.01).
Psychotropic medication class; usage among those with DS and any co-occurring ND or MH disordera. aSubjects may have more than one prescribed psychotropic medication class; therefore, counts exceed subset size. DS, Down syndrome; MH, mental health; ND, neurodevelopmental.
Psychotropic Medication Class Usage by Co-Occurring Neurodevelopmental Disorder or Mental Health Condition a
Subjects may have more than one prescribed psychotropic medication class; therefore, counts exceed subset size.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; DS, Down syndrome; EMR, Electronic Medical Records; MH, mental health; ND, neurodevelopmental; OCD, obsessive-compulsive disorder; SD, standard deviation.
We compared the classes of psychotropic medications prescribed relative to age (Fig. 1). Alpha-agonists were the most commonly prescribed psychotropic mediation class for 0- to 17-year-olds, followed by stimulants for 0- to 13-year-olds and antidepressants for 14- to 17-year-olds. Antidepressants were the most prescribed medication class for those 18 years and older.
Nearly every patient (96.1%) who was prescribed a psychotropic medication had at least one co-occurring ND/MH condition, with 37.8% having more than one co-occurring ND/MH disorder. The highest psychotropic medication usage was found among those with co-occurring ADHD (78.9%), catatonia (70.0%), depression (72.2%), or tic disorder (77.8%) (Table 2).
Nearly 80% of those with DS and co-occurring ADHD were prescribed a psychotropic medication, with 51.3% taking stimulants and 46.1% taking an alpha-agonist. Among those with co-occurring ASD, 40.0% were prescribed psychotropic medications, with alpha-agonists (31.3%) being the most commonly prescribed medication class; only a small portion were prescribed antipsychotics (10.0%), anxiolytics (8.8%), or antidepressants (8.8%) (Table 2).
Polypharmacy was common across the sample and increased with age (Fig. 2). Of the patients with DS and at least one co-occurring ND/MH condition, 53 (23.3%) were prescribed more than one medication class, and two patients (0.9%) were prescribed four different classes of medications.
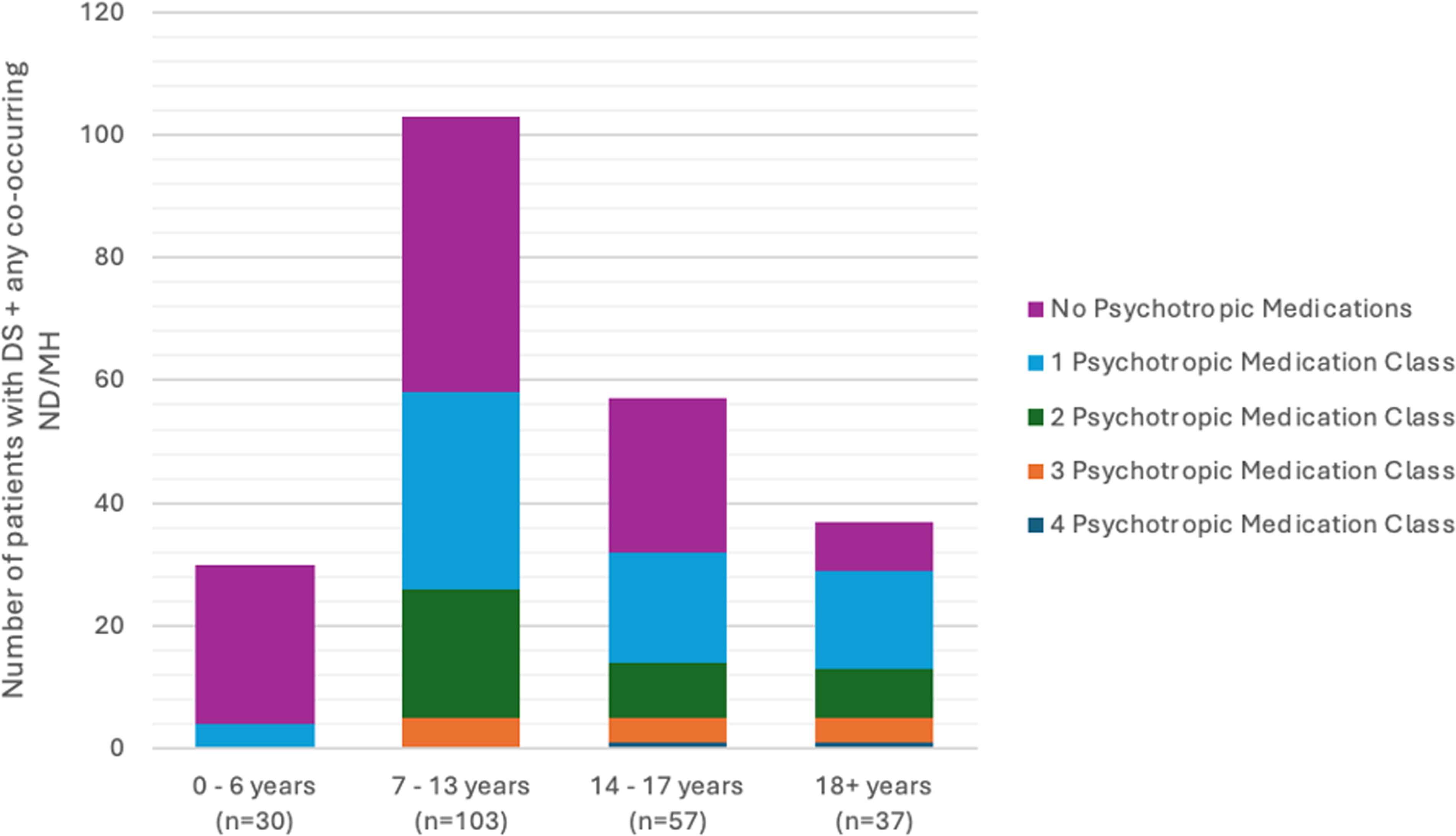
Number of psychotropic medication classes for patients with DS and any co-occurring ND or MH disorder. DS, Down syndrome; MH, mental health; ND, neurodevelopmental.
Discussion
This study characterized patterns and factors associated with psychotropic medication use among children and adolescents with DS. Broadly, we found relatively low rates of psychotropic medication use in this population, with only one-fifth of the patients seen in a large DS clinic at a specialty pediatric referral hospital being prescribed psychotropic medications. Although our findings are higher than reported rates of psychotropic medication use in the general population of children and adolescents, with estimates of 7%–10% (Shahidullah et al., 2023), it is much lower than psychotropic medication use in ASD, which is closer to 50% (Madden et al., 2017), in Fragile X Syndrome (63%; Dominick et al., 2021) or in ID (86%; McLaren et al., 2021). Although nearly a quarter of the cohort was prescribed more than one psychotropic medication class, rates of polypharmacy were lower than in other estimates of ID, where it is closer to 70% (McLaren et al., 2021).
We found no difference in prescribing rates across race, sex, and household income. The biggest predictor of a child with DS being prescribed a psychotropic medication was whether or not they have one or more formally diagnosed co-occurring ND/MH condition. Children with a co-occurring ND/MH condition were overwhelmingly more likely to be prescribed a psychotropic medication, which may be reflective of relatively strict prescription practice to only those with documented reason for medication and a provider hesitation to prescribe given lack of approved medications in DS, even among specialty providers. The five individuals who were prescribed a psychotropic medication who did not have a co-occurring ND or MH diagnosis were treated for targeted subthreshold symptoms of impulsivity, sleep disorders, and anxiety that did not meet full criteria for an ND or MH condition. The rate of psychotropic medication use increased with age, corresponding to an increased incidence of a co-occurring ND/MH condition.
Upon closer examination of those with DS and co-occurring ASD, prescription patterns in our sample mirror other psychotropic medication trends among children with ASD (Caplan et al., 2022). However, our population was less likely to be prescribed antipsychotics or antidepressants and more likely to be prescribed an alpha-agonist, which is important given that recommendations regarding the use of psychotropic medications in DS are largely guided by expert opinion (Baumer and Capone, 2023). Among those with co-occurring ADHD and DS, rates of medication use were much lower than in the general ADHD population (62%; Danielson et al., 2018). Furthermore, nearly half of our population with co-occurring ADHD was prescribed alpha-agonists. Alpha-agonists are one of the few medications that are known to be well tolerated in individuals with DS and have shown to have some improvements in the core symptoms of ADHD (Capone et al., 2016; Powers et al., 2024). Yet there is minimal evidence of their efficacy compared with stimulant medication (Cortese et al., 2018). There are currently no medications approved to treat the core symptoms of DS. Furthermore, no psychotropic medication has ever been tested in DS populations, leaving a lack of understanding on the safety and efficacy of these medications and how they are metabolized in individuals with DS.
Limitations to our dataset and the associated analyses should be acknowledged, including inclusion of patients from only one clinical site and geographic area, the high proportion of English-speaking and White individuals, and the presence of fewer patients in older age categories. Not including individuals with a known seizure disorder and those who are prescribed a subsequent antiseizure medication may have caused us to miss those who may have been prescribed an antiseizure medication to treat both seizures and behaviors. Our dataset did not include any information on indication of why psychotropic medications were prescribed, or about the tolerability of these medications. The increased psychotropic medication use in the older patients in this sample may be driven by the fact that patients with co-occurring NDs may require more frequent clinical care or may seek out treatment in a subspecialty clinic. Thus, the generalizability of our findings may be limited.
Integrating longitudinal data from more diverse cohorts in future analyses could help to reveal whether these trends hold true at the population level. Information from clinicians and families regarding the tolerability and effectiveness of therapies could also provide additional understanding of the utility of medication treatment, beyond the frequency of their use. In particular, the relative benefit of using alpha-agonists versus stimulants in these patients with a diagnosis of ADHD is still unknown, and clinicians rely on expert opinion when making decisions on medication treatment plans (Palumbo and McDougle, 2018). Future studies should provide information on specific safety and efficacy of these commonly used medications in DS.
Conclusions
This study provides clinicians with information on psychopharmacological medication prescription patterns in a large sample of children and adolescents with DS, which adds to existing clinical consensus information when making decisions on medication treatments. It highlights the need for additional research to understand how these medications are metabolized in children with DS to optimize dosing and efficacy in this population.
Footnotes
Authors’ Contributions
M.M. and N.B. conceived the study. S.W. and M.M. created the initial draft of the article. S.W. and R.D. conducted data analysis. All authors contributed to interpretation of the data and reviewed critically for content. All authors approved the final version of the article to be published.
Disclosures
The authors have no financial or commercial conflicts of interest to disclose.