
Abstract
Objective:
To compare the proportion of children and adolescents with incident psychotropic medication use from 2019 through 2022.
Methods:
This cross-sectional study used the IQVIA PharMetrics® Plus for Academics health plan claims database. Our study sample consisted of children and adolescents ages 6–18 who had at least one psychotropic medication in March 2019–February 2022. We examined psychotropic medication use in three distinct study periods: pre-pandemic (March 2019 to February 2020), pandemic-year-1 (March 2020–February 2021), and pandemic-year-2 (March 2021–February 2022). Incident use was defined as no evidence of psychotropic medication in the 12 months preceding the child and adolescent’s first psychotropic dispensing in each study period. We estimated incident psychotropic use in the three study periods. Average marginal effects tested for significant differences in psychotropic initiation, overall and stratified by age and sex.
Results:
In our sample of 42,346 children and adolescents who were dispensed any psychotropic medication during the study period, incident psychotropic users were 27.8% in pre-pandemic, 26.0% in pandemic-year-1, and 27.8% in pandemic-year-2. Incident use of antidepressants was 51.4% in pandemic-year-1 and 54.6% in pandemic-year-2. The probability of incident psychotropic use was 2.4% lower in pandemic-year-1 than in the pre-pandemic year (p < 0.001). The proportion of 6–11-year-olds and females initiating a psychotropic was higher in pandemic-year-2 than pre-pandemic.
Conclusion:
Incident psychotropic use was most notable in younger and female children 2 years after the pandemic onset.
Introduction
The COVID-19 pandemic contributed to a national mental health crisis among US children and adolescents (American Academy of Pediatrics, 2022). Previous studies reported increases in depression and anxiety (Madigan et al., 2023) and mental health-related emergency department visits, particularly in school-aged children (American Academy of Pediatrics, 2022; Holland et al., 2021). Psychotropic medication use among children and adolescents increased at the pandemic onset (Amill-Rosario et al., 2022). However, it is unknown if this increase reflects treatment for children and adolescents who had not previously used psychotropic medication, i.e., incident use. To date, few studies report incident psychotropic use in children and adolescents after the pandemic (Bliddal et al., 2023; Chai et al., 2024). One Danish study observed a continued increase in incident psychotropic use among persons ages 12 and older (Bliddal et al., 2023). A previous study evaluating pharmacy dispensing data did not distinguish between children and adolescents and only reported a select group of psychotropic classes (Chai et al., 2024). Knowledge of whether post-pandemic increase in psychotropic use (Amill-Rosario et al., 2022; Chua et al., 2024) reflects psychotropic naïve individuals would inform workforce needs to manage a larger patient population. To address this, we compared new initiation of psychotropic medication from 1-year pre-pandemic through 2-years post-pandemic onset.
Methods
Study design, data source, and study cohort
This cross-sectional study over the period of 2018–2022. We used a 25% random sample of the IQVIA PharMetrics® Plus for Academics data. This sample included 27.5 million individuals across the US. PharMetrics Plus for Academics is representative of the commercially insured US national population for patients under 65 years of age. The data also included a small percentage of individuals enrolled in Medicare Advantage, Medicare Supplement Insurance, and managed Medicaid plans. It contains a longitudinal view of inpatient and outpatient services, prescription and office/outpatient administered drugs, costs, and detailed enrollment information.
Over the period from March 2019 to February 2022, we defined three 12-month study periods: pre-pandemic (i.e., March 2019–February 2020), pandemic-year-1 (i.e., March 2020–February 2021), and pandemic-year-2 (i.e., March 2021–February 2022). We started each period in March to align with the start of the US public health emergency declaration.
Our study cohort included 6–18-year-old children and adolescents with any psychotropic medication dispensing during the study period. All individuals had to be continuously enrolled for 12 months preceding the date of the first psychotropic dispensing (i.e., index date) to be included in a study period (Supplementary Fig. S1).
Incident psychotropic user identification
We classified medications using the American Hospital Formulary System classifications into psychotropic therapeutic classes (Supplementary Table S1). The classes included attention-deficit/hyperactivity disorder medications (e.g., stimulants, atomoxetine), antidepressants, anxiolytics, antipsychotics, and mood stabilizers.
Incident use required individuals to be without any evidence of a psychotropic prescription in the 12 months preceding the index date and was measured in each study period. Prevalent psychotropic use included individuals with evidence of a psychotropic prescription in the 12 months preceding the index date and was measured in each study period. The 2018 data serve as the 12-month baseline for youth with psychotropic medication use in 2019. An individual could only be classified as an incident psychotropic user in one study period (Supplementary Fig. S2).
The incidence of new psychotropic use is the number of children and adolescents who initiated a new psychotropic medication (numerator) in a specific study period divided by the total number of children and adolescents with any psychotropic use (denominator) in the same period.
Statistical analysis
We compared the characteristics between children and adolescents who were incident and prevalent psychotropic users in each study period. Demographic characteristics and psychiatric diagnoses were identified in the 12 months preceding the index date for each study period. Chi-square statistics assessed significant differences between incident and prevalent users in each study period.
We used a generalized estimating equation model to estimate the average marginal effects, interpreted as the change in the probability of incident psychotropic use in each pandemic year relative to the pre-pandemic period. The model was adjusted for age, sex, and psychiatric diagnoses and robust standard errors were obtained by clustering at the person level. Models stratified by age (6–11 vs. 12–18 years-old) and sex tested for significant subgroup differences in incident psychotropic use. This study met the STROBE reporting guidelines. The University of Maryland Baltimore’s Institutional Review Board approved this study.
Results
Sample characteristics
In our sample of 42,346 children and adolescents, incident psychotropic users were 6563 (27.8% of 23,606) in the pre-pandemic period, 5402 (26.0% of 20,801) in pandemic-year-1, and 6047 (27.8% of 21,742) in pandemic-year-2 (Table 1). In all three study periods, adolescents aged 12–18-years-old were significantly less likely to be incident psychotropic users than children 6–11-years-old (71.3% vs. 74.6% pre-pandemic, 72.1% vs. 76.0% pandemic-year 1, and 73.6% vs. 77.1% pandemic-year 2, respectively, p < 0.001). Incident psychotropic users were more likely to be female than male, a finding that was consistent across all study periods (52.9% vs. 41.1% pre-pandemic, 57.1% vs. 43.0% pandemic-year-1, and 59.3% vs. 45.5% pandemic-year-2, respectively, p < 0.001; Table 1). More than half of psychotropic initiation in pandemic-year-1 and pandemic-year-2 involved an antidepressant (51.4% in pandemic-year-1 and 54.6% in pandemic-year-2) (Supplementary Table S2).
Baseline Characteristics of Psychotropic Users by Study Periods and Psychotropic Initiation
181 missing during the study period.
Incident and prevalent users for each year were compared. The chi-square test was used to calculate the p value for the comparison.
Psychotropic initiation period comparisons
The probability of psychotropic initiation significantly decreased by 2.4% points in pandemic-year-1 (p < 0.001) relative to the pre-pandemic period, but there was no significant difference between pandemic-year-2 and pre-pandemic (Fig. 1 and Supplementary Table S3). The age-stratified models for the probability of psychotropic initiation show a significant 2.3% (p = 0.009) point increase among 6–11-years-olds in the pandemic-year-2 relative to pre-pandemic but a 2.5% (p < 0.001) point decrease among 12–18-year-olds in pandemic-year-1 relative to pre-pandemic. Males had a significant 3.0% (p < 0.001) and 1.4% (p = 0.004) point decreases in the probability of psychotropic initiation in pandemic-year-1 and pandemic-year-2, respectively, relative to pre-pandemic. In contrast, females had a significant 1.6% (p = 0.008) point increase in the probability of psychotropic initiation in pandemic-year-2 relative to pre-pandemic.
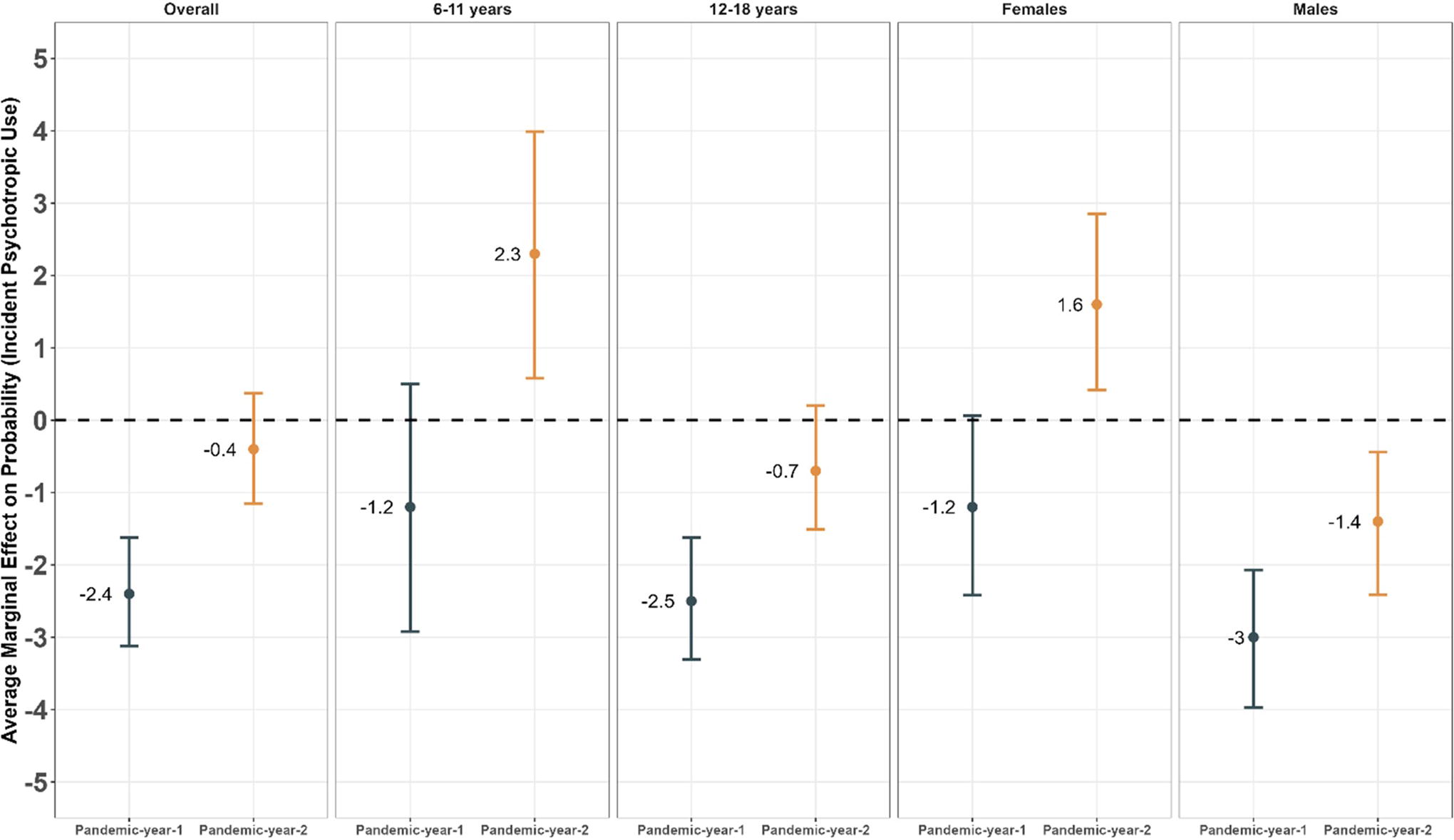
Average Marginal Effects on Probability (Incident Psychotropic Users) and 95% Confidence Interval in the Pandemic Years vs the Pre-pandemic Year among Children and Adolescents, Overall and by age and Sex Groups.
Discussion
The study findings show lower incident psychotropic use among commercially insured children and adolescents in the first pandemic year relative to pre-pandemic. The second pandemic year had a similar proportion of incident psychotropic use as the pre-pandemic period. Our findings contrast previous studies (Bliddal et al., 2023; Chai et al., 2024) that reported an increase in the incidence of psychotropic use following the pandemic onset. This may be due to differences in the population (Bliddal et al., 2023) and the measurement of incident users (Bliddal et al., 2023; Chai et al., 2024). It is also possible that the observed increase in these previous reports was among prevalent users.
The lower proportion of incident psychotropic users in the first pandemic year may reflect limited access to health care providers during the pandemic (Chavira et al., 2022). By the second pandemic year, there was expanded payment for virtual health care visits, and practices began seeing patients in person, which could contribute to the return to pre-pandemic levels (Randi, 2021).
Incident psychotropic use for 6–11-year-olds and females increased in pandemic-year-2, whereas this incident use in males decreased in both pandemic years relative to the pre-pandemic year. Several factors may underpin these findings. Youths 6–11-years-old experienced greater difficulty adjusting to virtual school than older youth (Scarpellini et al., 2021). Others have reported more significant emotional challenges and a higher depression risk in females than males (Halldorsdottir et al., 2021). Finally, mental health visits and psychotropic prescriptions for adolescent males declined during the pandemic (Burrell et al., 2024).
The findings in the study are limited to commercially insured children and adolescents in the US and cannot be generalized to those with public insurance, such as Medicaid, or those without insurance. Incident psychotropic use was based on a 12-month baseline period, and it is possible that the youth had previously been prescribed a psychotropic medication. Nonetheless, the absence of treatment for a year would constitute initiation. To mitigate information bias, we required continuous medical and prescription coverage to ensure we could observe prescription dispensing.
In summary, the increase in new psychotropic use was most notable in younger and female children 2 years after the pandemic onset. A future direction for this work is to assess potential interaction effects for specific therapeutic classes.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the University of Maryland, Baltimore. The statements, findings, conclusions, views, and opinions contained and expressed in this article are based in part on data obtained under license from IQVIA. Source: IQVIA PharMetrics® Plus for Academics, January 2006—December 2022. All Rights Reserved. The statements, findings, conclusions, views, and opinions contained and expressed herein are not necessarily those of IQVIA or any of its affiliated or subsidiary entities.
Authors’ Contributions
H.L.: Conceptualization, methodology, formal analysis, writing original draft. A.A.R.: Conceptualization, methodology, formal analysis, writing original draft, writing—review and editing, supervision. G.R.: Writing—reviewing and editing. S.D.R.: Conceptualization, methodology, formal analysis, writing original draft, writing—review and editing, and supervision.
Disclosures
S.D.R. receives funding from GSK and consults for Alexion for work unrelated to this paper. All other authors have no conflicts of interest to disclose.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.