
Abstract
Introduction:
Exposure to a range of stressful life events (SLE) is implicated in youth psychopathology. Previous studies point to a discrepancy between parents’/children’s reports regarding stressful life events. No study systematically assessed the correlation between such discrepancies and psychopathology in depressed youth. This study was designed to assess parent—youth discrepancies regarding stressful life events and its association with severity of psychopathology at baseline and response to selective serotonin reuptake inhibitor (SSRI) treatment in depressed youth.
Methods:
Reports regarding stressful life events were assessed in children/adolescents suffering from depressive/anxiety disorders using the life events checklist (LEC), a self-report questionnaire measuring the impact of negative life events (NLE) and positive life events (PLE), as reported by the children and their parents. The severity of depression/anxiety disorders and response to antidepressant treatment were evaluated and correlated with both measures of LEC.
Results:
Participants were 96 parent-child dyads (39 boys, 57 girls) aged 6–18 years (mean = 13.90 years, SD = 2.41). Parents reported more NLE and higher severity of NLE events than their children (number of NLE: 7.51 ± 4.17 vs. 6.04 ± 5.32; Cumulative severity of NLE: 24.95 ± 14.83 vs. 17.24 ± 12.94). Discrepancy in PLE, but not NLE, was associated with more severe psychopathology and reduced response to treatment.
Discussion:
Discrepancy in informant reports regarding life events in depressed/anxious youth, especially regarding PLE, is associated with more severe psychopathology and reduced response to pharmacotherapy. It is essential to use multiple reporters in assessing stressful life events in children.
Introduction
The agreement between the reports of parents and their children is a significant concern in child psychiatry) Zalsman et al., 2016). In most child psychopathologies and some physical disorders, parents and adolescents tend to give different reports of symptoms and signs, including depression (Nguyen et al., 1994) and anxiety (Weems et al., 2011). To achieve the most accurate assessment of psychopathology, there is a recommendation for separate interviews for different disorders, including anxiety (Weems et al., 2011), attention deficit and hyperactivity disorder (ADHD) (Klassen et al., 2006), and suicidality (Klaus et al., 2009). Discrepancy regarding negative life events (NLE) has specifically been reported, and some studies show that agreement between parents and children was lowest for life stressors (Yeh and Weisz, 2001). It has been noted that informant discrepancies for stressors are somewhat surprising given that stressors are supposedly concrete environmental events (Compas et al., 2004). Nevertheless, informant discrepancies for stressors may arise for similar reasons as for differences for other clinical constructs. For instance, it may reflect miscommunication in the family, especially regarding the reasons the child is in treatment. Discrepancies for youth stressors may also reveal important information regarding temperamental traits, both in youth and in the parent. Temperament has previously been linked to increased vulnerability for psychopathology or resilience in stressful contexts (Ferdinand et al., 2004). For example, high negative affectivity is associated with poorer emotion regulation in response to stressors (Cattane et al., 2022). In contrast, low negative affectivity and high effortful control are associated with positive outcomes (Flouri et al., 2019).
Checklist-style questionnaires are frequently used to assess the presence of stressors in both research and clinical practice. Such checklists measuring youth’s exposure to stressors have been developed for use with both adult informants (i.e., parent report) and child (i.e., self-report); however, researchers are constantly trying to examine the implications of relying on parent versus youth reports for stressors (Kushner and Tackett, 2017).
Compared with NLE, much less research has been conducted regarding the effects of positive life events (PLE) (Blonski et al., 2016). While some argue that PLE has a protective impact on well-being (Paykel, 2003), others say that positive events can have stress-generating properties and thus share an event-related, stress-generating component with negative events (Shahar and Priel, 2002).
Depression and anxiety are common in childhood and adolescence. Each disorder is associated with substantial functional impairment, and both disorders often co-occur (Cummings et al., 2014). Despite the significant differences between the two conditions, there is considerable overlap, specifically in the influence of NLE (Kneer et al., 2020). Since both disorders are multifactorial complex diseases, accumulated evidence suggests that both environmental and genetic factors are involved in the etiology of depression/anxiety. NLE are one of the most well-established risk factors for both disorders (Kendler et al., 1999; Paykel, 2003). A significant body of literature has shown that unipolar depressed adolescents have significantly more NLE than healthy controls and anxious children)Mayer et al., 2008; Williamson et al., 2005). Examples of such NLE include divorce of the parents, severe accidents or illnesses, and problems with school (Johnston et al., 2003). NLE during childhood have repeatedly been found to be associated with an increased risk of developing mental disorders during adulthood (Stikkelbroek et al., 2016).
However, no study systematically assessed the discrepancy in reports regarding NLE/PLE and psychopathology and response to treatment. The present investigation was designed around several goals. First, we examined the level of agreement between children and parents reporting of NLE/PLE across a sample of depressed/anxious children and adolescents. We hypothesized that, based on the current literature, depressed/anxious children would self-report more NLE and less PLE than their parents report for them. Second, we hypothesized that the higher the discrepancy between the parent and the child regarding life events, the higher the severity of the child’s psychopathology. Our third hypothesis was that discrepancy between the children and their parents would be associated with non-response to treatment with selective serotonin reuptake inhibitors (SSRIs), based on the hypothesis that disagreement may be related to heightened levels of stress and severe psychopathology.
Methods
The population: the clinical sample
All participants were children and adolescents between 6 to 18 years of age attending a tertiary hospital as new referrals and suffering from depression and/or anxiety disorders which demanded SSRI treatment. The study was approved by the Helsinki committee of Schneider Children Medical Center of Israel (SCMCI), and informed consent was obtained from the treated subjects and their parents.
Instruments
At intake, both youth and parents were asked to complete the life event checklist (LEC), a self-report questionnaire developed by Sarason (Sarason et al., 1978), which contains 51 life events. For each life event, the respondent is asked to indicate whether and when he experienced the events, if the event was positive or negative the degree to which the event was stressful/pleasant (coded on a 4-point scale ranging from no effect to great effect). Units of measure yielded by the LEC include the total number of PLE and NLE and the total impact of positive events (positive change score, PCS, range 0–204) and negative events (negative change score, NCS, range 0–204). Two weeks test-retest reliability of the LEC for children and adolescents has been reported to be 0.69 (positive events) and 0.72 (negative events) for simple unit weights, and 0.71 (positive events) and 0.66 (negative events) using weighted impact scores (Brand and Johnson, 1982). To check for levels of agreement between children and parents, the delta between the NCS/PCS of the parents and their children was calculated as follows: “NCS difference” = parent NCS—child NCS, “PCS difference” = parent PCS—child PCS (NCS range: ([−38]—[+66]), PCS range: ([−32]−[+28]). The higher the delta, the higher the disagreement between parents and child. These variables were referred to as “PSC difference” and “NCS difference”.
All the participants were assessed for clinical and demographic data (sex, age, body mass index [BMI], socioeconomic status).
The severity of psychopathology at baseline was established with several instruments: the severity of depressive symptoms was evaluated with the children’s depression rating scale (revised) (CDRS-R)—a structured interview for the evaluation of depressive disorders (Poznanski et al., 1985). The range of scores is between 0–119. The severity of anxiety symptoms was evaluated with the screen for child anxiety-related emotional disorders (SCARED)—a questionnaire filled out by the child and parents for the evaluation of anxiety disorders (Birmaher et al., 1999; Birmaher et al., 1997). The range of scores is between 0–76. Suicidality cluster symptoms were evaluated using the SIQ-SV –suicide ideation questionnaire, short version (SIQ-SV) completed by the child for the evaluation of suicidal ideation (SI) (Reynolds, 1987). The range of scores is between 8–56 (with high score indicating low suicidality level).
Response to treatment was measured with the Clinical Global Impressions–Improvement scale (Guy 1976). At the end of 8 weeks of treatment, a child was considered a responder if CGI-I = 1 or 2, or a non-responder if CGI-I ≥ 3. Also, the CDRS-R, SCARED, and SIQ-SV questionnaires were administered again to evaluate the severity of symptoms 8 weeks post-treatment. The psychopathology of the parents was assessed using the Family History Screen (Weissman et al., 2000). Ethnic background was determined according to the country of origin of the grandfathers and grandmothers and was divided into five regions (European, African, Asian, Americas, and Oceania and mixed) as was suggested for Israeli epidemiological studies (Lewin-Epstein and Cohen, 2019).
Procedure
For all the participants, research assistants individually administered the self-report measures for the children and the parents during the first clinic visit (i.e., before starting SSRI treatment). All parents and children were administered the same version of the LEC with instructions to complete the information regarding the children’s experiences. The mother or father filled out the LEC questionnaire for each child according to the family’s choice. The children were evaluated for the severity of depression and anxiety symptoms and SI. After 8 weeks of treatment, the children were evaluated again for response to treatment and severity of the different symptoms using the same questionnaires that were used at baseline.
Age and gender were inserted to all the statistical tests as covariates and were not found significant. Also, no siblings were included in this cohort.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS), version 26 for Windows (IBM corp, Armonk, NY) was used to create a database and conduct the statistical analyses. Two-way ANOVA, Mann–Whitney, chi-square tests, and Spearman’s correlations were used as appropriate. All analyses were two tailed and results expressed as Mean ± SD, with the level of significance set at 5%. p values were corrected for multiple testing using false discovery rate where applicable.
Results
Participants
Ninety-six children and adolescents and their parents participated in this study: 39 boys and 57 girls (average age = 13.90 ± 2.41 year). All children were treated with fluoxetine for 8 weeks. Six children were drawn out of the analysis due to missing data, thus leaving the sample with 90 children. The children suffered from depressive disorders (n = 7, 8%), anxiety disorders (n = 18, 20%) and comorbidity of depressive and anxiety disorders (n = 65, 73%). Out of children suffering from depression, 16 (18%) suffered from double depression (MDD+dysthymia). Most children suffering from anxiety disorders suffered from more than one anxiety disorder (usually social phobia): 31 suffered from a single anxiety disorder, 22 suffered from two anxiety disorders, 25 suffered from three anxiety disorders, and 5 suffered from four or more anxiety disorders. Forty-seven children (52%) suffered from ADHD. Fifteen children (17%) suffered also from OCD in addition to depression/anxiety disorders. The mean BDI score at baseline was 20.57 ± 11.08; The mean SCARED score at baseline was 31.64 ± 13.57; The mean CDRS-R score at baseline was 60.38 ± 18.03; The mean SIQ-RV score at baseline was 45.02 ± 12.08.
Out of the parents, 57 parents had anxiety/or depressive disorders (63%).
For the NLE/PLE reported by the children and their parents see Table 1. Gender, age, or main diagnosis did not have a significant effect of the number or severity of events reported by the children or their parents (p = NS for all). Also, there was no difference in the number and severity of PLE/NLE as assessed by the parents between parents with psychopathology vs. parents without (Mann–Whitney test, p = NS for all).
Number and Severity of Positive and Negative Events Reported by the Children and Parents
Number and Severity of Positive and Negative Events Reported by the Children and Parents
Number and severity of positive and negative events reported by the children and parents. Parents reported more negative events and a higher NCS than their children. No difference was observed regarding the positive events.
Adj. p value <0.05.
NGS, negative change score; PCS, positive change score.
A positive correlation was observed between parents’ reports and children’s reports on the number and intensity of positive/NLE (Spearman’s correlation: test for the number of positive events: r = 0.43, p < 0.001; test for PCS: r = 0.36, p = 0.001; test for the number of negative events: r = 0.44, p < 0.001, test for NCS: r = 0.52, p < 0.001).
Parents reported more negative events and a higher NCS as compared with their children. No difference was observed regarding the positive events (Fig. 1).
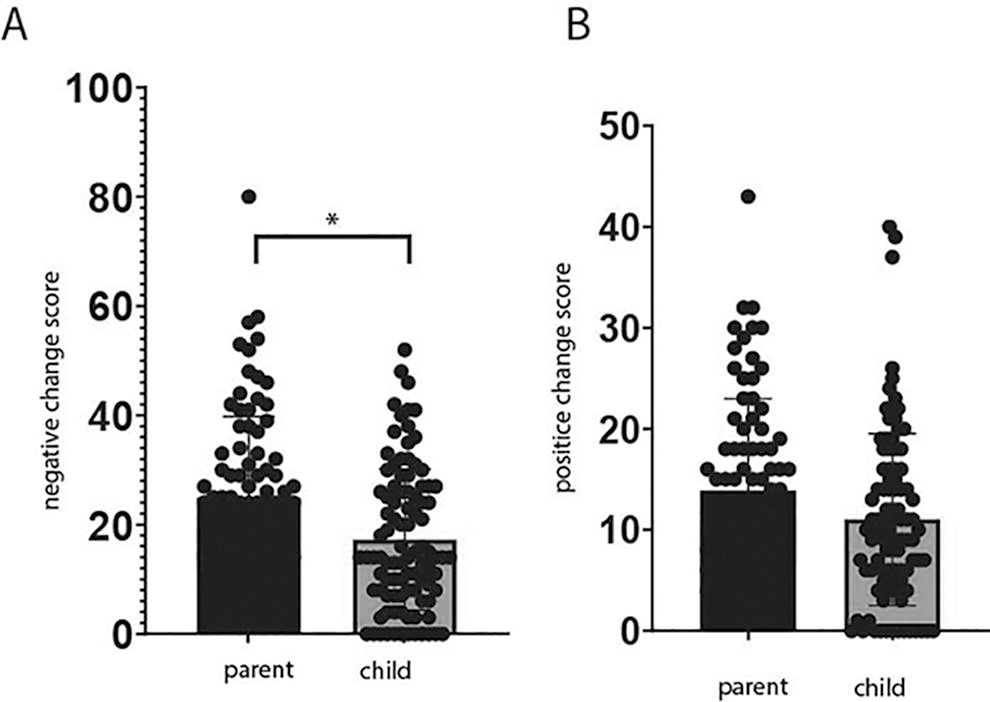
Parent–child discrepancy on the intensity of life events. A. Parents reported higher negative change scores than their children (related-samples Wilcoxon signed rank test, p value [adj.] = 0.0004). B. No difference was observed in the positive change score.
A positive correlation was found between parent PCS vs. child PCS (namely the “PCS difference”) and the CDRS-R score at baseline (Spearman’s correlation: r = 0.316, p = 0.005, p value[adj.] = 0.015). A negative correlation was found between parent PCS vs. child PCS (namely the “PCS difference”) and the SIQ-SV score at baseline (Spearman correlation: r=−0.28, p value[adj.] = 0.02), see Figure 2. No correlation was found regarding the NCS or parent NCS vs. child NCS.
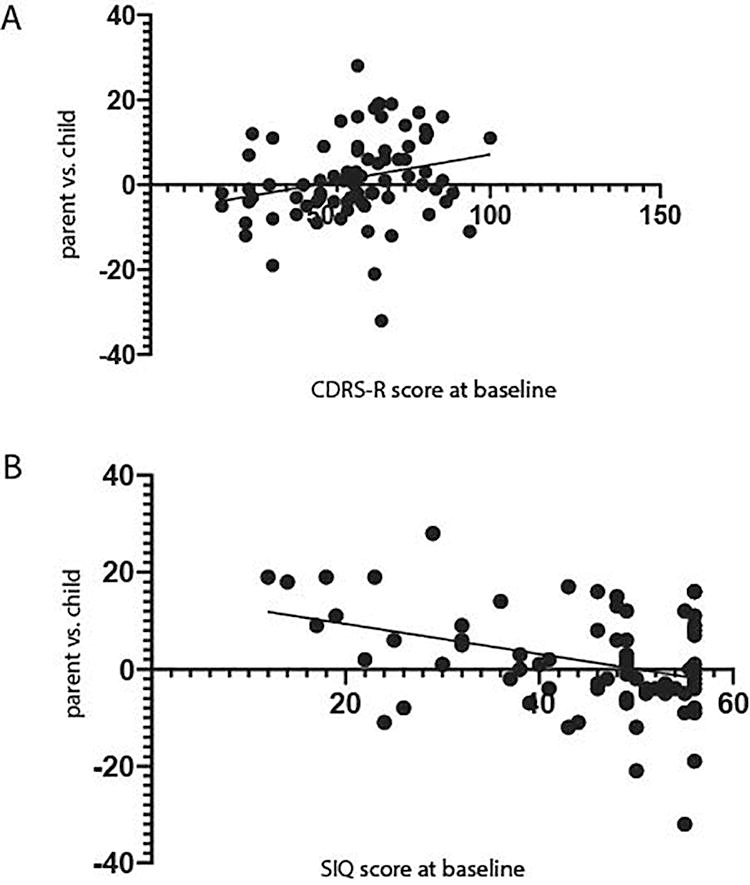
Correlation between child–parent disagreement and psychopathology of the child at baseline. A. A positive correlation was found between the “PCS difference” (i.e., parent vs. child) and the CDRS-R score at baseline (Spearman correlation: r = .0316, p value[adj.] = 0.015). The higher the delta, the higher the disagreement between parents and child. B. A negative correlation was found between the PCS difference and the SIQ-SV score at baseline (Spearman correlation: r = −0.28, p value[adj.] = 0.02). A higher SIQ-SV score reflects lower levels of suicidality. The higher the delta, the higher the disagreement between parents and child.
No correlation was found between parent PCS vs. child PCS (namely the “PCS difference”) and the SCARED score at baseline (Spearman’s correlation: r = 0.076, p = NS). Also, no correlation was found between parent NCS vs. child NCS (namely the “NCS difference”) and the SCARED score at baseline (Spearman’s correlation: r = −0.098 p = NS). No differences in all these values were observed between children and adolescents.
A negative correlation was observed between the parent vs. child PCS (namely the “PCS difference”) and CDRS-R scores between 8 weeks and bassline (Spearman’s correlation: r = −0.33, p value[adj.] = 0.012).; i.e., the higher the disagreement between parent and child regarding the intensity of PLE, the lower the improvement in depression severity. See Figure 3.

The correlation between parent-child disagreement on the severity of positive life events and improvement in CDRS-R scores. A negative correlation was found between the “PCS difference” (i.e., parent vs. child) and the delta in CDRS-R score between 8 weeks post-treatment and pretreamtnet (Spearman’s correlation: r = −0.33, p value[adj.] = 0.012). The higher the disagreement between parent and child, less improvement in depressive symptoms in response to treatment has occurred.
No correlation was found between “PCS difference and the delta in SCARED scores (Spearman’s correlation: r = 0.002, p = NS). Also, no correlation was found between “NCS difference” and the delta in SCARED scores (Spearman’s correlation: r = 0.012, p = NS).
No difference was found in the “PCS difference” between responders and non-responders to treatment according to CGI-I at week 8 (responders vs. non-responders: 0.97 ± 6.551 vs. 0.89 ± 11.39, Mann–Whitney: p = NS). Also, no difference was found in the “NCS difference” between responders and non-responders to treatment according to CGI-I at week 8 (responders vs. non-responders: 4.71 ± 14.39 vs. 6.91 ± 14.49, Mann–Whitney: p = sNS).
No differences were observed in all these values between children and adolescents.
Discussion
Three observations were made in this study regarding depressed youth. First, we found that the parents tend to report a higher intensity of NLE than their children, both in number and severity. Our second observation was that discrepancy between the parents and the children regarding PLE was associated with higher levels of depression and/or anxiety at baseline. Surprisingly, a discrepancy between child and parent regarding negative events was not related to the severity of psychopathology. Our third observation was that disagreement between the children and their parents regarding PLE, but not NLE, predicted non-response to treatment.
Discrepancies found between parents and children’s reporting of NLE differ as a function of different child illnesses or medical conditions (Johnston et al., 2003), while most prior studies have examined nonclinical samples of youth (Compas et al., 2004). In healthy children, parental ratings of life event-related stress for their child were significantly higher than their child’s ratings of stress) Rende and Plomin, 1991). One study showed that in children suffering from psychopathology, children report more events than their parents report for them (Bailey and Garralda, 1990). Based on this information, we hypothesized that in our cohort the children’s’ perceived stress levels would be higher than in the parents and more events would be reported, at least regarding NLE.
Our hypothesis was disputed: youth reported a lower intensity of NLE, both in severity and number, than their parents. This finding is interesting and deserves attention, especially since we expect depressed youth to perceive events in their lives as more stressful subjectively. Several explanations may exist for this finding: it may be that parents of depressed/anxious children perceive their child’ stress more severely than the child itself. Parental knowledge about their adolescent children is primarily informed by youth disclosure) Blonski et al., 2016). Depressed/anxious adolescents may not disclose potentially upsetting information, possibly not wanting to upset the parent, thereby limiting parental knowledge. This may lead to parents’ and adolescents’ variable perceptions of stressors, and possibly to overestimation of the parents’ level of stressful life events of the child. Alternatively, parents may withhold potentially upsetting information about family-level stressors (e.g., parental illness) from youth who are sensitive, anxious, or fearful in an effort to protect them from psychological distress (Shahar and Priel, 2002). Thus, the depressed/anxious youth may not be aware of a specific stressor which affects the parents’ mental state.
Important to note, we assumed that parents suffering from psychopathology would have higher NCS than healthy parents. It has been shown that depression-related cognitive biases or anxiety-related threat biases could result in more negative interpretations of events (for a review, see De Los Reyes et al., 2010), and thus we expected depressed parents to have higher perceived stress levels than healthy parents. Interestingly, no difference was noted between depressed vs. healthy parents. This may be because psychopathology in the child may be more influential to the parents than their own illness.
Given prior evidence for associations between parent—child discrepancies and youth psychopathology (Ferdinand et al., 2004), we hypothesized that in depressed/anxious youth, informant discrepancies for stressful life events would be positively correlated with psychopathology severity. Surprisingly, our results indicate that child-parent discrepancy regarding PLE, and not NLE, may lead to more severe psychopathology. It may be that when parents give more weight to PLE than the child, it is experienced as non-empathy by the children and thus exacerbates stress levels in the children. Discrepancy regarding NLE (with parents appraising events more severe than the children themselves), on the contrary, may be experienced as parents being empathic and thus lead to less symptom severity.
Previous data suggested that informant discrepancies can meaningfully affect treatment response as well as variability in treatment outcomes. This has already been shown regarding social phobia (De Los Reyes et al., 2010) as well as psychopathology in general (Ferdinand et al., 2004). Interestingly in this study, discrepancy in PLE, and not NLE, was correlated with non-response to treatment. The explanation again may be related to the fact that children experience the PLE difference as non-empathy by the parents.
Limitations
This study is not without limitations. First, different informant dyads may exhibit different patterns of consensus and disagreement on the occurrence of specific stressors. We did not include information regarding which of the parents (mother/father) filled out the questionnaire and thus could not address this point. A second major limitation is the lack of a control group of healthy children. Assessing children without psychopathology at baseline could contribute to our understanding of a possible causal relationship between discrepancies in reporting of NLE/PLE and severity of psychopathology. The potential confounding of the report with mental state and memory bias (both in parents and children) must be considered, i.e… there is a possibility that the severity of psychopathology is the cause of the discrepancy and not the result. Thus, we refrain from drawing any definite conclusions regarding causality. Another limitation is based on the nature of the collected data: data based on recall may be biased by falsification (Fennig et al., 2005). It may be that parents of depressed children report higher severity of NLE to explain their child’s illness. Similarly, subjects with depression might lessen the negative aspects and negative impact of life events based on the cognitive theory of depression focusing on increased negativity of cognitions about the self (Haaga et al., 1991). Another significant limitation is that we did not objectively measure the stress levels of the children and their parents, nor measures regarding post-traumatic symptoms as it is known that post-traumatic stress disorder or trauma in this population is a significant driver of differences in reporting of psychopathology.
Conclusion
Insights from the current research may yield promising applications for psychological assessment and therapeutic practice. Parent—youth disagreement in depressed/anxious children, especially regarding PLE, may identify adolescents who are prone to more severe psychopathology and also non-response to treatment. In contrast to prior research, youth reported lower levels of stressful life events than their parents. These results suggest that parents and adolescents may possess unique information about the informant stressors. It is essential to use multiple reporters in assessing stressful life events in children. Moreover, it is important to guide parents of depressed/anxious children to increase congruency and improve response to treatment.
Overall, these findings suggest important directions for future research to understand informant discrepancies as indicators of parental knowledge, youth disclosure, and psychopathology.
Footnotes
Acknowledgment
The authors acknowledge the previous version of this work that was available as a preprint: Amitai, M., Etedgi, E., Mevorach, T., et al. (2023). Discrepancy in the reports on life events between parents and their depressed/anxious children leads to severer psychopathology and lower responsiveness to SSRI treatment. Research Square [Preprint]. ![]()
Ethics Approval
The Helsinki committee of Schneider Children Medical Center of Israel (SCMCI) approved the study.
Informed Consent
Informed consent was obtained from the treated subjects and their parents.
Consent for Publication
All authors provided their consent for publication.
Authors’ Contributions
A.W., A.C., and A.A. conceptualized the research project; N.B.M. and S.F. helped in recruiting the patients; T.M., R.K., and A.A. passed the questionnaires to the participants and their parents; N.O.B. and N.H. helped perform the statistical analysis, M.A. wrote the article.
Author Disclosure Statement
No competing financial interests exist.