
Abstract
Objective:
The incidence of neuroleptic malignant syndrome (NMS), a rare, potentially fatal adverse effect of antipsychotics, among children and youth is unknown. This cohort study estimated NMS incidence in antipsychotic users age 5–24 years and described its variation according to patient and antipsychotic characteristics.
Methods:
We used national Medicaid data (2004–2013) to identify patients beginning antipsychotic treatment and calculated the incidence of NMS during antipsychotic current use. Adjusted hazard ratios (HRs) assessed the independent contribution of patient and antipsychotic characteristics to NMS risk.
Results:
The 1,032,084 patients had 131 NMS cases during 1,472,558 person-years of antipsychotic current use, or 8.9 per 100,000 person-years. The following five factors independently predicted increased incidence: age 18–24 years (HR [95% CI] = 2.45 [1.65–3.63]), schizophrenia spectrum and other psychotic disorders (HR = 5.86 [3.16–10.88]), neurodevelopmental disorders (HR = 7.11 [4.02–12.56]), antipsychotic dose >200mg chlorpromazine-equivalents (HR = 1.71 [1.15–2.54]), and first-generation antipsychotics (HR = 4.32 [2.74–6.82]). NMS incidence per 100,000 person-years increased from 1.8 (1.1–3.0) for those with none of these factors to 198.1 (132.8–295.6) for those with 4 or 5 factors. Findings were essentially unchanged in sensitivity analyses that restricted the study data to second-generation antipsychotics, children age 5–17 years, and the 5 most recent calendar years.
Conclusion:
In children and youth treated with antipsychotics, five factors independently identified patients with increased NMS incidence: age 18–24 years, schizophrenia spectrum and other psychotic disorders, neurodevelopmental disorders, first-generation drugs, and antipsychotic doses greater than 200 mg chlorpromazine-equivalents. Patients with 4 or 5 of these factors had more than 100 times the incidence of those with none. These findings could improve early identification of children and youth with elevated NMS risk, potentially leading to earlier detection and improved outcomes.
Introduction
Neuroleptic malignant syndrome (NMS) is a rare, potentially fatal neurological adverse effect of antipsychotics that presents with fever, rigidity, altered mental status, and autonomic and metabolic dysfunction (Schneider et al., 2020, Tse et al., 2015, Wijdicks, 2023). Case–control studies in adults have consistently linked higher doses (Berardi et al., 1998, Guinart et al., 2021, Keck et al., 1989, Sachdev et al., 1997, Su et al., 2014), rapid dose increase (Berardi et al., 1998, Keck et al., 1989), and first-generation antipsychotics—particularly haloperidol and other high-potency drugs (Nielsen et al., 2012, Su et al., 2014)—with increased incidence of NMS. Other markers of heightened NMS risk include prior NMS, catatonia, antipsychotic combinations, polypharmacy with lorazepam or other psychotropic medications, dehydration, and physical restraints (Berardi et al., 1998, Berman, 2011, Funayama et al., 2018, Nielsen et al., 2012, Su et al., 2014, Tse et al., 2015, Wijdicks, 2023), although some of these may be early manifestations of NMS or their treatment.
NMS has been reported for children and youth (Berloffa et al., 2021, Croarkin et al., 2008, Ghaziuddin et al., 2017, Henderson, 2011, León-Amenero and Huarcaya-Victoria, 2020, Neuhut et al., 2009, Ty and Rothner, 2001), who frequently are prescribed antipsychotics (Olfson et al., 2015) and who may be more vulnerable than adults to their adverse neurological effects (Correll et al., 2006). Case reports of NMS in children and adolescents have identified schizophrenia, neurodevelopmental disorders, and bipolar disorders as the diagnoses associated with antipsychotic treatment (Croarkin et al., 2008, Ghaziuddin et al., 2017, Henderson, 2011, León-Amenero and Huarcaya-Victoria, 2020), suggesting that, independent of antipsychotic dose and type, patients with certain major neuropsychiatric disorders might have increased risk of NMS. However, the case reports may simply reflect reporting bias, diagnosis-related differences in antipsychotic utilization, or antipsychotic treatment characteristics. Consequently, whether or not increased risk of NMS for children and youth is associated with specific antipsychotic indications, dose, or drug type is unknown.
Thus, we conducted a retrospective cohort study of NMS in a large national population of antipsychotic users 5–24 years of age (Ray et al., 2024). Our objectives were as follows: (1) to estimate the incidence of NMS in children and youth and (2) to describe variation in risk according to patient age, sex, diagnosis, and antipsychotic treatment characteristics, all of which are readily observable and potentially useful for identifying high-risk patients. To the best of our knowledge, this is the first controlled study of NMS in children and youth.
Methods
Cohort
Data
Study data came from a prior cohort study of antipsychotics and mortality in Medicaid beneficiaries 5–24 years of age (Ray et al., 2024). The data included enrollment, pharmacy, hospital, outpatient, and long-term care files from the Medicaid Analytic Extract, a national repository of data from the Medicaid and Children’s Health Insurance Programs (Supplementary Appendix SA1-a) (Leonard et al., 2017, Palmsten et al., 2013). The cohort was identified from data for 2004–2013; subsequent data availability and quality were adversely affected by a major transition in state Medicaid reporting requirements (Supplementary Appendix SA1-b) (anon, 2023a, anon, 2023b). Data came from 30 states collectively accounting for approximately 90% of Medicaid antipsychotic prescriptions for children and youth during the study period (Supplementary Appendix SA1-c, Supplementary Table SA1). Quality edits were performed to assure complete information on antipsychotic days of supply and dose (Supplementary Appendix S1-d, 1-e). Deaths were identified by linking Medicaid files with the National Death Index (NDI), a national registry of decedents (Supplementary Appendix SA1-f) (Wojcik et al., 2010). In accordance with Centers for Medicare and Medicaid Services policy, no data are reported for categories with fewer than 11 patients. The Vanderbilt University Medical Center IRB reviewed and approved the study, waiving informed consent.
Antipsychotics
Study antipsychotics were oral and intramuscular first- and second-generation drugs, including long-acting injectable antipsychotics and combinations with other medications (Supplementary Appendix SA2, Supplementary Table SA2). Antipsychotic prescriptions were identified from pharmacy claims, as well as outpatient claims, for administered antipsychotic injections. The prescription date was either that of dispensing (pharmacy) or administration (outpatient).
Cohort eligibility
The cohort included children and young adults (youth) 5 to 24 years of age. The lower age limit is that of initial school attendance for many children, with the consequent social and behavioral demands. The upper limit is that for the World Health Organization’s definition of youth (Bobo et al., 2013), which corresponds closely to definitions of emerging adulthood (Bennett et al., 2018, Kuwabara et al., 2007) and is consistent with other studies of psychotropic drugs in younger populations (Bobo et al., 2013, Cooper et al., 2011, Friedman and Leon, 2007, Olfson et al., 2012).
Cohort members were Medicaid beneficiaries in the 30 study states linked to the NDI with at least one antipsychotic prescription between January 1, 2004, and September 29, 2013, who met age and other cohort eligibility criteria (Supplementary Table SA3) on the prescription date. The patient had to have Medicaid enrollment on the qualifying prescription date and for the 4 preceding months and could not have Medicare or other insurance coverage. Because NMS risk is thought to be greatest early in treatment (Tse et al., 2015), there could be no antipsychotic prescription in the prior 120 days. There could be no inpatient, outpatient, or long-term care diagnosis of NMS in the past 120 days.
Follow-up
Follow-up began on t0, the date of the initial qualifying antipsychotic prescription. Follow-up ended on t1, the first of: September 29, 2013, the day preceding death or NMS occurrence, or 2 days prior to the 25th birthday. The analysis included all antipsychotic prescriptions with a date between t0 and t1 (Supplementary Appendix SA3, Supplementary Fig. SA1).
Neuroleptic malignant syndrome
NMS cases were identified from inpatient claims with an ICD-9-CM diagnosis code of 333.92 (neuroleptic malignant syndrome), which in one study had a positive predictive value of 82.9% (Lao et al., 2020), or an ICD-10 underlying cause of death code of G21.0 (malignant neuroleptic syndrome). The case definition did not consider emergency department or outpatient visits because it is unlikely that this life-threatening syndrome would be treated outside of inpatient settings. Secondary inpatient diagnoses were accepted because review of such claims indicated that the primary diagnosis typically was an NMS symptom (e.g., altered mental status), consequence (e.g., rhabdomyolysis), or psychiatric comorbidity (e.g., psychosis). The date of NMS generally was that of hospital admission, but was set to the prior day if there was an emergency department visit with an NMS diagnosis.
The case hospitalization was characterized according to length of stay and diagnoses and procedures during the stay. The stay included the initial hospitalization, as well as subsequent transfers. Because some lengthy hospital stays could include long-term care, the maximum length of stay was 30 days. Case fatality was defined as any death within 365 days of the NMS date.
Analysis
Antipsychotic prescription episode
Because antipsychotic use often is episodic and, over the 10-year study period, both patient and antipsychotic characteristics could change substantially, each prescription during follow-up defined an antipsychotic prescription episode (Supplementary Appendix SA4, Supplementary Fig. SA2). The definition of NMS generally requires recent antipsychotic exposure (Schneider et al., 2020); thus, analysis of person-time consisted of the current drug use defined by each episode, which began the day following the prescription date and ended with the first of the next prescription date, 30 days after the end of the days of supply (allowed for drug half-life, delayed outcome detection, nonadherence), or the day after t1.
Each antipsychotic prescription episode was characterized according to daily dose in chlorpromazine-equivalents (Supplementary Table SA2) (Lehman et al., 1998, Leucht et al., 2014, Meltzer et al., 2008, Woods, 2003), recent dose increase, antipsychotic type, and individual drug. If there were multiple prescriptions on a single date, the doses were summed and combinations with both first- and second-generation drugs were considered first generation. Recent dose increase was defined as either no antipsychotic prescription in the past 120 days or a dose greater than twice that of the prior prescription.
Diagnoses
Antipsychotic prescription episodes were classified into mutually exclusive diagnostic categories. The major neuropsychiatric disorders, for which there is an established clinical rationale for antipsychotic treatment in children and youth (DeBattista and Hawkins, 2009, Hirsch, 2018, Hodgins et al., 2022), included schizophrenia spectrum and other psychotic disorders, neurodevelopment disorders—autism spectrum disorders and intellectual disability, bipolar or major depressive disorder, and multiple major neuropsychiatric disorders (Supplementary Table SA4-a). The other diagnoses were defined hierarchically as other mood disorders, conduct or impulse control disorder, attention-deficit/hyperactivity disorder (ADHD), anxiety, panic or obsessive–compulsive disorder, stress, other psychiatric diagnosis, and no recorded psychiatric diagnosis (Supplementary Table SA4-b).
Diagnoses were identified from inpatient, outpatient, and long-term care claims during the 120 days preceding through the prescription date (Supplementary Fig. SA2). The primary analysis required only a single claim, which reduced misclassification of the “other diagnosis” category by inclusion of patients with major neuropsychiatric disorders. A sensitivity analysis required one inpatient or emergency department claim or at least two other outpatient claims on separate dates, similar to the claims-based studies that validated these diagnostic categories (Hartung et al., 2013, Lurie et al., 1992, Shea et al., 2024, Straub et al., 2021).
Statistical analyses
The unit of analysis was the individual antipsychotic prescription episode. Independence assumptions were not violated because the episodes were nonoverlapping and the outcome occurred only once (Arnold, 1990).
NMS incidence was calculated by dividing the number of events by person-years of current antipsychotic use; variances were estimated assuming the Poisson distribution. To determine the independent association of patient and treatment characteristics with NMS, a proportional hazards regression was performed with a model that included patient age, sex, prescription year, diagnosis, and antipsychotic treatment characteristics. The antipsychotic dose term indicated those in the upper quartile. The analysis of individual antipsychotics included those with at least 11 cases of NMS; the reference category was risperidone. All statistical analyses were performed with SAS version 9.4. Statistical significance was defined as a 95% confidence interval (CI) for the hazard ratio (HR) that excluded 1.
Sensitivity analyses
Sensitivity analyses focused on the following patient groups of particular interest: those receiving second-generation antipsychotics, children age 5–17 years, those with antipsychotic prescriptions in the 5 most recent study years, and patients without severe somatic illness (e.g., cerebral palsy, Supplementary Table SA5). They also assessed methodologic alternatives as follows: modeling antipsychotic dose as a continuous variable to control for residual confounding, a more restrictive definition of major neuropsychiatric diagnoses, and increasing the length of the look-back window for eligibility criteria to 365 days.
Results
Cohort
The study included 1,032,084 Medicaid patients age 5–24 years who began antipsychotic treatment between 1st January 2004 and 29th September 2013 (Supplementary Fig. SA3). Cohort members had 15,881,698 antipsychotic prescription episodes during follow-up (Table 1), of which 81.9% were for children age 5–17 years, 65.7% were for males, and 64.3% had a prescription date between 2009 and 2013. Major neuropsychiatric disorders were associated with 43.7% of prescription episodes, including schizophrenia spectrum and other psychotic disorders (5.1%), neurodevelopmental disorders (10.3%), bipolar or major depressive disorders (21.8%), and multiple major neuropsychiatric disorders (6.5%). The most frequent other diagnoses were other mood disorders (13.3%), conduct or impulse control disorders (12.3%), and ADHD (17.0%). The median (interquartile range [IQR]) antipsychotic daily dose was 100 (50–200) mg chlorpromazine-equivalents, 19.0% had a recent dose increase, and 97.3% of the prescription episodes were for second-generation drugs. The most frequently prescribed individual antipsychotics (Supplementary Table SA6) were risperidone (40.5%), aripiprazole (23.1%), quetiapine (20.4%), and ziprasidone (4.6%). Haloperidol was the most frequently prescribed first-generation drug (1.0%). Long-acting injectable antipsychotics accounted for 0.8% of prescription episodes (Supplementary Table SA6).
Characteristics of Antipsychotic Prescription Episodes During Cohort Follow-up
On the prescription date.
Categories defined hierarchically. For example, the “Conduct or impulse control disorder” does not include episodes with other mood disorders.
No antipsychotic prescription past 120 days or dose greater than twice that of prior prescription.
IQR, interquartile range.
NMS cases
Cohort members had 1,472,558 person-years of current antipsychotic use, during which there were 131 NMS cases, or 8.9 per 100,000 person-years. The median (IQR) length of the case inpatient stay was 7 (5–19) days (Table 2). During the hospital stay, 54.2% had an intensive care unit stay, 48.1% had CT or MRI imaging of the brain or head, and 21.4% had a lumbar puncture. Frequent diagnoses were altered mental status (46.6%), autonomic dysregulation (46.6%), fever (36.6%), rhabdomyolysis (35.9%), and metabolic disorders (19.1%). Case fatality could not be reported because of the small number of deaths.
Neuroleptic Malignant Syndrome Case Characteristics
Hypertension/hypotension, arrhythmia, dysphagia.
Pulmonary collapse, acute or chronic respiratory failure, respiratory arrest, other pulmonary insufficiency, tracheostomy/intubation, mechanical ventilation, cardiopulmonary respiration.
Dyspnea or other respiratory symptoms.
Hyperosmolality/hypernatremia, hypoosmolality/hyponatremia, acidosis/alkalosis, mixed acid–base balance disorder, hyperpotassemia, hypopotassemia, other electrolyte and fluid disorders.
indicates fewer than 11 cases. Characteristics determined from diagnoses and procedures during the inpatient stay for NMS.
IQR, interquartile range.
Factors associated with NMS incidence
Both patient and antipsychotic treatment characteristics were independently associated with the incidence of NMS (Table 3). Risk increased for patients age 18–24 years (HR [95% CI] = 2.45 [1.65–3.63]), but was not increased for males (HR = 0.94 [0.66–1.35]). When patients with a single major neuropsychiatric disorder were compared to those with other diagnoses, the incidence was significantly increased for schizophrenia spectrum and other psychotic disorders (HR = 5.86 [3.16–10.88]) and neurodevelopmental disorders (7.11 [4.02–12.56]), but was not significantly increased for bipolar or major depressive disorders (HR = 1.20 [0.61–2.37]). The incidence of NMS for prescriptions with daily doses >200mg chlorpromazine-equivalents was greater than that for lower doses (HR = 1.71 [1.15–2.54]). However, a recent dose increase was not associated with elevated risk (HR = 1.00 [0.68–1.47]).
Neuroleptic Malignant Syndrome Occurrence According to Patient and Antipsychotic Treatment Characteristics
No antipsychotic prescription in past 120 days or dose greater than twice that of prior prescription.
HRs are adjusted for the variables shown in table 1
CI, confidence interval; HR, Hazard ratio; NMS, Neuroleptic Malignant Syndrome.
The incidence of NMS for first-generation antipsychotics was greater than that for second-generation drugs (Table 3, HR = 4.32 [2.74–6.82]). When individual antipsychotics were compared with risperidone (Supplementary Table SA7), the HR was highest for haloperidol (7.10 [3.51–14.36]). The HRs for aripiprazole (0.92 [0.51–1.66]) and quetiapine (0.96 [0.51–1.80]) were not significantly increased, but that for ziprasidone (2.66 [1.34–5.29]) was. Patients administered long-acting injectable antipsychotics had too few cases of NMS for analysis.
We calculated the incidence of NMS according to the number of the following five factors each independently associated with increased risk: age 18–24 years, schizophrenia spectrum and other psychotic disorders, neurodevelopmental disorders, first-generation antipsychotic, and daily dose >200 mg chlorpromazine-equivalents. The incidence increased markedly with the number of these risk factors (Fig. 1). For those with none, the incidence was 1.8 (1.1–3.0) NMS cases per 100,000 person-years, whereas for those with 4 or 5 factors, the incidence was 198.1 (132.8–295.6) cases per 100,000 person-years.
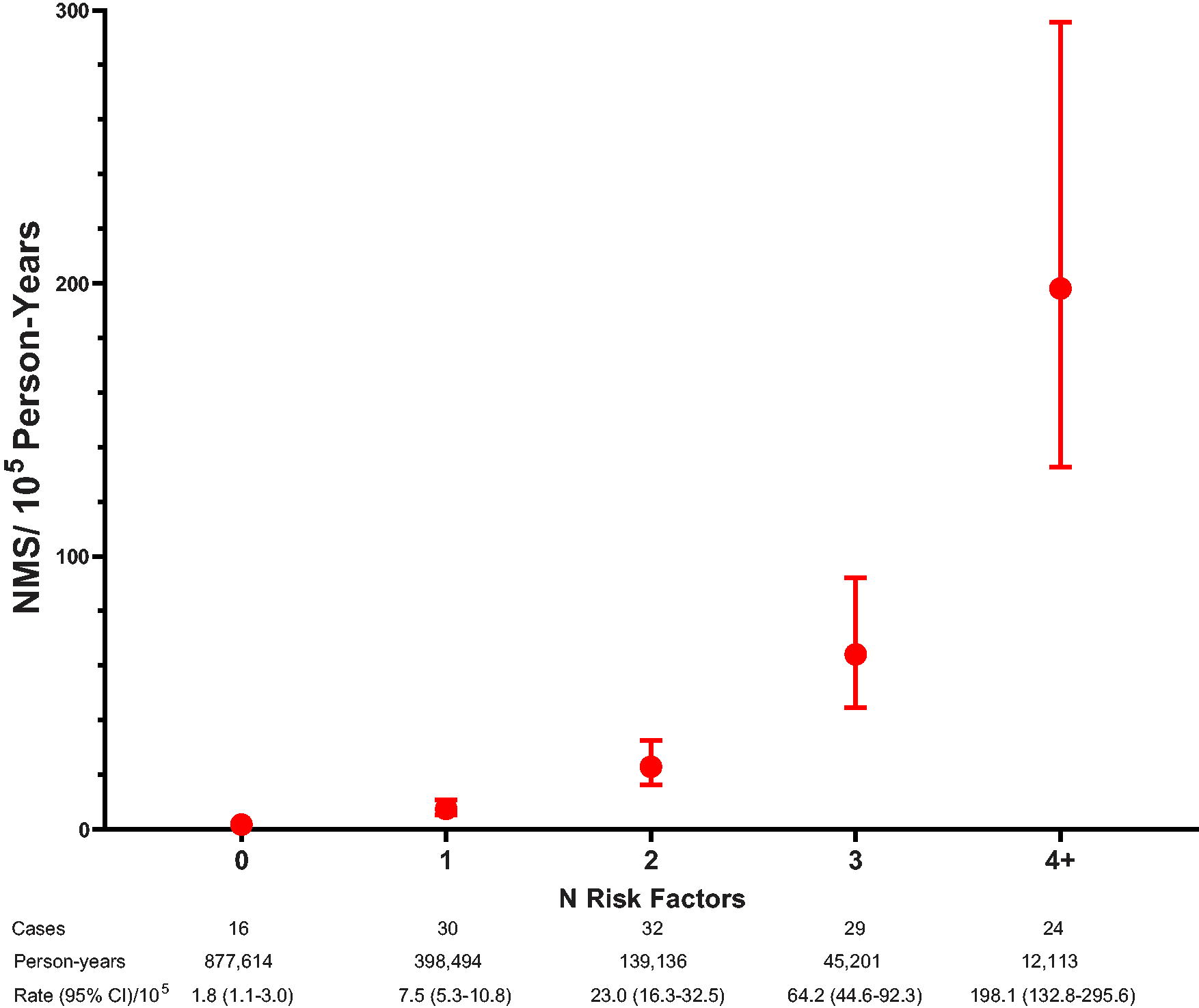
Incidence of NMS in children and youth according to N of risk factors: age 18–24 years, schizophrenia spectrum or other psychotic disorders, neurodevelopmental disorders, antipsychotic daily dose >200 mg chlorpromazine-equivalents, or first-generation antipsychotic. Whiskers represent the 95% CI. CI, confidence intervals; NMS, neuroleptic malignant syndrome.
Sensitivity analyses
The same five factors were independently associated with increased NMS incidence in each of the sensitivity analyses (Table 4). The 95% confidence intervals for the point estimates of the HRs in the sensitivity analyses included that of the primary analysis.
Sensitivity Analyses
See Supplementary Table S5.
Dose continuous variable. Units log(base 2) because change in risk hypothesized to be proportional to change in dose. The point estimate is the increase in HR for dose doubling.
Requires a single inpatient or emergency department diagnosis or outpatient diagnoses on at least two separate dates.
The look-back period is the interval preceding the prescription date to determine if cohort eligibility criteria are met.
No antipsychotic prescription in past 120 days or dose greater than twice that of prior prescription.
CI, confidence interval; HR, Hazard ratio.
Discussion
Neuroleptic malignant syndrome is one of the most serious adverse drug effects child and adolescent psychiatrists encounter in clinical practice. However, because this complication is rare, detection may be delayed or the syndrome misidentified, thus potentially leading to increased morbidity, prolonged inpatient stay, or death. This national cohort study of more than one million children and youth treated with antipsychotics during a 10-year period found that the following five factors were independently associated with significantly increased risk for NMS: age 18–24 years, schizophrenia spectrum and other psychotic disorders, neurodevelopmental disorders, antipsychotic dose greater than 200 mg chlorpromazine equivalents, and first-generation drugs. Incidence increased with the number of risk factors present; for patients with 4 or 5 the incidence was more than 100 times that for patients with none. These data thus provide a basis for early identification of children and youth at elevated risk for NMS for whom monitoring for signs of this life-threatening syndrome could be increased, potentially leading to earlier detection and improved outcomes.
The focus of prior NMS research has been adults with schizophrenia spectrum and other psychotic disorders (Berardi et al., 1998, Guinart et al., 2021, Keck et al., 1989, Nielsen et al., 2012, Sachdev et al., 1997, Su et al., 2014). However, we found that in the study cohort of children and youth there were more cases of NMS in patients with autism spectrum disorders or intellectual disability than for any other single study neuropsychiatric disorder. Furthermore, the point estimate of the HR for the study of neurodevelopmental disorders was greater than that for schizophrenia spectrum and other psychotic disorders. These findings underscore the need for practitioners who care for children and youth with neurodevelopmental disorders to monitor patients treated with antipsychotics for signs of NMS.
Several possible mechanisms may contribute to the strong association of schizophrenia spectrum and other psychotic disorders and neurodevelopmental disorders with increased incidence of NMS. In both disorders, the prevalence of the catatonia syndrome (Heckers and Walther, 2023) is elevated (Hauptman et al., 2023, Rogers et al., 2023, Walther et al., 2019), and in patients treated with antipsychotics, catatonia is associated with increased risk of NMS (Berardi et al., 1998, Funayama et al., 2018, Rogers et al., 2023). Disturbances in early brain development, thought to partially explain the psychopathology of both schizophrenia and neurodevelopmental disorders (Owen and O’Donovan, 2017, Rees et al., 2021), might also increase vulnerability to NMS. Other patient or treatment characteristics may be involved. Regardless of the mechanisms, our data indicate that these disorders identify children and youth for whom careful monitoring for signs of NMS should be considered.
Unlike some case–control studies in adults (Berardi et al., 1998, Keck et al., 1989), recent dose increase was not associated with increased risk for NMS. Differences in the study populations may explain this finding. The adult studies were set in inpatient psychiatric facilities where patients were predominantly treated with high doses of first-generation drugs, and rapid, substantial dose increases may have been more common than in outpatient settings. In contrast, the population in this study of children and youth was not restricted to inpatients, more than 97% of prescriptions were for second-generation antipsychotics, and dose escalation may have been more gradual.
Haloperidol had the highest incidence of NMS, which is consistent with the findings of one adult study (Su et al., 2014). Although haloperidol and other first-generation antipsychotics have more frequent extrapyramidal adverse effects than the second-generation drugs, haloperidol continues to be prescribed in emergency department and inpatient settings for children with agitation or delirium (Nash et al., 2023). Our findings suggest that younger patients in such settings who receive haloperidol, particularly those with schizophrenia spectrum and other psychotic disorders, or neurodevelopmental disorders, should be monitored for signs of NMS.
A case–control study in adults reported that aripiprazole was associated with increased risk of NMS (Su et al., 2014). In contrast, we found no significant differences in the incidence of NMS for risperidone, aripiprazole, and quetiapine, the most frequently prescribed antipsychotics in the study cohort. However, the incidence was significantly increased for ziprasidone; further research is needed to confirm this finding.
Limitations
There were several limitations. First, as in other studies (Guinart et al., 2021, Lao et al., 2020, Modi et al., 2016), NMS cases were identified retrospectively from inpatient discharge or underlying cause of death diagnostic codes and thus may be misclassified (Schneider et al., 2020, Wijdicks, 2023). Several lines of evidence suggest that the false positive rate for study cases was low. A chart-review study reported a positive predictive value of 82.9% for inpatient stays with an NMS discharge diagnosis (Lao et al., 2020), although whether this finding can be applied to the Medicaid database has not been demonstrated. The lengthy case inpatient stays indicated a severe neurological illness with diagnostic procedures consistent with NMS, and the incidence of complications such as rhabdomyolysis was similar to that reported in a national inpatient sample study of this syndrome (Modi et al., 2016). Finally, every case occurred during antipsychotic use, satisfying the criterion for recent exposure to a dopamine antagonist (Wijdicks, 2023). Nevertheless, residual misclassification, if nondifferential, would attenuate the association of patient and treatment characteristics with this syndrome.
However, cases of NMS may have been misdiagnosed and thus not included in the analysis. Although NMS is a severe disorder that is likely to lead to hospitalization, diagnosis is clinically based and the syndrome may be mistaken for many drug-related and other conditions such as malignant catatonia, malignant hyperthermia, serotonin syndrome, seizures, or infections (Berloffa et al., 2021, Duhan et al., 2023, Wijdicks, 2023). Consequently, the study estimates of NMS incidence in children and youth may be too low and thus understate the clinical impact of this antipsychotic adverse effect.
Second, the study’s neuropsychiatric disorders were defined from Medicaid claims. Although claims data can reliably identify the broad study diagnostic categories (Hartung et al., 2013, Lurie et al., 1992, Shea et al., 2024, Straub et al., 2021), their capacity to provide additional detail on important characteristics of the disorders that potentially could better identify patients with high risk of NMS—such as subtype, etiology, and severity—is uncertain.
Third, the number of NMS cases was limited. Thus, we could not perform more detailed analyses of various clinical subgroups of interest, particularly since privacy safeguards prohibited reporting of table cells with fewer than 11 cases. Similarly, we could not conduct exploratory analyses of several other potential correlates of NMS suggested by adult studies (Berardi et al., 1998, Berman, 2011, Funayama et al., 2018, Nielsen et al., 2012, Su et al., 2014, Wijdicks, 2023). Consequently, we focused on patient demographics, neuropsychiatric diagnoses, and antipsychotic treatment characteristics that are readily available to practitioners and plausibly could identify patients with increased NMS risk for whom more intense monitoring could be appropriate.
Fourth, the most recent study data were from 2013, as the availability and quality of more recent data were influenced by a major transition in state Medicaid reporting requirements (anon, 2023a, anon, 2023b). However, although antipsychotic prescribing for younger populations is decreasing (Bushnell et al., 2023), risperidone, aripiprazole, and quetiapine still are the most frequently prescribed drugs for children and youth (Hsueh et al., 2023), and haloperidol continues to be prescribed in pediatric patients (Nash et al., 2023). Furthermore, findings did not change in a sensitivity analysis that was restricted to the 5 most recent calendar years. Thus, the study findings should be applicable to contemporary practice.
Fifth, cohort members were all Medicaid beneficiaries, which limits generalizability. Nevertheless, the national Medicaid population is important per se, as this program provides health insurance coverage for an estimated 36% of U.S. children (Keisler-Starkey and Bunch, 2022), who have elevated prevalence of antipsychotic use (Edelsohn et al., 2017). Because study data were from prior to the Affordable Care Act Medicaid expansions in 2014 (Fung et al., 2022), Medicaid eligibility criteria were more restrictive for cohort members 18–24 years than for children, which would further limit generalizability for young adults.
Conclusion
In children and youth treated with antipsychotics, the following five factors independently identified patients with increased NMS incidence: age 18–24 years, schizophrenia spectrum and other psychotic disorders, neurodevelopmental disorders, first-generation drugs, and antipsychotic doses greater than 200 mg chlorpromazine-equivalents. Patients with 4 or 5 of these factors had more than 100 times the incidence of those with none. These findings could improve early identification of children and youth with elevated NMS risk, potentially leading to earlier detection and improved outcomes.
Footnotes
Clinical Significance
Practitioners who prescribe antipsychotics for children and youth, particularly for those with schizophrenia spectrum and other psychotic disorders, autism spectrum disorders, and intellectual disability, should be alert for signs and symptoms of neuroleptic malignant syndrome. Study findings strengthen recommendations to avoid limit or avoid, when possible, treatment of children and youth with FGAs, particularly haloperidol.
Authors’ Contributions
Concept and design: Ray, Fuchs, Olfson, Cooper. Acquisition, analysis, or interpretation of data: Ray, Fuchs, Olfson, Stein, Murray, Daugherty, Cooper. Drafting of the manuscript: Ray, Fuchs, Olfson, Daugherty. Critical review of the manuscript for important intellectual content: Ray, Fuchs, Olfson, Stein, Murray, Cooper. Statistical analysis: Ray. Obtained funding: Ray, Murray. Administrative, technical, or material support: Daugherty, Cooper. Supervision: Ray.
Disclosures
The authors disclose that the only financial affiliation is with Grant HD097344 from the National Institute for Child Health and Human Development, which funded the study. The sponsor had no role in study design or conduct. The authors have no other relevant commercial or financial relationships.
Data Availability Statement
Supplementary Material
Supplementary Figure SA1
Supplementary Figure SA2
Supplementary Figure SA3
Supplementary Appendix S1
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4
Supplementary Table SA1
Supplementary Table SA2
Supplementary Table SA3
Supplementary Table SA4
Supplementary Table SA5
Supplementary Table SA6
Supplementary Table SA7
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.