
Abstract
Objectives:
Long-acting injectable (LAI) antipsychotic medications are being prescribed to children and adolescents along a broad age range from 2 to 17 years old. However, there is no U.S. Food and Drug Administration (FDA) approved indication for the use of any LAI in a pediatric population. The goal of this article is to perform a systematic literature review regarding the use of LAIs in a pediatric population, to obtain pediatric LAI safety data, and to survey prescriber attitudes regarding LAI use in youth.
Methods:
A search for relevant articles between June 1986 and June 2021 was conducted. Safety data were obtained from FDA MedWatch postmarketing adverse event reports regarding LAI use in children and adolescents. A survey of practicing Child and Adolescent Psychiatrists in Wisconsin was done regarding the use of LAIs in youth.
Results:
The predominant reasons for LAI use in youth were illness severity and treatment noncompliance. Twenty-six of 30 identified studies and reports favored LAI use in youth, but were of low to very low quality. Overall, 587 FDA MedWatch reports between June 1986 and June 2021 were identified. Most adverse events occurred in modest numbers. Extrapyramidal symptoms accounted for 18% of all MedWatch reports, neuroleptic malignant syndrome accounted for 3% of all reports, and deaths accounted for 2% of all reports. The concern for safety was reflected in prescriber survey results along with a recognition that LAIs can be helpful to target severe psychiatric symptoms and address treatment noncompliance.
Conclusions:
No randomized controlled studies were found. Identified published studies and reports were of low to very low quality. However, it appeared reasonable that the use of LAIs in a select group of pediatric patients can be helpful to target severe psychiatric symptoms and to enhance treatment compliance.
Introduction
In adults, the use of a long-acting injectable (LAI) antipsychotic medication is common and effective in terms of reduced hospital inpatient stays and reduced emergency department visits for chief complaint of psychiatric emergency (Lin et al., 2021). Other advantages of the use of LAI in adults are to maintain an even and steady blood level of antipsychotic medication, to enhance compliance by eliminating daily pill taking, to avoid misuse and/or overdose of medication, and patients often prefer the convenience of an LAI (Kane and Correll, 2017). By extension, there is then reason to believe that the use of LAIs in youth (those individuals under 18 years old) may result in similar advantages. Published utilization studies reveal that LAIs are being prescribed to children and adolescents along a broad age range from 2 to 17 years old (Benarous et al., 2023; Modesitt et al., 2018). Several published reviews focusing on the use of LAIs in youth concluded that, although there were no randomized controlled clinical trials and those studies that were identified as relevant were of low sample size and low quality, the use of LAIs could be helpful in young patients with severe mental illness and treatment noncompliance (Baeza et al., 2023; Benarous et al., 2022; Lytle et al., 2017). However, there is no U.S. Food and Drug Administration (FDA) approved indication for the use of any LAI in a pediatric population. Further, there is a lack of safety data regarding the use of any LAI in children and adolescents, as well as very little guidance in the medical literature on how to use an LAI in a pediatric patient, and no recommended process to obtain appropriate informed consent and assent for a medical procedure that is invasive and lacking basic preclinical studies such as dose finding and pharmacokinetics.
The goal of this article is to perform a systematic review of the literature regarding the use of LAIs in a pediatric population augmenting with reports from the FDA MedWatch postmarketing adverse event reporting system along with survey results from practicing Child and Adolescent Psychiatrists in Wisconsin regarding their views of LAI use in youth. This systematic review is a comprehensive assessment of the use of LAIs in youth that includes as much safety data as could be located.
The systematic literature review and the human subjects research components were part of a study protocol approved by the Mendota Mental Health Institute Institutional Review Board, Madison, Wisconsin.
Methods
The design of the review was a systematic search of data contained in published studies and reports on the use of LAIs in a pediatric population. The search and data collection were accomplished according to standard guidelines (Higgins et al., 2022; Shamseer et al., 2022). Beyond accomplishing a systematic review, attitudes regarding the use of LAIs in youth from surveyed practicing Child and Adolescent Psychiatrists in Wisconsin were included. Further, to capture as much safety information as possible, data from the FDA MedWatch postmarketing adverse event reporting system regarding LAIs in a pediatric population were obtained.
Systematic review
The literature search was restricted to English language sources from June 1986 to June 2021. The start date of June 1986 was chosen because it was the date of introduction of haloperidol decanoate into the U.S. market (Haldol Decanoate, Package Insert, November 2020, Janssen Pharmaceuticals). A medical librarian (R.S.) conducted the electronic search. Databases searched were Ovid MedLine, PsychINFO, Scopus, and Web of Science for all available sources regarding the use of LAIs in youth. Keyword pairing using the general phrase, “long-acting injectable antipsychotic” and “child,” “adolescent,” and “youth” was done along with the generic and trade names of the at the time available LAIs: aripiprazole monohydrate and aripiprazole lauroxil (Abilify Maintena and Aristada), fluphenazine decanoate (Prolixin Decanoate), haloperidol decanoate (Haldol Decanoate), olanzapine pamoate (Zyprexa Relprevv), paliperidone palmitate (Invega Sustenna and Invega Trinza), and risperidone microspheres (Risperdal Consta). Inclusion criteria: any clinical trial involving the use of LAI in youth; any case report or case series of LAI use in youth; any reviews focusing on the use of LAI in youth (to hand search the reference list). Prescription utilization studies of LAI in youth were obtained for background information. Exclusion criteria: studies and reports with both pediatric and adult data, where pediatric data could not be separated; studies and reports that only included adults; and studies and reports within a pediatric population involving only oral antipsychotic medication.
Included studies and reports were divided into two groups: quantitative and qualitative. The quantitative group was those studies and reports that contained any numerical data amenable to statistical analysis, specifically the Clinical Global Impressions-Severity (CGI-S) Scale at baseline and end-of-trial (Guy, 2000). The qualitative group was those studies and reports that contain only descriptive results and not amenable to statistical analysis.
The principal investigator (A.M.S.) screened the titles and abstracts of those electronic database search results for articles that fit the inclusion criteria. In those cases, in which the title and abstract were unclear if children and/or adolescents were the focus of the report or study, the methods section was examined for age range. To identify additional articles that fit inclusion criteria, the reference lists of reports, studies, and review articles were hand-searched. A Google search was also done to capture any further articles appropriate for inclusion.
Survey of Wisconsin practicing child and adolescent psychiatrists
The email addresses of 160 practicing Child and Adolescent Psychiatrists in Wisconsin were obtained from the American Academy of Child and Adolescent Psychiatry-Wisconsin Branch Listserv. SurveyMonkey (San Mateo, California, USA, www.surveymonkey.com), an internet-based email survey tool, was utilized to contact those 160 psychiatrists. The following 10 survey questions were used: Are you aware that long-acting injectable antipsychotic medications are used in youth? [yes/no] Have you ever prescribed a long-acting injectable antipsychotic medication to a patient under 18 years old? [yes/no] Do you have any safety concerns regarding the use of long-acting injectable antipsychotic medication in youth? [yes/no] What are your concerns? [open-ended free text field]
Would a reason to use a long-acting injectable antipsychotic medication be (please respond to each item): To maintain even and steady blood level of antipsychotic medication? [yes/no] To specifically target the symptoms of a serious mental illness, such as early-onset schizophrenia or early-onset bipolar disorder? [yes/no] To specifically target severe aggressive and disruptive behaviors (nonautism)? [yes/no] To specifically target severe aggression and disruptive behaviors in the context of autism? [yes/no] To avoid misuse/overdose of antipsychotic medication? [yes/no] To address antipsychotic medication noncompliance? [yes/no]
SurveyMonkey responses were completely anonymous.
FDA MedWatch reports
In an effort to obtain whatever safety data might be available, a Freedom of Information Act (FOIA) request was made with the FDA for all MedWatch postmarketing adverse event reports involving the use of an LAI in youth between June 1986 and June 2021. The following items were abstracted from each report: LAI used; adverse event(s), age, sex, and outcome (death, disability, hospitalization, life threatening, and other serious medical event that required intervention to prevent impairment/damage).
Statistical analysis
Simple summary statistics were applied. For those studies and reports that contained usable CGI-S data, the pooled average and standard deviation were calculated for baseline and at the end-of-trial. A paired t-test was done to determine statistical significance between baseline and end-of-trial groups. Effect size (Cohen’s d) was also calculated.
Results
Systematic review
The electronic database search yielded 647 articles. Based on inclusion criteria, 22 relevant articles were eligible for evaluation. An additional 13 articles were identified by hand review of reference lists. See Figure 1 for the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram. Two studies (Petric et al., 2019; Ruan et al., 2010) that contained patients who were 18 years old were included, since by examination of age means and standard deviations, the majority of study patients were under 18 years old. Three articles outside of the June 1986 to June 2021 timeframe were included for further analysis: one case series (Perinpanayagam and Haig, 1977) along with one case report (Zaydlin et al., 2023) and one retrospective chart review (Moon et al., 2023). Four reviews were found including two reviews published in 2023 (Baeza et al., 2023; Benarous et al., 2022; Janssen Science, 2023; Lytle et al., 2017). Two LAI prescription utilization studies were found that focused on children and adolescents (Benarous et al., 2023; Modesitt et al., 2018). No randomized controlled studies were found. In total, 30 articles comprised 15 case reports, 4 case series, 4 open-label prospective observational studies, and 7 retrospective chart reviews were determined to be eligible for analysis. Those eligible articles represented a total of 277 individuals (138 males and 139 females) with an age range of 5–17 years old (along with a few individuals who were 18 years old, as stated above). Race and ethnicity were indicated in only five articles representing 17 patients.
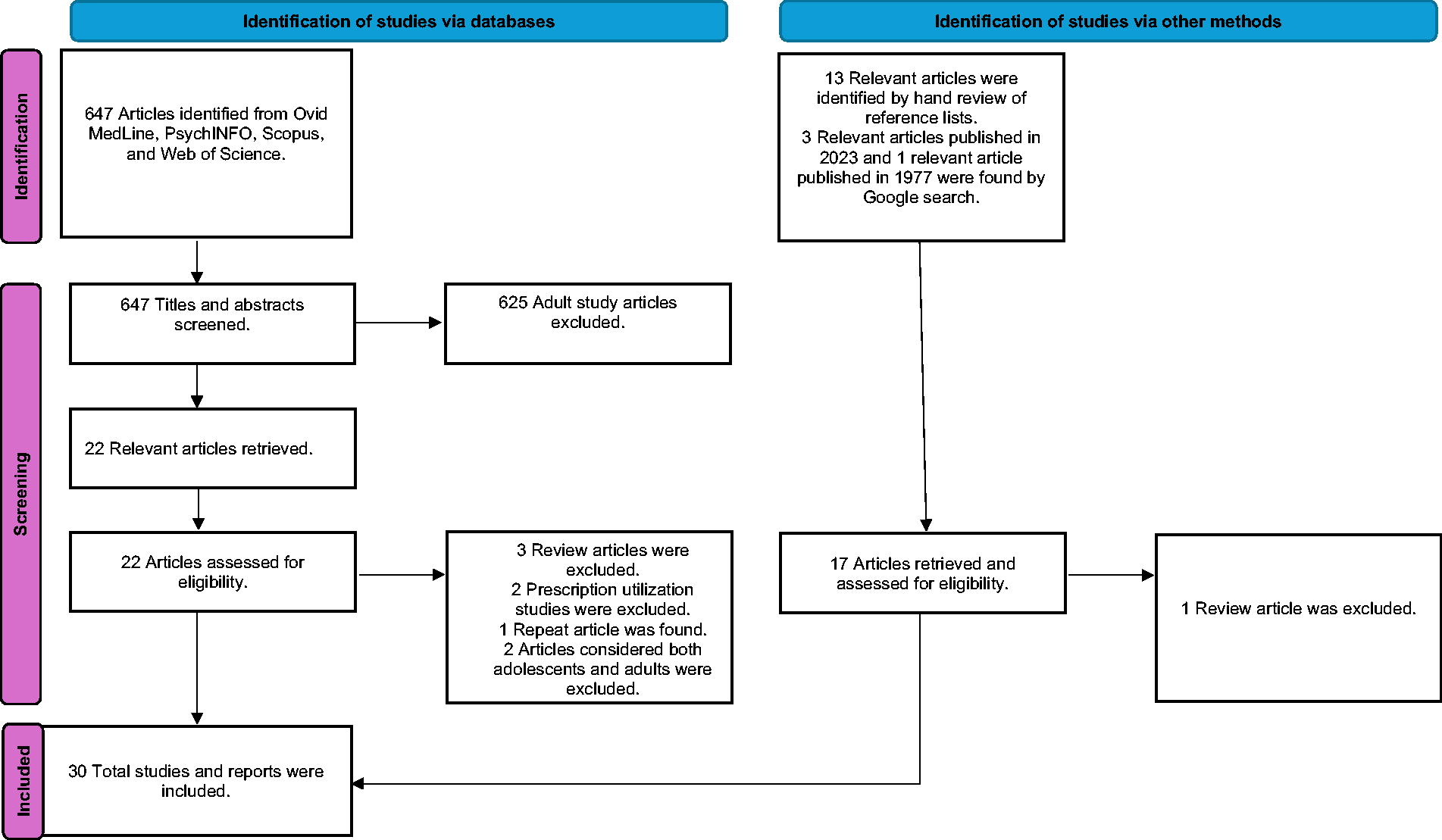
PRISMA flow diagram.
Fourteen studies and reports contained quantitative data (see Table 1). Nine of those 14 studies and reports possessed usable CGI-S baseline and end-of-trial data for further statistical analysis. The overall CGI-S average at baseline was 6 (severely ill), and the overall CGI-S average at end-of-trial was 2 (borderline mentally ill). The paired t-test showed that the improvement in symptoms was highly significant with p < 0.0001. The calculated effect size (Cohen’s d) was exceedingly robust at 7.2. However, significance was lost when treatment trial duration was considered. Although the remainder of those studies and reports in Table 1 contained quantitative data because of the heterogeneity of the measures used, no meaningful statistical analysis could be done. Essentially all studies and reports in Table 1 showed a beneficial effect of LAI use.
Quantitative Studies/Reports
Simple statistics were done only for those studies that provided CGI-S baseline and CGI-S end-of-trial data, either group average or single data points for a single case.
Of 42 total patients, 6 patients had one disorder, 30 patients had two disorders, and 6 patients had three disorders.
Unclear if aripiprazole monohydrate or aripiprazole lauroxil.
BMI, body mass index; BPRS, Brief Psychiatric Rating Scale; CGAS, Children’s Global Assessment Scale; CGI-S, Clinical Global Impressions-Severity; EPS, extrapyramidal symptoms; LAI, long-acting injectable antipsychotic medication; n, number of patients; PANSS, Positive and Negative Syndrome Scale; YMRS, Young Mania Rating Scale.
Sixteen studies and reports contained results in descriptive or qualitative form (see Table 2). Four of those 16 were case reports of specific adverse events related to an LAI (Erermis et al., 2007; Mirza et al., 2018; Patel et al., 2013; Solfanelli et al., 2013). Of those remaining 12 studies and reports, 2 did not indicate any result of LAI use, while 10 indicated some degree of symptom improvement.
Qualitative Studies/Reports
Unclear if aripiprazole monohydrate or aripiprazole lauroxil.
CGI-I, Clinical Global Impressions-Improvement; CK, creatine kinase; EPS, extrapyramidal symptoms; LAI, long-acting injectable antipsychotic medication; n, number of patients.
Considering the 30 studies and reports in Tables 1 and 2, apart from those four case reports in Table 2 which specifically cited an adverse event related to an LAI, safety data were sparse with 10 studies and reports citing no adverse events. Only 14 of the 30 studies and reports explicitly obtained consent for the use of an LAI in a minor. Along with the severity of illness, noncompliance was the most common factor necessitating LAI use.
Survey of practicing child and adolescent psychiatrists in Wisconsin
Of 160 email survey invitations, 19 responses were received (12% return). Although the return was low, those responses provided insight from practitioners regarding the use of LAIs in youth. Of those who responded, 95% were aware that LAIs are being used in children and adolescents; 63% had prescribed an LAI to a patient under 18 years old; 68% had safety concerns regarding the use of LAI in youth; 89% agreed that a reason to use an LAI would be to maintain an even and steady blood level of antipsychotic medication; 100% agreed that a reason to use an LAI would be to target symptoms of early-onset schizophrenia or early-onset bipolar disorder; 68% agreed that a reason to use an LAI would be to target severe aggression and disruptive behaviors; 63% agreed that a reason to use an LAI would be to target severe aggression and disruptive behaviors in the context of autism; 74% agreed that a reason to use an LAI would be to avoid misuse/overdose of antipsychotic medication; and 100% agreed that a reason to use an LAI would be to address antipsychotic medication noncompliance. Table 3 lists some of the subjective survey-derived practitioner’s concerns regarding LAI use in youth.
Selected Survey-Derived Practitioner’s Concerns Regarding the Use of Long-Acting Injectable Antipsychotic Medications in Youth
FDA, U.S. Food and Drug Administration; LAI, long-acting injectable antipsychotic medication; PO, by mouth.
FDA MedWatch reports
The FOIA request yielded 589 individual reports representing 589 pediatric patients who received an LAI and who experienced an adverse event(s) that was subsequently reported. Many of those 589 MedWatch reports were inconsistent in that some individual reports indicated one adverse event while the majority listed multiple adverse events ranging from a few to over 30. Some of the listed adverse events were challenging to categorize or define in the context of LAI use (examples include victim of child abuse, nerve injury, attention-seeking behavior, cyst, eructation, shunt malformation, and benign neoplasm of scrotum). In MedWatch reports containing multiple adverse events, those adverse events were edited and condensed to conform to previously published sources that focused on the safety and tolerability of antipsychotic medications (Correll, 2008; Stroup and Gray, 2018). Two of those 589 MedWatch reports were excluded as each described adverse events within a newborn secondary to LAI prescribed to the mother.
The majority of adverse events occurred in relatively modest numbers, but extrapyramidal symptoms were common in all LAIs considered with more than one MedWatch report. It was noteworthy that three deaths each were reported with aripiprazole lauroxil, aripiprazole monohydrate, and haloperidol decanoate, and four deaths were reported with risperidone microspheres. There were 3 reports of neuroleptic malignant syndrome with aripiprazole lauroxil, 2 reports each with aripiprazole monohydrate and with haloperidol decanoate, and 11 reports with risperidone microspheres. Table 4 displays the collected edited adverse events from 587 MedWatch reports. Also abstracted from those 587 MedWatch reports were individual patient outcomes that were serious in nature (see Table 5).
Adverse Events from 587 MedWatch Reports
In five reports, sex was not indicated.
Individual Patient Outcomes by MedWatch Reports—Serious Outcomes
LAI, long-acting injectable antipsychotic medication.
Discussion
Safety is a fundamental priority in clinical drug development. Phase 1 preclinical trials are done to assess the safety and tolerability of an investigational drug by characterizing the dose-limiting adverse reactions, identifying the maximum safe dose, determining the pharmacokinetics, and understanding the metabolism and interactions of the investigational drug (Naseer, S. Safety Considerations in Clinical Drug Development. FDA Clinical Investigator Training Course 2023, December 6, 2023). None of these preclinical studies have been published in the context of LAI use in a pediatric population. Because there is no FDA-approved indication for the use of any LAI in a pediatric population, the use of an LAI in a young person is termed off-label.
The systematic review presented here shows that LAIs are being used in youth to target severe psychiatric symptoms and treatment noncompliance with the great majority of those studies and reports indicating some degree of symptom improvement to the point of remarkable statistical significance in favor of LAI use. However, of the 30 studies and reports listed in Tables 1 and 2, except for four case reports that each focused on a specific adverse event (see Table 2), those resultant 26 studies and reports suffered from very low sample sizes, absence of randomization/control, heterogeneity or omission of a valid assessment tool, variable lengths of treatment, and selection bias. Those 26 studies and reports were judged as possessing low to very low quality.
Of further concern was the sparse safety data contained in those resultant 26 studies and reports that indicated some degree of symptom improvement. Concern over safety was reflected in the survey responses from practicing Wisconsin Child and Adolescent Psychiatrists along with a recognition that LAI use in youth can be helpful to target serious mental illness and medication noncompliance. FDA MedWatch reports were obtained to provide a window into the range of possible adverse events with the use of LAIs in youth. Although the majority of reported adverse events occurred in relatively modest numbers, a very wide range of adverse events were listed in most MedWatch reports indicating a need for safety studies that are more systematic and better defined. Remarkably, for LAI use in children and adolescents, a medical procedure that is off-label and invasive with sparse safety data, only 14 of the 30 studies and reports (47%) explicitly obtained consent for the use of an LAI in a minor.
Safety is a fundamental priority not only in clinical drug development, but in daily clinical practice. Although the lack of a sufficient evidence base and the lack of any published clinical guidance likely discourages LAI use in youth, it appears reasonable that the use of LAIs in a select group of pediatric patients can be helpful to target severe psychiatric symptoms and to enhance treatment compliance. The off-label use of medications is frequently appropriate and can be accomplished in an ethical manner for the benefit of a particular patient (Dell et al., 2011).
In terms of future research, pharmacokinetic and pharmacoepidemiologic studies may be less complicated to accomplish. A randomized clinical trial is the gold standard, but such a study of LAI use in youth would need to be multisite to achieve adequate statistical power and would be costly to conduct. Given that LAIs are already being used in a pediatric population, real-world data from treatment in mental health care systems could be collected, analyzed, and produce high-quality data that would fit-for-purpose the research questions regarding the effectiveness and safety of LAI use in youth (National Academies of Sciences, Engineering, and Medicine, 2019).
Limitations
The main limitation of this study is the lack of controlled clinical trials with high-quality data. Other limitations include the low response rate from surveyed practicing Wisconsin Child and Adolescent Psychiatrists and the often-perplexing number and kinds of adverse events contained in many of the FDA MedWatch reports. Therefore, the results must be interpreted with some caution.
Conclusions
Taking together the results and the limitations of this study, the balance of the evidence suggests that the use of LAIs in a subset of pediatric patients can be helpful to target severe psychiatric symptoms complicated by treatment noncompliance. No specific LAI could be determined as superior to any other and neither could an absolute lower age limit be determined for the exclusion of LAI use.
Clinical Significance
The use of LAIs in a select group of pediatric patients could be an important treatment modality that can potentially reduce hospital inpatient stays, minimize emergency department visits for chief complaint of psychiatric emergency, and better maintain complex patients in their community. Currently, there is no published practice parameter or clinical pathway to guide a clinician considering the use of an LAI in a young person with a serious mental illness. The systematic review presented here can be part of a foundation for the development of a clinical pathway for LAI use in youth that is consistent, ethically based, and as safe as possible.
Footnotes
Disclosures
The authors have no conflicts of interest to report.
Authors’ Contributions
A.M.S. conceived the study, authored the study protocol, obtained FDA MedWatch reports, conducted the online survey, and was responsible for all data collection. R.S. contributed to the literature search design, conducted the literature search, and curated the literature search results. A.M.S. and S.J.M. preformed data analysis and interpretation and wrote the manuscript. All authors read and approved the final manuscript. All authors had full access to all those data in the study and had final decision authority to submit for publication.