
Abstract
We present the case of a 16-year-old male with autism spectrum disorder, mood disorder, and psychotic symptoms who was admitted to Winnebago Mental Health Institute (WMHI), a State of Wisconsin psychiatric facility, on a 72-hour involuntary legal hold for aggression and hearing voices.
In February 2023, our patient began hearing voices to burn down the family home. Our patient was hospitalized April 2023 for 9 days, started on olanzapine, and his psychotic symptoms did ameliorate. However, he required rehospitalization in May 2023 for refusing prescribed olanzapine with resultant psychotic symptoms and poor sleep. Olanzapine was restarted, but he declined the olanzapine, and was discharged. Back home, his symptoms worsened with increased auditory hallucinations, physical aggression, not sleeping, and making persistent efforts to burn down the family home.
At WMHI, he consistently declined oral olanzapine until a Probable Cause Hearing held 3 days after admission issued an order for involuntary medication administration. Oral olanzapine was then restarted at 5 mg at bedtime along with intramuscular (IM) immediate release 5 mg olanzapine back-up. One-week later, olanzapine was increased to 5 mg twice daily. Our patient maintained that the oral olanzapine, “It’s bad for me…makes me hear voices,” and he explained that with IM olanzapine he does not hear any voices. He neither accepted crushed olanzapine in food nor did he accept the oral disintegrating tablet (ODT) form of olanzapine. Our patient was very pleased with receiving olanzapine 5 mg IM twice daily, but this greatly limited posthospital medication management. His parents and our patient’s outpatient medication provider agreed with the use of the long-acting injectable (LAI) aripiprazole lauroxil. Specific informed consent was obtained from the parents after a detailed discussion of the advantages and disadvantages of LAI use and alternative treatments.
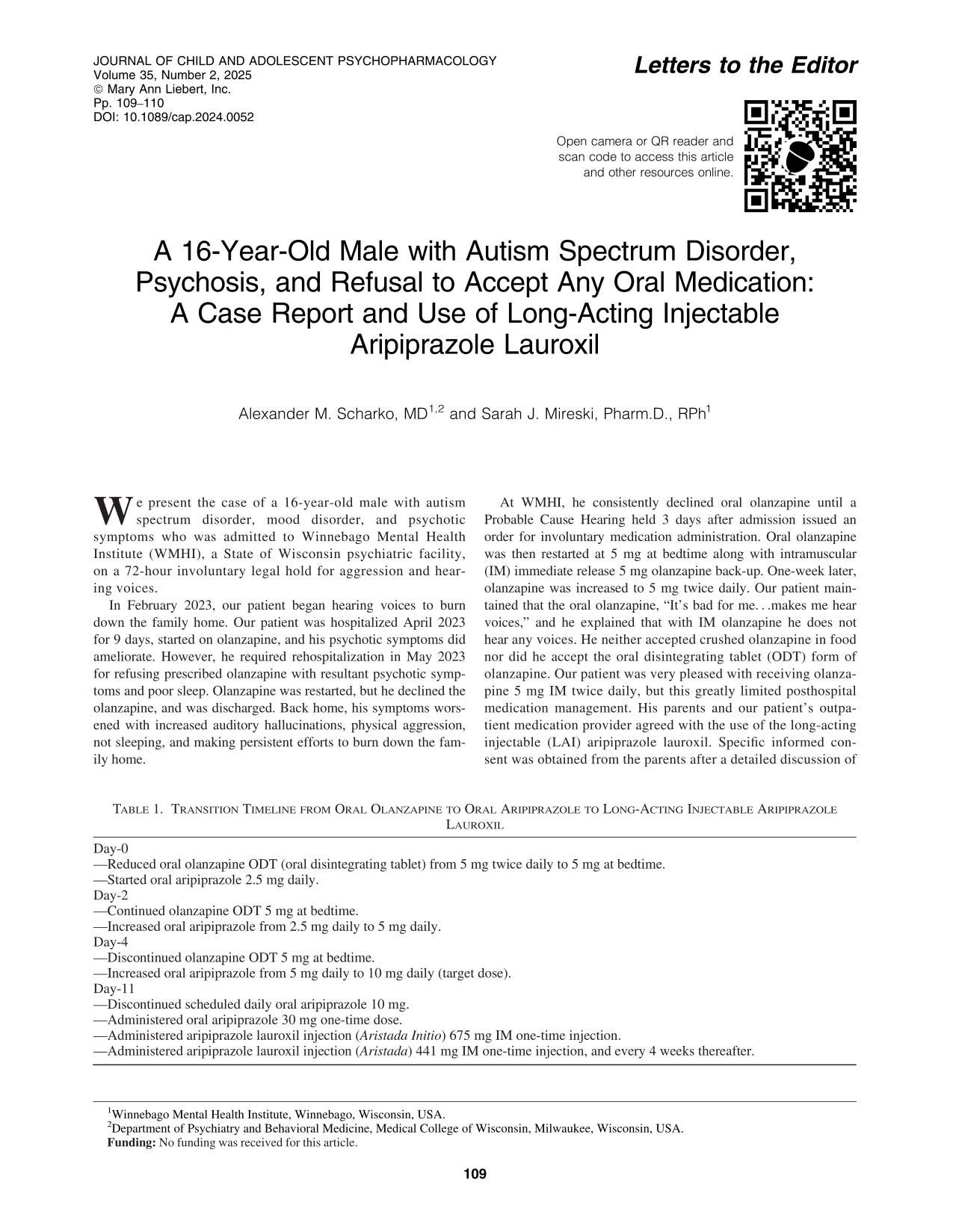
A calendar was constructed that showed the cross-titration from oral olanzapine to oral aripiprazole until administration of LAI aripiprazole lauroxil and discharge to home. Our patient then accepted oral aripiprazole and olanzapine ODT in the cross-titration process. Our patient tolerated oral aripiprazole well with good sleep and no reactivation of psychotic symptoms. Table 1 shows the medication transition timeline as recommended by WMHI Pharmacy.
Transition Timeline from Oral Olanzapine to Oral Aripiprazole to Long-Acting Injectable Aripiprazole Lauroxil
LAIs are being prescribed to children and adolescents along a broad age range 2–17 years old (Modesitt et al., 2018). However, there is no U.S. Food and Drug Administration indication for the use of LAIs in youth. The use of any LAI in youth is then, off-label. Although the lack of sufficient data regarding the use of LAIs in young patients is a major complicating factor, off-label use of medications is frequently appropriate and can be accomplished in an ethical manner for the benefit of a particular patient (Dell et al., 2011).
A draft of this case report was provided to our patient’s family. The parent then gave written consent for the publication of this case report.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interests to report.