
Abstract
Objectives:
To assess quality of life and outcomes associated with adverse effects (AEs) in pediatric patients receiving pharmacological treatment for attention-deficit/hyperactivity disorder (ADHD) and their parents/caregivers.
Methods:
An online survey was conducted (10/13/2023–10/20/2023) among parents/caregivers recruited from Dynata’s U.S. panel who lived with a pediatric patient (6–17 years) currently treated for ADHD. Patient and parent/caregiver characteristics and outcomes were descriptively reported. Patients were considered to have AEs if they experienced symptoms/complications in the past 30 days that appeared, worsened, or remained unchanged after initiating their latest ADHD treatment. Regression analyses were used to estimate correlations between the number of AEs and key outcomes, including patients’ health-related quality of life (HRQoL; based on the Pediatric Quality of Life Inventory) and parents/caregivers’ work and activity impairments (based on Work Productivity and Activity Impairment: Caregiver) and mental health (based on Patient Health Questionnaire-4).
Results:
A total of 401 parents/caregivers from all U.S. regions completed the survey (caregiver median age: 38 years, 58.9% female; patient median age: 11 years; 37.7% female). In the 30 days prior to data collection, 66.8% of patients had AEs (overall mean: 1.2 AEs), with insomnia/sleep disturbances and decreased appetite/weight loss being the most frequently reported (14.2% and 11.7%, respectively). The number of AEs was significantly correlated with reduced patient’s HRQoL (including reduced physical, emotional, and school functioning), increased parent/caregiver’s work and activity impairment, and a higher likelihood of parents/caregivers having generalized anxiety disorder or major depressive disorder, respectively (all p < 0.001).
Conclusions:
AEs are common among pediatric patients receiving pharmacological treatment for ADHD and are associated with poorer quality of life and outcomes in pediatric patients and their parents/caregivers. Therapies with better safety profiles may help improve patient’s HRQoL and parent/caregiver outcomes.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders of childhood (Faraone et al., 2015). Pharmacological options for treating children and adolescents with ADHD include stimulants (e.g., methylphenidate and amphetamine) and nonstimulants (e.g., atomoxetine, viloxazine extended-release, and α2-agonists) (Singh et al., 2022; Wolraich et al., 2019).
While pharmacological treatments for ADHD have demonstrated clinical benefits in terms of efficacy (Cortese et al., 2018), they are associated with a range of adverse effects (AEs), frequently including sleep disturbances, decreased appetite, and mood lability (Felt et al., 2014; Reed et al., 2016; Storebo et al., 2023). These AEs may negatively affect the daily functioning and quality of life of pediatric patients and their caregivers; for instance, sleep problems among adolescents with ADHD have been associated with reduced concentration and academic problems (Becker et al., 2019; Nelson et al., 2022). Meanwhile, caregivers of school-aged children with ADHD and moderate or severe sleep problems have reported more stress than those with children with ADHD but without sleep problems (Sung et al., 2008).
Prior studies have suggested that safety concerns or issues relating to ADHD treatments are common reasons for nonadherence and treatment discontinuation (Gajria et al., 2014; Schein et al., 2022d, Sondergaard et al., 2024). While these studies have shed light on how ADHD AEs may affect patients’ medication-taking behaviors and treatment changes, the impact of AEs on the overall well-being of pediatric patients is less clear. In addition, parents/caregivers living with children with ADHD are subject to increased parental stress, emotional burden, and disrupted daily life (Johnston and Mash, 2001; Laugesen et al., 2016); however, studies associating these parent/caregiver burdens with their children’s ADHD treatment experience, particularly in relation to AEs, are scarce.
Additional information on how AEs may affect the daily functioning and well-being of pediatric patients with ADHD and their parents/caregivers may help inform management strategies to improve their experience and outcomes during the treatment journey. To this end, we conducted a survey among parents/caregivers living with pediatric patients with ADHD to describe AEs experienced by pediatric patients receiving pharmacological treatments for ADHD and to assess the association of these AEs with patients’ health-related quality of life (HRQoL) and their parents/caregivers’ work productivity, everyday functioning, as well as mental health.
Methods
Study design
An online survey was conducted from 10/13/2023 to 10/20/2023 among parents/caregivers of pediatric patients with ADHD living in the United States, recruited through an existing panel of geographically and demographically diverse individuals from a well-established market research firm, Dynata. The survey began with a screening section that included an informed consent form followed by questions on parent/caregiver and patient characteristics and outcomes. Prior to data collection, pilot tests were conducted with eligible parent/caregiver participants in the form of semi-structured virtual interviews, and questions were refined as needed. This study was approved under the exemption category by the Western Copernicus Group Institutional Review Board prior to data collection.
Study population and cohorts
Eligible parent/caregiver participants were ≥18 years old, residing in the United States, and at minimum somewhat comfortable reading and understanding English. Participants were required to live with a child under the age of 18 years old who had been diagnosed with ADHD and who was treated with a prescription medication approved for ADHD by the U.S. Food and Drug Administration at the time of data collection.
Participants were classified into the following two mutually exclusive cohorts based on whether their child with ADHD (i.e., the patient) experienced AEs in the past 30 days. Specifically, the patients with AEs cohort included those who experienced symptoms/complications in the past 30 days that appeared, worsened, or remained unchanged after initiating their latest ADHD treatment; while the patients without AEs cohort included those who did not experience any symptoms/complications in the past 30 days. Patients experiencing symptoms/complications in the past 30 days that existed prior to the initiation of their latest ADHD treatment but improved while on treatment and did not have any other symptoms that appeared, worsened, or remained unchanged after the initiation of their latest ADHD treatment were not included in any of the cohorts.
Measures and outcomes
Information collected in the survey included parent/caregiver and patient characteristics and outcomes (e.g., demographics, patient clinical and treatment characteristics, health care resource utilization [HRU] in the past year), parent/caregiver-reported adherence and satisfaction with their child’s ADHD treatment, patient experience of AEs, and parent/caregiver-perceived impact of selected AEs. The survey also included several validated instruments to assess patients’ and parents/caregivers’ functioning and outcomes.
More specifically, the perceived impact of selected AEs on the child’s and parent/caregiver’s overall well-being in the past 30 days was assessed. These selected AEs included insomnia and other sleep disturbances, decreased appetite/weight loss, emotional impulsivity/mood lability, anxiety/panic attacks, depression, fatigue/somnolence, and gastro-intestinal symptoms (abdominal pain, nausea/vomiting), which were selected based on clinical input and how commonly they are associated with ADHD treatments in the literature (Felt et al., 2014; Mechler et al., 2022; Wolraich et al., 2019). The impact of these selected AEs was self-reported by parents/caregivers based on the following Likert scale: not at all, a little, somewhat, a lot, and extremely.
Patients’ HRQoL was assessed using the Pediatric Quality of Life Inventory (PedsQL), completed by parents/caregivers. The PedsQL is composed of physical functioning and psychosocial health (including emotional, social, and school functioning) components and has a total score range of 0–100; higher scores indicate better HRQoL (Varni et al., 2003; Varni et al., 2007). Parents/caregivers’ work and activity impairment was assessed using the Work Productivity and Activity Impairment: Caregiver (WPAI-CG) questionnaire (score range: 0%–100%; higher percentages indicate worse impairment) (Reilly Associates, 2019), and their mental health was assessed using the Patient Health Questionnaire-4 (PHQ-4) (Kroenke et al., 2009); specifically, PHQ-4 comprises the Generalized Anxiety Disorder-2 (GAD-2) subscale for assessing generalized anxiety disorder (GAD) (score range: 0–6 points; ≥3 indicates high likelihood of GAD) (Kroenke et al., 2007) and the PHQ-2 subscale for assessing major depressive disorder (MDD; score range: 0–6 points; ≥3 indicates high likelihood of MDD) (Kroenke et al., 2003).
Statistical analyses
Information on parent/caregiver and patient characteristics and outcomes collected in the survey was reported descriptively overall and by cohort. Means, medians, and standard deviations were reported for continuous variables; frequency counts and percentages were reported for categorical variables. Standardized differences were also reported; a standardized difference of >20% was considered to indicate a meaningful difference between the cohorts (Austin, 2009; Cohen, 1992).
Regression analyses were conducted to estimate the association between the number of AEs in the past 30 days and key outcomes. For binary outcomes (i.e., parents/caregivers having a high likelihood of GAD and MDD, respectively), odds ratios for each additional AE in the past 30 days were estimated using logistic regression models. For continuous variables (i.e., variables measured in PedsQL and WPAI-CG), differences in outcome for each additional AE in the past 30 days were estimated using ordinary least squares regressions. Regressions were adjusted for the following patient and parent/caregiver characteristics: patient gender, patient race/ethnicity, patient age, age at diagnosis, prior pharmacological treatment, parent/caregiver gender, parent/caregiver age, parent/caregiver education level, household situation, number of children in the household, and region of residence.
Results
Sample size
A total of 401 eligible parents/caregivers completed the survey, including 101 (25.2%) parents/caregivers living with patients without AEs and 268 (66.8%) living with patients with AEs. Thirty-two (8.0%) parents/caregivers were not included in any of the cohorts because they did not meet the inclusion criteria for any of the cohorts (i.e., their child experienced symptoms/complications in the past 30 days that existed prior to the initiation of their latest ADHD treatment but improved while on treatment and did not have any other symptoms that appeared, worsened, or remained unchanged after the initiation of their latest ADHD treatment).
Parent/caregiver characteristics
Parent/caregiver characteristics overall and by cohort are presented in Table 1. Overall, parents/caregivers had a median age of 38 years, and the majority self-identified as female (58.9%) and of White race (72.8%). Most parents/caregivers reported being in a household of a couple with their children (58.6%), and one in five had a postgraduate degree (19.5%). Parents/caregivers were from across all U.S. regions, with a higher representation from the south (43.6%). On average, there were 2.2 children and 1.2 children with ADHD per household.
Parent/Caregiver Characteristics
Standardized difference >20%.
Characteristics were measured at the time of data collection.
More than one option could have been selected (i.e., responses were not mutually exclusive).
ADHD, attention-deficit/hyperactivity disorder; AE, adverse effect; SD, standard deviation.
Patient characteristics
Patient demographic, clinical, and treatment characteristics overall and by cohort are presented in Table 2. Patients included in the overall sample had a median age of 11 years and 37.7% were female. The reported race/ethnicity of patients included White (73.8%), African American or Black (21.9%), and Hispanic or Latino (14.5%). On average, patients were diagnosed with ADHD at the age of 7 years.
Patient Characteristics
Standardized difference >20%.
Characteristics were measured at the time of data collection.
More than one option could have been selected (i.e., responses were not mutually exclusive).
Overall, 75.3% of patients received prior pharmacological treatment for ADHD (patients with AEs: 80.2%; patients without AEs: 57.4%). The most common reasons for treatment interruptions (N = 62) as reported by parents/caregivers included child experienced side effects (38.7%) and stopped taking treatment during vacation (32.3%), while the most common reasons for treatment switch (N = 219) included the treatment did not work/did not help with child’s ADHD symptoms enough (42.0%), and child experienced side effects (38.8%) (data not shown).
In the month preceding data collection, 92.3% of patients had a nonpharmacological treatment and all patients had a pharmacological treatment for their ADHD, with the majority (53.9%) having initiated their pharmacological treatment less than 12 months prior to data collection. Specifically, 90.0% of patients received a stimulant and 25.2% received a nonstimulant. The proportion of patients receiving more than one type of pharmacological treatment was higher among those with AEs compared with those without (32.8% vs. 17.8%). When asked about the selection process of the current ADHD treatment, 43.9% of parents/caregivers reported that the treatment was the option most recommended by health care provider out of several options presented to them, 27.9% reported making their decision collaboratively with their health care provider after being presented with multiple treatment alternatives, and 25.2% reported that the treatment was the only option presented by their health care provider. In addition, 70.6% of parents/caregivers reported discussing treatment efficacy and 59.4% discussed the risk of side effects with their health care provider when selecting their child’s ADHD treatment.
Patient adherence and parent/caregiver satisfaction with current pharmacological treatment
Overall, 64.6% of parents/caregivers reported their children skipped or missed a dose of current ADHD treatment at least sometimes, with this proportion being higher among those with an AE than those without (73.9% vs. 43.6%; Table 2). Among parents/caregivers whose child at least sometimes skipped or missed a dose of current pharmacological treatment (N = 258), the most commonly reported reasons were child forgets to take it (50.4%), timing of dosing conflicts with daily routine and/or other activities (25.2%), and actual or potential side effects (25.2%) (data not shown).
Parents/caregivers of patients with AEs were more likely to be very dissatisfied, moderately dissatisfied, or neither satisfied nor dissatisfied with their child’s current ADHD treatment compared with those of patients without AEs (13.4% vs. 2.0%; Table 2). The main reasons for the lack of satisfaction included symptoms not sufficiently improved (34.1%) and side effects (31.7%) (data not shown).
AEs and their perceived impact
In the 30 days prior to data collection, patients experienced an average of 1.2 AEs, with approximately two-thirds (66.8%) of patients experiencing at least one AE. The most frequently reported AEs were insomnia/sleep disturbances (14.2%), decreased appetite/weight loss (11.7%), and emotional impulsivity/mood lability (10.2%) (Fig. 1).
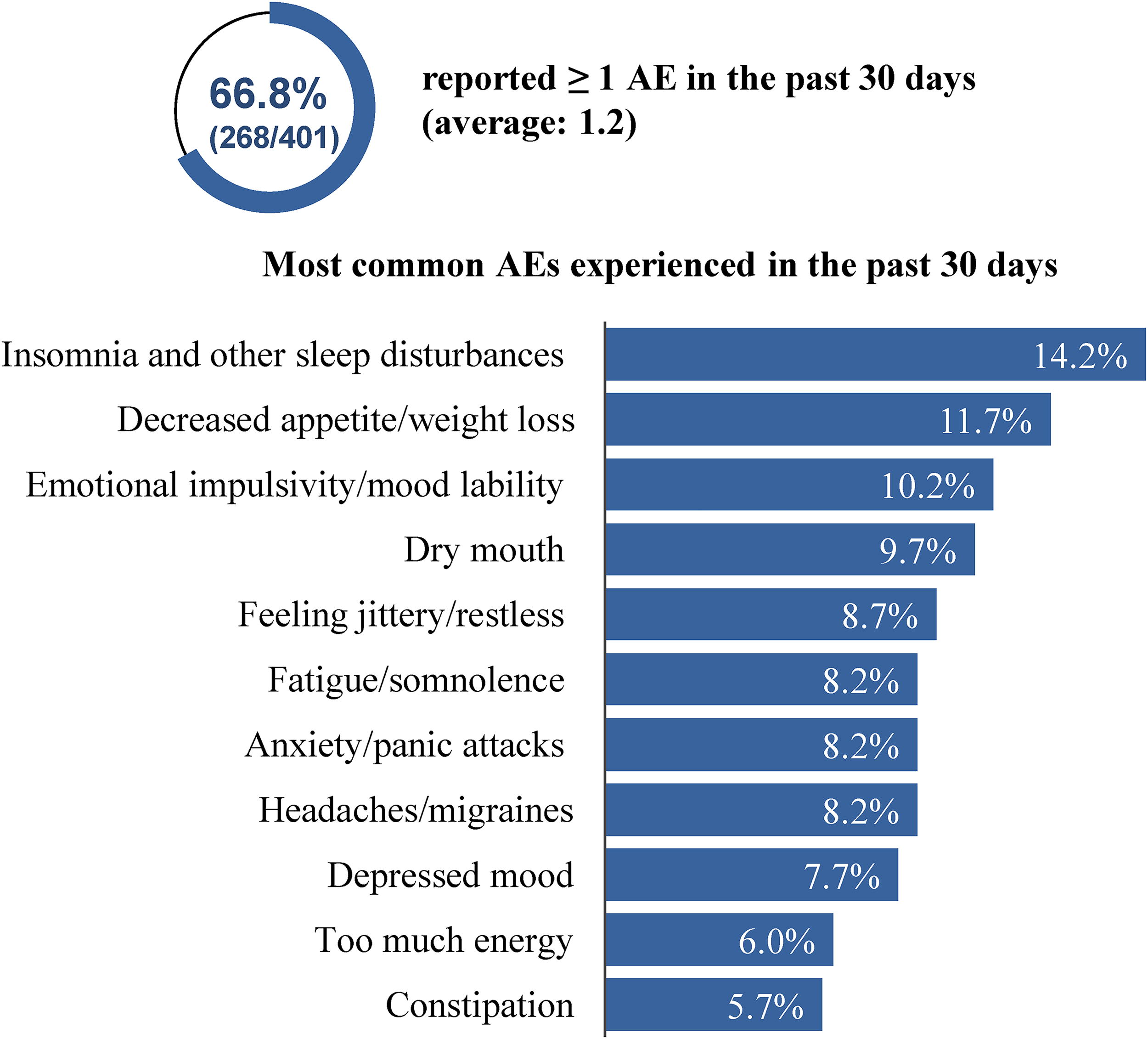
AEs experienced by patients in the past 30 days. AEs during ADHD treatment were symptoms/complications experienced in the past 30 days that appeared, worsened, or remained unchanged after patients initiated their latest ADHD treatment. More than one symptom could have been selected. ADHD, attention-deficit/hyperactivity disorder; AE, adverse effect.
A total of 162 parents/caregivers reported their child experienced insomnia and other sleep disturbances, decreased appetite/weight loss, emotional impulsivity/mood lability, anxiety/panic attacks, depression, fatigue/somnolence, or gastro-intestinal symptoms in the past 30 days of the study. The vast majority of them reported that these AEs had a negative impact on their child’s and their own well-being. Anxiety/panic attacks, emotional impulsivity/mood lability, and insomnia and other sleep disturbances had a particularly important impact, with more than one in three parents/caregivers reporting that each of these AEs had a lot or extremely negative impact on their child’s and their own overall well-being when present (Fig. 2). Nonetheless, among the parents/caregivers whose child experienced one of the selected AEs, 21.6% of parents/caregivers reported not discussing at least one AEs experienced by their child with their health care providers.
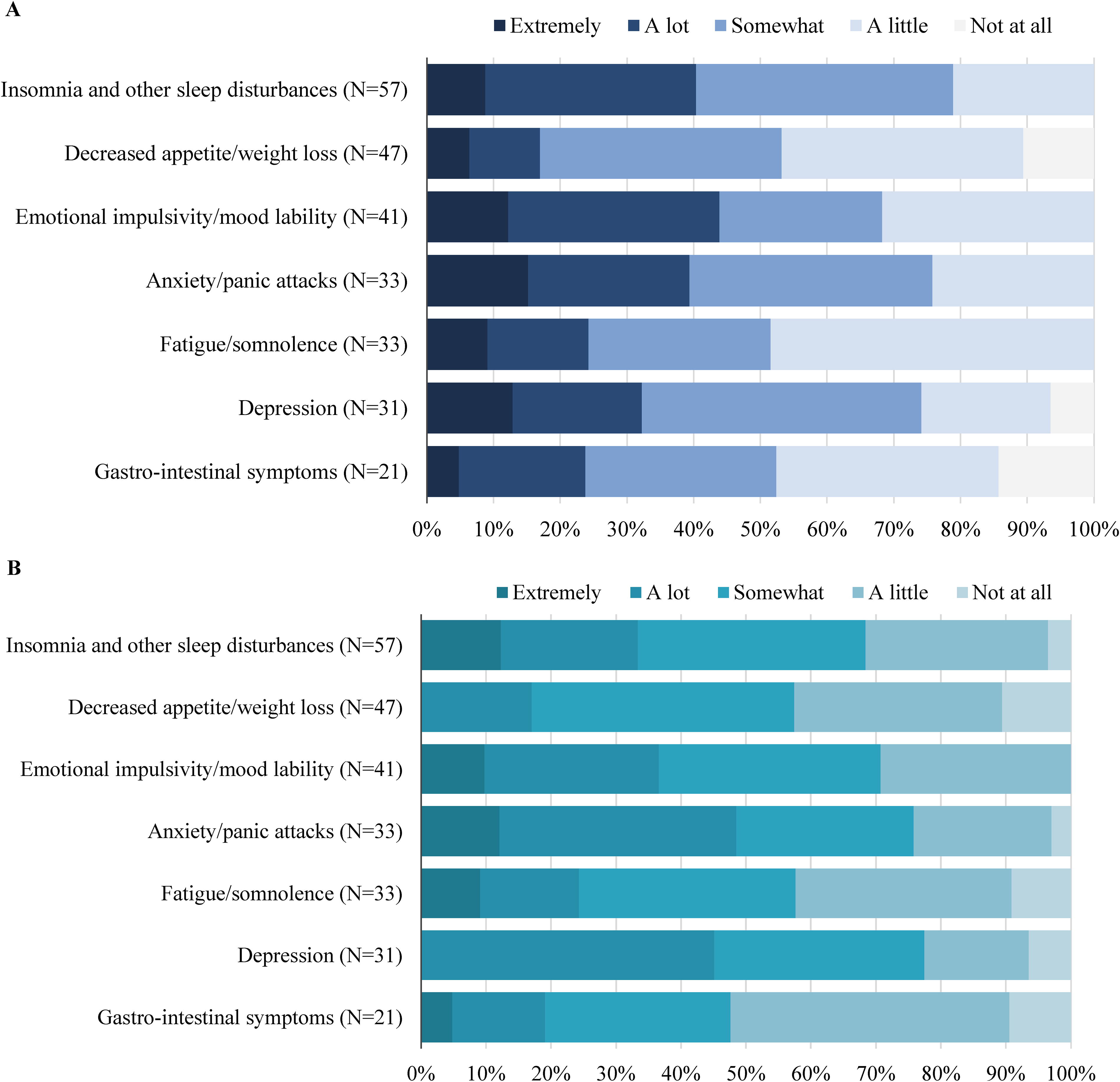
Perceived impact of selected AEs on (A) child’s overall well-being and (B) parent/caregiver’s overall well-being in the past 30 days.
Patient outcomes—HRQoL and HRU
Patients with AEs had significantly lower HRQoL than patients without AEs (PedsQL total score: 55.7 vs. 70.4; p < 0.001). All the PedsQL component scores, including those measuring physical functioning and psychosocial health (i.e., emotional, social, and school functioning), were also significantly lower among patients with AEs compared with those without (all p < 0.001; Fig. 3).

Overall, patients with AEs had significantly more ADHD-related health care visits to pediatricians (p < 0.001), psychiatrists (p < 0.001), and psychologists (p = 0.004) over the past year than those without AEs; the proportion of patients with primary care physician visits was not statistically different between the two cohorts (p = 0.105) (Supplementary Fig. S1).
Parent/caregiver outcomes—work and activity impairment, mental health, and HRU
Most parents/caregivers (71.8%) were currently employed at the time of data collection. Parents/caregivers of patients with AEs reported having nearly twice as much work and activity impairment due to caregiving as parents/caregivers of patients without AEs across all WPAI-CG metrics, including impairment in daily activities (43.2% vs. 24.5%) and overall work impairment (45.4% vs. 21.5%; absenteeism: 14.9% vs. 5.5%; presenteeism: 39.9% vs. 20.2%) (all p < 0.001; Fig. 4).

Parent/caregiver work and activity impairment. Work and activity impairment were measured by WPAI-CG and expressed as a percentage, with higher numbers indicating greater impairment. AE, adverse effect; WPAI-CG, Work Productivity and Activity Impairment: Caregiver.
Mental health outcomes also tended to be worse among parents/caregivers of patients with AEs than those of patients without AEs, with a larger proportion having a high likelihood of GAD (41.0% vs. 18.8%) and MDD (36.2% and 14.9%) (all p < 0.001; Fig. 5).
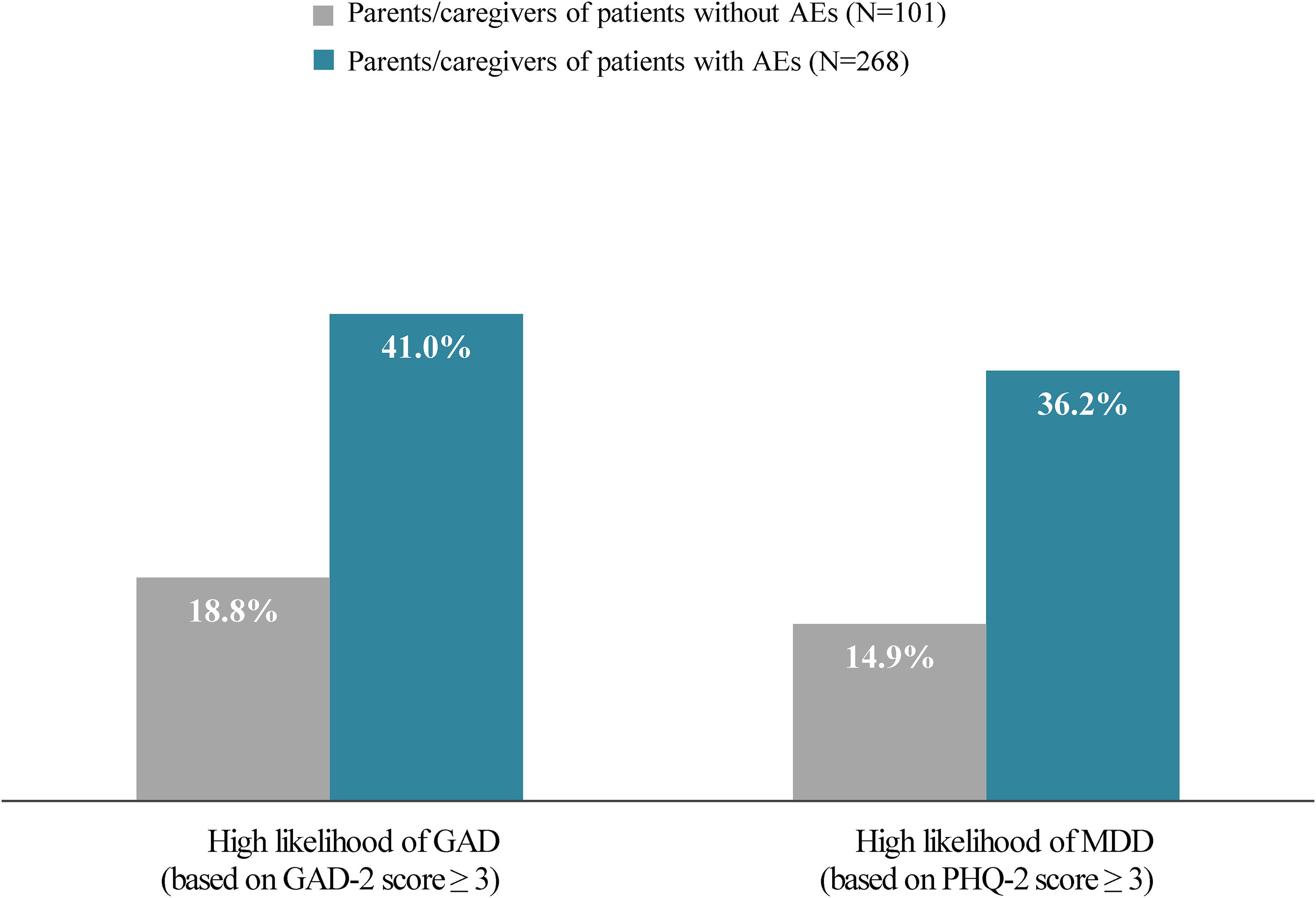
Parent/caregiver mental health. Mental health was measured by PHQ-4, which includes the GAD-2 for assessing GAD (score range: 0–6) and PHQ-2 subscales for assessing MDD (score range: 0–6); scores ≥3 indicate a likely diagnosis of the respective conditions. AE, adverse effect; GAD, generalized anxiety disorder; GAD-2, Generalized Anxiety Disorder 2-item; MDD, major depressive disorder; PHQ-2, Patient Health Questionnaire 2-item; PHQ-4, Patient Health Questionnaire 4-item.
The proportion of parents/caregivers who had five or more health care visits for any reason in the past year was significantly higher among those of patients with AEs than those of patients without AEs (35.1% vs. 14.9%; p < 0.001; Supplementary Fig. S2).
Association between AEs in the past 30 days and key outcomes
In adjusted regression analyses, the number of AEs was statistically significantly correlated with a reduction in patient’s HRQoL (Table 3). Specifically, each additional AE in the past 30 days was associated with a 4.9-point decrease (p < 0.001) in the PedsQL total score. Similar statistically significant correlations were observed for each of the PedsQL components (all p < 0.001).
Association Between the Number of AEs in the Past 30 Days and Key Outcomes
Significant at the 0.1% level.
Higher PedsQL scores indicate better HRQoL. Thus, a negative estimate indicates that AEs are associated with a lower HRQoL.
Work/activity impairment is expressed as a percentage, with higher numbers indicating greater impairment. Thus, a positive estimate indicates that AEs are associated with a larger impairment. Work impairment refers to the impact of caregiving on the ability to work and is equal to absenteeism (work time missed) plus presenteeism (impairment at work/reduced on-the-job effectiveness).
An OR >1 indicates that AEs are associated with a higher probability of having a high likelihood of GAD or MDD.
AE, adverse effect; CI, confidence interval; GAD, generalized anxiety disorder; GAD-2, Generalized Anxiety Disorder 2-item; HRQoL, health-related quality of life; MDD, major depressive disorder; OR, odds ratio; PedsQL, Pediatric Quality of Life, PHQ-2, Patient Health Questionnaire 2-item; WPAI-CG, Work Productivity and Activity Impairment: Caregiver.
For parents/caregiver outcomes, adjusted regression analyses found that AEs were statistically significantly correlated with increased work and activity impairment and worse mental health outcomes (Table 3). Specifically, each additional AE in the past 30 days was associated with a 6.0-percentage point increase in work impairment, 5.7-percentage point increase in activity impairment, 48% increased odds of having a high likelihood of GAD, and 44% increased odds of having a high likelihood of MDD (all p < 0.001).
Discussion
In this online parent/caregiver survey, more than two in three pediatric patients receiving pharmacological treatment for ADHD experienced AEs in the 30 days prior to data collection, and AEs were statistically significantly associated with worse patient and parent/caregiver outcomes. Notably, each additional AE was associated with a 4.9-point decrease in the parent proxy-report PedsQL total score, whereas the clinically important difference for this instrument has been reported to be 4.5 points (Varni et al., 2003). The impact of AEs in pediatric patients spilled over to their parents/caregivers, who had significantly impaired work productivity and daily function as well as higher risks of having mental health issues such as GAD and MDD (48% and 44% increased odds, respectively). The increased HRU among both the patients and parents/caregivers in the presence of AEs also highlighted the added burden of these AEs on the health care system.
The findings of this study are largely consistent with existing evidence of the impact of specific symptoms and complications associated with ADHD treatments on pediatric patient and caregiver outcomes (Becker et al., 2019; Chaulagain et al., 2023; Nelson et al., 2022; Sung et al., 2008; Waring and Lapane, 2008). A prior caregiver survey found that children with ADHD (about 90% used medication) had significantly lower PedsQL total score if they had sleep problems and that caregivers of children with moderate or severe sleep problems were almost three times more likely to be clinically depressed, anxious, or stressed than those with children who had no sleep problems (Sung et al., 2008). Another cross-sectional analysis based on a U.S. national survey found that children with ADHD managed by stimulants, which are known to suppress appetite, had a 1.6-time odds of being underweight compared with those without ADHD (Waring and Lapane, 2008), mandating patient behavioral management and parent education on their children’s dietary intake (Phillips, 2014).
While prior pediatric ADHD studies quantifying the overall impact of AEs have been limited, a prior survey among adult patients with ADHD in the United States has reported significant negative association of AEs with adult patient’s HRQoL, employment, work productivity, and daily functioning (Schein et al., 2023); these outcomes have previously been shown to account for large amounts of societal excess costs attributable to adult ADHD in the United States (Doshi et al., 2012; Schein et al., 2022b). Importantly, the current study showed that these negative outcomes seen in adults with ADHD also extended to the adult parents/caregivers of pediatric patients with ADHD who experienced AEs, underscoring the potentially profound indirect impact of these AEs on parents/caregivers and the society. Future research may evaluate how heterogeneities in ADHD clinical presentations and treatment strategies (e.g., polypharmacy vs. monotherapy) (Baker et al., 2021; Luo et al., 2019) may affect AEs experienced by pediatric patients with ADHD and their association with quality of life and outcomes of the patients and their families.
In this study, two-thirds of parents/caregivers reported their children at least sometimes skipped or missed a dose of their current ADHD treatments, aligning with prior observations that low adherence to ADHD treatment is common (Ahmed and Aslani, 2013). Factors associated with low adherence are multifactorial, and reasons reported in this study such as dosing inconvenience and actual or potential side effects have been shown to predict decreased adherence to ADHD medications (Charach and Fernandez, 2013). In addition, more parents/caregivers in this study expressed dissatisfaction with the treatment when their children experienced AEs, and that side effects were among the main reported reasons for dissatisfaction alongside insufficiently improved symptoms. Of note, safety and efficacy concerns have been recognized to contribute to treatment discontinuation among pediatric patients with ADHD (Gajria et al., 2014; Schein et al., 2022d; Sondergaard et al., 2024), and treatment discontinuation could further add to the already substantial health care costs associated with pediatric ADHD (Schein et al., 2022a; Schein et al., 2022c). Altogether, these results suggest that more tolerable and effective treatment options may increase patient satisfaction and potentially lead to greater adherence and persistence, which may in turn improve treatment efficacy (MTA Cooperative Group, 2004; Tsujii et al., 2020) and reduce subsequent health care costs.
Despite the substantial impact of AEs on their own and their child’s outcomes, more than 40% of parents/caregivers in this study reported not discussing the risk of side effects with their health care providers at treatment selection. Furthermore, more than one in four parents/caregivers reported that the treatment was the only option presented by their health care provider. These results highlight the need to improve patient–physician communication and to raise awareness among physicians regarding the impact of AEs on the well-being of pediatric patients and their parents/caregivers. The importance of shared decision-making is illustrated by two recent discrete choice experiments in the United States showing that, compared with adult patients, physicians tended to give a higher relative importance to improvement in ADHD symptoms for the treatment of adult ADHD, which resulted in discrepancies in the preferred treatment profile (Schein et al., 2024a; Schein et al., 2024b). The negative impact of AEs on patient’s well-being could have partially affected patient’s treatment preferences toward safer treatments compared with physician’s.
Collectively, the findings of this study suggest that more tolerable treatments have the potential to improve the experience for pediatric patients with ADHD and their parents/caregivers. Future studies are warranted to understand the impact of AEs experienced by pediatric patients with ADHD on health care costs and disease burden.
Limitations
First, participants of this survey were those who were accessible through the vendor’s panel and were willing to participate in the study; these participants tend to be younger and more educated. In addition, females are generally more likely than males to participate in surveys (Becker, 2022). Thus, participants of this survey may not be representative of the population of parents/caregivers of children with ADHD in the United States. Second, survey studies rely on participants’ recollection of past events for data, and hence recall bias or errors in the accuracy or completeness of the recalled experiences may have occurred; this survey aimed to minimize recall bias by asking about events that occurred in the recent past (e.g., past 30 days) as much as possible. Third, all survey responses were completed by parents/caregivers and may not represent the patients’ perspectives; nonetheless, a meta-analysis of studies using PedsQL as HRQoL measure has found no significant difference between parent-reported and child-reported HRQoL (Wanni Arachchige Dona et al., 2023). Fourth, the study measured AEs based on an operational definition and may not accurately capture all AEs experienced by pediatric patients with ADHD in real life. Finally, this is an observational study, as such our findings should be interpreted as correlation between AEs and quality of life in either direction, and no causal inferences can be made.
Conclusions
Findings from this study suggest that AEs are common among pediatric patients with ADHD receiving pharmacological treatment and have a significant negative association with both the patients’ HRQoL and their parents/caregivers’ work productivity, daily functioning, and mental health. Effective and tolerable treatment options along with better management of AEs and improved patient–physician communication have the potential to improve the experience for pediatric patients and their parents/caregivers.
Clinical Significance
Our findings demonstrate that AEs experienced by pediatric patients receiving ADHD medications may not only reduce their HRQoL but also impair their parents/caregivers’ work productivity, daily functioning, and mental health, which in turn have important implications for the health care system and the society. More tolerable treatment options for ADHD may help improve treatment adherence and persistence as well as the overall well-being of pediatric patients and their parents/caregivers.
Footnotes
Acknowledgments
Medical writing assistance was provided by professional medical writer, Flora Chik, PhD, MWC, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Otsuka Pharmaceutical Development & Commercialization, Inc, which funded the development and conduct of this study and article.
Authors’ Contributions
J.S.: Conceptualization, formal analysis, methodology, and writing—review and editing. M. Cloutier: Conceptualization, data curation, formal analysis, investigation, methodology, and writing—review and editing. M.G.-L.: Conceptualization, data curation, formal analysis, investigation, methodology, and writing—review and editing. M. Catillon: Data curation, formal analysis, investigation, methodology, and writing—review and editing. L.Y.: Data curation, formal analysis, investigation, methodology, and writing—review and editing. B.L.: Data curation, formal analysis, investigation, methodology, writing—review and editing. Y.W.: Data curation, formal analysis, investigation, methodology, and writing—review and editing. A.C.: Conceptualization, formal analysis, methodology, and writing—review and editing.
Funding Information
This study was funded by
Disclosures
J.S. is an employee of
Previous Presentations
Part of the material in this article was presented at the ISPOR 2024 held May 5–8, 2024, in Atlanta, GA, USA, as a poster presentation.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.