
Abstract
Introduction:
Transcranial magnetic stimulation (TMS) is a promising intervention for adolescents with treatment-resistant depression (TRD). However, the durability of TMS-related improvement in adolescents is unclear. This 6-month study followed adolescents with TRD who had responded to TMS and provided TMS retreatment for adolescents with a partial relapse.
Methods:
The study enrolled adolescents (12–21 years) with TRD who had at least a partial response to sham or active TMS in a randomized controlled trial. Partial response was defined as ≥25% reduction of Hamilton Depression Rating Scale-24 (HAMD24). Participants with a partial relapse (≥1 point increase in Clinical Global Impression–Severity) received retreatment with daily 10 Hz TMS sessions until depressive symptom severity returned to the baseline score or after 30 TMS treatments.
Results:
There were 84 eligible participants, 66 were enrolled, and 41 completed the 6-month study. Twenty-eight participants (42%) were retreated with TMS. TMS retreatment courses had a mean of 22 sessions. At the 6-month follow-up, the complete sample exhibited reduced depressive symptoms (mean HAMD24 of 5.24) compared with baseline at entry into follow-up (mean HAMD24 of 8.21). Baseline depressive symptom severity was positively correlated with the risk of partial relapse, while the number of previous TMS interventions showed no correlation with the risk of partial relapse. TMS was well tolerated.
Conclusions:
This is the largest, long-term follow-up study with TMS retreatment for adolescents with TRD. These findings demonstrate the feasibility and clinical effects of a TMS retreatment protocol for adolescents with TRD, following a standard course of acute TMS.
Introduction
Approximately 40% of adolescents with major depressive disorder (MDD) fail to benefit from antidepressant medications and evidence-based psychotherapies (Avenevoli et al., 2015; Brent et al., 2008). Studies suggest that adolescents with treatment-resistant depression (TRD) treated with a second antidepressant with or without cognitive behavioral therapy have a remission rate of less than 50% (Brent et al., 2008; Kennard et al., 2014; Saito et al., 2023). Approximately 20% of youth with TRD relapse within 24 weeks (Avenevoli et al., 2015; Brent et al., 2008; Kennard et al., 2014). Thus, better interventions are urgently needed for adolescents with MDD and TRD (Lam et al., 2024; Radecki et al., 2024). Transcranial magnetic stimulation (TMS) is a promising treatment for TRD that was recently cleared by the Food and Drug Administration (FDA) as an adjunctive treatment for adolescents aged 15 years and older with MDD (Hett et al., 2021; Qiu et al., 2023; Sigrist et al., 2022; Sun et al., 2023).
Pharmacologic and psychotherapeutic maintenance treatments for MDD and TRD have not been extensively studied in adolescents. The reemergence of depressive symptoms is common in adolescents who have had successful acute treatment courses for MDD. High relapse rates in adolescents with depressive disorders are concerning, and there are few studies on posttreatment strategies following initial clinical improvements (Kennard et al., 2014; Saito et al., 2023). Follow-up studies of adolescents with TRD over 6 months to 3 years after acute TMS treatment support its long-term effectiveness and safety (Mayer et al., 2012; Wall et al., 2011). There are various strategies for long-term TMS treatment for adults with MDD but no clear consensus on the optimal approach (Janicak et al., 2010; Wilson et al., 2022). Extended TMS treatment protocols have not been studied in adolescents, and the durability of acute TMS interventions in adolescents with TRD is unknown.
With these considerations in mind, this study enrolled adolescents with TRD who had clinical benefits after participating in a randomized controlled trial of TMS (Croarkin et al., 2021). We sought to evaluate the durability of the clinical effects of TMS intervention as well as the feasibility, tolerability, and clinical effects of TMS retreatment over 6 months. Our protocol mirrored a previous study by Janicak et al., which showed that early intervention with maintenance TMS could sustain clinical benefits and was well tolerated in adults with MDD (Janicak et al., 2010). As such, partial response was defined as ≥25% improvement from baseline (prior to any intervention in the phases of the clinical trial) 24-item Hamilton Depression Rating Scale (HAMD-24). During the present (Phase III) study, partial relapse was defined as a Clinical Global Impression–Severity (CGI-S) scale worsened by ≥1 point compared with the Phase III baseline for two consecutive weeks. Relapse was defined as symptoms meeting full criteria for MDD. Our secondary objective was to identify characteristics associated with the durability of TMS benefits. We hypothesized that TMS retreatment over 6 months would be feasible based on patient retention and clinical benefit in this sample. We also hypothesized that the level of treatment resistance, depressive symptom severity, and the number of prior active TMS sessions would predict the need for retreatment.
Methods
Study overview
This was a 13-site, multicenter study of adolescents with TRD who had participated in a randomized controlled trial (NCT02586688) of repetitive TMS as monotherapy over the left dorsolateral prefrontal cortex (Fig. 1). Institutional review board approval was obtained prior to any research activities. Adolescents aged 17 years or younger provided informed assent, and a parent or legal guardian provided written informed consent. Participants aged 18 years or older provided written informed consent. Participants and families received parking vouchers for visits to the study sites but no other remuneration.
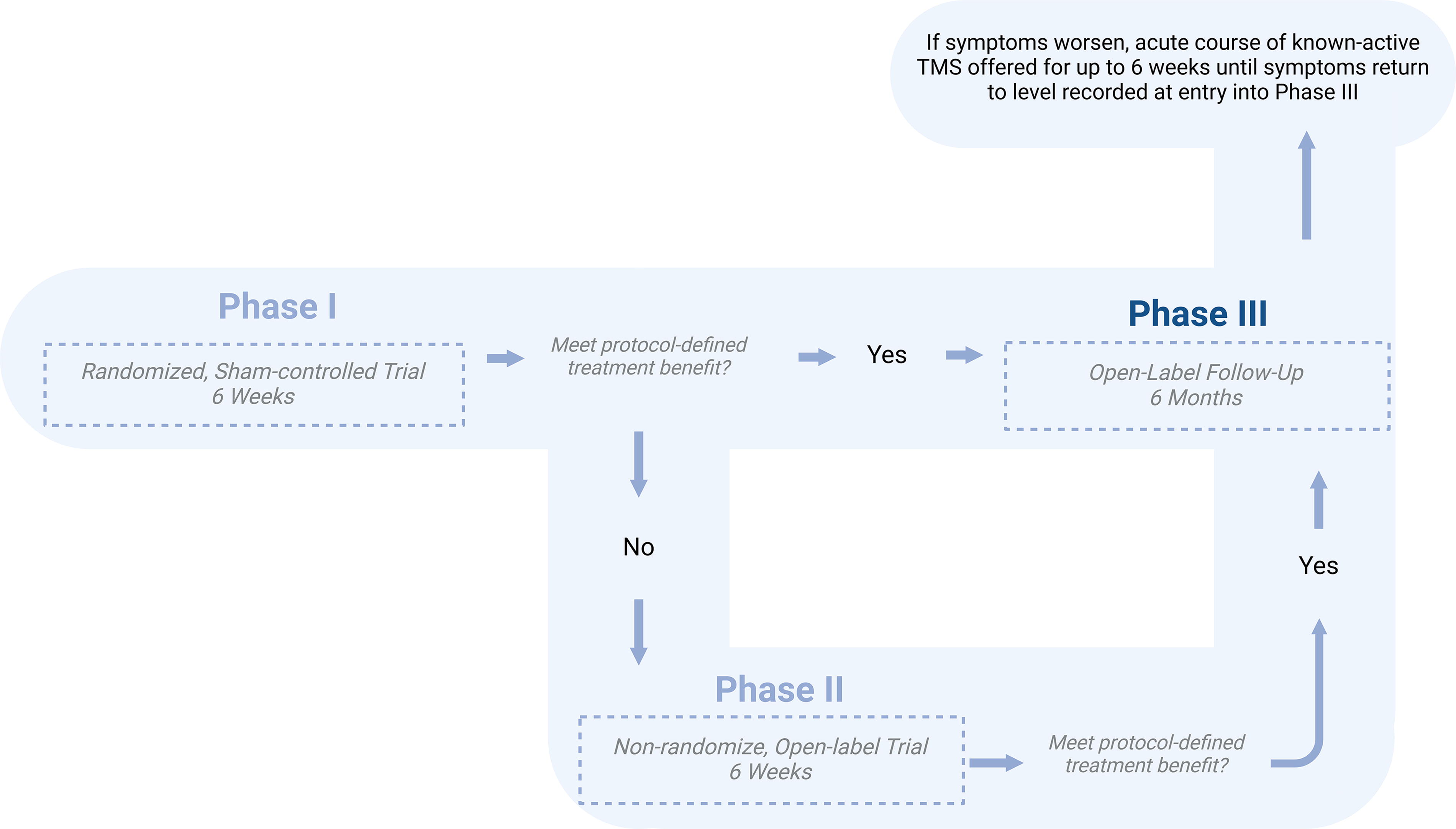
Clinical trial overview.
During the initial (acute) phase (Phase I), adolescents were randomized (1:1) to either active or sham stimulation arms and received 30 sessions over 6 weeks. Adolescents who did not have a partial response defined as ≥25% improvement from their baseline HAMD-24 score were eligible to participate in Phase II of the study. Phase II provided 6 weeks of 30 active (open label) 10 Hz TMS sessions, mirroring the intervention provided in the active arm of Phase I without unblinding the participants. At the end of either Phase I or II, each participant underwent a 3-week TMS tapering period. During tapering, participants received three TMS sessions in the first week, two in the second week, and one in the third week (Croarkin et al., 2021).
Adolescents who experienced a partial response to treatment in either phase of the study, defined as ≥25% reduction in the severity of their depressive symptom severity (based on HAMD-24), were eligible to participate in the Phase III study, which is the focus of this report. During Phase III, participants with a partial relapse, defined as a CGI-S scale worsened by ≥1 point compared with the Phase III baseline, for two consecutive weeks, were offered TMS retreatment for up to 30 sessions or until their CGI-S scale returned to Phase III baseline levels. Partial response and partial relapse thresholds were based on prior work and the intent to enroll and study as many participants as possible (Janicak et al., 2010).
Participants
Eligibility criteria for Phase III included participants who were aged 12–21 years, had a current episode of MDD without psychotic features, and had treatment resistance in the current episode (antidepressant treatment record [ATR] level of 1–4; Croarkin et al., 2021; Sackeim, 2001; Strawn et al., 2020). Inclusion and exclusion criteria have been described elsewhere (Croarkin et al., 2021). Concomitant medications for insomnia (including zaleplon, zolpidem, zopiclone, or lorazepam) were allowed on a limited basis, as described previously (Croarkin et al., 2021). Concurrent psychotherapy with a stable dose for 3 months before screening, with no planned changes in the frequency or focus during the study, was allowed.
Participants disposition
Of the 112 adolescents who started Phase I, 84 were eligible for participation (i.e., achieved a 25% reduction in HAMD-24 during Phase I or II), and 66 enrolled in Phase III. Among adolescents initiating Phase III, 44 demonstrated clinical benefit during Phase I, with 23 receiving active TMS (group A) and 21 receiving sham TMS (group S). There were 22 adolescents with clinical benefit during Phase II, with 8 who had received active TMS (group AA) and 14 who received sham TMS (group SA) during Phase I (Table 1). Figure 2 provides further details regarding participant enrollment and dropout for the present Phase III study.
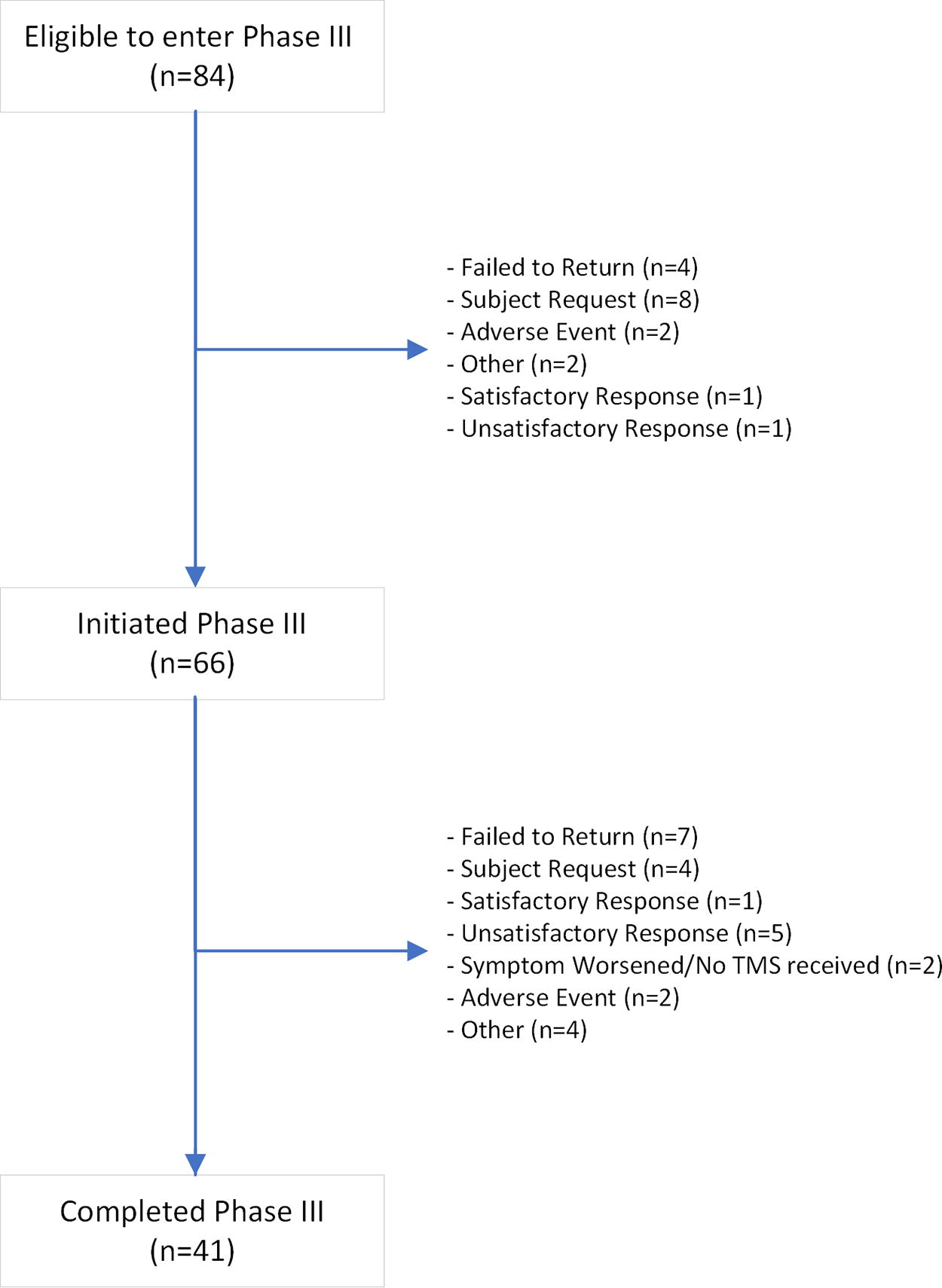
Phase III participant flow.
Baseline Demographic and Clinical Characteristics
Adolescents who received 6 weeks of active rTMS and transitioned from Phase I to Phase III.
Adolescents who received 6 weeks of sham rTMS and transitioned from Phase I to Phase III.
Adolescents who received 12 weeks of active rTMS and transitioned from Phase II to Phase III.
Adolescents who received 6 weeks of sham rTMS and 6 weeks of active rTMS, and transitioned from Phase II to Phase III.
Demographic and clinical data are based on the characteristics of the participants in Phase I entry.
Baseline clinical data of Phase III is based on the last assessment before entering the 6-month follow-up period phase.
ATR, antidepressant treatment record; CDRS-R, Children’s Depression Rating Scale–Revised; CGI-S, Clinical Global Impression–Severity of Illness; HAM-D-24, 24-item Hamilton Depression Rating Scale; MADRS, Montgomery–Asberg Depression Rating Scale; MDD, major depressive disorder; QIDSA17-SR, Quick Inventory of Depressive Symptomatology–Adolescent (17-Item)–Self-Report version; SD, standard deviation; rTMS, repetitive transcranial stimulation.
Interventions
Adolescents experiencing a partial relapse received active TMS retreatment using the NeuroStar® Advanced Therapy System, applying the same parameters of Phase I and II active TMS intervention (Croarkin et al., 2021). Adolescents were assessed weekly during retreatment, and TMS was discontinued when the CGI-S scores returned to the Phase III baseline score or at the completion of 30 TMS sessions. Coil placement, motor threshold determination, delivery, and session details have been described previously (Croarkin et al., 2021). The treatment site for the coil was the left dorsolateral prefrontal cortex localized with the 5 cm rule. TMS retreatment sessions (75 trains and 3000 pulses, spanning 37.5 minutes) were conducted daily, 5 days a week, for 1–6 weeks (5–30 sessions). A 3-week taper followed each retreatment course, with three TMS sessions during the first week, two during the second week, and one during the third week. After completing a TMS retreatment course followed by a tapering period, adolescents continued follow-up in the study and could receive additional TMS retreatment courses if subsequent reemergence of depressive symptoms were observed.
Participants who met diagnostic criteria for MDD confirmed on two occasions within 2 weeks were withdrawn from the study. Adolescents with a persisting partial relapse, evidenced by the CGI-S score failing to return to baseline after TMS retreatment, were withdrawn from the study. These withdrawal criteria ensured participant safety as additional treatment modalities could be initiated.
Assessments
Clinical raters were blind to the intervention assignments from Phase I and participation in Phase II. A comprehensive clinical status was assessed after completing 3 and 6 months of the follow-up period. Raters determined clinical status and outcomes during structured interviews using the HAM-D (Hamilton, 1967); the Montgomery–Asberg Depression Rating Scale (Montgomery and Asberg, 1979), the Children’s Depression Rating Scale–Revised (Poznanski et al., 1984), the CGI-S scale (Guy, 1976), and the Quick Inventory of Depressive Symptomatology–Adolescent (17-Item)–Self-Report (QIDS-A17-SR; Bernstein et al., 2010).
Monthly assessments were completed with the CGI-S and QIDS-A17-SR. If a CGI-S score worsened by one point during Phase III, a follow-up clinical assessment was conducted within a week. If the worsening of symptoms was confirmed during this follow-up visit, the participant was offered TMS retreatment. After each week of TMS retreatment, participants underwent a thorough clinical evaluation until their CGI-S score returned to the level observed at Phase III entry or until they had completed 30 TMS sessions.
Outcome variables
Adolescents were stratified into four categories based on prior TMS protocols received: those who benefited from active TMS in Phase I (group A), those who benefited from sham TMS in Phase I (group S), those who benefited from active TMS in Phase II after receiving active TMS during Phase I (group AA), and those who benefited from active TMS in Phase II after receiving sham TMS during Phase I (group SA; see Fig. 1 for the trial design). The primary outcome was the risk of partial relapse, defined as an increase of one or more points on the CGI-S scale for two consecutive weeks. Continuous secondary outcomes included clinical rating scales from baseline to endpoint and the number of TMS retreatment sessions. Categorical secondary outcomes included response, remission, and spontaneously reported adverse events during the follow-up period. The baseline clinical status of Phase III was determined by the last comprehensive clinical assessment before initiating the 6-month follow-up period, which could have been taken at the end of Phase I, Phase II, or corresponding TMS tapering periods. Partial response was defined as a ≥25% reduction from Phase I baseline HAMD-24, response as a ≥50% from Phase I baseline HAMD-24, and remission as a HAMD-24 total score of ≤3 points. The level of treatment resistance was determined based on the ATR level in the current episode, ranging from 1 to 4, or by the number of antidepressant trials in a previous episode at an adequate dose and duration. The adequate dose and duration were established according to the ATR (Sackeim, 2001; Strawn et al., 2020).
Statistical analysis
The clinical and demographic characteristics were described using sample mean and standard deviation for continuous variables and frequency with percentage for the categorical variables. For the primary objectives, groups based on prior intervention were compared. A Kaplan–Meier curve was used to estimate the risk of reappearance of depressive symptoms between groups and the complete sample. Subgroup analyses were conducted to examine the influence of prior intervention characteristics on the risk of depressive symptoms reappearance. These subgroups were defined by response to previous TMS interventions and medication resistance levels (ATR). To compare the clinical outcomes, changes in HAM-D 24 total scores at 3 and 6 months of Phase III were analyzed using mixed effects models. Fixed effects corresponded to the treatment groups. The restricted maximum likelihood method was employed for parameter estimation. Statistical significance of the treatment effects was assessed using type 3 tests of fixed effects and least squares means. Exploratory analyses were conducted to examine the influence of prior intervention characteristics, times of partial relapse, and groups on the number of sessions given during the follow-up period. The level of significance was set at α = 0.05 (two-tailed). Statistical computations were performed using SAS (version 9.4) and R (version 4.4.1).
Results
Clinical and demographic characteristics
Eighty-four adolescents had a partial or full response to TMS treatment in Phase I or II. Sixty-six participants enrolled in the Phase III protocol, with 28 (43%) requiring retreatment and 41 participants completing the 6-month follow-up assessments (Fig. 2). Among those who started Phase III, 62% were female, the average age was 17.3 years, and the mean duration of the depression episode at baseline was 12.8 months. Additional demographic and baseline clinical characteristics are summarized in Table 1.
Clinical outcomes during the follow-up
In the overall sample, there was a significant decrease in both HAMD-24 and CGI-S from baseline to the end of the 6-month period (Wilcoxon signed-rank test: HAMD-24, V-value: 468, p = 0.01; CGI-S, V-value: 266, p < 0.001). However, there were no significant differences in the change in HAM-D-24 scores among adolescents when comparing the four intervention groups at both 3 months (F = 0.50, p = 0.68) and 6 months (F = 0.51, p = 0.68). At 6 months considering all participants who had enrolled (n = 66), 39 adolescents were responders (59%) and 22 achieved remission (33%). During the 6-month study, 25 adolescents (38%) dropped out and 2 (3%) had a relapse. Table 2 summarizes the clinical changes observed during the follow-up. Figure 3 summarizes the CGI scores for the present study and all phases of the overall clinical trial.
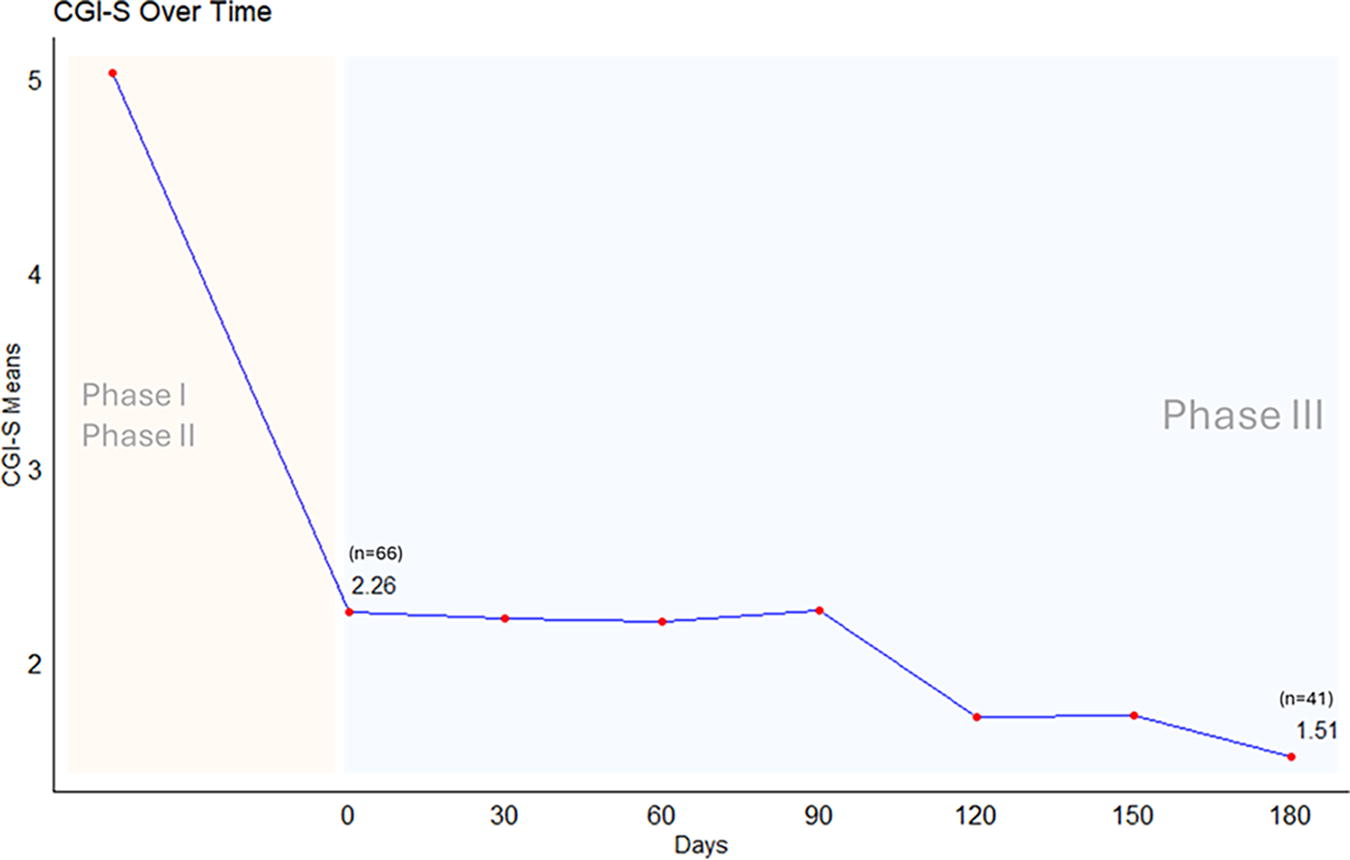
Clinical outcome. Illustration of the CGI-S mean of Phase III participants across all three trial phases. The CGI-S mean scores for Phases I and II (highlighted in yellow) reflect only the initial and final CGI-S scores of participants who progressed and entered Phase III. CGI-S, Clinical Global Impression–Severity.
Phase III Clinical Outcomes
Adolescents who received 6 weeks of active rTMS and transitioned from Phase I to Phase III.
Adolescents who received 6 weeks of sham rTMS and transitioned from Phase I to Phase III.
Adolescents who received 12 weeks of active rTMS and transitioned from Phase II to Phase III.
Adolescents who received 6 weeks of sham rTMS and 6 weeks of active rTMS and transitioned from Phase II to Phase III.
Score changes were based on the last assessment before entering in the follow-up period phase and the sixth month of the follow-up period. Subjects with missing data are excluded.
CDRS-R, Children’s Depression Rating Scale–Revised; CGI-S, Clinical Global Impressions–Severity of Illness; HAM-D-24, 24-item Hamilton Depression Rating Scale; QIDS-SR, Quick Inventory of Depressive Symptomatology–Self-Report version; SD, standard deviation; TMS, transcranial magnetic stimulation; rTMS, repetitive transcranial stimulation.
Partial relapse and TMS retreatment
Of the 66 adolescents, 28 (42.42%) required TMS retreatment; of these, 62% received 30 sessions of TMS. The restricted mean survival time until partial relapse was 152.7 days (SD: 10.1 days). The second month of the follow-up showed the highest rate of partial relapse across the complete sample (36%). There were no significant differences in the risk of partial relapse between groups (Kaplan–Meier analysis, log-rank p = 0.606) (Supplementary Fig. S1).
At Phase III entry (baseline in the current analysis), 54/66 (82%) of adolescents had a complete response (≥50% reduction in baseline HAMD-24 score), and 12/66 (18%) had a partial response (25%–49% reduction in baseline HAMD-24 score). Adolescents with a complete response after Phase I and II interventions (baseline in the current analysis) had a lower risk of partial relapse compared with those with partial response (Kaplan–Meier analysis, log-rank p ≤ 0.001) (Supplementary Fig. S2). Of the 54 adolescents with complete response at Phase III entry, 19 (35%) required TMS retreatment during the 6-month follow-up: 7/17 (41%) from group A, 5/18 (27%) from group S, 2/6 (33%) from group AA, and 5/13 (38%) from group SA. Higher baseline HAM-D24 scores were associated with a higher risk of partial relapse (Cox proportional hazard model, Hazard Ratio = 1.1126, p ≤ 0.001). In contrast, ATR levels were not associated with the risk of relapse (Cox proportional hazard model, Hazard Ratio = 1.06, p = 0.72).
Number of TMS retreatments sessions
The number of retreatment sessions after partial relapse ranged from 5 to 30 (mean: 22.5). Group AA consistently required 30 sessions; group SA had a mean of 15.83 sessions, group A had a mean of 24.17 sessions, and group S had a mean of 23.12 sessions per retreatment block. The number of TMS sessions per retreatment in Phase III was not associated with group, age, sex, ATR, duration of depressive episode, or the timing of partial relapse.
Safety and protocol adherence
Among the 25 adolescents who withdrew before completing the 6-month follow-up, the primary reason for discontinuation was failure to return. Patients who experienced clinical improvement after 30 sessions over 6 weeks in Phase I tended to have higher rates of discontinuation. Reasons for discontinuation during Phase III are summarized in Supplementary Table S1. During the present study, there were no seizures, suicide attempts, or other serious adverse events. There were two reported adverse events during the Phase III study. One participant reported a headache, and another reported increased anxiety. Both of these adverse events were classified as preexisting conditions. There were no reported adverse events or dropouts related to pain during treatment.
Discussion
This was the first study to assess the durability of antidepressant response to acute 10 Hz TMS in adolescents with TRD and the only study of its kind evaluating a TMS maintenance strategy over 6 months. Retreatment with TMS monotherapy when depressive symptoms reemerged was feasible, tolerable, and effective in adolescents with TRD. The relapse rate for adolescents in this 6-month study was 3% compared with 10% seen in a previous study with adults (Janicak et al., 2010). Adolescents with a full response to initial TMS treatment had a lower risk of depressive symptom reemergence (partial relapse) over 6 months compared with partial responders. Treatment resistance to previous pharmacological interventions did not influence outcomes over 6 months. Moreover, the number of prior TMS sessions did not affect clinical outcomes.
Two previous studies have examined the long-term effectiveness and safety of TMS in adolescents with TRD. Wall and colleagues followed seven adolescents for 6 months after 30 sessions of 10 Hz TMS (Wall et al., 2011), while Mayer and colleagues followed eight adolescents for 3 years after 14 sessions of 10 Hz TMS (Mayer et al., 2012). Both studies suggested that TMS was effective and safe for adolescents with TRD over the long term (Mayer et al., 2012; Wall et al., 2011). Our results align with these prior findings but in a larger cohort of adolescents with TRD. Emerging evidence indicates that ongoing TMS treatments in adults maintain the antidepressant effects of TMS, but there is no clear consensus on the best strategy for either adults or adolescents (Wilson et al., 2022). Our study demonstrated that TMS retreatment strategy for adolescents with TRD was safe and effective over a 6-month period. Notably, the adolescents in our present study did not take psychotropic medications during the 6-month monitoring and retreatment protocol.
There are unanswered questions related to the ideal duration of TMS treatments and how treatment frequency and dosing should be modified following acute response (Croarkin and Rotenberg, 2016; Sackeim et al., 2024; Wilson et al., 2022). While previous evidence suggests that TMS protocols in adolescents with TRD are safe, the number of TMS sessions in previous trials ranges from 10 to 60 sessions (Hett et al., 2021; Qiu et al., 2023). This is the first study evaluating the tolerability of TMS interventions following the reappearance of depressive symptoms after 30–60 sessions (6–12 weeks) of TMS interventions. Notably, throughout the three study phases (Phase I, Phase II, and the present study), adolescents received up to 90 sessions of 10 Hz TMS monotherapy. Furthermore, our results parallel evidence from psychopharmacologic trials, as adolescents with greater acute antidepressant benefit at baseline have a reduced risk of relapse during the 6-month TMS retreatment protocol (Brent et al., 2008; Hathaway et al., 2018).
The optimal TMS dosing patterns for adolescents with MDD remain undefined (Croarkin and Rotenberg, 2016; Zhao et al., 2023). Novel accelerated TMS protocols suggest that increasing the “density” of TMS—by increasing the number of sessions and pulses per day—may be a promising strategy (Cole et al., 2022; Geoly et al., 2024). However, regular, long-term TMS sessions may be another viable approach (Croarkin and Rotenberg, 2016; Sackeim et al., 2024; Wilson et al., 2022). Recent TMS research in adults suggests that interruptions in acute treatment courses may not be as problematic as noted in prior study protocols and guidelines (Carpenter et al., 2024). Long-term, flexible TMS protocols that treat and retreat to symptomatic improvement may be a promising approach for future studies (Croarkin and Rotenberg, 2016; Wilson et al., 2022). Neurodevelopmental factors, ages, and biological sex will be important variables to consider in future studies. Ultimately, improving TMS dosing in TRD will require precision approaches that consider individual patient characteristics, comorbidity, and circuit-level characteristics.
Large naturalistic studies in adults with depression suggest that early improvement and the number of TMS sessions received predict response (Hutton et al., 2023; Sackeim et al., 2024). However, our study did not identify differences in outcomes related to early improvement or the number of TMS sessions received. This highlights potential differences in TMS interventions for adult and adolescent depression disorders (Croarkin and Rotenberg, 2016). Adolescents with TRD often require multiple psychotropic medications and psychotherapeutic interventions (Dwyer et al., 2020). However, TMS may have a better tolerability and adverse effect profile compared to psychotropic medications, particularly some adjunctive medications that are commonly used in TRD (Dwyer et al., 2020; Hett et al., 2021; Qiu et al., 2023). In our study, adolescents with TRD were maintained without medications for 6 months while receiving TMS monotherapy for up to 30 sessions over 6 weeks if necessary. Minimal side effects were observed during the trial, and TMS was a safe alternative to medication. These findings highlight the potential for developing novel noninvasive neuromodulation alternatives such as TMS for acute and postacute interventions in this population (Croarkin and Rotenberg, 2016).
While this is the largest open-label study of adolescents with TRD managed with TMS retreatment, there are several important limitations. First, this Phase III study was open-label, which limits conclusions regarding the effectiveness of TMS retreatment. Prior and ongoing studies have consistently noted challenges controlling for the nonspecific factors of TMS and high sham response rates (Burke et al., 2022). Second, the inclusion of participants who never received active TMS at any point (group S) requires cautious interpretation. Improvements observed in these patients may be attributable to their natural clinical course or the placebo effects of sham interventions. Third, our study utilized the 5 cm rule for coil localization, which may have affected outcomes. The use of alternative methods, such as the Beam F3 approach (Beam et al., 2009), neuronavigation (Siddiqi et al., 2024), or computational approaches, might have strengthened the results (Croarkin and Opitz, 2024; Deng et al., 2023; Dhami et al., 2023; Siddiqi et al., 2024). Fourth, the conclusions regarding clinical outcomes must be interpreted with caution due to potential influences from the adherence and withdrawal rates observed in this follow-up study. These rates may have been impacted by the monotherapy nature of our protocol and exclusion criteria (Croarkin et al., 2021). However, it is important to note that despite these limitations, the blinding of interventions in phase I and the use of TMS as monotherapy were maintained consistently across all 13 centers throughout the follow-up period. Fifth, the exclusion criteria and protocol may have impacted our findings as while the sample was treatment-resistant, the severity and impairment of the sample was somewhat limited. For example, the time burden of frequent study visits and limitations on suicidal behaviors likely restricted the morbidity of our sample (Strawn et al., 2020). Sixth, using a partial response threshold potentially limits the generalizability of our findings, as insurance companies are currently unlikely to cover a repeat course of TMS for patients attaining only a partial response.
Conclusions
This study expands our understanding of the durability of the clinical benefits of acute TMS for adolescents with TRD. The findings provide support for the feasibility, safety, tolerability, and clinical effectiveness of TMS retreatment over a period of 6 months. Future controlled studies of maintenance TMS protocols for adolescents with TRD are urgently needed. These findings also raise questions about the current approaches to acute TMS treatment for adolescents. Longer, flexible TMS protocols that treat to clinical benefit for adolescents with TRD may be an approach to consider in future research efforts (Croarkin and Rotenberg, 2016; Wilson et al., 2022).
Clinical Significance
TMS has promise in treating adolescents with TRD. TMS is now FDA cleared as an adjunct treatment for adolescents aged 15 years and older with MDD. However, the adolescents with TRD in this study received TMS retreatment as monotherapy over 6 months. The level of treatment resistance did not predict relapse, suggesting equivalent responses even in those who have not responded to antidepressant medications. Fewer symptoms after an acute course of TMS course predicts greater durability, and therefore, emphasizes the need to treat until remission. This is supported by adult data showing the same relationship between acute response and durability (Janicak et al., 2010; Miljevic et al., 2019). Future research and clinical experience to improve the effectiveness of TMS must consider the durability of clinical effects, treatment duration, continuation therapy, and maintenance treatment. A flexible dosing approach could be particularly beneficial. Instead of following the standard 4–6 weeks of acute treatment, adolescents could continue receiving TMS until they show an antidepressant response, with additional sessions as needed. This approach is supported by findings that prior interventions, including sham TMS, active TMS, and the number of sessions, did not significantly impact outcomes at the 6-month mark. Therefore, longer-term TMS monotherapy, with the option for retreatment, may be a valuable approach for adolescents with TRD (Croarkin and Rotenberg, 2016; Wilson et al., 2022).
Footnotes
Acknowledgments
The authors are grateful to the patients and families who participated in the study. The authors would like to acknowledge the participating clinical trial sites and investigative teams: Dothan Behavioral Medicine, Dothan, Alabama; University of California, Los Angeles, Los Angeles, California; Stanford University, Palo Alto, California; Rocky Mountain TMS, Grand Junction, Colorado; Florida Clinical Practice Association, Inc, Gainesville, Florida; Anchor Neuroscience, Pensacola, Florida; Beacon Medical Group, South Bend, Indiana; Integrative Psychiatry, Louisville, Kentucky; Sheppard Pratt Health System, Baltimore, Maryland; Mayo Clinic, Rochester, Minnesota; University of Cincinnati College of Medicine, Cincinnati, Ohio; The Ohio State University, Columbus, Ohio; and Medical University of South Carolina, Charleston, South Carolina.
Authors’ Contributions
J.F.G.: Conceptualization, data analysis, writing, and editing original and subsequent drafts. A.Z.E.: Investigation, data curation, data analysis, writing (review and editing), and project administration. S.T.A.: Investigation, data curation, data analysis, writing (review and editing), and project administration. G.R.S.: Investigation, data curation, data analysis, and writing (review and editing). R.C.H.: Investigation, data curation, data analysis, writing (review and editing), and project administration. S.Z.: Conceptualization, data analysis, writing (review and editing), and project administration. M.A.D.: Conceptualization, investigation, data analysis, writing (review and editing), and project administration. J.R.S.: Investigation, data curation, data analysis, writing (original draft, review, and editing), and project administration. P.E.C.: Conceptualization, investigation, data curation, data analysis, writing (original draft, review, and editing), and project administration.
Disclosure
P.E.C. has received research grant support from the Agency for Healthcare Research and Quality, the National Institutes of Health, the National Science Foundation, the Brain and Behavior Research Foundation, the Mayo Clinic Foundation, Pfizer, Inc.,
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.