
Abstract
Objectives:
Current literature shows a benefit in clinical outcomes when long-acting injectable antipsychotics (LAIAs) are utilized in adult patients with psychiatric disorders such as schizophrenia, schizoaffective disorder, and bipolar disorder. Literature regarding LAIA use in pediatric patients is sparse. The objective of this study is to compare the number of acute psychiatric admissions, psychiatric emergency services (PES) visits, and total number of days admitted to an acute psychiatric hospital 1 year prior to and 1-year post-mirror point of index hospitalization and LAIA initiation.
Methods:
This was a single-site retrospective mirror-image review of patients <18 years of age initiated on an LAIA during an acute psychiatric hospitalization between October 1, 2015, and October 31, 2022. The number of admissions to the acute psychiatric hospital, number of PES visits, and total number of days hospitalized at the acute psychiatric hospital were captured 1-year pre-index hospitalization admission and 1-year post-index hospitalization discharge, with LAIA administration during index hospitalization being the mirror point. Descriptive statistics and a two-tailed paired t-test were utilized to analyze the data.
Results:
There were 45 unique pediatric patients initiated on an LAIA during the specified timeframe. Across these 45 patients, there were 47 psychiatric admissions 1-year pre-index hospitalization and 38 psychiatric admissions 1-year post-index hospitalization discharge (p = 0.37). Additionally, there were 24 PES visits 1-year pre-index hospitalization admission and 16 PES visits 1-year post-index hospitalization discharge (p = 0.25). Finally, across the 45 patients, there were a total of 1040 days admitted to the acute psychiatric hospital in the 1-year prior to index hospitalization admission compared with 774 days admitted to the acute psychiatric hospital in the 1-year post-index hospitalization discharge (p = 0.48).
Conclusions:
In this cohort of pediatric patients initiated on an LAIA, there was a positive trend favoring LAIA therapy over oral antipsychotic therapy with LAIA injection as the mirror point; however, there was no statistically significant difference in the number of psychiatric admissions, number of PES visits, or total number of days admitted to an acute psychiatric hospital. Further studies are required to fully understand the impact of LAIA therapy on clinical outcomes for child and adolescent patients with psychiatric disorders.
Introduction
Long-acting injectable antipsychotics (LAIAs) are a well-established treatment option for adult patients with schizophrenia, schizoaffective disorder, and bipolar disorder with several studies showcasing increased adherence rates, reduced hospitalizations, and an overall reduction in healthcare costs with LAIA utilization (Correll et al., 2017; Park et al., 2018; Huang et al., 2021; Thaman et al., 2024). Mirror-image study designs, where outcomes are compared within the same patient prior to and after an intervention, have previously been used to compare clinical outcomes between oral antipsychotic therapy and LAIA therapy in adult patients. These mirror studies have shown favorable clinical outcomes for LAIA therapy (Kishimoto et al., 2013; Kishimoto et al., 2021; Boyer et al., 2023).
Despite robust evidence supporting LAIA use in adult patients, literature documenting the clinical outcomes of LAIA utilization in pediatric patients is limited. There are currently no LAIAs approved by the Food and Drug Administration for use in the pediatric population; however, there are reports of off-label use (Pope and Zaraa, 2016; Ceylan et al., 2017; Lytle et al., 2017; Fortea et al., 2018; Moon et al., 2023; Sun et al., 2024). A recent retrospective study published by Chowdhury et al. found a statistically significant reduction in hospitalizations at 1-year for pediatric patients on LAIA therapy compared with oral antipsychotic therapy, with trends toward decreased length of stay and fewer adverse effects in the LAIA cohort (Chowdhury et al., 2024).
Previously, our study group analyzed a cohort of 45 pediatric patients initiated on an LAIA. In this study, we reported on initiation and maintenance LAIA dosing strategies, 6-month rehospitalization rates, length of stay, reported adverse effects, and LAIA treatment retention (Sun et al., 2024). This previous study provided a descriptive report of these patients and did not have a focus on comparing outcomes of patients prior to and after initiating LAIA therapy. There is a need for more literature to further understand the clinical outcomes associated with LAIA therapy in pediatric patients.
To date, there have been no mirror studies looking at LAIA utilization in pediatric patients with psychiatric disorders. The primary objective of this study is to compare the number of acute psychiatric admissions 1-year prior to index hospitalization admission, when LAIA therapy was initiated, and 1-year post-index hospitalization discharge. Secondary outcomes include the number of psychiatric emergency services (PES) visits and total number of days admitted to the acute psychiatric hospital 1-year prior to index hospitalization admission and 1-year post-index hospitalization discharge.
Materials and Methods
This was a single-site retrospective mirror-image review of patients <18 years of age discharged from an acute psychiatric hospital between October 1, 2015, and October 31, 2022. This study was reviewed and approved by the institution’s Quality-Improvement Review Committee. Patients were included if they were newly initiated on one of the following LAIA agents: aripiprazole lauroxil (Aristada®), aripiprazole monohydrate (Abilify Maintena®), olanzapine pamoate (Zyprexa Relprevv®), paliperidone palmitate (Invega Sustenna®), risperidone microspheres (Risperdal Consta®), risperidone subcutaneous (Perseris®), haloperidol decanoate (Haldol Decanoate®), and fluphenazine decanoate (Prolixin Decanoate®). All patients were treated with the parent oral antipsychotic during the index hospitalization and were deemed appropriate candidates for LAIA therapy based on clinical efficacy and tolerability. Parent oral antipsychotic is defined as the oral formulation of the LAIA that was administered, with paliperidone and risperidone being categorized as the same parent oral antipsychotic compound. Additionally, all patients were confirmed to have active prescription insurance coverage, and all necessary insurance authorizations were obtained prior to LAIA initiation. Electronic chart review was performed to obtain patient demographics including age on admission, sex, and race. Primary diagnosis at discharge via International Classification of Diseases (ICD)-10 codes, hospital admission and readmission data, and PES encounter information were also captured.
Given the mirror-image design of the study, patient outcomes were captured prior to and immediately following the mirror point, defined as LAIA initiation during the index hospitalization (see Fig. 1). The primary outcome of this study was the number of acute psychiatric hospital admissions in the 1-year prior to index hospitalization admission compared with the number of acute psychiatric hospital admissions in the 1-year post-index hospitalization discharge. Secondary outcomes include the number of PES visits and total number of days hospitalized at the acute psychiatric hospital 1-year pre-index hospitalization admission versus 1-year post-index hospitalization discharge. Descriptive statistics and a two-tailed paired t-test were performed in Microsoft Excel® to analyze baseline demographic information and outcomes data.
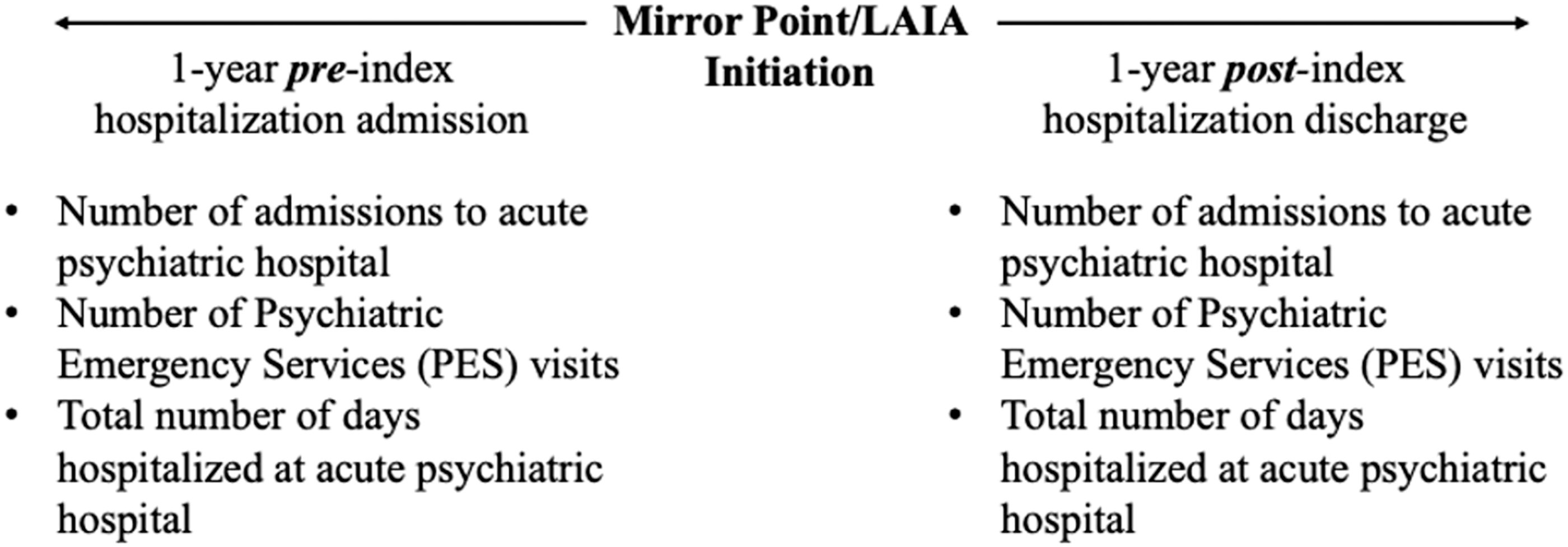
Methods.
Results
Patient demographics
There were 6402 unique pediatric patients admitted to the acute psychiatric hospital between October 1, 2015, and October 31, 2022. Of those 6402 patients, 54 patients received an LAIA during their hospitalization. Nine patients were excluded due to previous LAIA therapy, resulting in 45 patients included in the study and the analysis. The average age of the 45 included patients was 15.6 years, with the youngest patient being 10 years of age. Sex and race were reported by the patient and clinician-documented in the electronic health record with the majority of patients identifying as Black or African American (n = 27, 60%) and male (n = 26, 57.8%).
There was a wide variation in number of oral antipsychotics trialed prior to LAIA initiation; 10 patients (22.2%) had not received the parent oral antipsychotic compound prior to index hospitalization. Seventeen patients (37.8%) had trialed another oral antipsychotic prior to LAIA initiation. Nine patients (20%) had trialed two other oral antipsychotics and, similarly, nine patients (20%) had trialed three or more other oral antipsychotics prior to LAIA initiation.
The most commonly initiated LAIA was paliperidone palmitate (n = 21, 46.7%), followed by aripiprazole lauroxil (n = 15, 33.3%) and aripiprazole monohydrate (n = 7, 15.6%). One patient each was initiated on haloperidol decanoate (n = 1, 2.2%) and risperidone microspheres (n = 1, 2.2%). Additional demographic information can be seen in Table 1.
Baseline Demographics
Baseline demographic information of included patients.
Paliperidone and risperidone categorized as same parent antipsychotic compound.
Additional scheduled oral antipsychotic at discharge that differed from parent compound of LAIA.
Selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors included.
Community discharge arrangement includes home and with child, youth, and family services. Step down discharge arrangement includes residential treatment facility.
ICD-10, International Classification of Diseases, 10th Revision; LAIA, long-acting injectable antipsychotic.
Primary outcomes
Across the 45 included patients, there were a total of 47 acute psychiatric hospitalizations in the 1-year prior to index hospitalization admission, compared with 38 acute psychiatric hospitalizations in the 1-year post-index hospitalization discharge (p = 0.37). The number of admissions was further divided into 1–90 days, 91–180 days, and 181–365 days from index hospitalization, as seen in Figure 2. At each of the time points, there was a trend, although nonsignificant, favoring LAIA therapy.
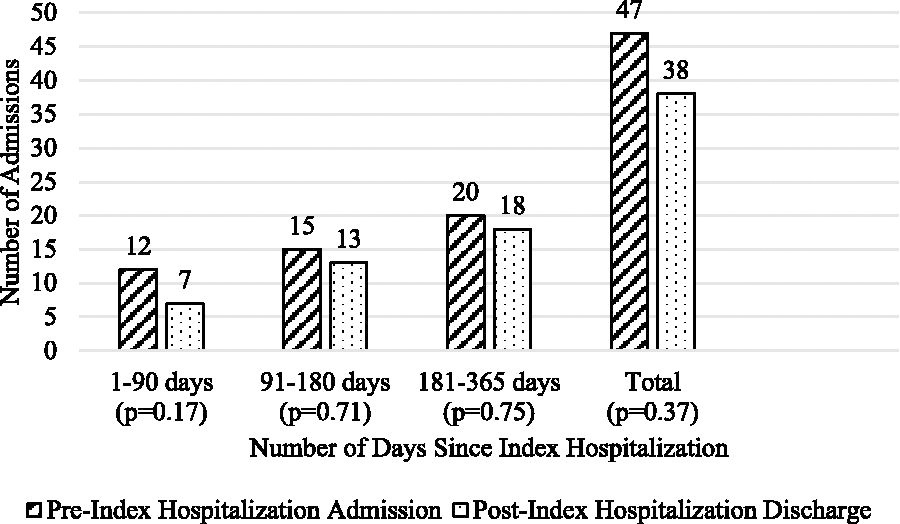
Primary outcome—number of psychiatric admissions 1-year pre-index hospitalization admission versus 1-year post-index hospitalization discharge.
Secondary outcomes
Secondary outcomes are shown in Table 2. There were a total of 24 PES visits in the 1-year prior to index hospitalization admission, compared with 16 PES visits in the 1-year post-index hospitalization discharge (p = 0.25). Regarding total number of days admitted to the acute psychiatric hospital, across all 45 patients there were a total of 1040 days admitted 1-year pre-index hospitalization admission compared with 774 days admitted 1-year post-index hospitalization discharge (p = 0.48).
Secondary Outcomes—Number of PES Visits and Number of Days Admitted to Acute Psychiatric Hospital 1-Year Preindex Hospitalization Admission Versus. 1-Year Postindex Hospitalization Discharge
Secondary outcomes, comparison of PES visits and total days admitted to acute psychiatric hospital in the 1 year prior to index hospitalization admission (prior to LAIA therapy) and in the 1-year post-LAIA initiation (after LAIA has been initiated).
LAIA, long-acting injectable antipsychotic; PES, psychiatric emergency services.
Discussion
In this retrospective mirror-image review of pediatric patients initiated on an LAIA, there were positive trends toward a reduction in the number of acute psychiatric admissions, PES visits, and days admitted to an acute psychiatric hospital; however, these trends did not reach statistical significance. These results align with current literature regarding clinical outcomes for pediatric patients initiated on LAIA therapy. A recent retrospective chart review published by Chowdhury et al. yielded similar results, concluding that patients initiated on LAIA therapy had a numerical reduction in hospital admissions and length of stay compared with propensity-matched patients on oral antipsychotic therapy. Their study showed statistical significance for cumulative readmissions at the 1-year mark, however, all other outcomes only showed favorable trends (Chowdhury et al., 2024).
There was a large range in the number of antipsychotics previously trialed prior to LAIA initiation. Ten patients (22.2%) had only ever received treatment with the parent oral antipsychotic, whereas nine patients (20%) had previously trialed three or more different antipsychotic compounds prior to LAIA initiation. This large variation indicates varying levels of illness severity between the cohort of patients, emphasizing that there is no clear place where LAIAs fit into therapy for pediatric patients. Most patients (95.6%) had a history of nonadherence to outpatient medications or a concern for nonadherence documented during index hospitalization. This is similar to what would be expected in the adult population, where nonadherence can be a primary driving factor for selecting LAIA therapy (Keepers et al., 2020).
There are a few notable limitations to this study. First, this was a retrospective chart review that had a relatively small sample size. While other pediatric LAIA studies had similar sample sizes, the number of patients included in this study is significantly smaller than the patient population seen in comparable studies in the adult population. Given the small sample size, subanalysis regarding specific patient characteristics and LAIA agents was not feasible. Moreover, this was a single-site study that only captured admissions and PES visits to one singular acute psychiatric hospital. Psychiatric hospital admissions and PES utilization at different institutions were not included in this study. Additionally, this study was one-directional in analysis, comparing outcomes for patients prior to and after LAIA initiation. This study did not look at the change in clinical outcomes for patients previously on LAIA therapy who transitioned to oral antipsychotic therapy. Lastly, the retrospective mirror-image study design may not have truly compared equivalent oral antipsychotic therapy with LAIA therapy, as not all patients had been on the parent oral antipsychotic prior to index hospitalization. Other factors, such as a more robust therapeutic response to one antipsychotic compared with another, may confound the outcomes captured. Further studies are required to fully understand the impact of LAIA therapy on clinical outcomes for pediatric and adolescent patients with psychiatric disorders.
Conclusions
In this cohort of pediatric patients initiated on an LAIA, there was a positive trend favoring LAIA therapy over oral antipsychotic therapy with LAIA injection as the mirror point; however, there was no statistically significant difference in the number of psychiatric admissions, the number of PES visits, or the total number of days admitted to an acute psychiatric hospital.
Clinical Significance
To our knowledge, this is the first retrospective mirror-image review of LAIA utilization in the pediatric population. This study provides insight into the potential benefits of LAIA therapy in improving clinical outcomes. Given the limited knowledge on this topic, we hope to contribute to the literature and facilitate discussion regarding place in therapy of LAIA in pediatric patients with psychiatric disorders.
Authors’ Contributions
All authors were involved in and contributed to the development of this manuscript.
Footnotes
Disclosures
No competing financial interests exist, and none of the authors have any conflicts of interest to disclose.