
Abstract
Background:
Approximately 20%–40% of individuals with Tourette syndrome (TS) have rage attacks (RAs), which are recurrent, explosive behavioral outbursts that can cause significant functional impairment. Despite the impact of RA in TS, there has been limited research on treatment, and most studies have focused on pharmacologic interventions. Nonpharmacologic interventions have the potential to improve symptoms with fewer side effects. Mightier, a video game-based biofeedback therapy, may help teach emotional regulation through heart rate control and has the potential to improve RA in youth with TS.
Objective:
To evaluate the feasibility and acceptability of Mightier as a therapeutic intervention for RA in youth with TS.
Methods:
Subjects aged 6–12 years old with a diagnosis of TS and RA were enrolled between October 2021 and May 2022 into a 20-week single-arm trial. Feasibility was assessed by the rate of enrollment, screen failures, and retention and device engagement. We also evaluated efficacy by assessing rage severity (Clinical Global Impressions of Rage), Rage Outbursts and Anger Rating Scale (ROARS) and overall aggression severity (Modified Overt Aggression Scale [MOAS]) pre- and postintervention. CGI-Improvement (CGI-I) was completed postintervention.
Results:
We enrolled 11 participants. The study was feasible based on enrollment rate (one participant every 2.5 months), screen failures (n = 1), and retention rate (91%). Mean weekly play time was 38 (SD 18) minutes/week. No adverse effects were reported. Median rage severity scores improved across all assessment measures. All participants reported overall improvement on the post-intervention CGI-I.
Conclusions:
This Mightier study was feasible in terms of recruitment and retention. Participants with TS and RA used the device often and engaged with the device throughout the 12-week intervention period. Rage severity overall improved across the various outcome measures, and all participants had at least some improvement by parent report. Mightier may be a helpful tool for reducing rage severity in children with RA and TS.
Introduction
Rage attacks (RA) (repeated anger-generated episodes) are severe, recurrent, impulsive outbursts of verbal and/or physical aggression that are present in 20%–40% of people with Tourette syndrome (TS) (Budman et al., 1998; Chen et al., 2013; Coccaro, 2012). TS is a neuropsychiatric disorder characterized by childhood onset of motor and phonic tics. Although not part of the definition of TS, nonmotor symptoms such as attention-deficit/hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD), anxiety disorders, and disruptive behavior disorders are common. Disruptive behavior disorders, such as RA, lead to increased family distress, impaired school function, social difficulties, or a combination. These impacts are costly to the public health system and may lead to increased rates of psychiatric hospitalization (Budman et al., 2008; Sukhodolsky et al., 2003). Parents report that RA are the most concerning symptom for their families (Dooley et al., 1999), which may augment stress and health impacts on caregivers.
Pharmacologic treatment for RA may include medications commonly used to treat impulsivity (e.g., alpha-2 agonists), anxiety and OCD (e.g., selective serotonin reuptake inhibitors), or impulsive aggression (e.g., atypical antipsychotic medications). Unfortunately, the strength of data on pharmacologic management of RA has been limited by retrospective study design (Budman et al., 2008) and uncontrolled trials (Budman et al., 1998; Budman et al., 2001). For example, in a retrospective study of aripiprazole in 29 youth with RA and TS, RA severity improved in most participants (Budman et al., 2008). However, adverse effects such as weight gain were common. In a single-arm trial of paroxetine in 45 children and adults with RA and TS, most (76%) reported decreased frequency of RA at the end of 8 weeks (Budman et al., 1998). However, 16% of participants did not complete the trial either due to side effects or worsened RA. These studies underscore the risk of adverse effects from medication use. In addition, medications do not teach children skills for managing their emotions. Thus, nonpharmacologic interventions are important considerations in this population. For example, anger control training (ACT) is a nonpharmacologic approach that may be beneficial for disruptive behaviors in TS (Sukhodolsky et al., 2009). ACT typically includes modules on arousal management, cognitive restructuring, and behavioral practice. The arousal management modules incorporate skills, such as deep breathing. ACT was more effective than usual treatment in a study of adolescents with TS and disruptive behaviors. While ACT may be promising for RA in TS, the primary outcome measures in this trial did not specifically assess RA. In addition, access to ACT may be limited based on low availability of trained therapists and financial barriers.
Self-directed, nonpharmacologic strategies that employ arousal management skills from ACT may be beneficial in youth with RA and TS. Perhaps the best-known self-directed strategy is biofeedback, which teaches the individual to control physiological variables, such as heart rate (Medicine SoI, 2016). An RCT of biofeedback for TS showed that biofeedback was not more effective than placebo in reducing tic severity (Nagai et al., 2014). However, biofeedback may be effective in treating mental health disorders that commonly co-occur in youth with TS. For example, biofeedback reduced disruptive classroom behaviors in a small group of adolescents (Bossenbroek et al., 2020) and reduced anxiety and mood symptoms in adolescents with migraines and comorbid anxiety and depression (Minen et al., 2021).
Most youth with RA have symptoms of autonomic activation, such as a reddening face, sweating, racing heart, and shaking during an episode (Budman et al., 2003). Therefore, we hypothesized that a biofeedback-based intervention targeting autonomic symptoms may reduce RA in youth with TS by teaching arousal management skills. Home-based interventions may be more accessible and cost-effective than clinic-based interventions (Burke and Andrasik, 1989). In addition, home-based biofeedback treatment may be as effective as clinic-based biofeedback treatment (Burke and Andrasik, 1989; Guarnieri and Blanchard, 1990). In home-based programs, children can practice biofeedback exercises without missing school for frequent clinic appointments. This can also be a helpful option for families who do not live close to an experienced biofeedback clinician.
Mightier, a video game-based intervention, is a safe and engaging tool that can decrease aggressive symptoms in children (Ducharme et al., 2021; Kahn et al., 2013; Kahn et al., 2009). Mightier is an innovative platform that teaches emotional regulation through heart rate control (Ducharme et al., 2012; Kahn et al., 2013). Players wear a heart rate monitor; when their heart rate increases, the game difficulty rises. Players use relaxation techniques that they learn within the game to reduce their heart rate and make the game easier to play. Mightier has been evaluated in youth with oppositional defiant disorder, ADHD, and anxiety disorders (Ducharme et al., 2021), which are common co-occurring conditions in TS (Hirschtritt et al., 2015; Kurlan et al., 2002). We performed a pilot trial with the primary aim to assess the feasibility of using Mightier to treat RA in children with TS. The secondary aim was to gather preliminary data on potential efficacy.
Methods
Participants
Participants were recruited from the University of Rochester Tourette Association of America Center of Excellence. Children aged 6–12 years old with a diagnosis of TS and at least 4 RA per month were eligible for inclusion. Children with other potential etiologies for RA, such as autism spectrum disorder or a history of abuse, were excluded. Participants could be on medications to treat tics, RA, or both, but dosing had to be stable for at least 4 weeks prior to the start of the study and expected to be stable throughout the study. Children receiving psychotherapy for RA were also excluded. This study was approved by the IRB at the University of Rochester. Parental permission and child assent (for participants ≥8 years) were obtained for all participants.
Study design
This was a 20-week, single-arm feasibility study assessing the use of Mightier in children with RA and TS. The study was conducted remotely via teleresearch. The study consisted of three phases (Fig. 1): Preintervention, intervention, and postintervention. Participants completed a 4-week preintervention phase during which parents tracked RA. Parents documented RA on a calendar, indicating when RA occurred and the duration and intensity (mild, moderate, or severe) of each episode. The PI reviewed the calendar with the parent at the baseline study visit and asked parents to describe the RA to confirm that episodes were consistent with RA. This information was used to inform scoring on rage outcome measures. At the end of the preintervention phase, a baseline assessment was completed to evaluate the severity of RA, tics, and symptoms of ADHD and OCD. Participants were connected to a Mightier coach, a member of the Mightier team, who provided technical guidance on the setup and use of the tablet and armband. The coach also gave helpful tips on how to help children engage with the games. Participants were given a play goal of 45 minutes per week over the course of 12 weeks and told that additional exposure to the intervention was acceptable. During the 12-week intervention phase, weekly play and cooldowns were tracked. Cooldowns represent a child’s ability successfully to bring their heart rate from an elevated level back to baseline. If playtime was lower than the expected 45 minutes, families were contacted to discuss and troubleshoot any barriers to play. Parents also met with the coach at weeks 4 and 8 during the intervention phase to review barriers to play, unexpected treatment changes, and adverse effects. After the intervention phase, the parent again tracked rage frequency, duration, and severity on a calendar over the next 4 weeks. A postintervention assessment was completed to evaluate the severity of RA, tics, and symptoms of ADHD and OCD in addition to the overall impression of improvement. A semi-structured questionnaire was also administered by a study team member to assess parent and child feedback of the device and study design.
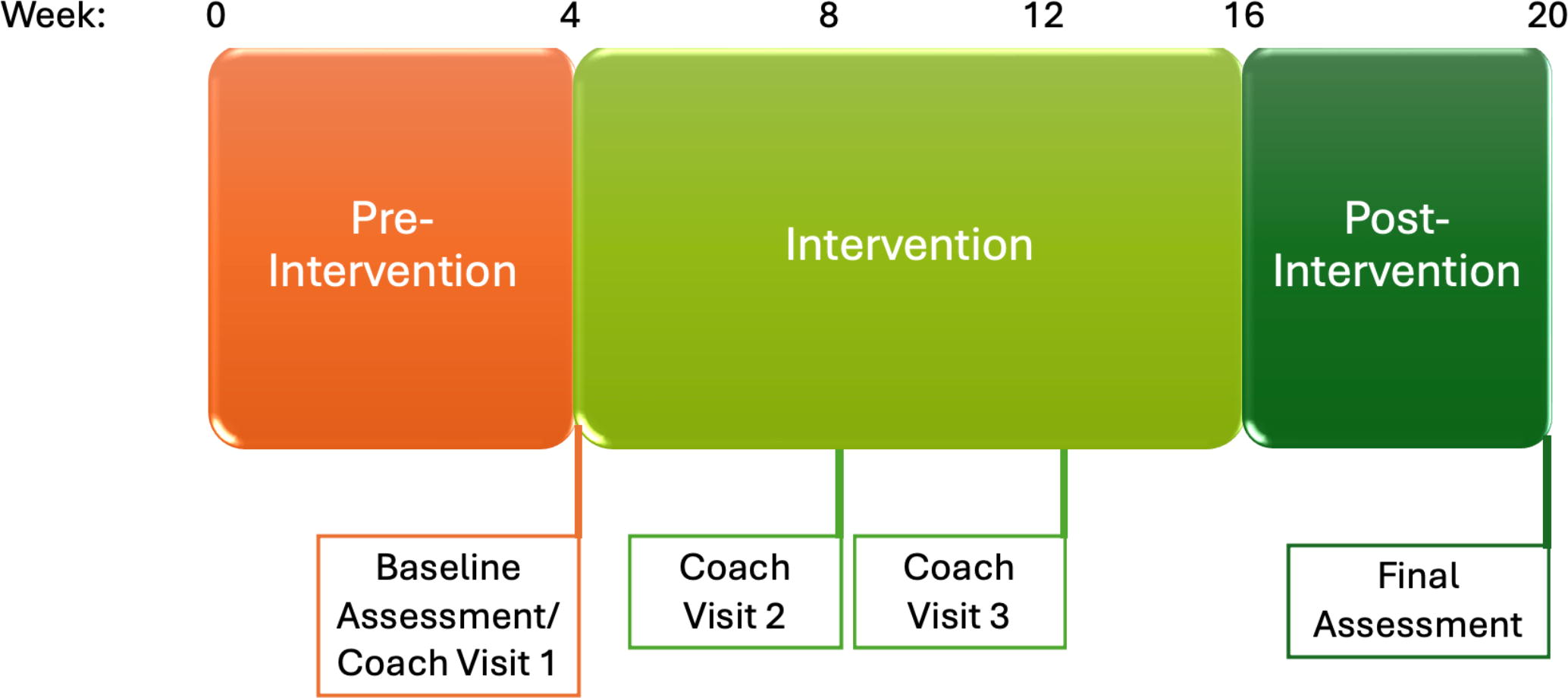
Schematic of trial design. Preintervention: the parent tracked rage attacks for 4 weeks. Intervention: the child used Mightier for 12 weeks and parent completed 2 coaching visits. Postintervention: the parent tracked rage attacks for 4 weeks.
Study measures
Feasibility
To assess feasibility of studying Mightier in TS, we measured rate of enrollment, screen failures, and retention. We also assessed engagement with the device by tracking weekly minutes played and cooldowns. To assess tolerability, we assessed for adverse effects at each coaching visit. We also conducted a semi-structured interview of the parent and child at the final study visit. We asked how likely each one would be to recommend Mightier for kids with RA and TS, whether Mightier was helpful and barriers to using Mightier. We also asked for feedback on the study design.
Rage severity
There is not a gold standard for assessing rage severity for children with TS; thus, we used multiple scales to assess rage and aggression. The Clinical Global Impression-Rage (CGI-Rage) is a clinician-rated 6-point scale evaluating the average frequency of RA over the prior month (Budman et al., 2008). A score of 1 indicates no RA, and a score of 6 indicates severe rage with RA occurring multiple times daily. A CGI-Rage difference of one point is considered clinically significant (Budman et al., 2008). The Rage Outbursts and Anger Rating Scale (ROARS) is a clinician-rated measure of RA that assesses frequency, intensity, and duration of RA over the past week (Budman et al., 2008). Scores range from 0–9. Clinicometric properties and minimal clinically meaningful change values have not been reported for the ROARS, which has been used in previous intervention studies for RA. (Storch et al., 2012; Wu and Storch, 2015) The Modified Overt Aggression Scale (MOAS) is a clinician-rated measure of the frequency and severity of aggressive episodes over the prior week. It is not specific to RA but encompasses all causes of verbal or physical aggression (Yudofsky et al., 1986). Scores range from 0 to 40 with higher scores indicating more severe aggression. Parents rated improvement based on the CGI-Improvement (CGI-I) scale, a 7-point scale evaluating change since the start of treatment. This was administered only at the final study visit.
Tics and co-occurring conditions
Tic severity was assessed using the Yale Global Tic Severity Scale-Total Tic Score (YGTSS-TTS). The YGTSS is a clinician-administered tool based on interview and direct observation of the child. It assesses the number, frequency, intensity, complexity, and interference of motor and vocal tics, based on defined anchor points (Leckman et al., 1989). Total tic scores (TTSs), overall impairment ratings, and global severity scores are generated. We focused on the TTS as a measure of tic severity. This scale has established validity and is considered the best currently available scale to rate the severity of tics (Leckman et al., 1989).
ADHD symptom severity was assessed using the Swanson, Nolan, and Pelham Questionnaire IV (SNAP-IV), a 40-item parent-proxy assessment of hyperactivity, impulsivity, and inattention, which are key symptoms of ADHD, in accordance to the DSM-IV (Bussing et al., 2008). It is validated for use in children of age 6–18 years. The short form is not currently available for symptoms in accordance with the DSM-5.
OCD symptom severity was assessed using the Children’s Yale-Brown Obsessive Compulsive Scale (CY-BOCS), a clinician-administered instrument (Scahill et al., 1997). This scale is the most widely used instrument to assess the presence, type, and severity of obsessive-compulsive symptoms in research studies involving children. It is validated for use in children of age 6–17 years. It includes a checklist of specific obsessions and compulsions, followed by examiner ratings of time spent, interference, distress, resistance, and control over obsessions and compulsions. Examiner ratings are independently based on the interview with the child and parent. The CY-BOCS has well-established psychometric properties (Scahill et al., 1997).
Statistical analysis
Statistical analyses were completed using JMP Pro 17.0. Descriptive statistics, including mean, median, standard deviation (SD), and range, were used for demographic variables and symptom severities at baseline and final study visits. Engagement data were normally distributed; thus, mean (SD) statistics were analyzed. Data were assessed by mean minutes/week, mean cooldowns/week, and change in minutes/week and cooldowns/week from weeks 1 to 12. Preliminary efficacy was assessed by mean (SD) and median (range) changes in CGI-Rage, ROARS, and MOAS and by mean (SD) and median (range) CGI-I score. Pre- and postintervention score for RA and TS-related symptoms were compared by the Wilcoxon Rank Sums test.
Results
Participant demographics
We enrolled 11 participants and have demographic and symptom baseline data on 10 participants (Table 1) due to one screen failure. Most participants were male (n = 9, 91%) with a mean age at enrollment of 8.6 (SD 1.8) years. The median age at onset of RA was 4 (range 2–10) years. Prior to the intervention phase, participants had moderate rage severity (CGI-Rage median 4, range 2–5) and moderate tic severity (median YGTSS-TTS 21.5, range 19–39). Co-occurring diagnoses such as ADHD (n = 6), OCD (n = 4), and/or anxiety disorder (n = 5) were common. Only one participant did not have any of these co-occurring conditions. On the SNAP-IV ADHD assessment, parents reported elevated scores in the inattention (median 1.6, range 0.7–2.1), hyperactive/impulsive (median 1.7, range 0.9–2.3), and combined (median 1.6, range 0.8–2.1) subscales. OCD symptoms were moderately severe (median 16, range 0–28).
Participant Demographics
ADHD, attention-deficit/hyperactivity disorder; OCD, obsessive-compulsive disorder.
Feasibility and engagement
We screened 18 subjects and enrolled 11. Those who did not enroll either did not have current RA (n = 1), had recent medication/therapy changes (n = 2), or were not interested in participating (n = 4). The 11 participants were enrolled over the course of 28 months for an average enrollment of one participant every 2.5 months. One participant screen-failed due to resolution of his RA during the preintervention phase. One participant withdrew during the intervention phase due to impairing anxiety after he suddenly discontinued his anxiety treatment. Retention was high with nine participants completing the trial (90%). For these participants, all visits were attended and completed successfully.
Participants engaged with Mightier during the intervention period. Over the course of the 12-week intervention phase, participants played a mean of 459 (SD 211) minutes total. Mean weekly play time was 38 (SD 18) minutes/week, playing a mean of 2.2 (SD 0.6) days/week. In addition, participants were able to successfully cool down while playing. They completed a mean of 36 (SD 15) cooldowns/week. Individual participant weekly play and cooldowns are shown in Figure 2.

Individual participant data of weekly play
Participants tolerated Mightier without adverse effects. Tic severity (Z = 0.13, p = 0.89), OCD symptom severity (Z = 0.80, p = 0.43), and ADHD symptom severity (Z = 0.22, p = 0.82) did not significantly change over the course of the trial. On a Likert scale from 1 (not at all recommend) to 5 (definitely recommend), the median parent score was 4.3 (range 4–5), and the child score was 3.8 (range 3–4). Positive aspects per parent report were that it helped to improve RA and to teach strategies for self-regulation. However, multiple parents also noted that their child became bored with the game over the course of the study. Barriers to using Mightier included competing technology, such as other video games, boredom, and easy frustration with the games. One participant reported being bothered by the texture of the armband, requiring changing positions of the band. Despite these barriers, most parents reported a plan to continue using Mightier.
Change in RA
Median preintervention rage severity was 4 (range 2–5) on the CGI-Rage, 5 (range 4–8) on the ROARS, and 14 (range 3–17) on the MOAS. Median postintervention rage severity was 3 (range 1–5) on the CGI-Rage, 4 (range 0–8) on the ROARS, and 13 (range 1–18) on the MOAS. Individual participant scores are shown in Figure 3. Median CGI-I postintervention was 2, which indicates “much improved” (range 1–3). Each subject’s parent reported that Mightier was helpful. Specifically, two parents reported a decrease in rage severity (frequency, intensity, and/or duration). Three parents reported that their child was able to recognize frustration feelings and use self-regulation tools. Five children reported that the device helped them calm down.
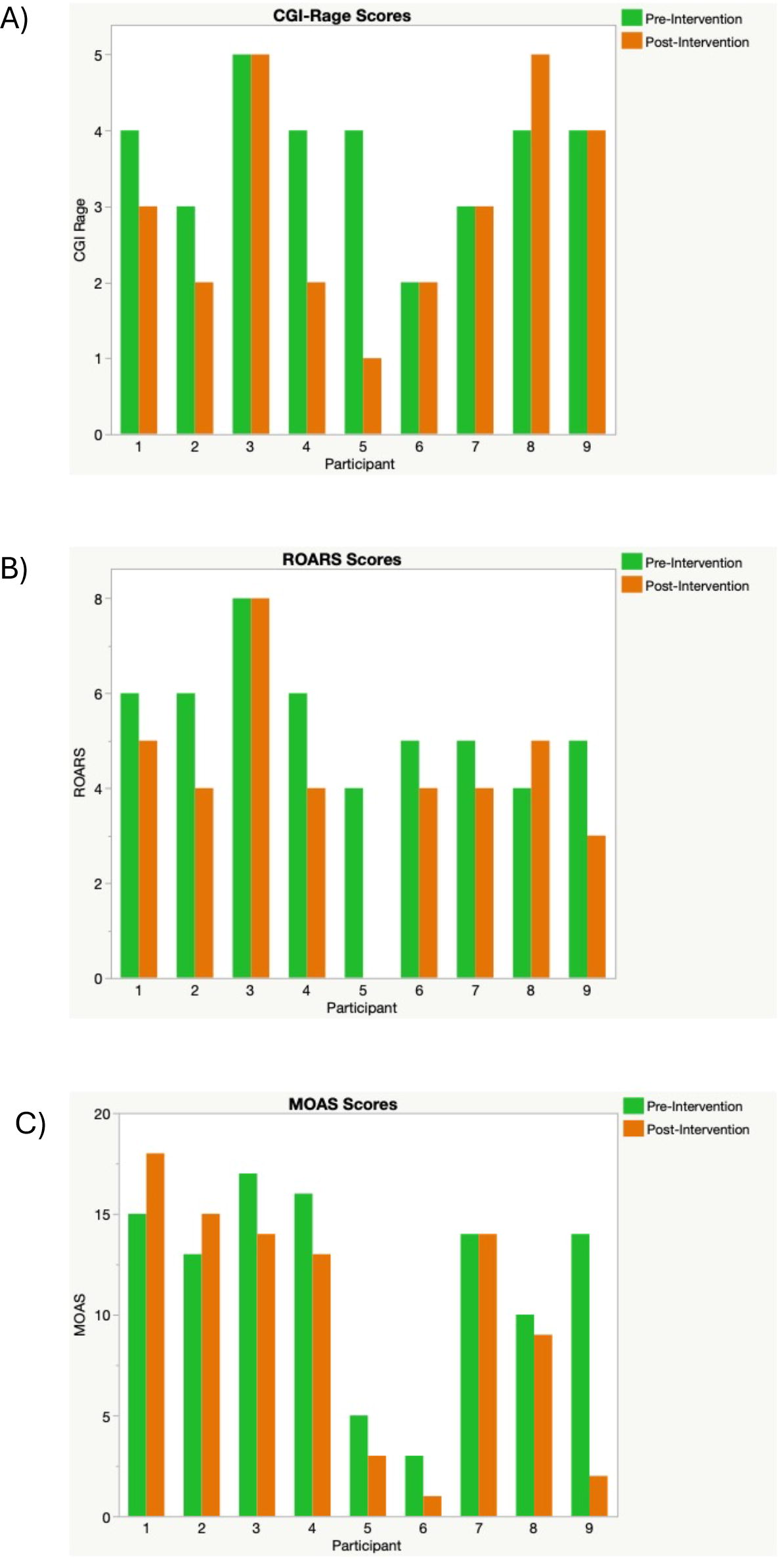
Individual participant Pre- and Post assessment scores for CGI-Rage
Discussion
This feasibility trial tested the use of a biofeedback-based video game device in children with RA and TS. We fulfilled our primary objectives to assess feasibility and engagement with the device. We demonstrated that recruitment into this study was feasible with excellent retention, only one screen failure, and one withdrawal unrelated to the intervention. Participants demonstrated excellent engagement with the device over the 12-week period as demonstrated by minutes played and cooldowns. Our results provide preliminary evidence that the device may improve RA, particularly in this sample of children who mostly had mild to moderate rage severity.
Although the neurobiology underlying RA is incompletely understood, physiological arousal does occur clinically. Most children with TS experience an elevated physiological state during RA, manifested by elevated heart rate and psychomotor agitation (Ashurova et al., 2021; Budman et al., 2003) and followed by feelings of physical and emotional calm after the outburst (Ashurova et al., 2021). Neurobiologic studies support the role of the autonomic nervous system in aggressive explosive outbursts, with the hypothalamus playing a critical role in autonomic activation (Rizzi et al., 2021). Indeed, lesions to the bilateral posterior hypothalamic regions were previously used to treat severe aggression in patients (Rizzi et al., 2021). In addition, impulsive aggression that is seen in RA may be related to overexcitation from an overactive amygdala and/or lack of inhibition from underactive frontal cortices (Nassif and Felthous, 2022). A functional MRI (fMRI) study in adults with explosive anger outbursts demonstrated reduced activity in the prefrontal cortex and elevated activity in the amygdala (Fanning et al., 2017). In a separate fMRI study, patients with RA and TS demonstrated decreased connectivity in the sensorimotor cortico-basal ganglia network, including abnormal connectivity between the amygdala and related structures (Atkinson-Clement et al., 2020). Biofeedback may impact the networks implicated in explosive outbursts. For example, techniques such as controlled breathing may activate sensory afferents of the vagus nerve, which can affect the prefrontal cortex, hypothalamus, amygdala, and hippocampus through nucleus tractus solitarius projections (Raad et al., 2021). Thus, learning to manage one’s physiological arousal response through biofeedback has the potential to affect brain areas implicated in RA.
Biofeedback is designed to improve control of one’s physiological state. With Mightier, children learn to decrease their heart rate using relaxation techniques. Parents reported that deep breathing exercises were most frequently used. While deep breathing may seem simple, learning this skill through digital interventions, such as video games, may make skill-building more accessible and appealing to children (Prins et al., 2011; Wols et al., 2024). In addition, games can provide high intensity and immediate feedback on skill use (Jaeggi et al., 2014) alongside an environment in which to safely and repeatedly practice. Applied games such as Mightier employ game design to make interventions more engaging, motivating the player to change their behaviors (Wols et al., 2024). Video game-based treatments can be engaging and effective for children. In a review of RCTs evaluating video games for pediatric mental health conditions, video games were as effective or more effective than active control treatments in most studies across a range of disorders (Wols et al., 2024).
Data on effective medications for RA in TS are limited. In addition, because TS is associated with multiple co-occurring neuropsychiatric conditions, current treatment strategies commonly employ psychotropic polypharmacy, which can lead to potentially irreversible side effects (Scahill et al., 2006). Prescriptions for pediatric psychotropic medications have increased substantially in recent decades, leading to calls by groups such as the American Academy of Pediatrics for deprescribing in children (Barnett et al., 2020). Evidence-based nonpharmacologic management strategies may reduce or eliminate the use of multiple psychotropic medications in children with TS. Furthermore, teaching self-regulation skills may improve long-term outcomes for children. Indeed, developing emotional self-regulation skills is critical to child development. Poor emotional self-regulation is linked to the development of mental health disorders and is associated with worse school performance (Graziano et al., 2007; Wyman et al., 2010). Thus, it is important to investigate potential nonpharmacologic options for children with complex neurodevelopmental disorders, such as TS.
There were limitations to our study. The sample size was small, and the trial was not powered to determine efficacy. In addition, because there was no control group for comparison, we are not able to account for a potential placebo effect. The study assessed outcomes after completing a 12-week intervention, but we do not have data on lasting effects. Finally, there is not a specific, validated tool to assess rage severity in children. We used multiple tools employed in other rage treatment studies, but each tool has potential limitations to its use. We found that the ROARS was most helpful because it assessed frequency, severity, and duration of RA rather than a global impression score. Despite these limitations, this study adds important information about potential home-based, nonpharmacologic treatment options for children with RA and TS.
Conclusions
The primary aim of the study was to assess feasibility, which is a key step to designing a future efficacy trial. We were able to determine that both the study design, particularly the fully remote approach, and the intervention were feasible in this cohort. Further studies on treatment approaches for RA in TS are critically important to the TS community. These data will provide the foundation for a larger efficacy trial for biofeedback-based treatment for RA.
Clinical Significance
RAs are common in TS and evidence-based studies on treatment approaches are lacking. In this feasibility trial of a biofeedback-based videogame device, we demonstrate that the study design and intervention were feasible in this population. This study may pave the way for a larger efficacy trial to test this device in youth with RA and TS.
Footnotes
Acknowledgments
Preliminary data from this study were previously presented in poster format at the Annual American Academy of Neurology Conference (2023) and the Annual Child Neurology Society Meeting (2024).
Disclosures
Nicole Walsh has nothing to disclosures.
Matthew Tae has nothing to disclosures.
J.K., J.R., E.S., and A.P. report salary and equity from Neuromotion Inc., outside the submitted work. In addition, J.K. has a pending patent US20140323013A1: Emotional control methods and apparatus licensed.
J.W.M. serves a consultant for Neurogene, Inc. He serves on a central rating committee for Emalex, Inc. He serves on a Data and Safety Monitoring Board for PTC Therapeutics.