
Abstract
Introduction:
Despite advances in obstetric care, postpartum hemorrhage (PPH) is a leading cause of maternal mortality worldwide. Prior reviews of studies published through 2016 suggest an association of antidepressant use during late pregnancy and increased risk of PPH. However, a causal link between prenatal antidepressants and PPH remains controversial.
Objectives:
This systematic literature review aimed to synthesize the empirical evidence on the association of antidepressant exposure in late pregnancy with the risk of PPH, including studies published before and after 2016.
Methods:
A systematic literature search was conducted using PubMed, OVID Medline, EMBASE, SCOPUS, PsycINFO, and CINAHL from inception to September 9, 2023. Original, peer-reviewed studies (published in English) that reported on the frequency or risk of PPH in women with evidence of antidepressant use during pregnancy and included at least one control group were included.
Results:
Twenty studies (eight published after 2016) met inclusion criteria, most of which focused on the risks of PPH associated with selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs). The main findings from the individual studies were mixed, but the majority documented statistically significant associations of PPH with late prenatal exposure, especially for exposures occurring within 30 days of delivery, compared with unexposed deliveries. Fourteen studies addressed underlying antidepressant indications or their correlates. Few studies focused on prenatal antidepressants and the risk of well-defined severe PPH or on antidepressant dose changes and general PPH risk. None examined competing risks of antidepressant discontinuation on mental health outcomes.
Conclusions:
Late pregnancy exposure to antidepressants may be a minor risk factor for PPH, but it is unclear to what extent reported associations are causal in nature, as opposed to correlational (effects related to nonpharmacological factors including maternal indication). For patients needing antidepressants during pregnancy, current evidence does not favor routinely discontinuing antidepressants specifically to reduce the risk of PPH.
Introduction
Postpartum hemorrhage (PPH), the occurrence of greater-than-expected levels of blood loss after delivery, is diagnosed in approximately 14 million patients worldwide (WHO, 2018). Although PPH is believed to occur in 1–3% of deliveries (Corbetta-Rastelli et al., 2023), rates vary depending on the definition of PPH that is used (Huang et al., 2023). PPH presents clinically along a spectrum ranging from mild cases to potentially life-threatening obstetric emergencies (Sheldon et al., 2014). Despite advances in obstetric care, PPH is still a leading cause of maternal mortality worldwide (Say et al., 2014), underscoring its importance from a public health perspective.
As concerning, the frequency of PPH in the United States is increasing. Between 2000 and 2009, the frequency of PPH increased in the United States from 2.7% to 4.3% (Corbetta-Rastelli et al., 2023). Increasing occurrences of PPH have been linked to higher rates of cesarean deliveries and diagnosed placenta accreta and placenta previa (Corbetta-Rastelli et al., 2023). However, increases in PPH diagnoses also parallel climbing rates of antidepressant use in pregnant women—approximately 6% to 8% of pregnant women in the United States are prescribed antidepressants (as reported in Anderson et al., 2020).
Although exact pharmaco-mechanistic causes are uncertain, antidepressants have been associated with multiple types of abnormal bleeding including gastrointestinal, menstrual, postsurgical, and perinatal blood loss (Andrade and Sharma, 2016). The potential link between prenatal exposure to serotonergic antidepressants with PPH has been evaluated in observational studies of diverse designs. The most recent meta-analysis reviewed studies published through 2016 (six cohort studies, two case-control studies) and concluded that the overall risk of PPH was increased with prenatal exposure to serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) (odds ratio [OR] 1.23, 95% confidence interval [CI] 1.06 to 1.44) (Jiang et al., 2016). Significant associations were reported with current (on the delivery date) and recent (within 30 days of the delivery date) antidepressant exposure, but not past exposure (at least 30 days preceding the date of delivery), consistent with a potentially direct pharmacological mechanism.
Despite these findings, a causal link between serotonergic antidepressants and PPH remains controversial. In the same meta-analysis, prenatal exposure to non-SSRI and non-SNRI antidepressants was also associated with increased risk of PPH (OR 1.31, 95% CI 1.1 to 1.56) and the impacts of unmeasured maternal factors (including antidepressant indications) on the observed associations were unknown (Jiang et al., 2016). Numerous reports on the association of antidepressants in pregnancy with PPH have been published after 2016, many of which account for maternal antidepressant indications or correlates of those indications using various study design features or analytic approaches. An updated systematic review focused on prenatal antidepressants in late pregnancy and the risk of PPH is needed.
Materials and Methods
Inclusion and exclusion criteria
A systematic literature search was conducted using PubMed, OVID Medline, EMBASE, SCOPUS, PsycINFO, and CINAHL (from inception to September 9, 2023) to identify original, peer-reviewed studies, published in English, that reported on the frequency or risk of PPH (primary or secondary) in women with evidence of antidepressant use during pregnancy. In addition, inclusion criteria required at least one comparison or referent group and sufficient reporting of study methods and outcomes to permit quality assessment. Abstracts and unpublished data were ineligible for inclusion. Although the highest quality clinical evidence comes from randomized trials, such designs cannot be used for investigating antidepressant safety in pregnancy. Therefore, we targeted controlled observational studies for review, including prospective cohort studies, retrospective cohort studies (using registries or claims databases), case-control studies, and nested case-control studies.
Identification and screening of studies
The literature search strategy included a combination of text-word fields for the following terms or concepts: (a) postpartum hemorrhage, as well as combined terms (e.g., postpartum, postpartum period, puerperium, hemorrhage, blood loss); (b) antidepressants or antidepressive agents, including broad classes (SSRIs, SNRIs, tricyclic antidepressants [TCAs], monoamine oxidase inhibitors [MAOIs]), individual agents within these classes, and other individual drugs (bupropion, mirtazapine, trazodone, nefazodone, vilazodone, and vortioxetine); and (c) cohort studies, prospective studies, retrospective studies, or related terms (observational design). In addition to electronic database searching, the reference lists from individual studies and relevant systematic reviews, meta-analyses, and nonsystematic reviews were reviewed for additional articles. The titles and abstracts of all retrieved citations were screened by a study team member (W.V.B.) to find potentially relevant publications.
Exposures
Qualifying antidepressant exposures included evidence of exposure to SSRIs, SNRIs, TCA, MAOIs (including conventional oral agents, transdermal selegiline, and the reversible inhibitor of MAO-A, moclobemide), bupropion, mirtazapine, vortioxetine, vilazodone, nefazodone, and/or trazodone (150–600 mg/day) during pregnancy. We chose late pregnancy (third trimester) as our main exposure window given presumed increases in biological plausibility with exposures closer to or overlapping with the date of delivery. Although confirmed daily exposure to antidepressants within days of delivery would be desirable, we expected that this definition would be excessively stringent, resulting in too few included studies to permit meaningful review. Instead, we used any third trimester antidepressant exposure as a proxy for late pregnancy. Acceptable referent groups included antidepressant non-users (during pregnancy), early (nonthird trimester) pregnancy antidepressant users, former antidepressant users (before but not during pregnancy), and bupropion users (without coexposure to serotonergic antidepressants).
Endpoints
For this report, PPH was clinically defined as an estimated blood loss (EBL) of >500 mL or >1000 mL within 24 hours following vaginal or cesarean delivery, respectively. In 2017, the definition of PPH was amended by the American College of Obstetrics and Gynecology to a cumulative blood loss >1000 mL with signs and symptoms of hypovolemia within 24 hours following delivery, regardless of delivery mode (ACOG, 2017). ICD-10 codes used to define PPH in Swedish pregnancy registers have used an EBL >1000 mL as a reference standard (Ladfors et al., 2021). However, most of the qualifying North American studies in this review were published before 2017, and given the time needed to implement changes in clinical practice, reports published in 2017 or soon thereafter may not have classified PPH using the amended definition. Formal definitions for PPH severity classification and staging were not used in this review, although such definitions exist (American College of Surgeons, 1997; Lagrew et al., 2022). Instead, we report results from the reviewed studies using the definitions of PPH severity used by the authors. Similarly, when studies reported on subtypes of PPH, such as PPH secondary to diffuse or focal uterine atony, the case definitions used by the authors were reviewed.
Data abstraction
Data on study design, study period, year of publication, inclusion and exclusion criteria, total number of individuals (or deliveries) in each exposure group, information regarding antidepressant exposure (including exposure intensity and exposure windows), outcome measures and definitions, and confounding variables and approaches to confounding management were extracted. Although raw and adjusted effect sizes were abstracted, the emphasis for reviewed studies was on the most-adjusted effect size estimates and associated 95% CIs.
Quality assessment
The quality of the included studies was assessed by two independent investigators (H.K.B., K.M.M., or W.V.B.) using the Newcastle-Ottawa scale for nonrandomized studies (Higgins et al., 2019). Discrepancies were resolved by a third investigator (M.C.). The definitions for high-, medium-, and low-quality cohort and case-control studies are shown in Supplementary Tables S1a and S2a. To assess follow-up adequacy in cohort studies, we chose the upper limit (80%) of the recommended follow-up threshold of 60%–80% based on the high likelihood of a “missing not at random” mechanism for loss-to-follow-up.
Results
The electronic database search yielded 50 citations from PubMed, 30 from OVID Medline, 317 from EMBASE, 102 from SCOPUS, 48 from PsycINFO, and 24 from CINAHL. After removing duplicate reports and after adding 3 citations following the bibliographic review, a total of 389 unique studies remained (Fig. 1). After screening titles and abstracts, 366 records were excluded and 23 reports were further assessed for eligibility. One report each was excluded owing to PPH not being a reported outcome, absence of a control group, and nonqualifying study design (data mining study), leaving 20 reports that met inclusion criteria (Table 1).
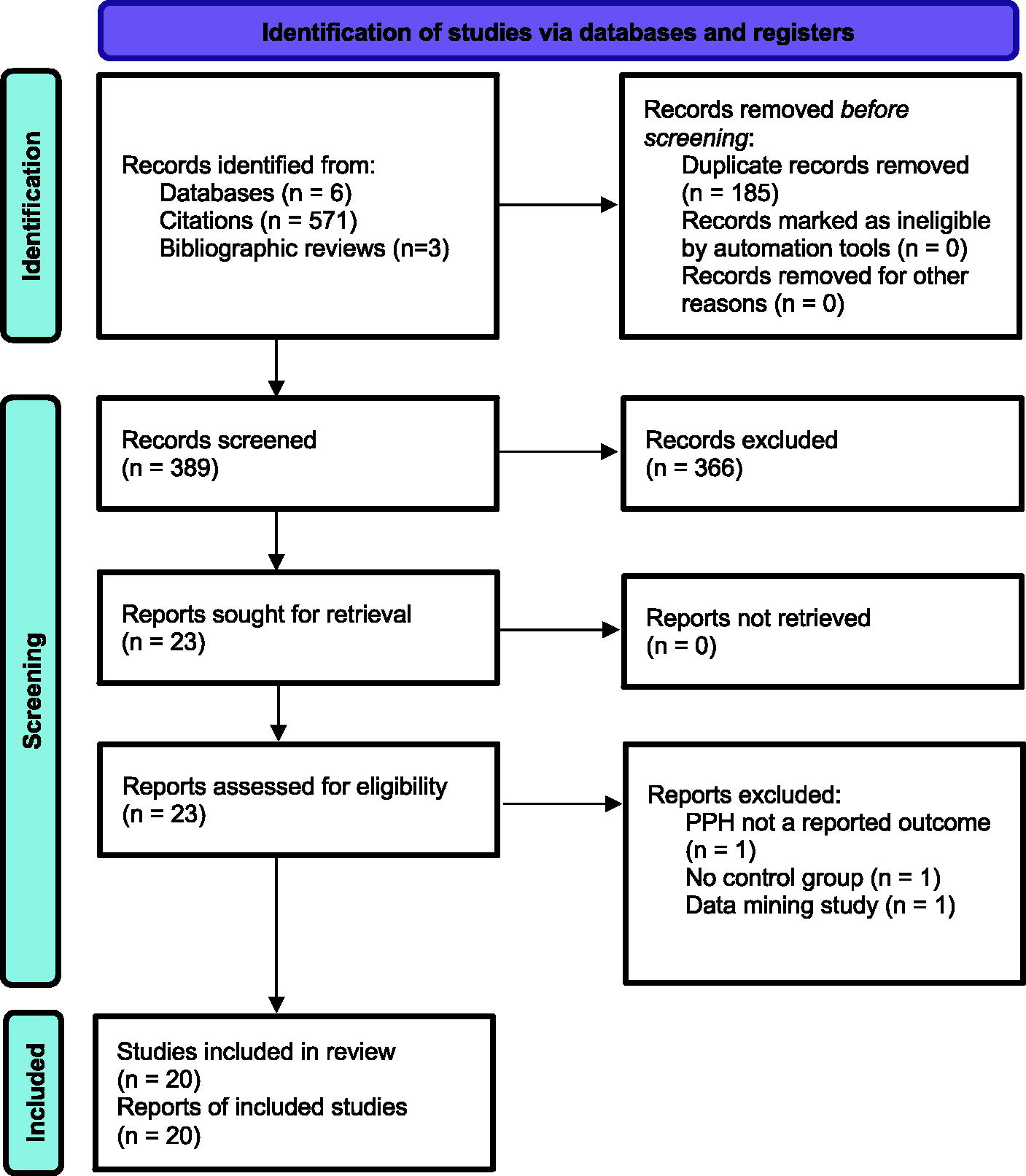
PRISMA flow diagram. PPH, postpartum hemorrhage.
Summary of the Design Characteristics and Main Results of Controlled Observational Studies of Antidepressants and the Risk of Postpartum Hemorrhage
Study designs included case-control studies (CC), prospective cohort studies (PC), and retrospective cohort studies (RC).
Refers to the number of pregnancies or deliveries.
Broad approaches to the management of potential confounding factors are listed. Specific confounding factors or PPH risk factors accounted for in individual studies are summarized in Tables 2 and 3.
Results presented in the table are for fully adjusted (multivariable) models, as indicated by lower-case a (e.g., aOR, aRR, aHR, etc.), unless otherwise specified. Unadjusted results are presented only for studies in which no multivariable models were used.
Results from two register-based cohorts (one from Sweden, one from British Columbia, Canada) were reported. All cohort members had diagnosed OCD based on corresponding ICD-9/-10 diagnosis codes.
Study antidepressants included SSRIs, SNRIs, tricyclic antidepressants, mirtazapine, and moclobemide. Although an additional exposure group included cohort members with a psychiatric diagnosis but no exposure to ADs during pregnancy, the risk of PPH was not compared between AD-exposed deliveries and those exposed to psychiatric diagnoses only.
Unexposed cohort members were matched 5:1 with exposed cohort members from an original control pool of 641,364 women.
Analyses of study data included an adjusted analysis, an analysis restricted to women with specific diagnoses (diagnosed depression, anxiety disorders, or specific pain conditions), an analysis stratified by propensity score (fully adjusted models), and an analysis stratified on high-dimensional propensity score. Fully adjusted models used PS stratification to at least partially account for imbalances in pre-defined potential confounding factors.
Case-control study included 6378 cases of PPH and 31,795 controls.
SRI antidepressants (n = 29,222) included SSRIs, SNRIs, and selected TCAs (amitriptyline, clomipramine, imipramine). Non-SRI antidepressants (n = 4456) included bupropion, mirtazapine, nefazodone, trazodone, and selected TCAs (amoxapine, desipramine, doxepin, maprotiline, nortriptyline, trimipramine).
AD exposures were identified using pharmacy dispensing records and were converted to fluoxetine-equivalent weekly doses. Longitudinal AD exposure trajectories (through 35 weeks’ gestation) were identified using k-means clustering. Low, moderate, and high (dose) exposures corresponded to approximately 10–20 mg, 40 mg, and 70–80 mg, respectively, in fluoxetine equivalents. The low prenatal AD exposure with dose reduction or discontinuation group was exposed to approximately 10 mg/day in fluoxetine equivalents with first trimester dose reduction or discontinuation.
Case-control study included 2460 cases of PPH and 23,943 controls.
Missing information was handled by imputation for the exposure variable, smoking, country of birth, and occupation. This table displays only the results of analyses performed before multivariate imputation since imputation did not affect the overall results of the main analyses including estimated strengths of associations.
Case-control study included 327 cases of severe PPH. Four controls were selected for each case.
AD, antidepressants; CI, confidence interval; C-section, cesarean section delivery; dx, diagnosis; Hgb, hemoglobin; OCD, obsessive-compulsive disorder; OR, odds ratio; PPH, postpartum hemorrhage; PS, propensity score; RR, relative risk; SNRIs, serotonin-norepinephrine reuptake inhibitors; SRI, serotonin reuptake inhibitor; SSRIs, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant; UK, United Kingdom.
Study characteristics
Data from over 117,000 exposed deliveries, 8.6 million unexposed deliveries, and 360,000 variously defined cases of PPH were represented among the 20 qualifying studies. These included 3 prospective cohort studies, 14 retrospective cohort studies, and 3 case-control studies, as shown in Table 1.
The most common approach to defining PPH used ICD-9/-10 diagnosis codes, either exclusively (n = 7 studies) or in combination with data on EBL at delivery (n = 1 study). EBL data was used exclusively to define PPH in 7 studies, three of which used an EBL diagnostic threshold >1000 mL as the main endpoint definition (Heller et al., 2017; Lindqvist et al., 2014; Skalskidou et al., 2020). Three studies used alternative definitions for PPH, including “bleeding during or after delivery” (Malm et al., 2015), “bleeding after partus” (Reis and Kallen, 2010), or “severe PPH” involving postpartum blood loss >1500 mL, a drop in peripartum hemoglobin concentration, or transfusion of 4 or more units of blood (Waterstone et al., 2001). No studies used quantitative blood loss (QBL).
Two studies each included severe PPH (Grzeskowiak et al., 2015; Waterstone et al., 2001) or atonic PPH as specific endpoints (Joseph et al., 2015; Palmsten et al., 2013), while PPH was undefined in two studies (Su et al., 2023; Suzuki and Kato, 2017). Thirteen studies focused specifically on the association of prenatal antidepressants with PPH, while the remaining studies examined prenatal antidepressants associated with a broad range of pregnancy and/or neonatal complications (Colvin et al., 2011; Malm et al., 2015; Huybrechts et al., 2020; Reis and Kallen, 2010; Su et al., 2023), assessed a variety of risk factors for PPH—antidepressants included (Anouilh et al., 2023), or evaluated risk factors (including antidepressants) for severe obstetric morbidity (Waterstone et al., 2001).
Nearly all studies controlled for or otherwise addressed general confounding or known risk factors for PPH (Table 2). Eight of the 20 reviewed studies addressed potential confounding by indication (Table 3) or accounted for potential correlates of maternal indication such as maternal smoking, drug and alcohol use, and psychotropic medication use (other than antidepressants) during pregnancy. Methods for addressing potential confounding by maternal indication included restricting to mothers with associated mental health or pain-related diagnoses (n = 3 studies), statistical adjustment for maternal psychiatric diagnoses (n = 3 studies), or a combination of approaches including propensity score (PS) methods (n = 2 studies). Maternal antidepressant indications were identified using ICD-9/-10 diagnosis codes (n = 5 studies), self-report (n = 1 study), or validated diagnostic instruments/rating scales (n = 2 studies).
Summary of Selected Risk Factors and Confounding Factors That Were Addressed in Reviewed Studies of Prenatal Antidepressants and the Risk of Postpartum Hemorrhage
The information above refers only to risk factors that were accounted for in either the design or analysis of data focused on the risk of PPH conditioned on antidepressant exposure. Risk factors could have been included as part of the main set of analyses or as part of sensitivity analyses. A solid circle (●) indicates that a given variable or element of data was adjusted for in multivariable analyses. An open circle (○) indicates that a given variable or element of data was used for matching. A gray circle (●) indicates that a given variable or element of data was subject to stratified analysis. A blue open circle (○) indicates that an analysis was performed that restricted the cohort according to the presence or absence of that factor.
Or gestational length.
Includes hypertensive disorders or pregnancy and maternal hypertension.
Analysis of study data include statistical adjustment for variables or data elements specified using a solid circle (●) in the table. Not shown are additional factors that were accounted for in analyses that used propensity score (PS) methods.
Summary of Methods for Addressing Potential Effects of Maternal Antidepressant Indications on the Association of Prenatal Antidepressants and the Risk of Postpartum Hemorrhage
Each of the methods for managing confounding by indication were counted as present (either for the main analysis or in sensitivity analyses) as long as they directly addressed maternal indication for antidepressants, selected correlates of maternal indication (such as maternal smoking, alcohol and drug use, or use of psychotropic medications during pregnancy other than antidepressants), or maternal symptoms potentially managed by antidepressants (e.g., depression, anxiety, pain).
Alternative exposure windows refers, in general, to study designs in which exposure groups included antidepressant exposure during late pregnancy and during time windows preceding (but not including) late pregnancy. A solid circle (●) indicates that the study compared the risks of postpartum hemorrhage (PPH) with antidepressant exposure in late pregnancy compared with exposure to antidepressants in earlier stages of pregnancy. A gray circle (●) indicates the study included late pregnancy and earlier pregnancy exposure windows for prenatal antidepressants, but comparisons were against unexposed referent groups (rather than comparisons between late and earlier pregnancy exposure).
Disease comparison group refers, in general, to study designs in which at least one referent group was unexposed to prenatal antidepressants despite evidence of a maternal indication for antidepressants.
A solid circle (●) indicates that the multivariable analysis was adjusted for at least one maternal diagnosis for which antidepressants are used (diagnosed maternal indication) or symptoms for which antidepressants may be used (such as depressive or anxiety symptoms, or pain). An open circle (○) indicates that the multivariable analysis was adjusted for correlates of maternal depression, such as maternal smoking, drug and alcohol use, and psychotropic medication use (other than antidepressants) during pregnancy.
A solid circle (●) indicates the use of propensity score (PS) or high-dimensional PS (hd-PS) methods to manage confounding, including but not limited to confounding by maternal indication and other potential sources of residual confounding.
Unsupervised machine learning to identify five prenatal antidepressant exposure trajectories based on standardized daily antidepressant doses (fluoxetine equivalents): high sustained antidepressant use (75 mg/day), moderate sustained antidepressant use (40 mg/day), moderate antidepressant use with dose reduction or discontinuation in pregnancy, low sustained antidepressant use (20 mg/day), and low antidepressant use with dose reduction or discontinuation in pregnancy. The latter served as a referent group for statistical analyses adjusted for PPH risk factors and relevant maternal mental health diagnoses. Other referent groups consisted of women with diagnosed depression or anxiety, each with no evidence of prenatal antidepressants.
Exposure groups were composed of women with depression who continued their antidepressants throughout pregnancy (main exposure group) and women with depression who discontinued their antidepressants during the first or second trimester of pregnancy (comparator group).
Quality assessment
Quality assessment based on Newcastle-Ottawa criteria are summarized in Supplementary Tables S1 and S2. With few exceptions, the reviewed studies were generally representative of their underlying populations. All 14 retrospective cohort studies and two case-control studies used registry data or linked claims databases and relied primarily on electronic/automated data from prescription records and diagnosis codes to define exposures and outcomes. Fourteen of the 16 studies that used automated databases were considered high quality based on rigorous management of potential confounding and other steps taken to permit valid comparisons between exposure groups or between cases and controls. However, only eight such studies accounted specifically for maternal indication.
Studies of prenatal antidepressants vs. unexposed
Nine studies documented an increased risk of PPH associated with prenatal antidepressant exposure compared with unexposed controls, defined as no evidence of antidepressant exposure (and no diagnosed maternal antidepressant indication, when specified) during pregnancy. Six of these studies are summarized below, while the remaining three, which also utilized alternative exposure windows, are reviewed in later sections (Hanley et al., 2016; Joseph et al., 2015; Palmsten et al., 2013).
In a retrospective cohort study by Colvin et al., 2011, the risk of PPH was compared between 3703 deliveries with evidence of SSRI exposure at any time during pregnancy and 92,995 control deliveries involving no prenatal SSRI exposure. There was an increased risk of PPH with prenatal SSRIs vs. unexposed deliveries (10.8% vs. 9.1%, OR 1.21 [95% CI 1.09, 1.35]), with an unadjusted risk difference of 17/1000 deliveries. Analyses of PPH risk by prenatal exposure to individual SSRIs showed a significant positive association with fluoxetine but not with sertraline, citalopram, or paroxetine exposure.
A second study by Heller et al., 2017 documented a significantly increased risk of PPH in a cohort of 578 antidepressant-exposed pregnancies that were matched 5:1 (see Table 2) to unexposed control pregnancies. Antidepressant exposures included SSRIs, SNRIs, and TCAs. Adjusted risks of PPH were significantly higher with prenatal antidepressants, both before and after matching. A subanalysis also showed significantly increased PPH risk with prenatal exposure to nonantidepressants (n = 50 deliveries exposed to mood stabilizers, atypical antipsychotics, and/or benzodiazepines; aOR 3.3 [1.1, 9.8]). Associations of PPH were not compared between antidepressants and nonantidepressants.
Grzeskowiak and colleagues (2015) also studied the associations of third trimester exposure to multiple antidepressants (n = 558 exposed deliveries) with primary PPH. Study antidepressants included SSRIs, SNRIs, TCAs, mirtazapine, and moclobemide. An added exposure group included 1292 deliveries involving women with evidence of at least one maternal psychiatric diagnosis but no prenatal antidepressants. Unexposed control deliveries (n = 28,348) had no evidence of a maternal psychiatric diagnosis or prenatal antidepressants. Analyses were adjusted for correlates of maternal indications such as exposure to other (non-AD) psychotropic drugs, but not maternal mental health diagnoses. Compared with unexposed deliveries, the risk of primary PPH was significantly higher with third trimester antidepressants but not maternal psychiatric illness without antidepressants. Comparable results were observed in subgroup analyses restricting to vaginal deliveries and deliveries by cesarean section and in sensitivity analyses restricting the outcome to severe primary PPH (postpartum blood loss ≥1000 mL and the occurrence of postpartum anemia). The risk of PPH was not compared between antidepressant-exposed deliveries and those exposed to psychiatric diagnoses only.
Lindqvist et al. (2014) also found an increased risk of PPH with prenatal SSRIs compared with SSRI-unexposed deliveries. Increased PPH risk was observed for any type of delivery, for nonoperative vaginal deliveries, and for operative vaginal deliveries. Average blood loss was higher with SSRI exposure than controls but was still within normal parameters (484 mL vs. 398 mL, p < 0.001).
A retrospective cohort study using Swedish registry data examined associations of SSRIs at any time in pregnancy (n = 8643) with the risk of PPH, compared with no prenatal SSRIs or maternal psychiatric illness (n = 268,006) (Skalskidou et al., 2020). A second exposure group consisted of prior or current psychiatric illness without prenatal SSRIs (n = 28,672). There were significantly higher adjusted risks of PPH with both prenatal SSRIs and prior/current psychiatric illness without prenatal SSRIs, compared with unexposed controls. PPH risks were not compared between deliveries exposed to prenatal SSRIs and those exposed to psychiatric illness only.
In a well-controlled retrospective cohort study, Huybrechts et al. (2020) examined PPH risk in 955 deliveries exposed to the SNRI, duloxetine, compared with antidepressant-unexposed deliveries (n = 4,128,460), SSRI-exposed deliveries (n = 65,303), and venlafaxine-exposed deliveries (n = 3573). Late pregnancy exposures to duloxetine, SSRIs, and venlafaxine were defined as occurring within the 30 days preceding delivery. Multiple analytic approaches were used including an adjusted analysis with maternal antidepressant indication, an analysis restricted to women with specific diagnoses (depression, anxiety, and pain conditions), and analyses stratified by PSs. In fully adjusted models with PS stratification, the risk of diagnosed PPH was significantly increased with late pregnancy duloxetine compared with unexposed deliveries and SSRI-exposed deliveries. Risk differences with duloxetine vs. unexposed and duloxetine vs. SSRIs were 12.3/1000 and 10.0/1000, respectively. The risk of PPH was similar between duloxetine- and venlafaxine-exposed deliveries.
An early case-control study by Waterstone and colleagues (2001) examined risk factors for severe obstetric morbidity including “severe hemorrhage,” defined as an EBL >1500 mL, a peripartum drop in hemoglobin concentration ≥40 g/L or requiring an acute blood transfusion of ≥4 units. Self-reported use of antidepressants during pregnancy was associated with an increased adjusted risk of severe PPH compared with no self-reported antidepressant use during pregnancy.
Two smaller prospective studies, three large retrospective cohort studies (two of which are reviewed in later sections [Malm et al., 2015; Reis and Kallen, 2010]), and one case-control study did not find a significantly increased risk of PPH with prenatal antidepressants compared with unexposed controls.
In a prospective cohort study, 51 pregnant women taking SSRIs during the third trimester and 212 women who took no prenatal antidepressants were followed from enrollment (at or before the 20th week of pregnancy) until 52 weeks after delivery (Kim et al., 2016). Maternal psychiatric diagnoses were confirmed at baseline using structured diagnostic interviews. Depressive symptoms were measured using validated rating scales (Williams and Terman, 2003). No significantly increased risk of PPH was found with third trimester SSRIs. The main findings were supported after restricting the analyses to antidepressant exposure at the time of delivery and after including women taking concomitant medications that could increase the risk of abnormal bleeding.
A more recent prospective cohort study designed to find risk factors for PPH followed 20,238 pregnant women from the date of prenatal enrollment through the date of delivery (Anouilh et al., 2023). The cohort was restricted to vaginal deliveries. Self-reported prenatal antidepressant exposure was not associated with a significantly increased risk of PPH in univariable analyses.
Lupattelli and colleagues (2014) conducted a retrospective cohort study using registry data from Norway. Exposure groups included any prenatal antidepressant use (527 deliveries exposed to SSRIs or SNRIs and 59 deliveries exposed to TCAs or other antidepressants). Exposures were further classified as occurring in later pregnancy (from 30 weeks gestation to the date of delivery). A disease comparison group consisted of deliveries to women with depression but no prenatal antidepressants (n = 1282), defined using cutoff scores on a validated rating scale (Fink et al., 2004; Strand et al., 2003). Unexposed control deliveries had neither depression nor prenatal exposure to antidepressants (n = 55,411). Analyses were adjusted for both PPH risk factors and maternal depressive symptoms (see Tables 2 and 3). There was no significantly increased risk of PPH with later pregnancy SSRIs or SNRIs, or with prenatal depression/no prenatal antidepressants. The risk of PPH was not compared between prenatal antidepressants and prenatal depression without antidepressants.
In a large case-control study that included 2460 PPH cases (defined using ICD-9 or ICD-10 diagnosis codes) and 23,943 controls, Salkeld and colleagues (2008) found no significantly increased adjusted risk of PPH with exposure to prenatal SSRIs or non-SSRIs occurring within 90 days of delivery. Adjusting the exposure window to 30 days preceding delivery resulted in similar findings.
One large study used data from two separate register-based cohorts from Sweden (2990 exposed deliveries, 5053 control deliveries) and from Canada (1896 exposed deliveries, 355 control deliveries) to study the associations of antidepressants used to treat obsessive-compulsive disorder (OCD) with adverse pregnancy and neonatal outcomes (Fernandez de la Cruz et al., 2023). All cohort members had a diagnosis of OCD based on ICD-9/-10 diagnosis codes. The main antidepressant exposure group consisted of deliveries with evidence of SSRI or clomipramine use during pregnancy. Control deliveries had no evidence of prenatal SSRIs or clomipramine. Significantly higher adjusted risk of PPH was observed with prenatal antidepressants in the Swedish cohort, but not the Canadian cohort.
Studies using alternative antidepressant exposure windows
Four studies compared PPH risk with unexposed controls using alternative exposure windows, generally consistent with late pregnancy exposure vs. exposure occurring earlier in pregnancy. The main comparisons, however, were with antidepressant-unexposed deliveries, not between late and early pregnancy exposures. Three studies reported an increased risk of PPH with antidepressant exposure within 30 days of delivery, while two reports showed no significant increased risk of PPH with prenatal antidepressant exposure before the month preceding delivery, and one study reported increased PPH risk with both earlier and later prenatal antidepressant exposure.
Reis and Kallen (2010) conducted a retrospective cohort study of self-reported prenatal antidepressant use and the risk of a variety of delivery outcomes including “bleeding after partus.” Antidepressant exposures were defined as occurring in “early” pregnancy (n = 13,080), “later” in pregnancy (n = 6066), or both (n = 4127). Control pregnancies had no self-reported antidepressant use (n = 1,236,053). In general, early exposures occurred between 10 and 12 weeks’ gestation and later exposures occurred afterwards. The adjusted risk of PPH was significantly higher with early prenatal antidepressant use than controls; however, no significant increase in PPH risk was associated with later prenatal exposure or with both early and later prenatal exposure.
A second retrospective cohort study compared the risks of PPH in a cohort of 8027 deliveries exposed to SSRIs or SNRIs on the delivery date or during late pregnancy (at least 15 of the 30 days preceding the date of delivery) and 1747 deliveries with exposures during mid-pregnancy (Hanley et al., 2016). An unexposed control group consisted of 310,813 deliveries with no evidence of prenatal SSRI/SNRI exposure. Analyses controlled for maternal indications, psychotropic medications other than antidepressants, and PPH risk factors (see Tables 2 and 3). There was a significantly higher adjusted risk of PPH with SNRIs, both in late pregnancy and on the delivery date. Nonsignificant risks of PPH were observed with late pregnancy SSRIs, SSRI exposure on the date of delivery, mid-pregnancy SNRI exposure, and mid-pregnancy SSRI exposure.
Joseph and colleagues (2015) conducted a case-control study of PPH risk conditioned on exposure to antidepressants during pregnancy. Study data were derived from linked physician claims, hospitalization, and vital statistics databases. PPH and atonic PPH cases (n = 6378) were identified using ICD-9 and ICD-10 diagnosis codes. Controls (n = 31,795) were randomly selected after matching on index date and the delivering hospital. Antidepressant exposures consisted mainly of SSRIs but also included SNRIs, TCAs, bupropion, mirtazapine, trazodone, and moclobemide. The nutraceutical serotonin precursor, l-tryptophan, and the anxiolytic, buspirone (a serotonin 5-HT1A partial agonist), were also included as study drugs. Antidepressant exposure windows included any prenatal exposure, recent use (within 30 days of delivery), and past use (outside of the last 30 days of pregnancy). There was a significantly increased adjusted risk of PPH with any prenatal AD exposure, compared with no prenatal antidepressants. Both recent and past use of antidepressants were also associated with an increased risk of PPH.
Palmsten and colleagues (2013) conducted a well-controlled retrospective cohort study of the risk of PPH associated with current antidepressant use (on the delivery date), recent use (within 30 days of delivery), and past use (>1–5 months preceding delivery), as compared with controls having no evidence of antidepressant use in the 5 months preceding delivery. Study drugs were classified as SRIs based on a dissociation constant (Kd) threshold of 0–9.9 nM at 5-HTT. Other antidepressants were considered non-SRIs. High-, medium-, and low-dose exposures to study drugs were defined according to “usual” doses from a standard clinical pharmacology textbook. There was a total of 29,222 deliveries with prenatal exposure to SRI monotherapy, 4456 deliveries exposed to non-SRI monotherapy, and 69,044 unexposed (control) deliveries. The cohort was restricted to women with evidence of a diagnosed mood or anxiety disorder identified using ICD-9/-10 codes. PS methods were used to manage confounding. There was a significantly higher adjusted risk of PPH with current SRIs and recent SRIs, but not past SRIs, compared with unexposed deliveries. PPH risk was also associated with current non-SRI exposure, but not recent or past non-SRI exposure. The risk estimates for PPH were highest with high-dose exposure, followed by medium-, then low-dose exposure.
Studies with disease comparison controls
Two studies reviewed in this section compared the risk of PPH between prenatal antidepressant use and disease comparison controls (maternal psychiatric diagnosis without prenatal antidepressants). Neither study found increased PPH risk associated with prenatal antidepressants. A third study, reviewed in the next section below, documented an increased risk of PPH with prenatal antidepressants vs. depression and anxiety disease comparison groups (Palmsten et al., 2020). Three studies reviewed earlier included disease exposure groups (Grzeskowiak et al., 2015; Lupattelli et al., 2014; Skalskidou et al., 2020), but none compared PPH risks between prenatal antidepressants and psychiatric diagnoses with no prenatal antidepressants.
A retrospective cohort study using registry data from Finland examined the risk of “bleeding during or after delivery” with prenatal SSRIs (n = 15,729), compared with unexposed (no SSRIs/no evidence of maternal mental health diagnoses, n = 31,294) and disease comparison (no SSRIs/evidence of a maternal psychiatric diagnosis, n = 9652) controls (Malm et al., 2015). Analyses were adjusted for PPH risk factors and correlates of underlying antidepressant indications. The risk of PPH was not significantly increased with prenatal SSRIs vs. unexposed deliveries. The adjusted risk of PPH was significantly lower with prenatal SSRIs than disease comparison controls and was significantly higher in the disease comparison group than unexposed controls.
Su et al. (2023) conducted a retrospective cohort study of prenatal antidepressants and the risk of PPH using registry data from Taiwan. Exposure groups included prenatal antidepressant users with diagnosed depression (n = 7857) and prenatal antidepressant nonusers with diagnosed maternal depression (n = 2006). Unexposed deliveries had no evidence of prenatal antidepressants and no diagnosed maternal depression (n = 1,619,198). Analyses were adjusted for maternal use of psychotropic medications other than antidepressants. The risk of PPH was not increased with third trimester antidepressants compared with maternal depression only. The risks of PPH in the prenatal antidepressants group and the unexposed group were not compared. There was a nonsignificant risk of PPH in the depression-only group compared with the unexposed group.
Studies with antidepressant discontinuation or dose reduction
Two studies included exposure groups in which there was evidence of either a reduction in the dose of prenatal antidepressants or antidepressant discontinuation during pregnancy.
Suzuki and Kato (2017) conducted a prospective cohort study of 60 women who continued their antidepressants throughout pregnancy and 26 women who discontinued their antidepressants during the first or second trimester. There was a nonsignificant reduced risk of PPH with continuation of antidepressants throughout pregnancy compared with antidepressant discontinuation despite a high frequency of diagnosed PPH cases (43.3% vs. 53.8%). It is unclear if there were significant differences in PPH risk profiles between women who continued antidepressants and those who stopped them during pregnancy.
An interesting retrospective cohort study by Palmsten et al. (2020) used unsupervised machine learning to identify five prenatal antidepressant exposure categories using administrative claims data. Exposure categories were based on standardized daily antidepressant doses (in fluoxetine equivalents) at multiple time points through 20 and 35 weeks gestation. These included high sustained antidepressant use (75 mg/day, n = 424), moderate sustained antidepressant use (40 mg/day, n = 1918), moderate antidepressant use with dose reduction or discontinuation in pregnancy (40 mg/day with first trimester dose reduction or discontinuation, n = 1907), low sustained antidepressant use (20 mg/day, n = 3170), and low antidepressant use with dose reduction or discontinuation in pregnancy (20 mg/day with first trimester dose reduction or discontinuation, n = 7622). The latter served as a referent group for statistical analyses adjusted for PPH risk factors and relevant maternal mental health diagnoses (see Tables 2 and 3). Other referent groups consisted of women with diagnosed depression (depression only, n = 4949) or anxiety (anxiety only, n = 9406), each with no evidence of prenatal antidepressants. There was a significantly higher risk of PPH with high sustained, moderate sustained, and low sustained antidepressant use, compared with low antidepressant exposure with dose reduction/discontinuation. Comparable results were observed using anxiety only as the referent category. When depression only was used as a referent category, only high sustained antidepressant use was associated with a significantly higher risk of PPH.
Discussion
This systematic review provides an updated summary of evidence linking prenatal antidepressants with the risk of PPH. Two prior comprehensive reviews that were focused specifically on this topic were a meta-analysis of eight studies published prior to 2017 (Jiang et al., 2016) and a systematic review of four studies published before 2015 (Bruning et al., 2015). We summarized the findings of 20 studies, eight of which were published between 2017 and 2023. These added studies, like those preceding, were focused mainly on the risks of PPH associated with late prenatal exposure to SSRIs and SNRIs. Although the main findings from the individual studies in this review were mixed, the majority document a statistically significant increased risk of PPH with late pregnancy antidepressants, especially for exposures occurring within 30 days of delivery, compared with unexposed deliveries.
Whether the association between prenatal antidepressants and PPH is causal or correlational in nature is still debated. Several lines of evidence support causal theories including previously reported associations of serotonergic antidepressants with other types of abnormal and operative bleeding (Andrade and Sharma, 2016), serotoninergic mechanisms governing platelet and myometrial functioning that may also be targeted by antidepressants (Berger et al., 2009; López Bernal, 2003; Walther et al., 2003), and pooled results of observational studies showing increased PPH risk with antidepressant exposure in late but not early pregnancy (Jiang et al., 2016). On the contrary, it is unknown if antidepressant-mediated platelet dysfunction or interference with hemostatic postpartum uterine contractility contributes to the risk of PPH. Activation of myometrial serotonin receptors has been shown, in preclinical models, to cause either increased or decreased uterine contractility (Li et al., 2016; Lychkova et al., 2014; Mihalyi et al., 2003; Minosyan et al., 2007; Nakamura et al., 2008), and multiple studies documented significant associations of PPH with prenatal antidepressant exposures occurring in time windows too far in advance of the date of delivery to support a directly acting pharmacological mechanism (Joseph et al., 2015; Palmsten et al., 2013; Reis and Kallen, 2010). If biological plausibility increases with proximity to the date of delivery, as might be expected in this case, these results weaken—though do not necessarily refute—a pharmacologically mediated link between late pregnancy exposure to serotonergic antidepressants and heighted PPH risk.
Also in support of a potential causal mechanism, the results of some individual studies suggest a linear effect of relative antidepressant dose/cumulative exposure and PPH risk (Palmsten et al., 2013, 2020), including a hospital-based cohort study published after the dates of inclusion for this review that documented significantly higher rates of PPH, defined as postpartum EBL >1000 mL, with high- (23.9%) and moderate- (14.6%) dose SSRIs at delivery than with unexposed deliveries (8.4%) (Ondemark et al., 2024). In this case, pharmacologically based causality may be strongly inferred if higher antidepressant doses result in greater levels of 5-HTT blockade or activation of other mechanisms leading to increasing platelet dysfunction and/or abnormal uterine contractility. To the best of our knowledge, however, such correlations have not been shown and experimental evidence suggests that the relationship between antidepressant dose and 5-HTT occupancy is hyperbolic rather than linear, plateauing at 80% 5-HTT occupancy, generally when minimum recommended doses are reached (Sorensen et al., 2022). Alternatively, higher doses of antidepressants in late pregnancy may be a proxy for more severe psychopathology or may reflect compensatory dose adjustments due to the increased activity of drug metabolizing isoenzymes (CYP 3A4, 2D6, and 2C9) known to occur in pregnancy (Feghali et al., 2015; Pariente et al., 2016), with as yet undetermined effects pertaining to PPH risk (Delegiannidis et al., 2014).
With relatively few exceptions (Grzeskowiak et al., 2015; Huybrechts et al., 2020; Lupattelli et al., 2014; Palmsten et al., 2020; Waterstone et al., 2001), the associations between prenatal antidepressants and PPH were generally weak, making them especially susceptible to confounding. This includes confounding by indication given associations of prenatal depression with PPH risk factors including prolonged labor, pre-eclampsia, placental abnormalities, and cesarean section or instrumental delivery (ACOG, 2023; Jahan et al., 2021). Confounding by maternal indication is indirectly suggested by studies that showed elevated PPH risk with maternal indications only (no exposures to antidepressants) (Malm et al., 2015; Skalskidou et al., 2020; Su et al., 2023), and is more directly implied in studies documenting no significant differences in the risk of PPH between third trimester antidepressants and depression only (Su et al., 2023). Large, well-designed retrospective cohort studies enabled a more complete accounting of maternal depression and additional PPH risk factors (Fernandez de la Cruz et al., 2023; Huybrechts et al., 2020; Lupattelli et al., 2014; Palmsten et al., 2020; Palmsten et al., 2013) as well as the consideration of potential proxies for increased severity or complexity of antidepressant indications (Grzeskowiak et al., 2015; Hanley et al., 2016; Lupattelli et al., 2014; Malm et al., 2015; Palmsten et al., 2020; Palmsten et al., 2013; Su et al., 2023). However, even these studies yielded mixed results, leaving open the question of whether positive associations of antidepressants with PPH are truly independent of maternal indications or relevant correlates of those indications.
The comparative risks of PPH between different antidepressants or antidepressant classes also remain uncertain. Palmsten and colleagues (2013) found an increased risk of PPH with individual antidepressants and Hanley et al. (2016) documented a significantly higher risk of PPH with late pregnancy SNRIs but not SSRIs, each compared with unexposed controls. Colvin and colleagues (2011) documented a significantly increased risk of PPH with fluoxetine, but not sertraline, citalopram, or paroxetine. One study directly compared the risk of PPH between SSRIs and SNRIs and found that the use of duloxetine during late pregnancy was associated with a significantly greater risk of PPH than late pregnancy SSRIs, but not the alternative SNRI, venlafaxine (Huybrechts et al., 2020). More comparisons of PPH risk between individual antidepressants are needed, especially for fluoxetine, a medication that may have an extended window of risk for abnormal bleeding given the long elimination half-life of its major active metabolite, norfluoxetine (T½ =7–15 days) (Bergstrom et al., 1993). Comparisons involving selected SNRIs and TCAs used to manage various forms of chronic pain will need to account for the likelihood of concurrent anti-inflammatory analgesics that may increase the risk of bleeding and may not be accounted for in prescription records if available over the counter (Hamrick and Nykamp, 2015). To the best of our knowledge, no published studies have examined PPH risks associated with bupropion, a first-line antidepressant lacking serotonergic activity (Ascher et al., 1995) that may be often prescribed for pregnant women to address depression and/or smoking cessation (Bérard et al., 2016).
At present, it is unknown if the severity of PPH is greater with prenatal exposure to antidepressants. The clinical significance of nearly all reviewed studies is limited by generally small absolute differences in PPH risk and estimated postpartum blood loss (as reported in one study) between exposed and unexposed groups. As noted earlier, PPH presents along a spectrum of severity ranging from mild cases requiring no specific interventions to life-threatening events. Even minor differences in the risk of severe, life-threatening PPH would be of major clinical significance. However, nearly all of the reviewed studies defined PPH based on minimum EBL thresholds or ICD codes that likely reflect the clinical application of these same criteria. Without more information on laboratory or physiological indices of acute blood loss and interventions needed to manage the same, these studies cannot fully address questions related to prenatal antidepressants and the risk of severe PPH (Kerr and Weeks, 2017). One study applied a stringent definition of severe PPH requiring postpartum blood loss >1500 mL, associated physiological changes (peripartum fall in hemoglobin concentration >40 g/L), or aggressive intervention (acute transfusion of >4 units of blood) (Waterstone et al., 2001). Although the adjusted risk estimate was large (aOR 10.55), it was also imprecise, given the very wide 95% confidence limits. More well-controlled studies of antidepressants and the risk of severe PPH are needed.
The clinical risk for PPH in general, and severe PPH in particular, requires thorough evaluation for patients who require antidepressants in late pregnancy and present with additional PPH risk factors, even if late pregnancy antidepressant exposure is only an indirect marker for heightened risk. However, the collective literature offers little guidance for stratifying antidepressant-treated patients based on their individual PPH risk profiles. For the reviewed studies, important patient-level characteristics that bear on PPH risk were necessarily controlled for at the population level to show independent associations of PPH with antidepressants. In future studies, these same factors may be useful in addressing questions about which antidepressant-exposed patients are at heightened risk for PPH and other adverse obstetric outcomes and, on that basis, may need alterations to their therapeutic plans, closer clinical monitoring, or both.
More antidepressant discontinuation and dose adjustment studies (or retrospective studies that account for time-varying antidepressant exposure) are also needed. One prospective study documented no significant differences in the risk of PPH with antidepressant continuation throughout pregnancy, as compared with antidepressant discontinuation during the first or second trimester (Suzuki and Kato, 2017), but data from only 60 subjects were analyzed. Palmsten and colleagues (2020) classified prenatal antidepressant exposure in terms of relative standard doses and discontinuation (or dose reductions) of antidepressants. However, the relative merits of continuation, discontinuation, or dose-alteration of antidepressants as it pertains to PPH risk are still unclear. Future perinatal antidepressant discontinuation studies will need to account for systematic differences in PPH risk between women who are able to stop or reduce the dose of their antidepressants compared with women who must maintain or increase their antidepressant doses during pregnancy. These factors must be balanced against the risk of clinical deterioration and relapse if antidepressants are stopped, particularly for individuals with a history of severe or recurrent illness (Bayrampour et al., 2020).
There are limitations to this review in addition to those mentioned above. Ours was not a quantitative synthesis owing to broad heterogeneity in study designs, data sources, statistical/analytical approaches, and exposure and outcome definitions. The conclusions in this review nevertheless comport with those of the meta-analysis by Jiang et al. (2016). Our quality rating procedures penalized studies that did not focus specifically on the association of prenatal antidepressants and PPH, many of which reported unadjusted results. This does not mean that such studies were necessarily lower in quality for their intended purposes. Although adjusted comparisons led to higher quality ratings on comparability, the results must still be interpreted cautiously due to the risk of residual confounding. Similar precautions apply to studies that used alternative exposure groups owing to foreseeable differences in indication severity or recurrence risk between patients who continue antidepressants throughout pregnancy and those who are able to reduce antidepressant doses or discontinue them prior to late pregnancy. Finally, several large-scale studies used pharmacy claims and diagnosis codes to define exposures and endpoints, with reduced risk of selection and recall biases (Cooper et al., 2007); however, they were not collected for research purposes and are subject to misclassification. Although prior research has documented reasonably good concordance with various gold standard indicators (Bobo et al., 2014; Johnson and Vollmer, 1991; Landry et al., 1988; West et al., 1995) and PPH (Ladfors et al., 2021; Lain et al., 2008; Romano et al., 2005), medication use cannot be confirmed using pharmacy claims, and the use of diagnosis codes alone for identifying PPH may underestimate both the occurrence of PPH (Butwick et al., 2018; Griffin et al., 2019; He et al., 2020; Walther et al., 2021) and the strength of antidepressant-PPH associations—the latter assuming no significant differences between exposure groups in the risk of misclassification.
Based on our review, late pregnancy exposure to antidepressants may be considered a minor risk factor for PPH. Therefore, clinicians and patients should continue to be appraised regarding the risk of PPH with antidepressants in late pregnancy. Whether the increased risk is the result of causation (a direct effect of antidepressants) or correlation (effects related to non-pharmacological factors) remains unclear. However, increased use of antidepressants in pregnancy, associations of antidepressants with bleeding problems, and associations of antidepressants and depression with bleeding complications and PPH risk factors suggest that heightened vigilance is appropriate within the larger context of pregnancy and depression care. More studies with time-varying measures of both maternal illness and antidepressant exposure during pregnancy, clinically relevant indicators of PPH severity, and valid indicators of the clinical consequences of antidepressant discontinuation or dose adjustments are needed. For patients who require antidepressants during pregnancy to maintain clinical stability and functioning, the current evidence base does not appear to favor routine dose reduction or discontinuation of antidepressants during late pregnancy specifically to reduce the risk of PPH. Instead, decisions about continuing antidepressant treatment into late pregnancy must remain highly individualized, based on a thorough consideration of competing risks associated with both treatment and the lack of treatment, clinical needs, available resources, and patient preferences. Continuation of best-practice risk management strategies should be employed for these patients, including routine IV access, admission type and screen, and close proximity of pharmacologic agents to treat PPH.
Footnotes
Author Disclosure Statement
W.V.B. has received grant or research support from the Mayo Clinic, NIH, National Science Foundation, the Watzinger Foundation, and the Myocarditis Foundation. He has contributed chapters to UpToDate concerning the pharmacological management of bipolar depression. No competing financial interests exist for the remaining authors.
Supplementary Material
Supplementary Tables S1
Supplementary Tables S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.